Embed Size (px)
Citation preview

OBJECTIVES:
The implications of the changing face
of cancer survivors and the
survivorship experience for health
promotion are explored.
DATA SOURCES:
National Cancer Institute and Office of
Cancer Survivorship, and research
and journal articles.
CONCLUSION:
Health promotion has become one of
the most rapidly expanding topics of
interest in the broader arena of
survivorship research.
IMPLICATIONS FOR NURSING
PRACTICE:
Nurses have been vital champions for
a holistic or ‘whole person’ approach
to cancer care and are uniquely
positioned to play a central role in
ensuring that we deliver on the
promise of a valued future life for each
cancer survivor and family member
alive. Promoting healthy lifestyle
behaviors is one of those roles.
KEYWORDS:Cancer survivors, cancer
survivorship, health promotion,
aging, follow-up care, survivorship
research
Julia H. Rowland, PhD: Director, Office of
Cancer Survivorship, Division of Cancer
Control and Population Sciences, National
Cancer Institute, NIH/DHHS, Bethesda, MD
Address correspondence to Julia H.
Rowland, PhD, Office of Cancer
Survivorship, 6116 Executive Blvd, Suite
404, Bethesda, MD 20892; e-mail: rowlandj@
mail.nih.gov
� 2008 Elsevier Inc. All rights reserved.
0749-2081/08/2403-$30.00/0
doi:10.1016/j.soncn.2008.05.002
CANCER
SURVIVORSHIP:RETHINKING THE
CANCER CONTROL
CONTINUUM
JULIA H. ROWLAND
THE CHANGING face of cancer survivors and the survivorshipexperience are dictating a new approach to post-treat-ment cancer care. Specifically, with more survivors, in
particular those aged 65 and older, living longer with a history ofcancer (often as a chronic illness), the need for nurses and otherhealth professionals to identify and address cancer’s lingering andlate health-related consequences is rapidly growing. The implica-tions of these changes for future research and the design and deliv-ery of quality care after cancer are discussed and a new model forconceptualizing this care advanced.
CANCER SURVIVORSHIP: SECURING A PLACE ON THE CANCER
CONTROL CONTINUUM
I n 1996 when the National Cancer Institute established theOffice of Cancer Survivorship (OCS), interest in the care and
outcomes of those living long term following a cancer diagnosiswas just beginning to garner the attention of clinical researchers.Pressure to attend to this sector of the cancer control continuum,that expanding period between the completion of active treatmentand the end of life (whether from cancer or some unrelated illness),was driven largely by survivors themselves. With the prospect ofyears of life ahead of them, the new generation of cancer survivors,beneficiaries of the many advances in early detection, more effec-tive treatments, better supportive care, and long-term surveil-lance, began to turn to their health care providers in the hopesthat these individuals could provide them with information aboutwhat to expect in the future. The OCS was expected to help provide
Seminars in Oncology Nursing, Vol 24, No 3 (August), 2008: pp 145-152 145

146 J.H. ROWLAND
cancer survivors and their health care practi-tioners with the evidence base to inform thesedialogues.
The overall mandate of the OCS was, and re-mains, to improve the length and, importantly,the quality of life of those living with a history ofcancer. Initially, the OCS achieved this goal by fo-cusing on the support and direction of researchdesigned to identify and prevent or control ad-verse cancer- and treatment-related outcomes(such as pain, lymphedema, sexual dysfunction,second cancers, and poor quality of life). Becauseso few studies in this earlier period followed survi-vors much beyond 2 years post-treatment, a sec-ondary mission of the OCS was to encourageresearch among long-term cancer survivors, thosealready 5 or more years post-diagnosis. However,it quickly became apparent that knowledge ofthe long-term and late effects of cancer and howto mitigate these was only part of the challengeof survivorship. To be effective, this informationhad to be coupled with an understanding of howbest to provide surveillance and follow-up care tocancer survivors and communicate with themabout future risks, so as to decrease morbidityand mortality and optimize health after cancertreatment. Research addressing these latter setsof questions form a special and expanding corecomponent of the science nurtured by the OCS.
There is growing evidence that in the past de-cade, cancer survivorship has ‘‘come of age’’ bothas a topic of research and as a specialized focusof clinical care. Intensification of interest in thehealth and well-being of survivors who are post-treatment for their cancer is reflected in the pub-lication in the past 5 years alone of an equal num-ber of major reports addressing the research inthis area.1-5 Since the appearance of the earlierSeminars in Oncology Nursing special issue in2001, other major non-cancer as well as cancerscientific journals, including the Journal of Pedi-
atric Psychology, American Journal of Nursing,and the Journal of Clinical Oncology, have de-voted special issues to this aspect of the cancercontrol continuum.6-8 New texts have appearedsummarizing our accomplishments in the field ofsurvivorship research and promoting evidence-based care,9,10 and there is even a new scientificjournal to feature this burgeoning area of sci-ence.11 At the same time, personal accounts ofsurvivors’ experiences of living through and be-yond their illness now routinely capture the pub-lic’s attention. Nurses have been in the front
lines watching, studying, and striving to accom-modate the evolving demands of survivors’ post-treatment care. They are often witness to theneeds, as well as hopes and dreams, of those forwhom they care. In the remainder of this article,the implications of the changing face of cancersurvivors and the survivorship experience forhealth promotion are explored. Based on this, rec-ommendations are made regarding where survi-vorship research and survivors’ care need tofocus in the future if we are to realize the publicmandate envisioned for the OCS to improve qual-ity of life hand-in-hand with length of survival forall those diagnosed with cancer.
HEALTH PROMOTION: WHAT ROLE DOES IT
HAVE IN SURVIVORS’ CARE?
T here are seven compelling reasons whyhealth promotion has become one of the
most rapidly expanding topics of interest in thebroader arena of survivorship research. All ofthese mirror the changing demography or ‘face’of cancer survivors and their associated survivor-ship experience as we race into the 21st century.First, and most obvious, is the growing populationof cancer survivors. Currently estimated as includ-ing over 10.8 million individuals in the UnitedStates alone,12 the number of cancer survivors isexpected to continue to increase in the decadesto come, as advances in early detection, therapy,and supportive care diffuse into the community.Fewer deaths from cardiovascular disease, andcritically, the aging of the population will contrib-ute to this trend. Today’s prevalence figure repre-sents a three-fold increase from the 3 millionestimate calculated for 1971, when PresidentNixon signed the National Cancer Act into law.In recent years, cancer prevalence has increasedat a rate of approximately 3% per year, and survi-vors now represent 3.6% of the population. 13
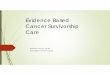
Breast cancer survivors have historically and con-tinue to represent the largest segment of the survi-vor population (23%), followed by prostate cancersurvivors (19%) and colorectal cancer survivors(10%) (Fig 1). Among female survivors, cancersof the breast (42%), corpus and uterus (10%), andcolon and rectum (9%) account for almost twothirds (61%) of prevalent cases. Cancers of theprostate (41%), colon and rectum (11%), and he-matologic sites (9%) comprise the majority ofprevalent cases in male survivors.13

RETHINKING THE CANCER CONTROL CONTINUUM 147
A second reason to be concerned about thehealth of cancer survivors is that most of these in-dividuals can expect to live long term with a cancerhistory. In the past, concern about late health con-sequences of being treated for cancer was a relativeluxury. Few people survived long enough for theserisks to become a problem; the focus of care waslargely on helping those diagnosed with cancerto die of their disease, not live with it. Today, deal-ing with the human cost of survival has becomewhat might be viewed as a ‘high-end problem.’The good news is that survivors are living longterm; the bad news is that they are living longenough to be troubled by the persistent and lateconsequences of their illness and its treatment.The associated shift in the conceptualization ofcancer away from being a largely fatal illness toone that is now curable for some, and a chroniccondition for many more, demands that the healthcare community find ways to help survivors pre-vent, control, or mitigate the negative effects ofsurviving cancer.
In the absence of other competing causes, sur-vival estimates for adults diagnosed with cancertoday indicate that 66% can expect to be alive in5 years. These figures are even higher for thosediagnosed as children (less than 19 years of age)where 5-year survival is approaching 80% and10-year survival is close to 75%.12 More womenthan men become long-term survivors (> 5 years).This is due to higher proportions of women havingmore easily diagnosed and controlled cancers
Estimated Number of Persons Alive in the U.S. Diagnosed with
Cancer on January 1,2004 by Site (N = 10.8 M)
Other
15%
Urinary Tract
(Bladder, Kidney,
Renal Pelvis)
7%
Female Breast
23%
Prostate
19%
Colorectal
10%
Gynecologic
9%
Hematologic
(HD,NHL,Leukemia,
ALL, Myeloma)
8%
Melanoma
6%
Lung and
Bronchus
3%
FIGURE 1. Estimated number of persons alive in theUnited States diagnosed with cancer by cancer site (inva-sive/first primary cases only, N ¼ 10.8 million).
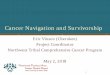
(eg, breast and gynecologic), lower incidence andmortality from lung cancer, and generally lowerall-cause mortality rates among women as com-pared with men in the United States (Fig 2).
A third reason that greater attention must be di-rected to health promotion among survivors isthat these individuals tend to be older and at riskfor competing co-morbid conditions that may becomplicated by cancer. With improvements inthe delivery of quality cancer care, our survivorpopulation of all ages is also getting older, becom-ing at risk for developing subsequent complicatinghealth conditions, including other cancers. Age isthe single most important risk factor for develop-ing cancer. This is why, with the aging of the pop-ulation, in particular that of the ‘baby boom’generation (those born between the years 1946and 1964), we can expect the numbers of survi-vors to rapidly increase over the next severalyears.14
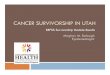
Currently, 60% of all incident malignancies inthe United States occur in adults over the age of65, and 16% of those over 65 have a history ofcancer.13 An estimated 6.5 million of the 10.8million cancer survivors are 65 years of age orolder, with the ‘‘oldest old’’ (those 85 and older)accounting for 15% of this 6.5 million (Fig 3).Forty-three percent of the 6.5 million older menand women were more than 10-year survivorsof their disease; 17% had survived more than 20years beyond their initial diagnosis.13 The experi-ence of cancer among older adult survivors is of-ten superimposed on existing health conditions,such as heart disease, arthritis, diabetes, andvarious geriatric syndromes that affect the el-derly.15-17 These co-existing medical conditionscan complicate delivery of optimal therapy, andimportantly, have the potential to downstreamhealth and well-being. In one large population-
0.0
0.5
1.0
1.5
2.0
2.5
0 to <5 5 to 10 10 to<15 15 to<20 20 to<25 25
Years from Diagnosis
Peo
ple in
m
illio
ns
Males
Females
<
FIGURE 2. Estimated number of persons alive in theUnited States diagnoses with cancer on January 1, 2004by time from diagnosis and gender (invasive/first primarycases only, N ¼ 10.8 million).

148 J.H. ROWLAND
based study, older cancer patients were found to bein poorer health (34% vs 10% of the general popula-tion), were more likely to have two or more chronicmedical conditions (16% vs 4%), report signifi-cantly more functional limitations (70% vs<30%), and experience greater limitations inactivities of daily living (eg, bathing, dressing,eating) and instrumental activities of daily living(eg, cooking, cleaning house, shopping) (17% vs3%).18 Not surprisingly, the interface between agingand cancer has itself become a major focus ofinquiry.19-22
The fourth reason to focus on health promotionis that cancer, together with the multi-modal ther-apies used to treat and control it, have the capac-ity to compromise health in a host of domains.Indeed, the most important lesson learned fromthe growing and increasingly sophisticated bodyof survivorship studies (a finding articulated dailyin clinics across the country by survivors them-selves) is that being told you are cancer-free isnot the same as being free of your disease. Cancerhas the potential to affect virtually every aspect ofa survivor’s life: physical, emotional, cognitive, so-cial, and/or financial. To date, the physical ormedically related spectrum of these remain themost extensively documented.23-25 Some effectsare acute or transient (eg, hair loss, anemia, nau-sea), others can persist over time and result inchronic or long-term problems (eg, fatigue, pain,problems with memory and concentration, sexualdysfunction, fear of recurrence), and still othersmay not appear for months or years after theend of therapy, resulting in late-occurring compli-cations (eg, cardiac dysfunction, osteoporosis,second malignancies, infertility).
30-39 Years
4%
40-49 Years
8%
70+ Years
50%
60-69 Years
22%
50-59 Years
16%
20-29 Years
1%
0-19 Years
1%
FIGURE 3. Estimated number of persons alive in theUnited States diagnosed with cancer by current age (inva-sive/first primary cases only, N ¼ 10.8 million).
It is already estimated that over 750,000 of to-day’s cancer survivors have a history of two ormore cancers; three quarters of these affectingsites different from the original malignancy.26
With survivors living longer, it can be expectedthat more will develop multiple cancers. Some ofthese will be iatrogenic in nature or secondary totreatments received, while others will be linkedto the original cancer by genes, behavior (eg,smoking, poor diet, alcohol use), or toxic expo-sures. The majority, however, will simply be dueto aging.27 Thus, ensuring that survivors are rou-tinely screened for cancers for which they maybe at increased risk by virtue of therapy (eg, breastcancer among female survivors of Hodgkin’s dis-ease exposed to mantle radiation) or getting older(eg, colorectal cancer screening in those over theage of 50) is becoming increasingly important.Fortunately, information to date suggests thatage-appropriate cancer screening appears to beoccurring for most older survivors,28 althoughwho is best equipped to provide this care remainsa topic of debate.29-31
What we know about cancer’s long-term andlate effects is that: 1) they can affect survivorsof all ages, young and old; 2) some survivorshave few effects while others experience many;3) there may be long latencies in the develop-ment of some effects; 4) degree of risk to individ-ual patients is often difficult to predict; and 5)adverse sequelae contribute to the individual,family, and societal burden of illness. While sec-ond (or recurrent) malignancies are often citedas the greatest source of concern to most survi-vors as well as many clinicians, other disablingconditions occur and need to be monitored forand addressed. Some research suggests thatcompeting health conditions (including diabetes,stroke, heart disease), whether cancer-related,pre-existing, or developing over time, may bemore life-threatening than the cancer itself.32
Importantly, interventions to limit or treat theseconditions have the potential to reduce deathand morbidity related to cancer. This is thefifth reason to attend to post-treatment healthpromotion.
A growing body of research is examining the rolethat lifestyle and behavior change have in improv-ing the health and function of cancer survivors ofall ages.33,34 In fiscal year 2006, a total of 21 ofthe 86 intervention studies (24%) being conductedamong post-treatment survivors and funded by theNational Institutes of Health had a health

RETHINKING THE CANCER CONTROL CONTINUUM 149
promotion target or component. Interest in phys-ical activity in particular has been spurred bystudies, several led by nursing research teams,demonstrating its beneficial effects on survivors’emotional and functional well-being,35-37 and pro-vocative data from three observational studiessuggesting a survival benefit among cancer survi-vors who have a prior history of being or remainmoderately physically active after cancer.38-40
The greatest source of inspiration for this work,however, has been survivors themselves. Eagerto take control of their lives again, many survivorsuse physical activity as a means to improve bodyimage, combat depression and fatigue, and to re-gain a sense of general well-being. When asked,most indicate interest in learning more aboutthese and other types of interventions that are ac-cessible, can be individually tailored, and do notinvolve taking more drugs.41-43 The ever louderdemand by survivors for help in decreasing can-cer’s morbidity and reducing risk of mortality isthe sixth driving force behind the growing interestin health promotion efforts.
The seventh and final reason to championhealth promotion among cancer survivors isbecause cancer may well represent a ‘‘teachablemoment’’ for many of those diagnosed.44 Life-threatening illness has the capacity to profoundlyaffect personal world views, in particular the indi-vidual’s relationship with mortality. For oncologypractitioners, this may create a window of oppor-tunity in which to intervene, to help patients iden-tify behaviors that put them at risk for poor healthoutcomes (eg, smoking, lack of exercise, poor die-tary patterns, sun exposure), and provide themwith the support required to make and adhere todesired lifestyle modifications.45 While theremay be no guarantee that such changes will altercancer outcomes, the probability that if sustainedthey will lead to improved emotional and func-tional health and potentially reduce other morbidconditions (eg, cardiovascular disease, bone loss,diabetes) is significant.
CHAMPIONING CANCER SURVIVORS’ HEALTH:
WHERE DO WE GO FROM HERE?
T here are a number of challenges facing the on-cology research and clinical community if we
are to successfully act on our current knowledge ofthe benefits and approaches to health promotionamong cancer survivors, and engage cancer survi-
vors themselves in efforts to partner with theirhealth care team to optimize their long-termhealth outcomes. Chief among these is ensuringa continuing flow of researchers and clinicians de-voted to studying and caring for our growing pop-ulation of cancer survivors. The current andprojected shortage of not only oncologists, butcritically of oncology nurses, is already strainingour capacity to meet this demand. The past 4years have witnessed declining budgets acrossthe National Institutes of Health. Unless reversed,this trend will further erode our capacity to sup-port the research necessary to keep pace withchanges in cancer care and outcomes by restrict-ing the flow of clinical investigators entering thefield of survivorship research. In addition to sus-taining these vital professional and academic sup-ply lines, there are a set of specific scientific areaswhere, based on previously described gaps in cur-rent funding,46,47 and what has been identified as
needed research in a number of the national survi-vorship reports cited earlier,1-5 we need to direct
our efforts to champion cancer survivors’ health.These include:
1) Understanding the health impact of cancer onolder adults, and normal aging on cancer survi-
vors’ health. Despite the fact that they areamong the fastest growing segment of the pop-
ulation, already representing more than half(60%) of today’s survivors (Fig 3), and will pop-
ulate ever larger proportions of future survivorcohorts, survivors age 65 and older remain
a neglected group in the survivorship litera-ture. Of the 251 grants funded in 2006, only
23 (less than 10%) specifically targeted survi-
vors aged 65 or older. At the same time, weneed more research on the interaction of can-
cer and aging (among both pediatric and child-hood cancer survivors) to understand who
may be at risk for what types of late cancer-re-lated complications, which underlying or fu-
ture co-morbid conditions may be adverselyaffected after a cancer diagnosis, and which
conditions are uniquely attributable to cancerversus normal aging. Understanding the con-
straints imposed by aging on health promotionefforts will also be important.48
2) Developing tools to permit us to describe thesurvivorship experience, including the occur-rence and evolution of co-morbid conditions.
A number of well-developed tools now exist todescribe the impact of cancer diagnosis and

150 J.H. ROWLAND
treatment on individuals’ health-related qual-
ity of life,49 several of these generated by
nurse researchers.50-52 However, as survivors
live longer and age, new instruments are
needed that will enable us to both more accu-
rately describe the late effects of treatment
and also compare the well-being of those liv-
ing with a history of cancer to that of their
similarly aging peers without such a history.53
In particular, we will need access to standard-
ized and well-validated tools that allow us to
capture easily and early in the course of
care information on conditions that in some
cases may predate cancer onset, and track
this over time.3) Examining models of post-treatment care.
Research is already beginning to inform us
about the impact of cancer on work, economicstatus, and insurability. All of this is importantas survivors’ status with regard to these do-mains has major implications for their accessto and use of health-related services. However,efforts to understand the impact that patternsof follow-up care have on survivors’ health sta-tus, morbidity, and mortality are still very lim-ited.2,54 Devising strategies to compare thecosts and benefits of different models of deliv-ering post-treatment care to survivors, andspecifically the role of health promotion activ-ities in these settings, will be a significant issueas we look to the future. A key question for thiswork will be what can and indeed should be therole of nurses in the delivery of such care. Atthe same time, we need to have a clearer un-derstanding of the cost of delivery of many ofthe behavioral and lifestyle interventions thatare found to improve quality of life and func-tion of survivors post-treatment. Because thistype of health services research adds signifi-cantly to the expense of conducting a typicalpsychosocial or behavioral intervention study,the number of projects incorporating this datais limited.55
4) Understanding the impact of cancer on thehealth of the family. Although the advocacycommunity, along with the National CancerInstitute’s OCS, views caregivers as includedin the definition of ‘cancer survivors’ (http://dccps.nci.nih.gov/ocs), we are only justbeginning to appreciate the impact cancerhas on the functioning and well-being of themillions of family members affected by this
illness. It is well known that social supportis an important buffer to negative healthoutcomes.56-58 It also well established thatfor individuals to successfully adopt andmaintain major lifestyle changes (eg, smokingcessation, dietary practices), enlisting thesupport of key family members at home ineffectuating these may be critical.59,60 Re-search is already beginning to show thatintervening with cancer caregivers may im-prove not only patients’ but also caregivers’health outcomes.61-63
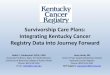
In summary, rapid advances in our ability to de-tect, treat, and control cancer have turned theseonce almost uniformly fatal illnesses into condi-tions that can be cured in some cases and con-trolled or managed as a chronic disease in manyothers. The consequence is that cancer survivorscan no longer be viewed as moving along an inexo-rable, unilinear trajectory toward a predictablecancer death. Rather, care of those with a cancerhistory must embrace a new, circular cancer-con-trol model. One in which survivors who are post-treatment are seen as beginning a new phase ofcare where the focus is on treating current lingeringeffects of illness, preventing where possible(or finding early and controlling when not), late ad-verse effects, and promoting best possible health(Fig 4). Nurses have traditionally been vital cham-pions for a holistic or ‘whole person’ approach tocancer care. Thus, they are uniquely positionedto play a central role in ensuring that we deliveron the promise of a valued future life for each can-cer survivor and family member alive today, andthose who will become survivors tomorrow.
End of life
Prevention
Detection
Survivorship
Treatment
Diagnosis
FIGURE 4. Cancer Control Continuum – Revisited. (Re-printed with permission.64

RETHINKING THE CANCER CONTROL CONTINUUM 151
REFERENCES
1. Hewitt M, Weiner SL, Simone JV. Childhood cancer survi-
vorship: improving care and quality of life. Washington, DC:
The National Academies Press; 2003.
2. Hewitt M, Greenfield S, Stovall E. From cancer patient to
cancer survivor: lost in transition. Washington, DC: Institute
of Medicine and National Research Council of the National
Academies; 2006.
3. Lance Armstrong Foundation. Centers for Disease Control
and Prevention. A national action plan for cancer survivorship:
advancing public health strategies. Atlanta, GA: U.S. Depart-
ment of Health and Human Services, Center for Disease Control
and Prevention; 2004.
4. President’s Cancer Panel. Living beyond cancer: finding
a new balance. Bethesda, MD: National Cancer Institute; 2004.
5. President’s Cancer Panel. Assessing progress, advancing
change. Bethesda, MD: National Cancer Institute; 2005.
6. Rowland JH. Foreward: looking beyond cure: pediatric
cancer as a model. J Pediatr Psychol 2005;30:1-3.
7. Rowland JH, Hewitt M, Ganz PA. Cancer survivorship:
a new challenge in delivering quality cancer care. J Clin Oncol
2006;24:5101-5104.
8. Aziz NM. Foreward: nursing and cancer survivorship. AJN
2006;106(suppl):3.
9. Feuerstein M. Handbook of cancer survivorship. New York:
Springer; 2007.
10. Ganz PA. Cancer survivorship: today and tomorrow. New
York: Springer; 2007.
11. Feuerstein M. Optimizing cancer survivorship. J Cancer
Survivorship 2007;1:1-4.
12. Espey DK, Wu XC, Swan J, et al. Annual report to the na-
tion on the status of cancer, 1975-2004, featuring cancer in
American Indians and Alaska natives. Cancer 2007;110:2119-
2152.
13. Surveillance, Epidemiology, and End Results (SEER)
Program. Prevalence database: US Estimated Complete
Prevalence Counts on 1/1/2004. National Cancer Institute,
DCCPS, Surveillance Research Program, Statistical Research
and Applications Branch, released April 2007, based on the
November 2006 SEER data submission. Available at:
www.seer.cancer.gov.
14. Edwards BK, Howe HL, Ries LAG, et al. Annual report to
the nation on the status of cancer, 1973-1999, featuring impli-
cations of age and aging on U.S. cancer burden. Cancer 2002;
94:2766-2792.
15. Extermann M. Interaction between comorbidity and can-
cer. Cancer Control 2007;14:13-22.
16. Balducci L. Aging, frailty, and chemotherapy. Cancer
Control 2007;14:7-12.
17. Hurria A. Clinical trials in older adults with cancer: past
and future. Oncology 2007;21:351-358.
18. Hewitt M, Rowland JH, Yancik R. Cancer survivors in the
United States: age, health, and disability. J Gerontol A Biol Sci
Med Sci 2003;58:82-91.
19. Institute of Medicine. Cancer in elderly people: Work-
shop proceedings. Washington, DC: The National Academies
Press; 2007.
20. Lichtman SM, Balducci L, Aapro M. Geriatric oncology:
a field coming of age. J Clin Oncol 2007;25:1821-1823.
21. Rao AV, Demark-Wahnefried W. The older cancer survi-
vor. Crit Rev Oncol Hematol 2006;60:131-143.
22. Bellizzi KM, Rowland JH. The role of comorbidity,
symptoms and age in the health of older survivors following
treatment for cancer. Aging Health 2007;3:625-635.
23. Aziz NM. Long-term survivorship: late effects. In:
Berger AM, Portenoy RK, Weissman DE, eds. Principles and
practice of palliative care and supportive oncology. Philadel-
phia, PA: Lippincott Williams & Wilkins; 2002; pp. 1019-1033.
24. Oeffinger KC, Mertens AC, Sklar CA, et al. Chronic health
conditions in survivors of childhood cancer. N Engl J Med 2006;
355:1572-1582.
25. Stein K, Andrykowski M, Syrjala K. Physical and psycho-
logical long-term and late effects of cancer. Cancer 2008;
112(Suppl 11):2577-2592.
26. Mariotto AB, Rowland JH, Ries LAG, et al. Multiple can-
cer prevalence: a growing challenge in long-term survivorship.
Cancer Epidemiol Biomarkers Prev 2007;16:566-571.
27. Hayat MJ, Howlader N, Reichman ME, et al. Cancer statis-
tics, trends, and multiple primary cancer analyses from the
Surveillance, Epidemiology, and End Results (SEER) Program.
The Oncologist 2007;12:1-20.
28. Bellizzi KM, Rowland JH, Jeffery DD, et al. Health behav-
iors of cancer survivors: examining opportunities for cancer
control intervention. J Clin Oncol 2005;23:8884-8893.
29. Etim AE, Schellhase KG, Sparapani R, et al. Effect of
model of care delivery on mammography use among elderly
breast cancer survivors. Breast Cancer Res Treat 2006;96:
293-299.
30. Oeffinger KC, McCabe MS. Models for delivering survivor-
ship care. J Clin Oncol 2006;24:5117-5124.
31. Ko C, Chaudhry S. The need for a multidisciplinary
approach to cancer care. J Surg Res 2002;105:51-57.
32. Brown BW, Brauner C, Minnotte MC. Non cancer deaths
in white adult cancer patients. J Natl Cancer Inst 1993;85:979-
987.
33. Demark-Wahnefried W, Pinto BM, Gritz ER. Promoting
health and physical function among cancer survivors: potential
for prevention and questions that remain. J Clin Oncol 2006;24:
5125-5131.
34. Alfano CM, Rowland JH. Recovery issues in cancer survi-
vorship: a new challenge for supportive care. Cancer J 2006;12:
432-443.
35. Schwartz AL. Physical activity after a cancer diagnosis:
psychosocial outcomes. Cancer Invest 2004;22:82-92.
36. McTiernan A. Physical activity after cancer: physiologic
outcomes. Cancer Invest 2004;22:68-81.
37. Oldervoll LM, Kaasa S, Hjermstad MJ, et al. Physical exer-
cise results in the improved subjective well-being of a few or is
effective rehabilitation for all cancer patients? Eur J Cancer
2004;40:951-962.
38. Holmes MD, Chen WY, Feskanich D, et al. Physical activ-
ity and survival after breast cancer. JAMA 2005;293:2479-2486.
39. Meyerhardt JA, Giovannucci EL, Holmes MD, et al. Phys-
ical activity and survival after colorectal cancer diagnosis. J Clin
Oncol 2006;24:3527-3534.
40. Meyerhardt JA, Hesletine D, Niedzwiecki D, et al. Impact
of physical activity on cancer recurrence and survival in
patients with stage III colon cancer: findings from CALGB
89803. J Clin Oncol 2006;24:3535-3541.
41. Demark-Wahnefried W, Peterson B, McBride C, et al.
Current health behaviors and readiness to pursue life-style

152 J.H. ROWLAND
changes among men and women diagnosed with early stage
prostate and breast carcinomas. Cancer 2000;88:674-684.
42. Ganz PA, Desmond KA, Leedham B, et al. Quality of life in
long-term, disease-free survivors of breast cancer: a follow-up
study. J Natl Cancer Inst 2002;94:39-49.
43. Patterson RE, Neuhouser ML, Hedderson MM, et al.
Changes in diet, physical activity, and supplement use among
adults diagnosed with cancer. J Am Diet Assoc 2003;103:323-
328.
44. Demark-Wahnefried W, Aziz NM, Rowland JH, et al. Rid-
ing the crest of the teachable moment: promoting long-term
health after the diagnosis of cancer. J Clin Oncol 2005;23:
5814-5830.
45. Ganz PA. A teachable moment for oncologists: cancer
survivors 10 million and growing. J Clin Oncol 2005;23:5458-
5460.
46. Rowland JH. Survivorship research: past, present and
future. In: Ganz PA, ed. Cancer survivorship: today and tomor-
row. New York: Springer; 2007: pp. 28-42.
47. Aziz NM, Rowland JH. Trends and advances in cancer
survivorship research: challenge and opportunity. Semin
Radiat Oncol 2003;13:248-266.
48. Deimling GT, Sterns S, Bowman KF, et al. Functioning
and activity participation restrictions among older adult, long-
term cancer survivors. Cancer Invest 2007;25:106-116.
49. Lipscomb J, Gotay CC, Snyder DF. Patient-reported out-
comes in cancer: a review of recent research and policy initia-
tives. CA Cancer J Clin 2007;57:278-300.
50. Ferrans CE, Powers MJ. Psychometric assessment of the
Quality of Life Index. Res Nurs Health 1992;15:29-38.
51. Ferrell B, Dow KH, Grant M. Measurement of the quality
of life in cancer survivors. Qual Life Res 1995;4:523-531.
52. Hinds PS, Burghen EA, Haase JE, et al. Advances in defin-
ing, conceptualizing, and measuring quality of life in pediatric
patients with cancer. Oncol Nurs Forum 2006;33(suppl):23-29.
53. Fitzsimmons D. What are we trying to measure? Rethink-
ing approaches to health outcome assessment for the older
person with cancer. Eur J Cancer Care 2004;13:416-423.
54. Implementing survivorship care planning. Workshop
summary. Washington, DC: The National Academies Press;
2007.
55. Carlson LE, Bultz BD. Benefits of psychosocial oncology
care: improved quality of life and medical cost offset. Health
Qual Life Outcomes 2003;17:1-8.
56. Cohen S. Psychosocial models of the role of social
support in the etiology of physical disease. Health Psychol
1988;7:269-297.
57. Wortman CB. Social support and the cancer patient.
Conceptual and methodologic issues. Cancer 1984;53(suppl):
2339-2362.
58. Kroenke CH, Kubzansky LD, Schernhammer ES, et al.
Social networks, social support and survival after breast cancer
diagnosis. J Clin Oncol 2006;24:1105-1111.
59. Niederhauser VP, Arnold M. Assess health risk status for
intervention and risk reduction. Nurse Pract 2004;29:35-42.
60. Humpel N, Magee C, Jones SC. The impact of a cancer
diagnosis on the health behaviors of cancer survivors and their
family and friends. Support Care Cancer 2007;15:621-630.
61. Northouse LL, Mood DW, Schafenacker A, et al. Random-
ized clinical trial of a family intervention for prostate cancer
patients and their spouses. Cancer 2007;110:2809-2818.
62. Northouse LL. Helping families of patients with cancer.
Oncol Nurs Forum 2005;32:743-750.
63. Kurtz ME, Kurtz JC, Given CW, et al. Depression and
physical health among family caregivers of geriatric patients
with cancer: a longitudinal view. Med Sci Monit 2004;10:
CR447-CR456.
64. Rowland JH, Bellizzi K. Cancer survivors and survivor-
ship research: a reflection on today’s successes and tomorrow’s
challenges. Hematol Oncol Clin North Am 2008;22:181-200.