Embed Size (px)
DESCRIPTION
tumor kuli
Citation preview

TUMOR KULITTUMOR KULIT
neoplasmaneoplasma 22
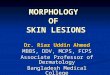
EpidermisEpidermis

neoplasmaneoplasma 33
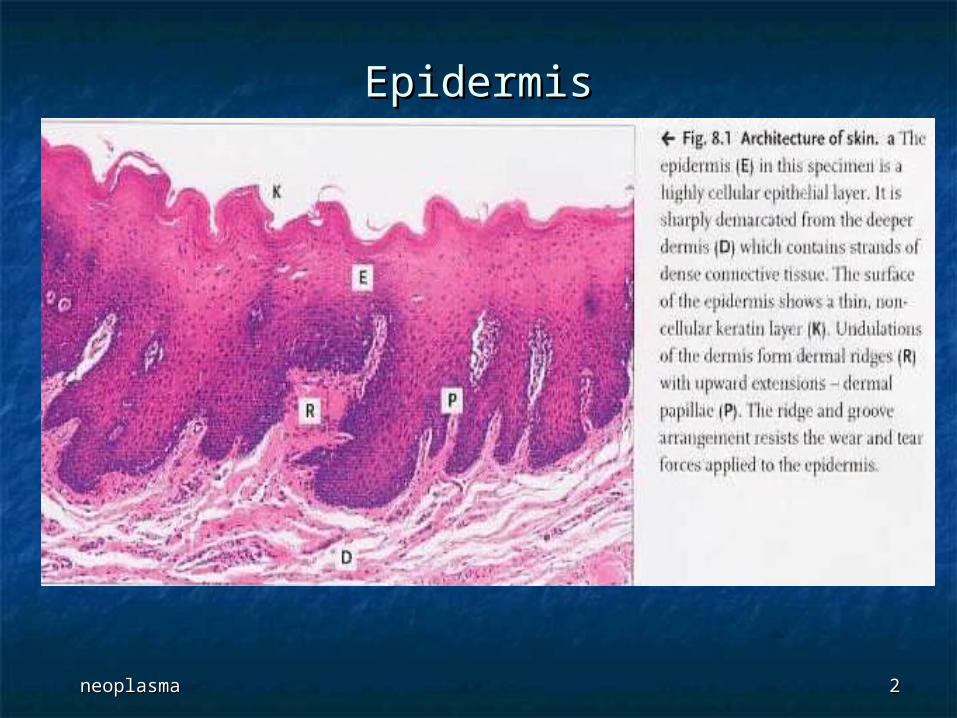
EpidermisEpidermis
neoplasmaneoplasma 44
EpidermisEpidermis
BENIGN SQUAMOUS BENIGN SQUAMOUS KERATOSISKERATOSIS

neoplasmaneoplasma 66
SEBORRHEIC KERATOSISSEBORRHEIC KERATOSIS
neoplasmaneoplasma 88
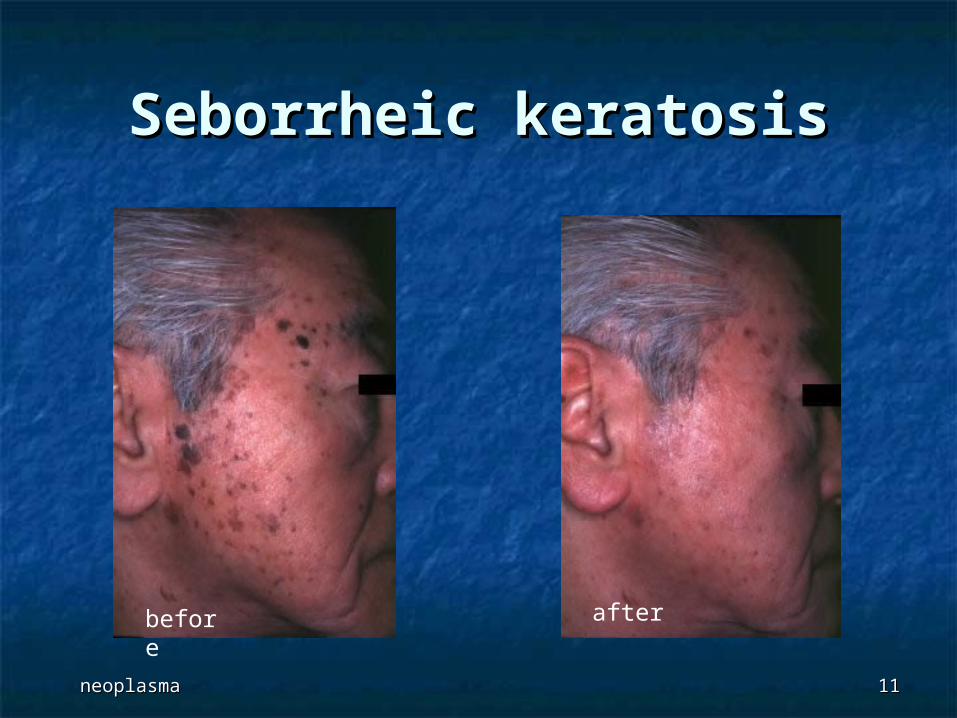
A seborrheic keratosis is one of the most A seborrheic keratosis is one of the most common growths that occur on the skin. In common growths that occur on the skin. In general terms these are often referred to as general terms these are often referred to as "barnacles of time or age spots" I prefer to "barnacles of time or age spots" I prefer to call them “wisdom spots”. call them “wisdom spots”.
Seborrheic keratoses are most frequently Seborrheic keratoses are most frequently seen in adults over thirty, and they can seen in adults over thirty, and they can occur almost anywhere on the skin. occur almost anywhere on the skin. Looking a lot like waxy lumps they are Looking a lot like waxy lumps they are typically brown or black in color, and typically brown or black in color, and appear like they have been stuck on the appear like they have been stuck on the skin. When they are very flat they can look skin. When they are very flat they can look like large “liver spots”/lentigolike large “liver spots”/lentigo
Seborrheic keratosisSeborrheic keratosis
neoplasmaneoplasma 99
Seborrheic keratosisSeborrheic keratosis Common; usually age 40+ yearsCommon; usually age 40+ years Benign, although may coexist with malignancyBenign, although may coexist with malignancy Usually affects trunk, head and neck, Usually affects trunk, head and neck,
extremities; only hair bearing skinextremities; only hair bearing skin Not HPV related, although HPV present in Not HPV related, although HPV present in
morphologically similar cases of morphologically similar cases of epidermodysplasia verruciformis and bowenoid epidermodysplasia verruciformis and bowenoid changeschanges
Dermatosis papulosa nigra:Dermatosis papulosa nigra: in blacks in blacks Leser-Trelat sign:Leser-Trelat sign: sudden appearance or sudden appearance or
increase in number and size of seborrheic increase in number and size of seborrheic keratoses, associated with internal malignancykeratoses, associated with internal malignancy
neoplasmaneoplasma 1010
Treatment:Treatment: superficial curettage, superficial curettage, freezingfreezing
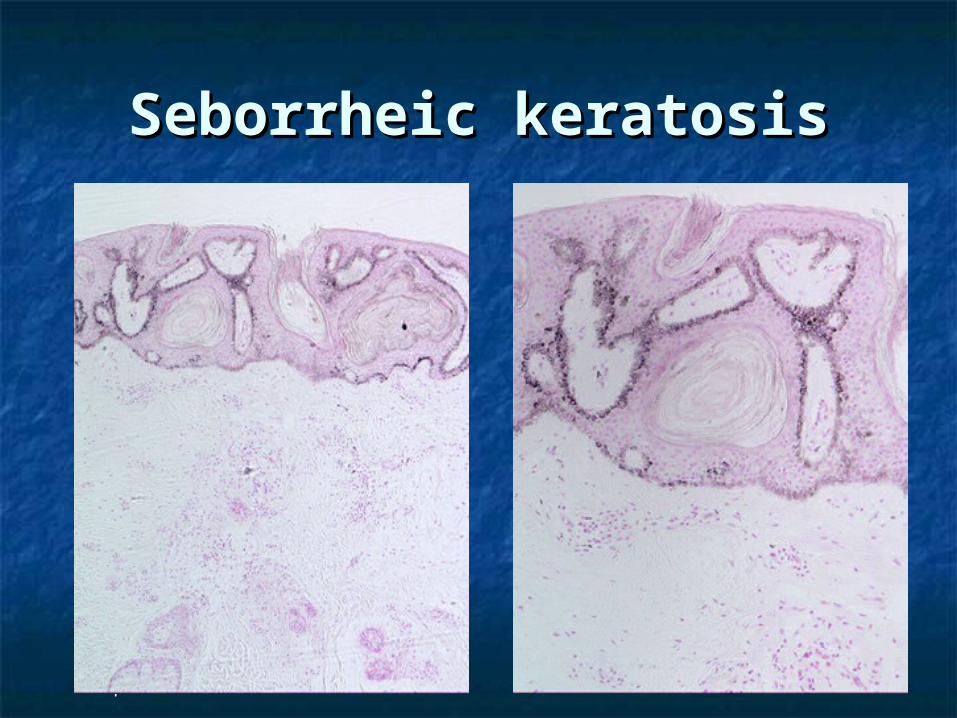
Gross:Gross: exophytic, sharply demarcated, exophytic, sharply demarcated, pigmented lesions that protrude above pigmented lesions that protrude above surface of skin, appear to be stuck to surface of skin, appear to be stuck to skin, single or multiple, soft, tan-blackskin, single or multiple, soft, tan-black
Micro:Micro: basal keratinocyte proliferations basal keratinocyte proliferations
Seborrheic keratosisSeborrheic keratosis
neoplasmaneoplasma 1111
before after
Seborrheic keratosisSeborrheic keratosis

neoplasmaneoplasma 1212
Seborrheic Seborrheic keratosiskeratosis
neoplasmaneoplasma 1313
Seborrheic keratosisSeborrheic keratosis

ACTINIC KERATOSISACTINIC KERATOSIS
neoplasmaneoplasma 1515
Actinic keratosisActinic keratosis
Also called solar keratosis, senile Also called solar keratosis, senile keratosiskeratosis
Buildup of excessive keratin due to Buildup of excessive keratin due to chronic exposure to sunlightchronic exposure to sunlight
On sun-exposed sites (face, arms, On sun-exposed sites (face, arms, dorsum of hands)dorsum of hands)
Called actinic cheilitis in lipsCalled actinic cheilitis in lips May become invasive with only a May become invasive with only a
single layer of atypical keratinocytessingle layer of atypical keratinocytes
neoplasmaneoplasma 1616
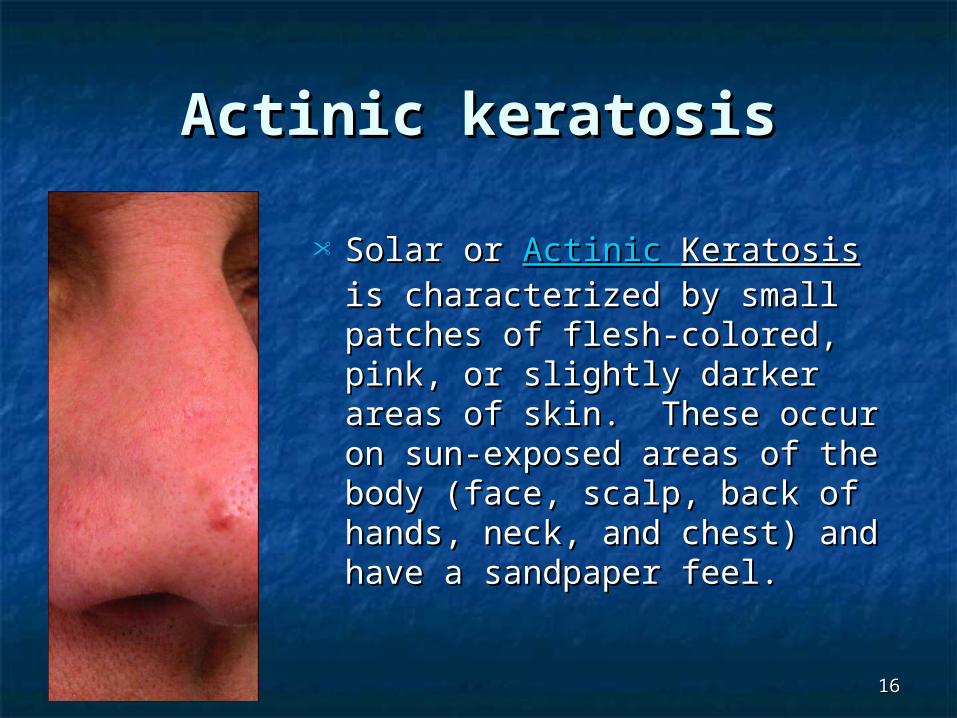
Solar or Solar or Actinic Actinic KeratosisKeratosis is is characterized by small characterized by small patches of flesh-colored, patches of flesh-colored, pink, or slightly darker areas pink, or slightly darker areas of skin. These occur on sun-of skin. These occur on sun-exposed areas of the body exposed areas of the body (face, scalp, back of hands, (face, scalp, back of hands, neck, and chest) and have a neck, and chest) and have a sandpaper feel. sandpaper feel.
Actinic keratosisActinic keratosis
neoplasmaneoplasma 1717
Risk factors:Risk factors: fair skin, fair skin, ionizing radiation, ionizing radiation, hydrocarbon or arsenic exposure, hydrocarbon or arsenic exposure, renal transplantrenal transplant
Treatment:Treatment: curettage, curettage, cryotherapy, cryotherapy, topical chemotherapeutic agentstopical chemotherapeutic agents
Gross:Gross: tan-brown, red or skin colored, tan-brown, red or skin colored, circumscribed lesions, sandpaper texture, circumscribed lesions, sandpaper texture, may have cutaneous horn (due to may have cutaneous horn (due to excessive production of parakeratotic scale)excessive production of parakeratotic scale)
Actinic keratosisActinic keratosis

neoplasmaneoplasma 1818
Actinic keratosisActinic keratosis

neoplasmaneoplasma 1919
Actinic keratosisActinic keratosis
neoplasmaneoplasma 2020
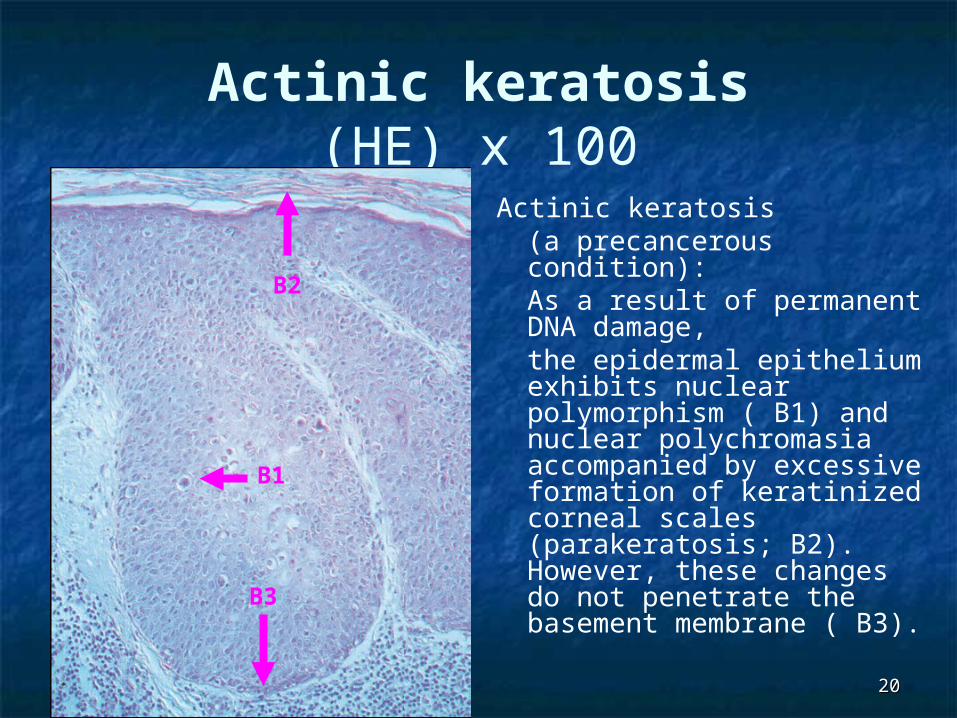
Actinic keratosis(HE) x 100
Actinic keratosis (a precancerous condition): As a result of permanent DNA damage,the epidermal epithelium exhibits nuclear polymorphism ( B1) and nuclear polychromasia accompanied by excessive formation of keratinized corneal scales (parakeratosis; B2). However, these changes do not penetrate the basement membrane ( B3).
B1
B2
B3
FIBROEPITHELIAL POLYPFIBROEPITHELIAL POLYP
neoplasmaneoplasma 2222
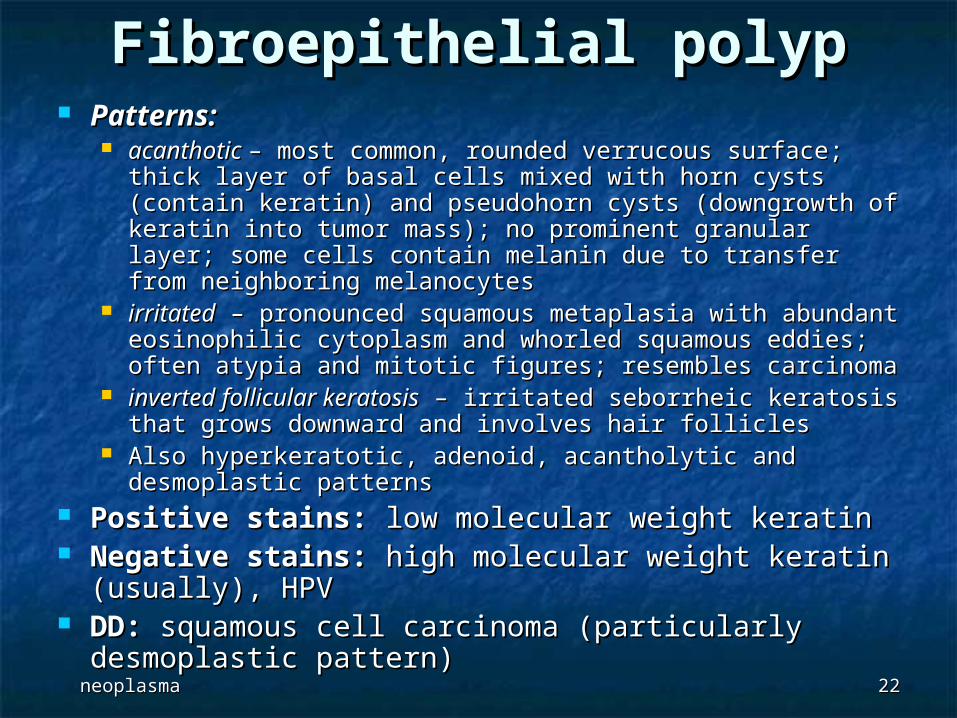
Patterns:Patterns: acanthotic acanthotic – most common, rounded verrucous surface; – most common, rounded verrucous surface;
thick layer of basal cells mixed with horn cysts (contain thick layer of basal cells mixed with horn cysts (contain keratin) and pseudohorn cysts (downgrowth of keratin into keratin) and pseudohorn cysts (downgrowth of keratin into tumor mass); no prominent granular layer; some cells tumor mass); no prominent granular layer; some cells contain melanin due to transfer from neighboring contain melanin due to transfer from neighboring melanocytesmelanocytes
irritatedirritated – pronounced squamous metaplasia with – pronounced squamous metaplasia with abundant eosinophilic cytoplasm and whorled squamous abundant eosinophilic cytoplasm and whorled squamous eddies; often atypia and mitotic figures; resembles eddies; often atypia and mitotic figures; resembles carcinomacarcinoma
inverted follicular keratosisinverted follicular keratosis – irritated seborrheic keratosis – irritated seborrheic keratosis that grows downward and involves hair folliclesthat grows downward and involves hair follicles
Also hyperkeratotic, adenoid, acantholytic and Also hyperkeratotic, adenoid, acantholytic and desmoplastic patternsdesmoplastic patterns
Positive stains:Positive stains: low molecular weight keratin low molecular weight keratin Negative stains:Negative stains: high molecular weight keratin high molecular weight keratin
(usually), HPV(usually), HPV DD:DD: squamous cell carcinoma (particularly squamous cell carcinoma (particularly
desmoplastic pattern)desmoplastic pattern)
Fibroepithelial polypFibroepithelial polyp
neoplasmaneoplasma 2323
Fibroepithelial polypFibroepithelial polyp
Also called acrochordon, squamous Also called acrochordon, squamous papilloma, skin tag, soft fibromapapilloma, skin tag, soft fibroma
Common, non-neoplastic, no clinical Common, non-neoplastic, no clinical significancesignificance
Ages 40+ years; usually face, neck, Ages 40+ years; usually face, neck, trunk, intertriginous areastrunk, intertriginous areas
Associated with diabetes, intestinal Associated with diabetes, intestinal polyposis; increase during pregnancypolyposis; increase during pregnancy
May be a common endpoint of May be a common endpoint of various processes, including various processes, including seborrheic keratosis or wartsseborrheic keratosis or warts
neoplasmaneoplasma 2424
Acquired (digital) fibrokeratoma:Acquired (digital) fibrokeratoma: collagenous protrusions covered by collagenous protrusions covered by hyperkeratotic epithelium, often at hyperkeratotic epithelium, often at interphalangeal joints; dermis lacks adnexaeinterphalangeal joints; dermis lacks adnexae
Gross:Gross: soft, flesh-colored, baglike tumor, soft, flesh-colored, baglike tumor, attached to skin by slender stalkattached to skin by slender stalk
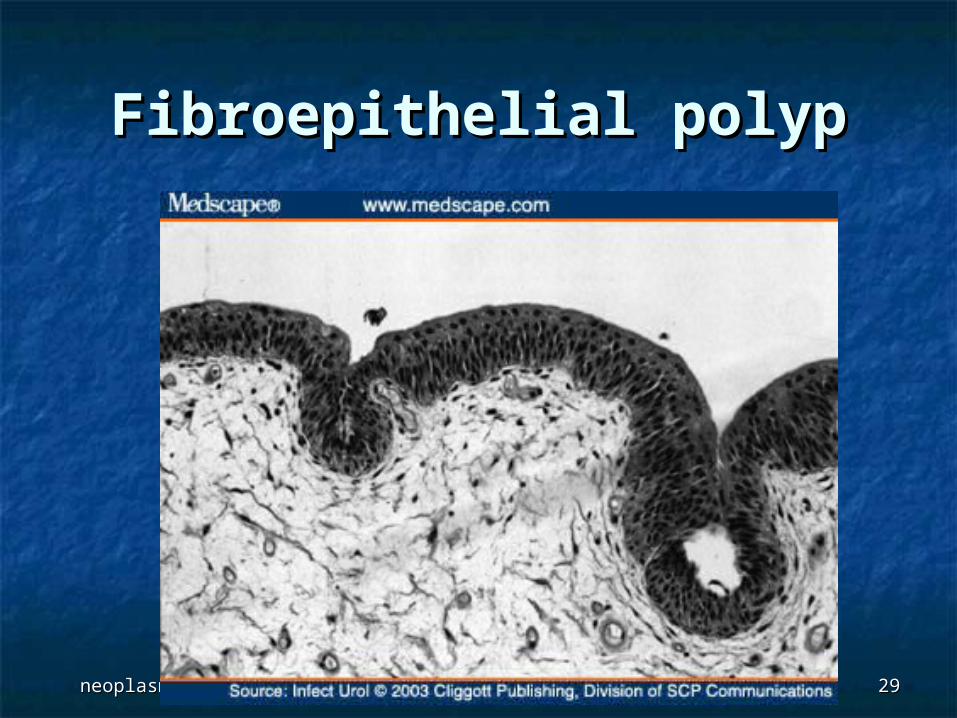
Micro:Micro: papillary, fibrovascular cores covered papillary, fibrovascular cores covered by squamous epithelium; may have ischemic by squamous epithelium; may have ischemic necrosis due to torsionnecrosis due to torsion
Fibroepithelial polypFibroepithelial polyp
neoplasmaneoplasma 2525
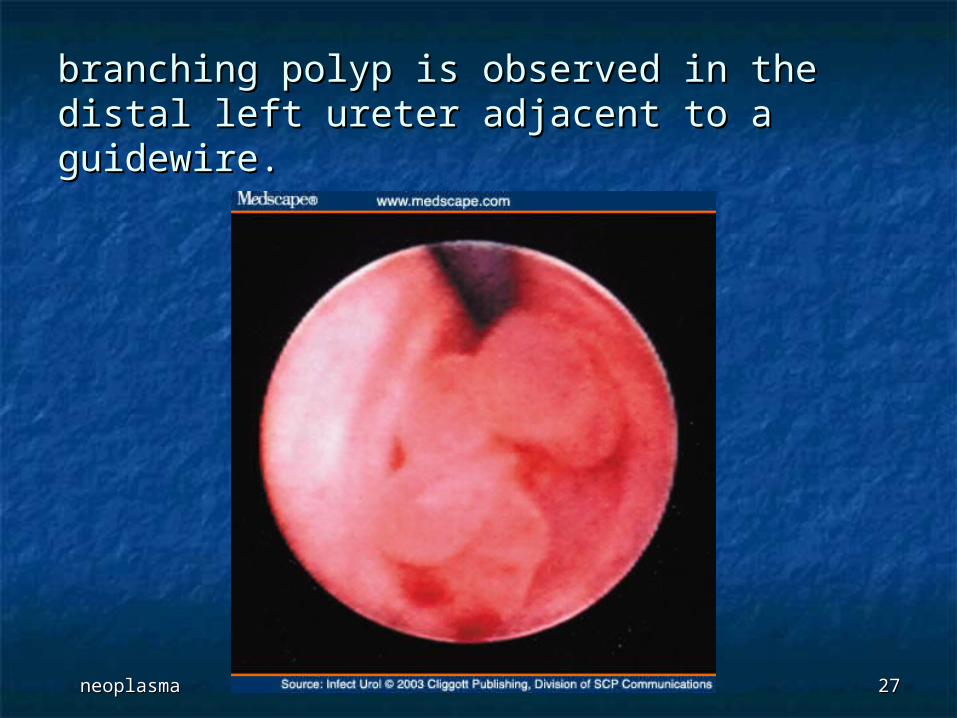
Fibroepithelial Polyp of the Fibroepithelial Polyp of the UreterUreter
A 73-year-old woman presented with A 73-year-old woman presented with asymptomatic gross hematuria. Her asymptomatic gross hematuria. Her physical examination was unremarkable. A physical examination was unremarkable. A complete blood cell count, levels of serum complete blood cell count, levels of serum electrolytes and creatinine, and results of electrolytes and creatinine, and results of cytologic evaluation of voided urine were cytologic evaluation of voided urine were normal. Urinalysis showed 0 to 2 white normal. Urinalysis showed 0 to 2 white blood cells and 25 to 50 red blood cells per blood cells and 25 to 50 red blood cells per high-power field. Urine culture was high-power field. Urine culture was negative.negative.
neoplasmaneoplasma 2626
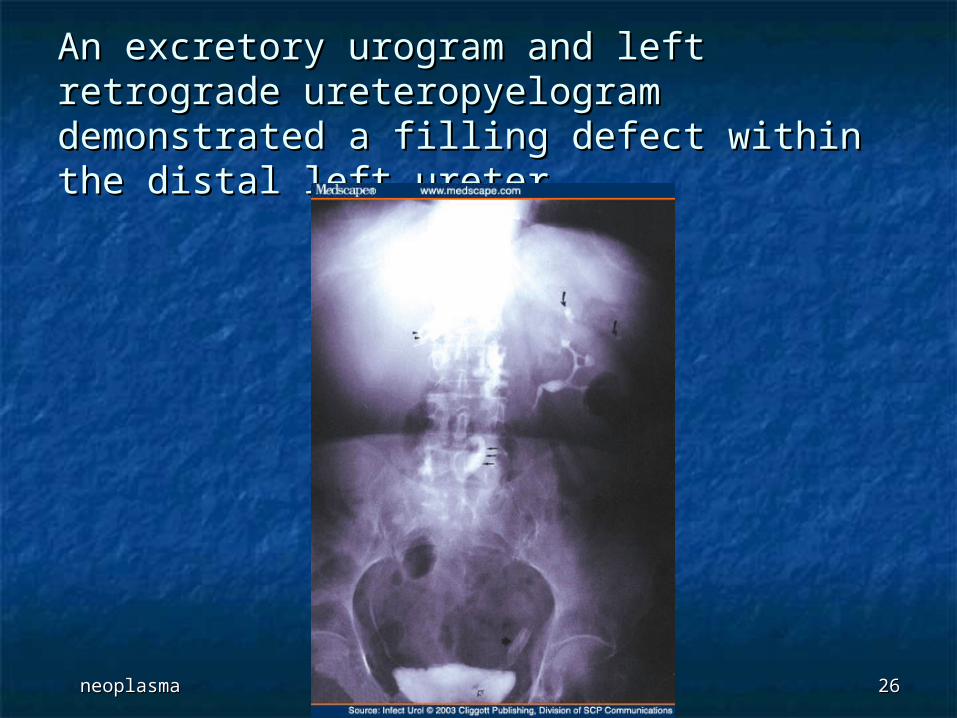
An excretory urogram and left retrograde An excretory urogram and left retrograde ureteropyelogram demonstrated a filling ureteropyelogram demonstrated a filling defect within the distal left ureter defect within the distal left ureter
neoplasmaneoplasma 2727
branching polyp is observed in the distal left branching polyp is observed in the distal left ureter adjacent to a guidewire. ureter adjacent to a guidewire.
neoplasmaneoplasma 2828
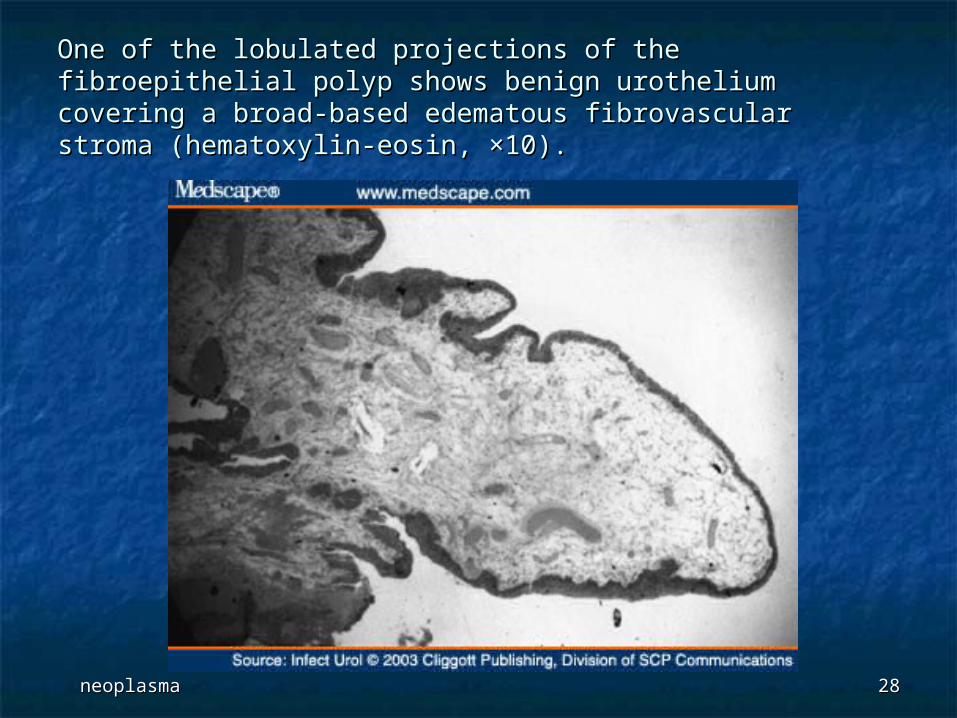
One of the lobulated projections of the fibroepithelial polyp One of the lobulated projections of the fibroepithelial polyp shows benign urothelium covering a broad-based edematous shows benign urothelium covering a broad-based edematous fibrovascular stroma (hematoxylin-eosin, ×10).fibrovascular stroma (hematoxylin-eosin, ×10).
neoplasmaneoplasma 2929
Fibroepithelial polypFibroepithelial polyp
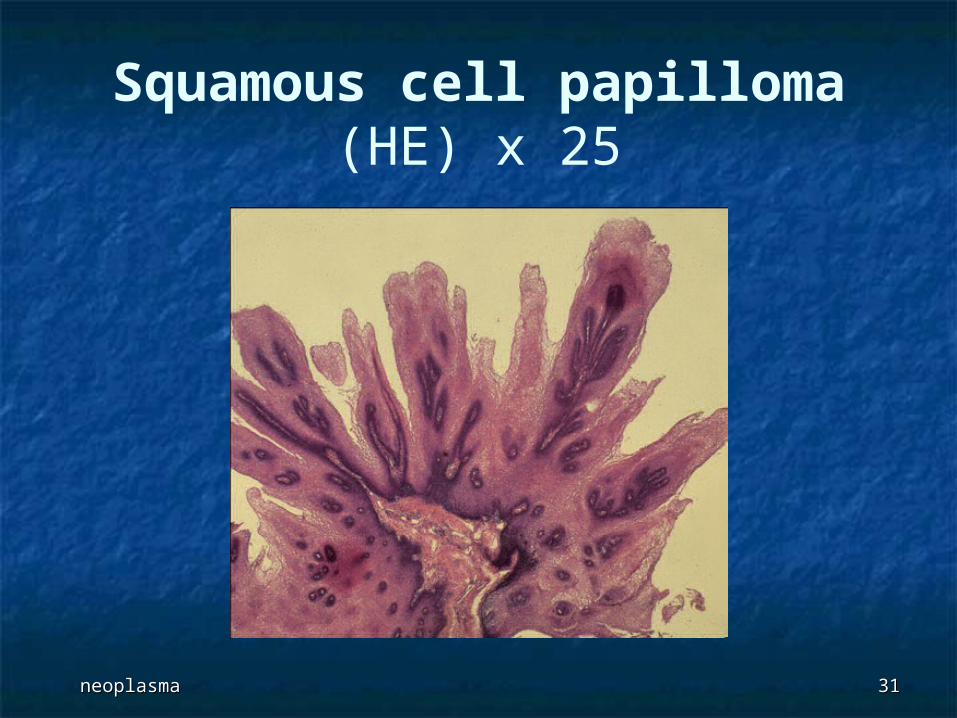
PAPILLOMAPAPILLOMA
neoplasmaneoplasma 3131
Squamous cell papilloma(HE) x 25
neoplasmaneoplasma 3232
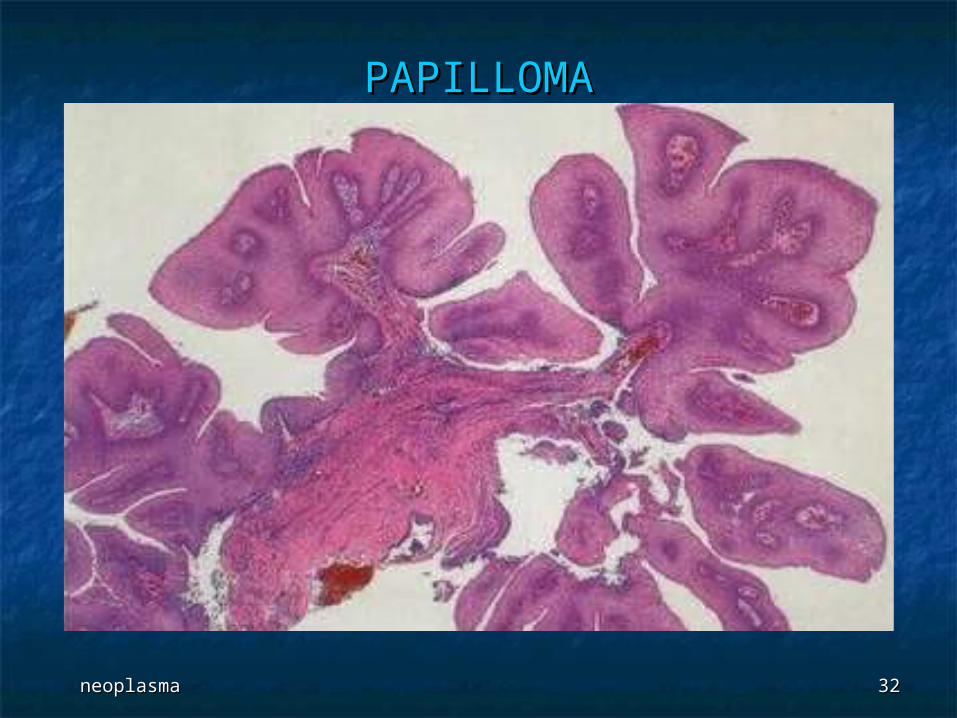
PAPILLOMAPAPILLOMA

neoplasmaneoplasma 3333
PAPILLOMAPAPILLOMA
INTRADERMAL INTRADERMAL PIGMENTED NEVIPIGMENTED NEVI

neoplasmaneoplasma 3535
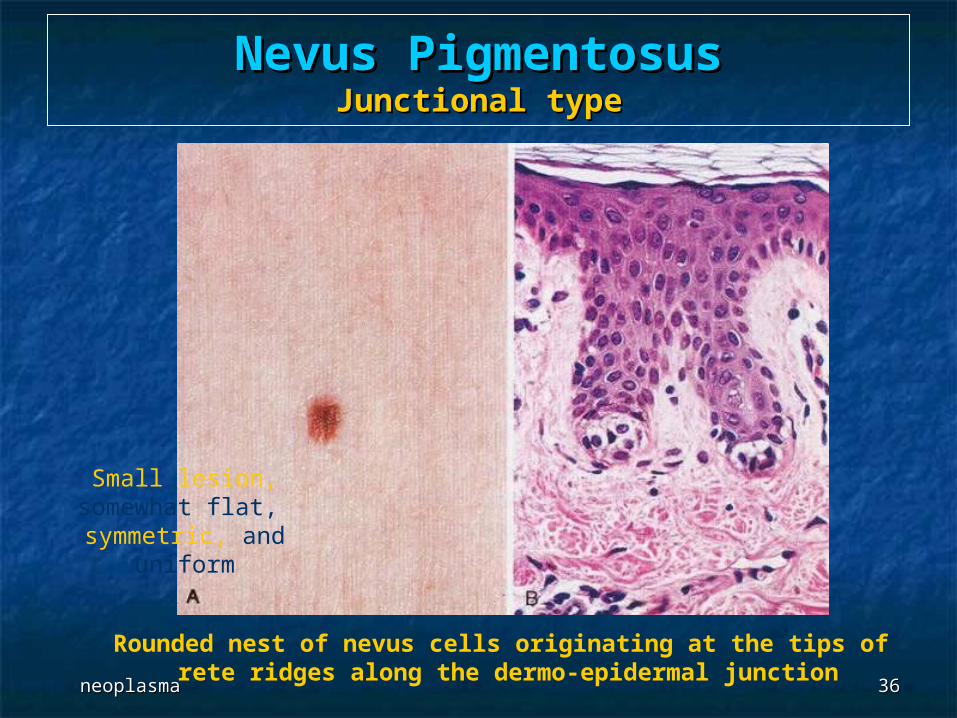
Nevus PigmentosusNevus Pigmentosus
neoplasmaneoplasma 3636
Nevus PigmentosusNevus PigmentosusJunctional typeJunctional type
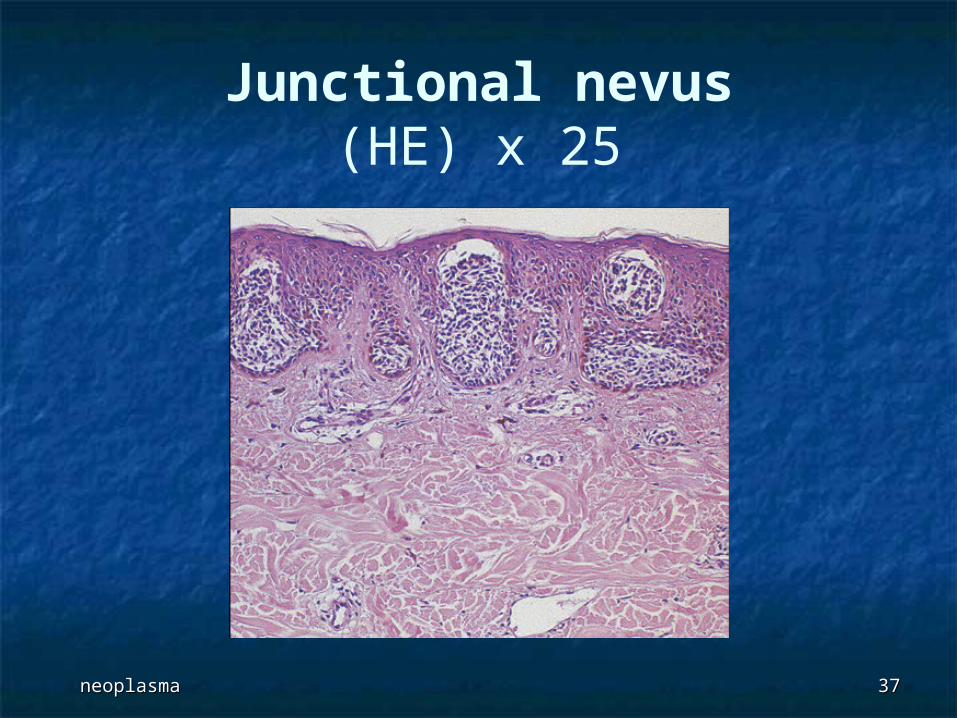
Rounded nest of nevus cells originating at the tips of rete ridges along the dermo-epidermal junction
Small lesion, somewhat flat, symmetric, and uniform
neoplasmaneoplasma 3737
Junctional nevus(HE) x 25
neoplasmaneoplasma 3838
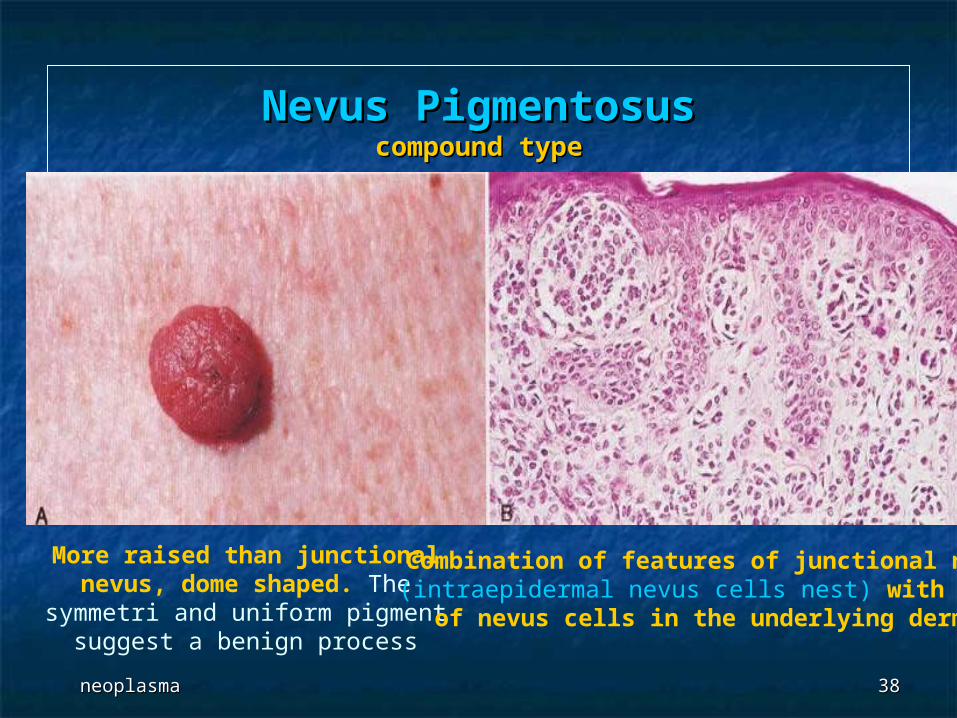
Nevus PigmentosusNevus Pigmentosuscompound typecompound type
More raised than junctional nevus, dome shaped. The symmetri and uniform
pigment suggest a benign process
Combination of features of junctional nevi (intraepidermal nevus cells nest) with nest of nevus cells in the underlying dermis
neoplasmaneoplasma 3939
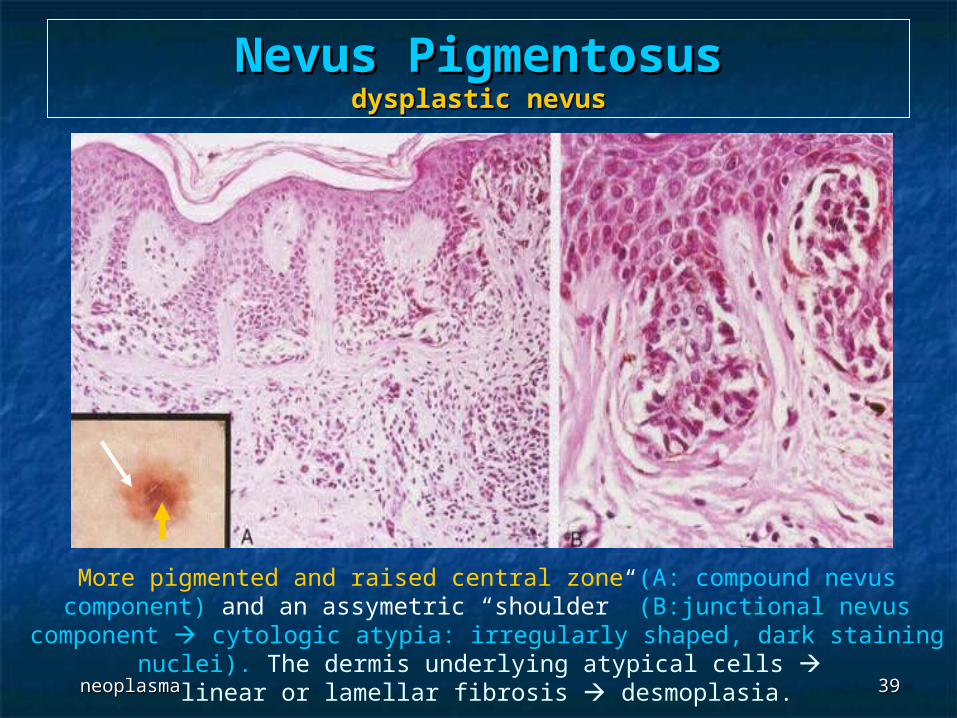
Nevus PigmentosusNevus Pigmentosusdysplastic nevusdysplastic nevus
More pigmented and raised central zone (A: compound nevus component) and an assymetric “shoulder” (B:junctional nevus component cytologic atypia: irregularly
shaped, dark staining nuclei). The dermis underlying atypical cells linear or lamellar fibrosis desmoplasia.

neoplasmaneoplasma 4040
PIGMENTED NEVIPIGMENTED NEVI
MALIGNANT MELANOMAMALIGNANT MELANOMA
neoplasmaneoplasma 4242
MelanomaMelanoma Incidence increasing worldwide - 48,000 cases Incidence increasing worldwide - 48,000 cases
and 9,200 deaths in US in 2000and 9,200 deaths in US in 2000 Usually due to sun (UV light) exposureUsually due to sun (UV light) exposure Warning signs:Warning signs: change in color of change in color of
pigmented lesion, enlargement of existing pigmented lesion, enlargement of existing mole, itching or pain in preexisting mole, mole, itching or pain in preexisting mole, development of new pigmented lesion in adult development of new pigmented lesion in adult life, irregular borders in pigmented lesion, life, irregular borders in pigmented lesion, variegation of color in pigmented lesionvariegation of color in pigmented lesion
Head and neck, lower extremities (particularly Head and neck, lower extremities (particularly in women); rarely subungual (“melanotic in women); rarely subungual (“melanotic whitlow”), palm, sole. Also oral and anogenital whitlow”), palm, sole. Also oral and anogenital mucosa, esophagus, meninges, eyemucosa, esophagus, meninges, eye
neoplasmaneoplasma 4343
Populations at higher risk:Populations at higher risk: whites with fair skin, whites with fair skin, red hair, tendency to burn or freckle from sun red hair, tendency to burn or freckle from sun exposure, large number of melanocytic nevi, exposure, large number of melanocytic nevi, xeroderma pigmentosum, familial dysplastic nevi, xeroderma pigmentosum, familial dysplastic nevi, melanosis, vitiligo, possibly neurofibromatosis type Imelanosis, vitiligo, possibly neurofibromatosis type I
Up to 10% may be familial due to CMM1 gene at 1p36Up to 10% may be familial due to CMM1 gene at 1p36 Blacks have low risk, their common melanoma sites Blacks have low risk, their common melanoma sites
are palms, soles, nail beds or mucous membranesare palms, soles, nail beds or mucous membranes Usually after puberty, occasionally children - all have Usually after puberty, occasionally children - all have
same morphologysame morphology 5% are multiple, although prognosis is related to type 5% are multiple, although prognosis is related to type
and stage of largest lesion, not number of lesions; and stage of largest lesion, not number of lesions; must distinguish multiple lesions from “hot nevi” / must distinguish multiple lesions from “hot nevi” / nevus activationnevus activation
Achilles tendon tumors are often spindledAchilles tendon tumors are often spindled Tend to grow laterally and deep; common metastases Tend to grow laterally and deep; common metastases
to regional lymph nodes, also liver, lungs, GI tract, to regional lymph nodes, also liver, lungs, GI tract, bone, CNS, heart (50% at autopsy), skin (satellite bone, CNS, heart (50% at autopsy), skin (satellite tumors within 2 cm of primary tumor), other sitestumors within 2 cm of primary tumor), other sites
Overall 5 year survival is 60%Overall 5 year survival is 60%
neoplasmaneoplasma 4444
Poor prognostic factors:Poor prognostic factors: increased Breslow (vertical) thickness in primary increased Breslow (vertical) thickness in primary
tumor, tumor, high stage (TNM), high stage (TNM), males (do worse than females), males (do worse than females), high mitotic rate, high mitotic rate, ulceration, ulceration, microscopic satellites (tumor nests 50 microns microscopic satellites (tumor nests 50 microns
or larger and separated from main tumor mass), or larger and separated from main tumor mass), deeper level of invasion for T1 tumors, deeper level of invasion for T1 tumors, higher % tumor area/volume in sentinel node, higher % tumor area/volume in sentinel node, increased density of dendritic leukocytes in increased density of dendritic leukocytes in
nodal paracortex (associated with risk of tumor nodal paracortex (associated with risk of tumor in non-sentinel nodes, recurrence and death, in non-sentinel nodes, recurrence and death, Mod Path 2004;17:747Mod Path 2004;17:747))
Overall behavior is variable, with occasional Overall behavior is variable, with occasional late deaths or long survival even with late deaths or long survival even with widespread satellite noduleswidespread satellite nodules
neoplasmaneoplasma 4545
S100:S100: nuclear and cytoplasmic, 90%+ sensitive but not specific nuclear and cytoplasmic, 90%+ sensitive but not specific
(although usually negative in tumors considered in the (although usually negative in tumors considered in the differential)differential)
HMB45:HMB45: less sensitive but more specific than S100; negative in less sensitive but more specific than S100; negative in
desmoplastic melanomadesmoplastic melanoma MelanA/Mart1:MelanA/Mart1:
sensitive, but also stains steroid-producing cells in ovary, sensitive, but also stains steroid-producing cells in ovary, testis, adrenal cortextestis, adrenal cortex
Tyrosinase:Tyrosinase: sensitive, but also stains peripheral nerve sheath and sensitive, but also stains peripheral nerve sheath and
neuroendocrine tumorsneuroendocrine tumors Microphthalmia transcription factor:Microphthalmia transcription factor:
sensitive, but also stains dermatofibroma and smooth muscle sensitive, but also stains dermatofibroma and smooth muscle tumors; negative in spindle cell / desmoplastic melanomatumors; negative in spindle cell / desmoplastic melanoma
NKI-C3 and NSE:NKI-C3 and NSE: nonspecific nonspecific Negative stains:Negative stains: p53 p53
MelanomaMelanoma
neoplasmaneoplasma 4646
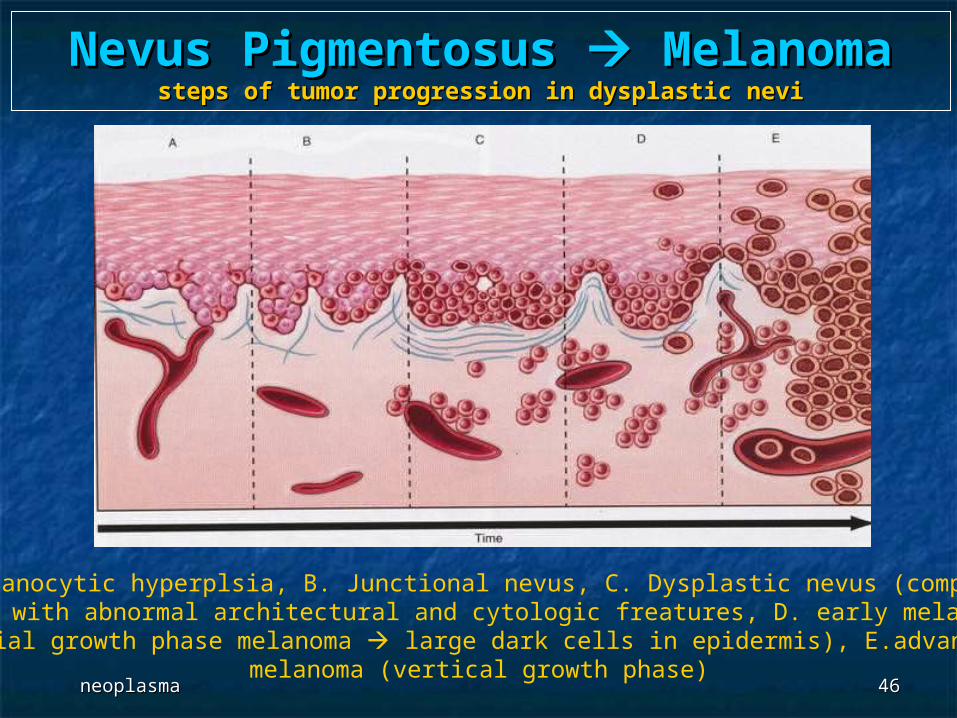
Nevus Pigmentosus Nevus Pigmentosus Melanoma Melanomasteps of tumor progression in dysplastic nevisteps of tumor progression in dysplastic nevi
A. Melanocytic hyperplsia, B. Junctional nevus, C. Dysplastic nevus (compound nevus with abnormal architectural and cytologic freatures, D. early melanoma (radial growth phase melanoma large dark cells in epidermis), E.advanced
melanoma (vertical growth phase)
neoplasmaneoplasma 4747
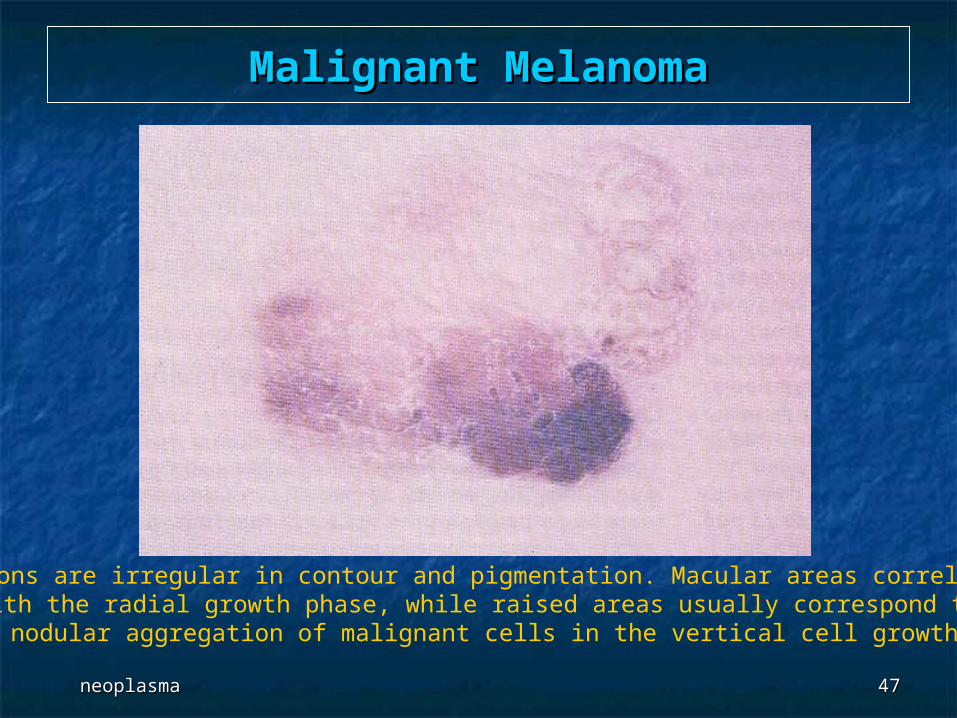
Malignant MelanomaMalignant Melanoma
Lesions are irregular in contour and pigmentation. Macular areas correlated with the radial growth phase, while raised areas usually correspond to
nodular aggregation of malignant cells in the vertical cell growth
neoplasmaneoplasma 4848
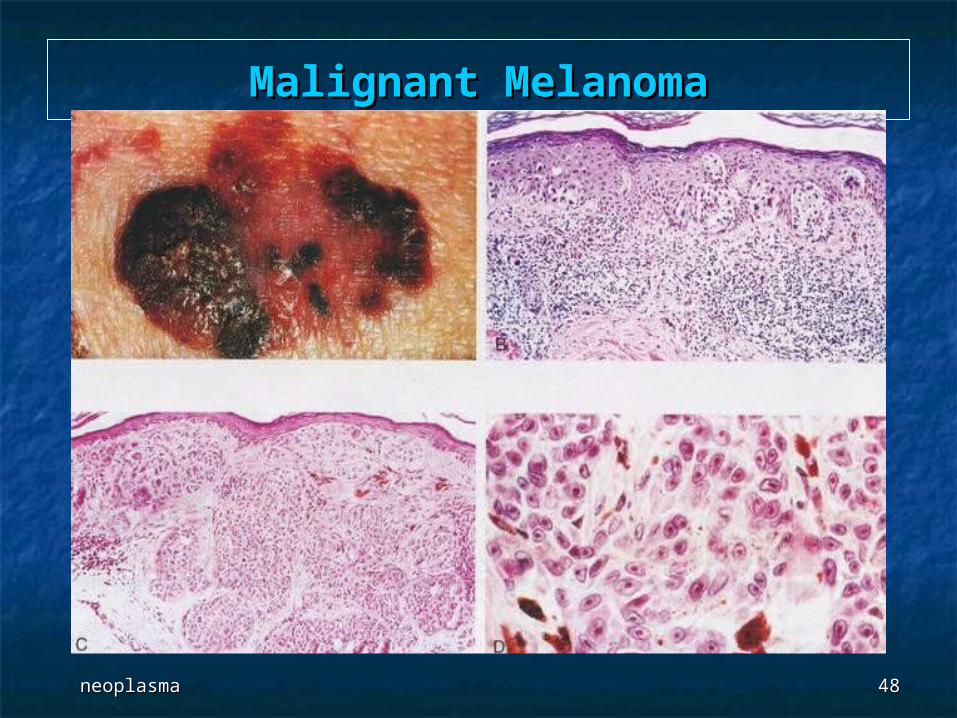
Malignant MelanomaMalignant Melanoma
neoplasmaneoplasma 4949
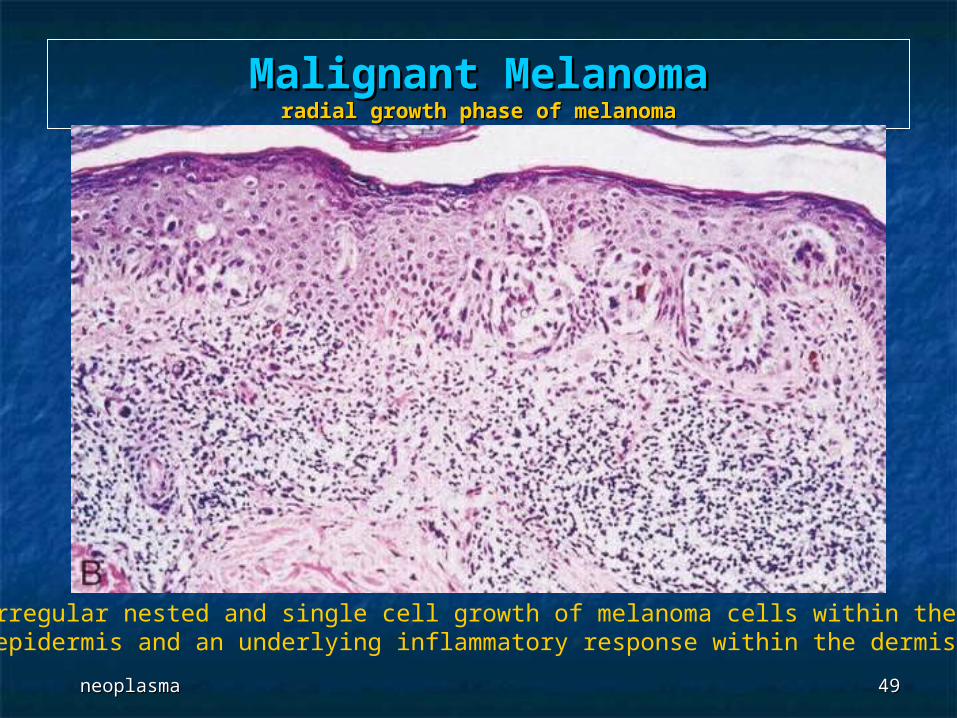
Malignant MelanomaMalignant Melanomaradial growth phase of melanomaradial growth phase of melanoma
Irregular nested and single cell growth of melanoma cells within the epidermis and an underlying inflammatory response within the dermis
neoplasmaneoplasma 5050
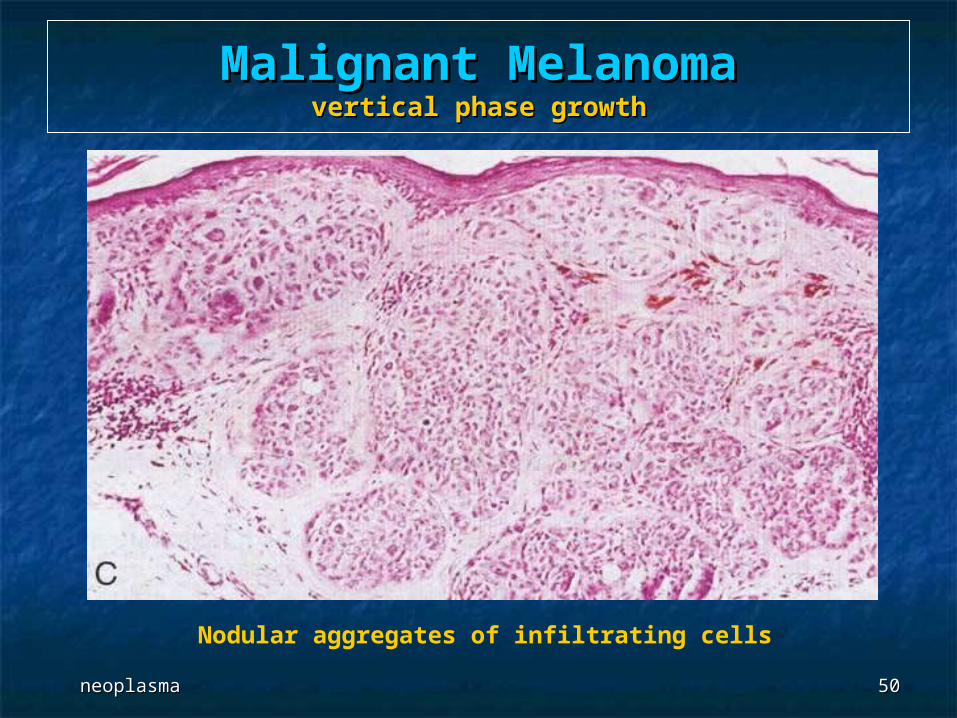
Malignant MelanomaMalignant Melanomavertical phase growthvertical phase growth
Nodular aggregates of infiltrating cells
neoplasmaneoplasma 5151
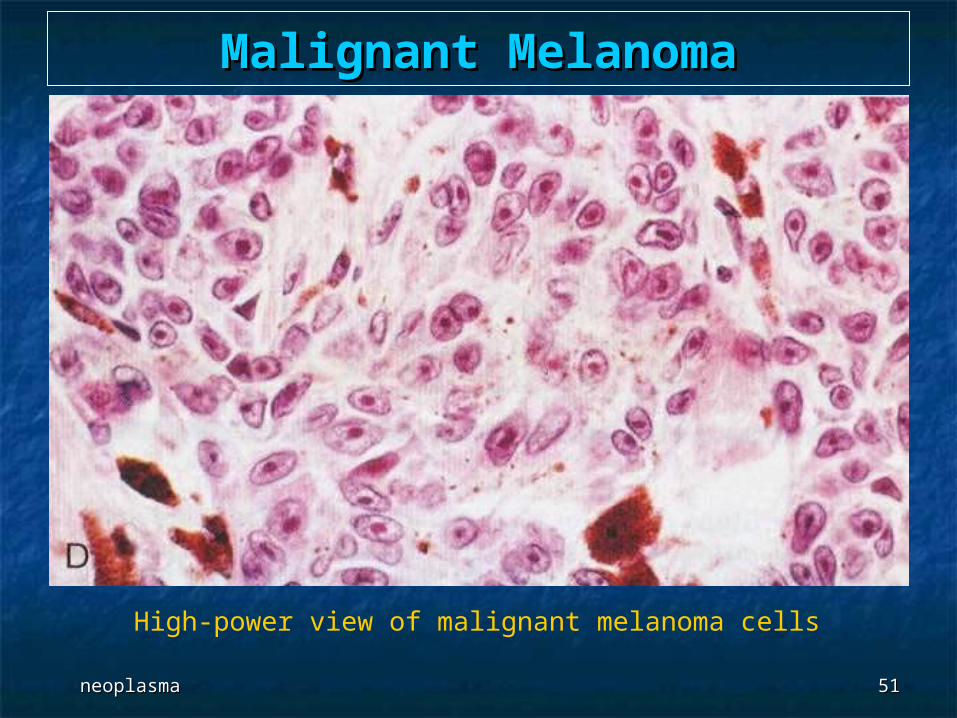
Malignant MelanomaMalignant Melanoma
High-power view of malignant melanoma cells
neoplasmaneoplasma 5252
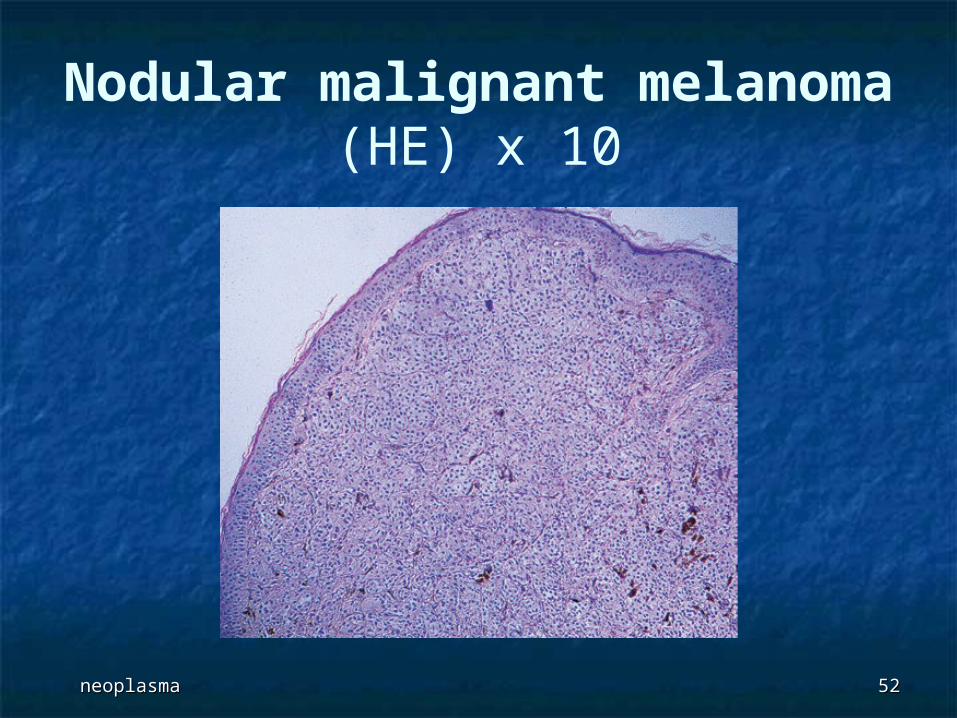
Nodular malignant melanoma(HE) x 10
neoplasmaneoplasma 5353
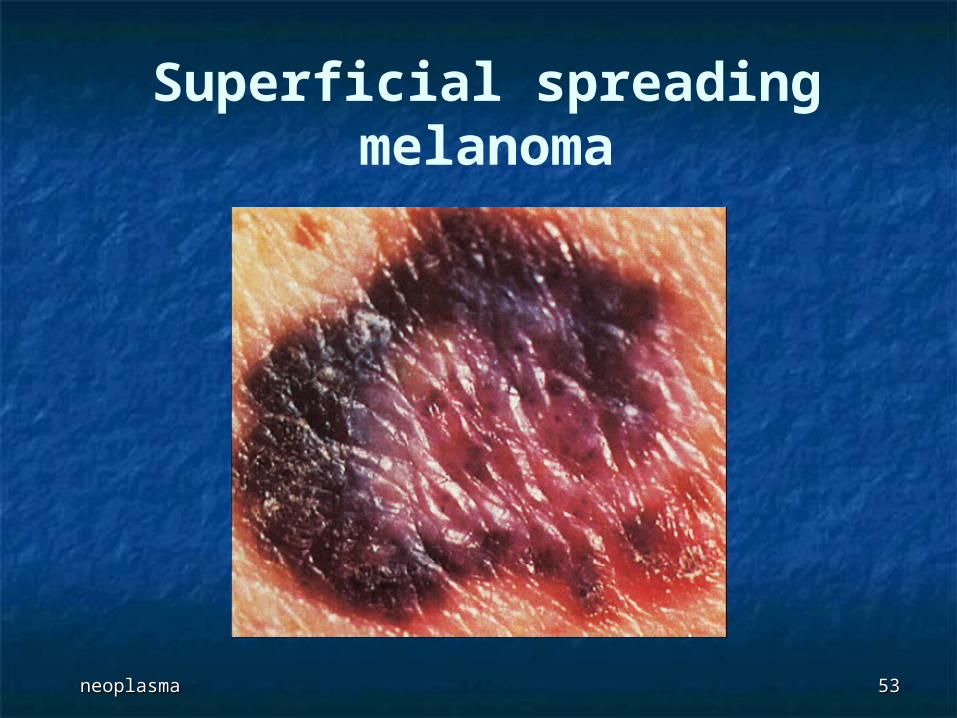
Superficial spreading melanoma
neoplasmaneoplasma 5454
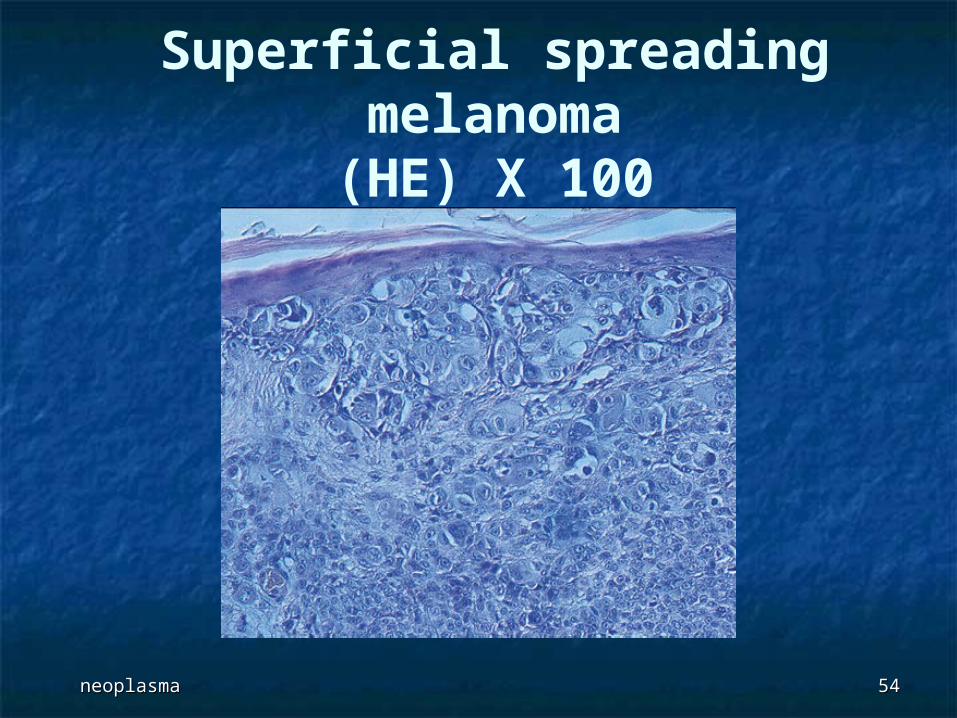
Superficial spreading melanoma(HE) X 100
neoplasmaneoplasma 5555
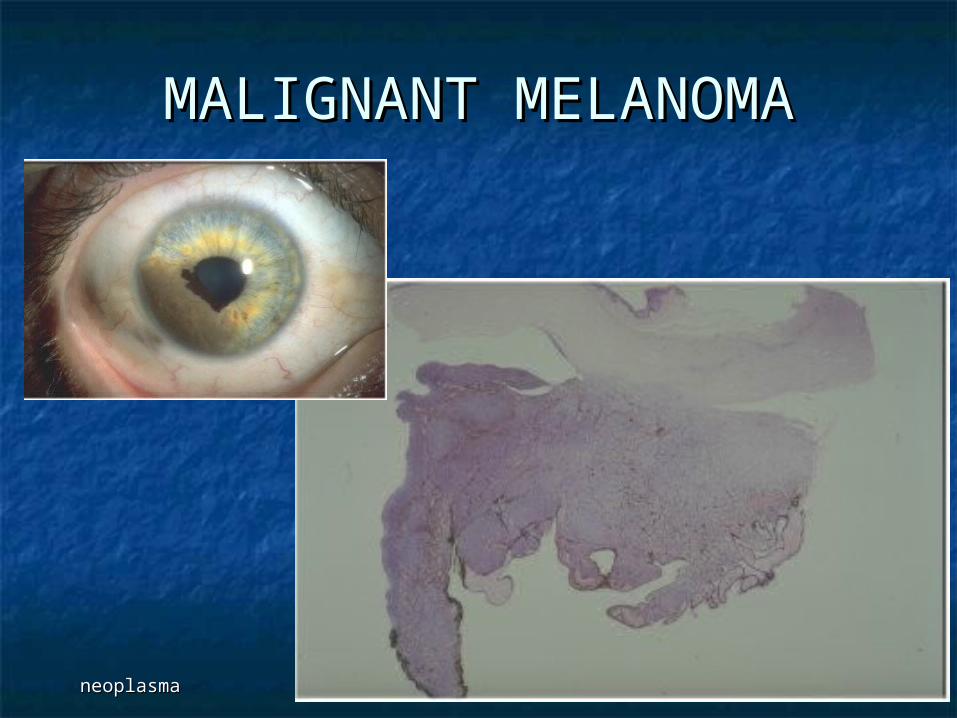
MALIGNANT MELANOMAMALIGNANT MELANOMA

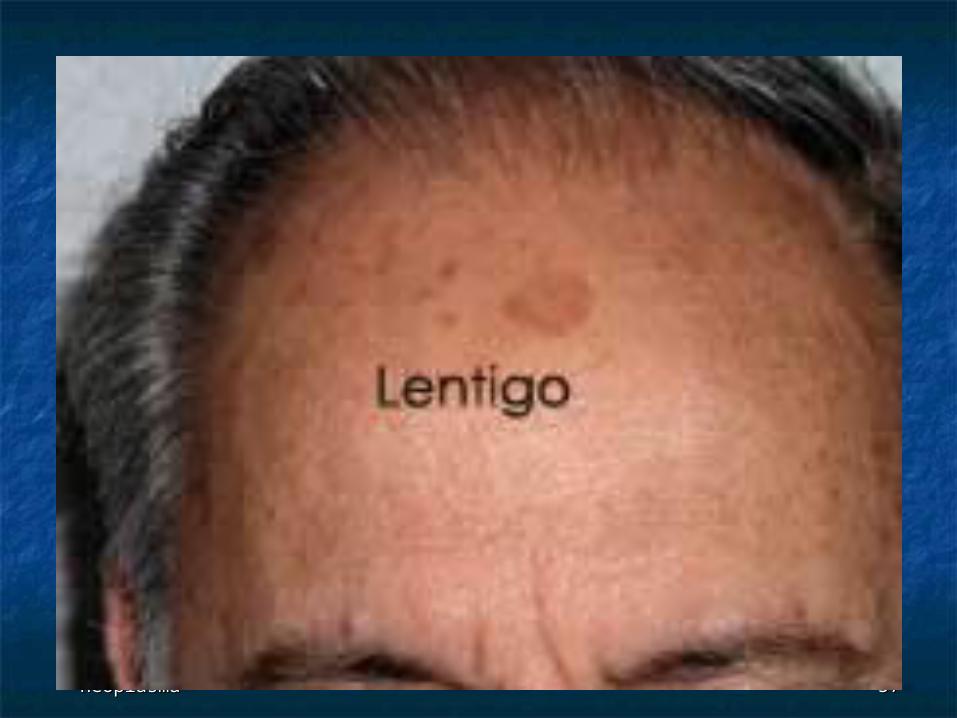
LENTIGOLENTIGO
neoplasmaneoplasma 5757
neoplasmaneoplasma 5858
Lentiginous melanocytic Lentiginous melanocytic nevusnevus
Often benign mole with increase in size, formation Often benign mole with increase in size, formation of irregular borders or peripheral change in colorof irregular borders or peripheral change in color
May be due to “reactivation” of radial proliferationMay be due to “reactivation” of radial proliferation Benign, but complete excision is recommendedBenign, but complete excision is recommended Micro:Micro: “shoulder” area of lentiginous junctional “shoulder” area of lentiginous junctional
melanocytic proliferation beyond lateral border of melanocytic proliferation beyond lateral border of underlying dermal nevus; no atypiaunderlying dermal nevus; no atypia
DD:DD: dysplastic nevi, superficial spreading dysplastic nevi, superficial spreading melanomamelanoma
neoplasmaneoplasma 5959
Lentigo malignaLentigo maligna
Also called melanoma arising in Also called melanoma arising in Hutchinson’s freckle, actinic melanosisHutchinson’s freckle, actinic melanosis
Consisted the melanocytic equivalent Consisted the melanocytic equivalent of actinic keratosisof actinic keratosis
Slow growing lesion of sun exposed Slow growing lesion of sun exposed skin of elderly whites, often cheekskin of elderly whites, often cheek
Unusual to die of diseaseUnusual to die of disease Partial regression is commonPartial regression is common
neoplasmaneoplasma 6060
lentigo maligna, by definition, does NOT infiltrate into lentigo maligna, by definition, does NOT infiltrate into dermis, but lentigo maligna melanoma has single cell dermis, but lentigo maligna melanoma has single cell infiltration into papillary dermisinfiltration into papillary dermis
Treatment:Treatment: excision, radiation excision, radiation Gross:Gross: flat, tan to black with flat, tan to black with irregular hyperpigmentation, > 2 irregular hyperpigmentation, > 2
cmcm Micro:Micro: atypical melanocytes in basal layer, individually atypical melanocytes in basal layer, individually
and in nests (theques); cells are often spindled, and in nests (theques); cells are often spindled, pleomorphic and have cytoplasmic retraction; dermis pleomorphic and have cytoplasmic retraction; dermis shows solar elastosis; also epidermal atrophy, actinic shows solar elastosis; also epidermal atrophy, actinic damage, basilar keratinocyte hyperpigmentationdamage, basilar keratinocyte hyperpigmentation
DD:DD: invasive melanoma (clear cut dermal infiltration, not invasive melanoma (clear cut dermal infiltration, not just atypical melanocytes in deep rete ridges), just atypical melanocytes in deep rete ridges), desmoplastic melanoma (may arise secondary to lentigo desmoplastic melanoma (may arise secondary to lentigo maligna)maligna)
Lentigo malignaLentigo maligna

neoplasmaneoplasma 6161
Lentigo maligna
neoplasmaneoplasma 6262
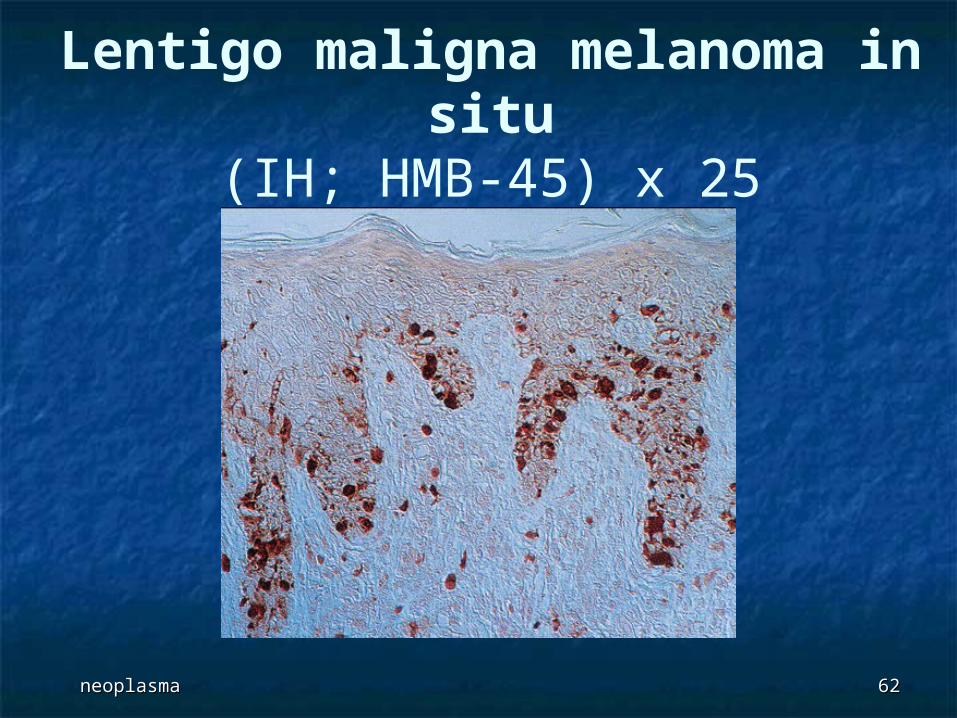
Lentigo maligna melanoma in situ
(IH; HMB-45) x 25
BOWEN’S DISEASEBOWEN’S DISEASE
neoplasmaneoplasma 6464
Bowen’s diseaseBowen’s disease
Usually on skin NOT exposed to Usually on skin NOT exposed to sunlight, such as trunksunlight, such as trunk
Called erythroplasia if at glans penis, Called erythroplasia if at glans penis, vulva, oral cavityvulva, oral cavity
Often considered as carcinoma in Often considered as carcinoma in situ or squamous intraepidermal situ or squamous intraepidermal neoplasianeoplasia
neoplasmaneoplasma 6565
Gross:Gross: slightly raised, large scaly slightly raised, large scaly erythematous plaque with irregular border; erythematous plaque with irregular border; usually single patch or verrucous growthusually single patch or verrucous growth
Micro:Micro: atypia is prominent and throughout epidermis; atypia is prominent and throughout epidermis;
includes nuclear hyperchromasia and includes nuclear hyperchromasia and multinucleation, individual cell dyskeratosis, multinucleation, individual cell dyskeratosis,
increased mitotic figures, atypical mitotic increased mitotic figures, atypical mitotic figures; figures;
also cytoplasmic vacuoles, markedly altered also cytoplasmic vacuoles, markedly altered maturation, but usually still some surface maturation, but usually still some surface keratinization; keratinization;
may extend into eccrine sweat glands (not may extend into eccrine sweat glands (not considered invasive disease); considered invasive disease);
intercellular bridges present; intercellular bridges present; rarely pagetoid cells or ground glass cytoplasmrarely pagetoid cells or ground glass cytoplasm
neoplasmaneoplasma 6666
Micro images:Micro images: - - Positive stains:Positive stains: p53, HPV, high molecular weight p53, HPV, high molecular weight cytokeratincytokeratin
Molecular:Molecular: aneuploid aneuploid DD:DD: bowenoid actinic keratosis bowenoid actinic keratosis
(circumscribed, in sun-exposed areas (circumscribed, in sun-exposed areas with clinical appearance of actinic with clinical appearance of actinic keratosis), chronic arsenic ingestionkeratosis), chronic arsenic ingestion

neoplasmaneoplasma 6767
Bowen’s diseaseBowen’s disease

neoplasmaneoplasma 6868
Bowen’s diseaseBowen’s disease
SQUAMOUS CELL SQUAMOUS CELL CARCINOMACARCINOMA
neoplasmaneoplasma 7070
Common, derived from keratinocytes in Common, derived from keratinocytes in epidermal layerepidermal layer
Usually men, associated with Usually men, associated with sun exposure (UV light may induce p53 sun exposure (UV light may induce p53
mutations and diminish surveillance function of mutations and diminish surveillance function of Langerhans cells in epidermis), Langerhans cells in epidermis),
PUVA treatment for psoriasis, arsenic, tars/oils, PUVA treatment for psoriasis, arsenic, tars/oils, chronic ulcers, chronic ulcers,
draining osteomyelitis, draining osteomyelitis, old burn scars, old burn scars, necrobiosis lipoidica, necrobiosis lipoidica, hidradenitis suppurativa, hidradenitis suppurativa, ionizing radiationionizing radiation
SQUAMOUS CELL SQUAMOUS CELL CARCINOMACARCINOMA
neoplasmaneoplasma 7171
Risk factors: Risk factors: immunosuppression (post-transplant or HIV), immunosuppression (post-transplant or HIV), xeroderma pigmentosa (disorder with diminished xeroderma pigmentosa (disorder with diminished
capacity for DNA repair after UV light exposure, due to capacity for DNA repair after UV light exposure, due to gene at 9q22.3; associated with squamous cell, basal gene at 9q22.3; associated with squamous cell, basal cell carcinoma and melanoma), cell carcinoma and melanoma),
lack of pigmentation in skin, lack of pigmentation in skin, actinic keratosis (precursor lesion), actinic keratosis (precursor lesion), epidermodysplasia verruciformis; epidermodysplasia verruciformis; very rare in blacksvery rare in blacks
5% are node positive at diagnosis; metastatic 5% are node positive at diagnosis; metastatic rate is 5-10% in transplant patients, who do rate is 5-10% in transplant patients, who do poorly with metastatic diseasepoorly with metastatic disease
Slow growing, locally invasive but rarely Slow growing, locally invasive but rarely metastasizes outside nodes (but see above); metastasizes outside nodes (but see above); most common site is lungmost common site is lung
Metastases more likely in tumors that originate in Metastases more likely in tumors that originate in scars or ulcersscars or ulcers
neoplasmaneoplasma 7272
Prognosis:Prognosis: excellent; metastases uncommon if excellent; metastases uncommon if tumor < 1.5 cm deep; 5% metastasize if 2 cm or tumor < 1.5 cm deep; 5% metastasize if 2 cm or more and definite dermal invasionmore and definite dermal invasion
Good prognostic factors:Good prognostic factors: low stage, low stage, no/superficial dermal invasion, small vertical tumor no/superficial dermal invasion, small vertical tumor
thickness (< 4 mm), thickness (< 4 mm), well differentiated, well differentiated, short duration, short duration, location other than scalp, ears, lips, nose, eyelids or soft location other than scalp, ears, lips, nose, eyelids or soft
tissue (which readily invade subcutaneous tissue)tissue (which readily invade subcutaneous tissue) Treatment:Treatment: surgical excision with adequate surgical excision with adequate
margins; also currettage, electrodesiccation, margins; also currettage, electrodesiccation, cryotherapy, radiation therapycryotherapy, radiation therapy
SQUAMOUS CELL SQUAMOUS CELL CARCINOMACARCINOMA
neoplasmaneoplasma 7373
Gross: Gross: often white plaque (leukoplakia); may have often white plaque (leukoplakia); may have induration, ulceration, hemorrhageinduration, ulceration, hemorrhage
Micro:Micro: atypia at all levels of epidermis; 80% are well atypia at all levels of epidermis; 80% are well differentiated with keratin pearls, intercellular bridges differentiated with keratin pearls, intercellular bridges and no/rare keratohyaline granules; invade dermis by and no/rare keratohyaline granules; invade dermis by definition; definition; may contain non-neoplastic melanocytes that transfer may contain non-neoplastic melanocytes that transfer
melanin to tumor cells; occasionally clear cells, rarely signet melanin to tumor cells; occasionally clear cells, rarely signet ring cellsring cells
Spindle, adenoid and verrucous variants are described Spindle, adenoid and verrucous variants are described separatelyseparately
Other variants are acantholytic (pseudoglandular, tumor Other variants are acantholytic (pseudoglandular, tumor clefts produed by acantholysis of tumor cells) and clefts produed by acantholysis of tumor cells) and pseudoangiosarcomatous (clefts separate neoplastic lobules)pseudoangiosarcomatous (clefts separate neoplastic lobules)
Low grade (well differentiated):Low grade (well differentiated): cell cell differentiation, uniform cell size, intact intercellular differentiation, uniform cell size, intact intercellular bridges, no/rare mitotic figures, no/mild pleomorphismbridges, no/rare mitotic figures, no/mild pleomorphism
High grade (poorly differentiated):High grade (poorly differentiated): little cell little cell differentiation, pleomorphism with spindle cells, differentiation, pleomorphism with spindle cells, necrosis, marked mitotic activity, deep invasionnecrosis, marked mitotic activity, deep invasion
neoplasmaneoplasma 7474
Positive stains:Positive stains: high molecular weight keratin, high molecular weight keratin, EMA, EMA, involucrin, involucrin, p53 (50%), p53 (50%), variable CEAvariable CEA
Negative stains:Negative stains: Ber-EP4, usually CK7 and CK20 (head and neck Ber-EP4, usually CK7 and CK20 (head and neck
tumors, tumors, Mod Path 2004;17:407Mod Path 2004;17:407)) DD:DD: keratoacanthoma (for well keratoacanthoma (for well
differentiated tumors)differentiated tumors)
SQUAMOUS CELL SQUAMOUS CELL CARCINOMACARCINOMA

neoplasmaneoplasma 7575
Squamous Cell CaSquamous Cell Ca

neoplasmaneoplasma 7676
Squamous Cell CaSquamous Cell Ca
neoplasmaneoplasma 7777
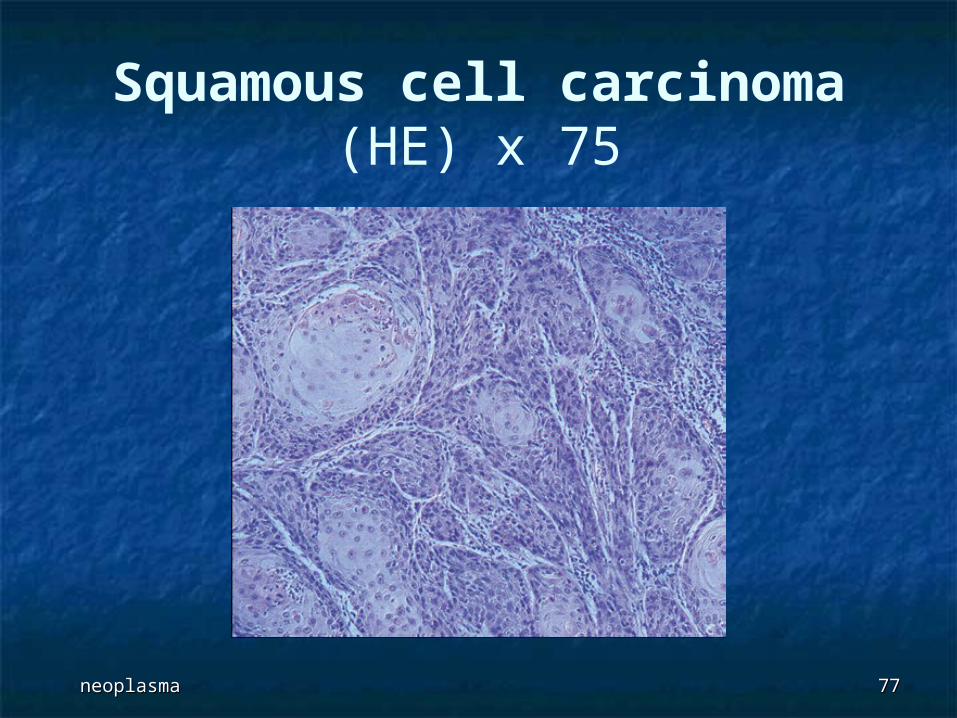
Squamous cell carcinoma(HE) x 75
neoplasmaneoplasma 7878
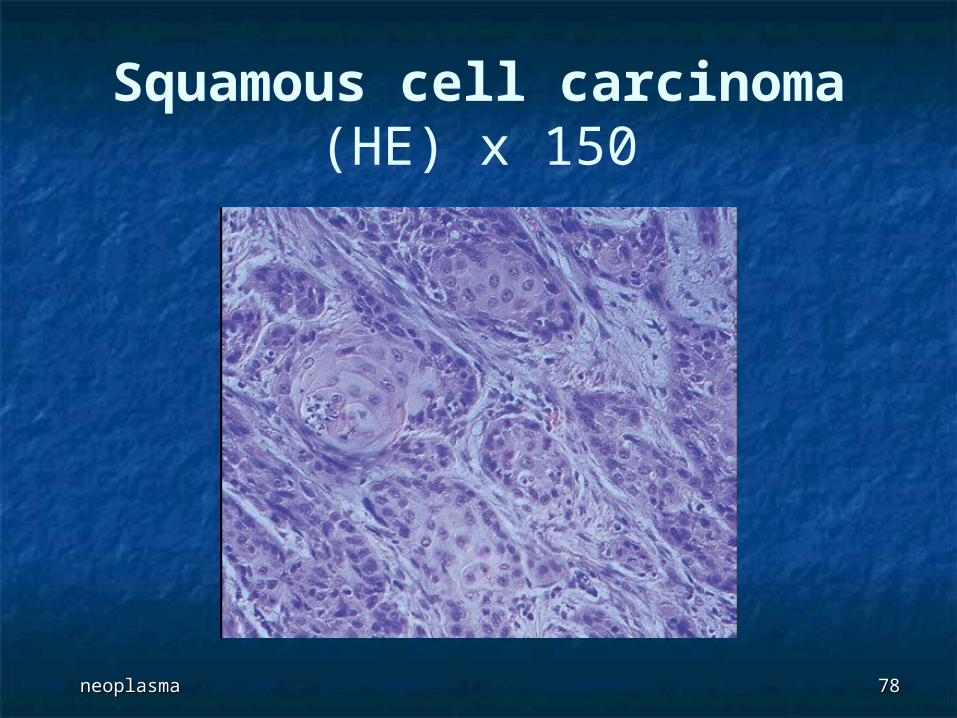
Squamous cell carcinoma(HE) x 150
neoplasmaneoplasma 7979
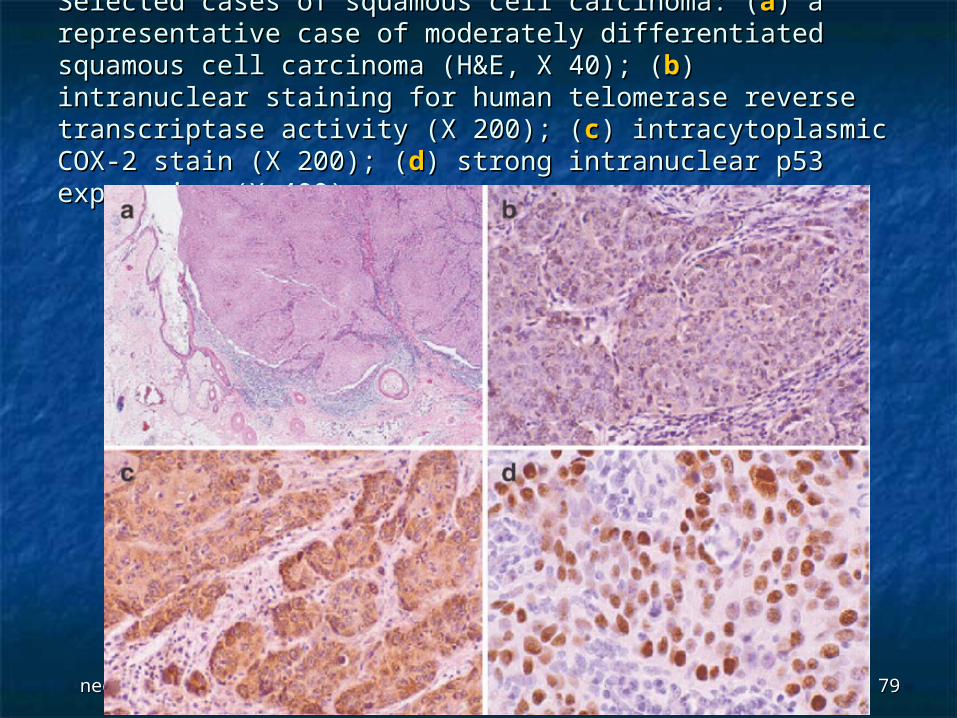
Selected cases of squamous cell carcinoma: (Selected cases of squamous cell carcinoma: (aa) a ) a representative case of moderately differentiated squamous representative case of moderately differentiated squamous cell carcinoma (H&E, X 40); (cell carcinoma (H&E, X 40); (bb) intranuclear staining for ) intranuclear staining for human telomerase reverse transcriptase activity (X 200); (human telomerase reverse transcriptase activity (X 200); (cc) ) intracytoplasmic COX-2 stain (X 200); (intracytoplasmic COX-2 stain (X 200); (dd) strong intranuclear ) strong intranuclear p53 expression (X 400).p53 expression (X 400).
neoplasmaneoplasma 8080
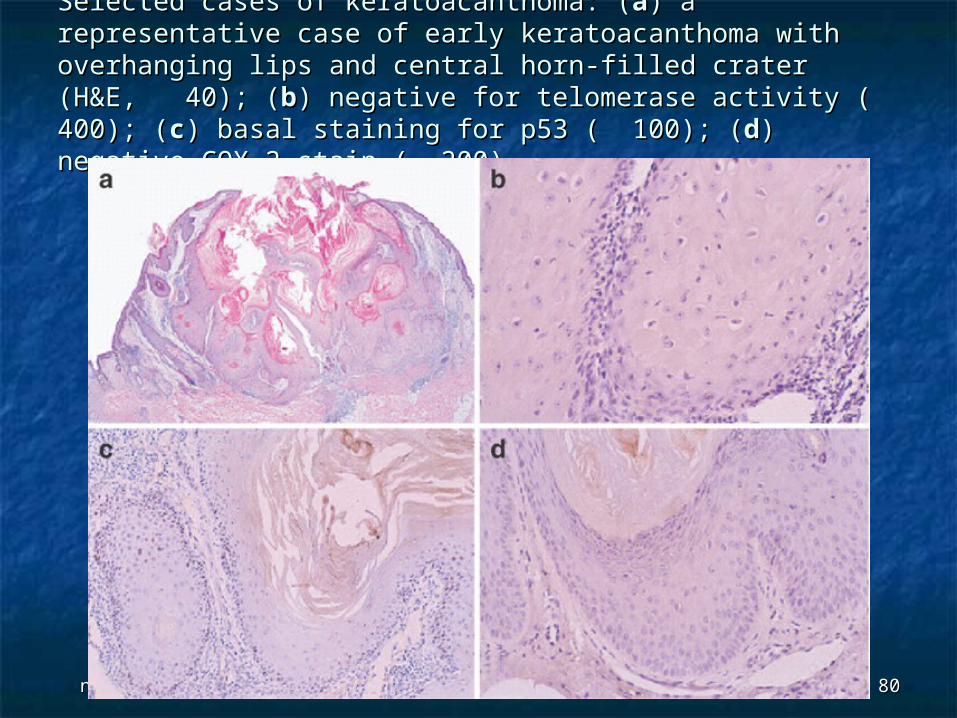
Selected cases of keratoacanthoma: (Selected cases of keratoacanthoma: (aa) a representative case ) a representative case of early keratoacanthoma with overhanging lips and central of early keratoacanthoma with overhanging lips and central horn-filled crater (H&E, 40); (horn-filled crater (H&E, 40); (bb) negative for telomerase ) negative for telomerase activity ( 400); (activity ( 400); (cc) basal staining for p53 ( 100); () basal staining for p53 ( 100); (dd) negative ) negative COX-2 stain ( 200). COX-2 stain ( 200).
TABLE …..TABLE …..
Histopathologic criteria to Histopathologic criteria to differentiate early differentiate early
keratoacanthomakeratoacanthoma from a well to from a well to moderately differentiated moderately differentiated
squamous cell carcinomasquamous cell carcinoma (Ackerman (Ackerman et et
alal and Cribier and Cribier et alet al))
neoplasmaneoplasma 8282
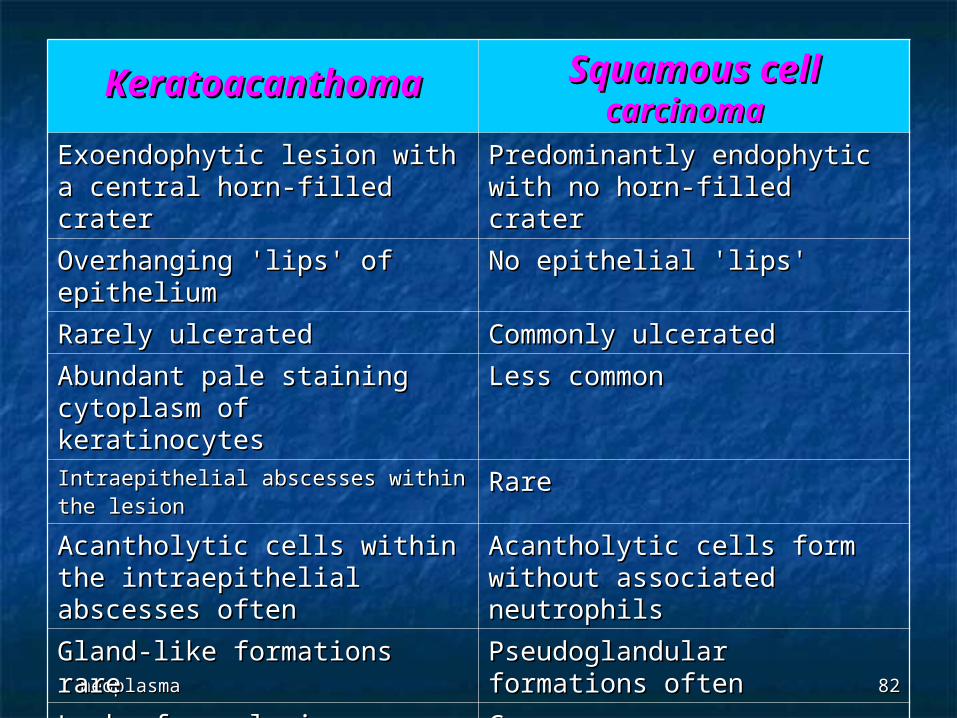
KeratoacanthomaKeratoacanthoma Squamous cell Squamous cell carcinomacarcinoma
Exoendophytic lesion with a Exoendophytic lesion with a central horn-filled crater central horn-filled crater
Predominantly endophytic Predominantly endophytic with no horn-filled craterwith no horn-filled crater
Overhanging 'lips' of Overhanging 'lips' of epithelium epithelium
No epithelial 'lips' No epithelial 'lips'
Rarely ulcerated Rarely ulcerated Commonly ulcerated Commonly ulcerated
Abundant pale staining Abundant pale staining cytoplasm of keratinocytes cytoplasm of keratinocytes
Less common Less common
Intraepithelial abscesses within the Intraepithelial abscesses within the lesionlesion
Rare Rare
Acantholytic cells within the Acantholytic cells within the intraepithelial abscesses often intraepithelial abscesses often
Acantholytic cells form Acantholytic cells form without associated neutrophils without associated neutrophils
Gland-like formations rare Gland-like formations rare Pseudoglandular formations Pseudoglandular formations often often
Lack of anaplasiaLack of anaplasia Common Common
Sharp outline between tumor Sharp outline between tumor nests and stromanests and stroma
IndistinctIndistinct
Absence of stroma Absence of stroma desmoplasiadesmoplasia
PresentPresent
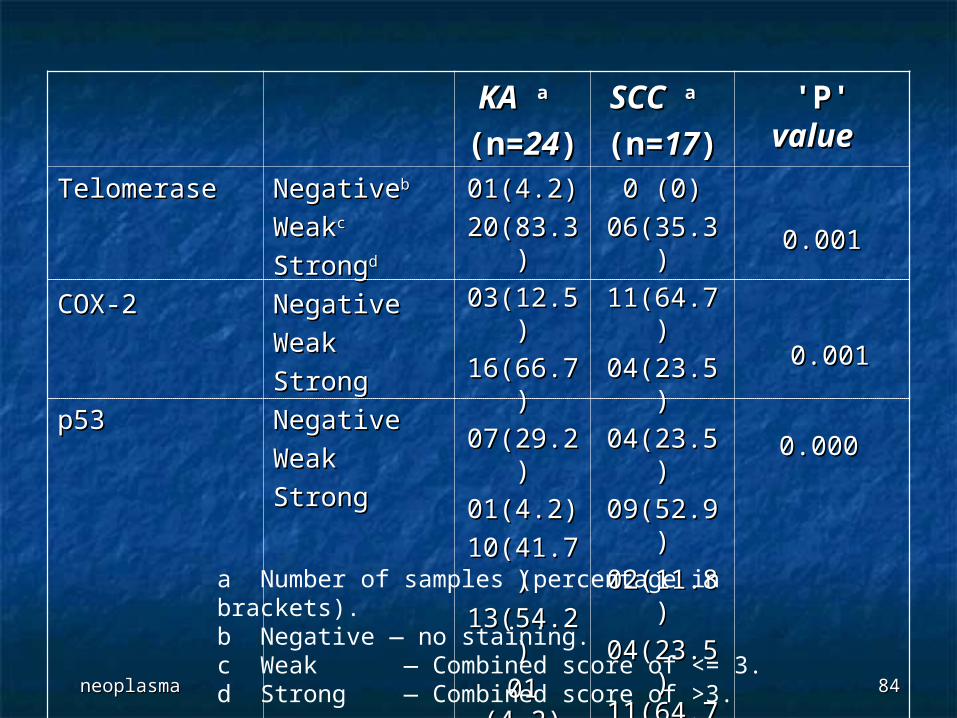
Immunohistochemical expression of Immunohistochemical expression of telomerase activity, COX-2, and p53 telomerase activity, COX-2, and p53
in keratoacanthoma (KA) and in keratoacanthoma (KA) and squamous cell carcinoma (SCC). squamous cell carcinoma (SCC).
TABLE …..TABLE …..
neoplasmaneoplasma 8484
KAKA aa
(n=(n=2424))
SCCSCC aa
(n=(n=1717)) 'P' 'P' valuevalue
TelomeraseTelomerase
COX-2COX-2
p53p53
NegativeNegativebb
WeakWeakcc
StrongStrongdd
NegativeNegative
WeakWeak
StrongStrong
NegativeNegative
WeakWeak
Strong Strong
01(4.2)01(4.2)
20(83.3)20(83.3)
03(12.5)03(12.5)
16(66.7)16(66.7)
07(29.2)07(29.2)
01(4.2)01(4.2)
10(41.7)10(41.7)
13(54.2)13(54.2)
01 (4.2)01 (4.2)
0 (0)0 (0)
06(35.3)06(35.3)
11(64.7)11(64.7)
04(23.5)04(23.5)
04(23.5)04(23.5)
09(52.9)09(52.9)
02(11.8)02(11.8)
04(23.5)04(23.5)11(64.7)11(64.7)
0.0010.001
0.0010.001
0.0000.000
a Number of samples (percentage in brackets).b Negative — no staining.c Weak — Combined score of <= 3.d Strong — Combined score of >3.

BASAL CELL CARCINOMABASAL CELL CARCINOMA
neoplasmaneoplasma 8686
Most frequent form of skin cancerMost frequent form of skin cancer Usually sun exposed skin (not mucosal surfaces), in Usually sun exposed skin (not mucosal surfaces), in
proportion to number of pilosebaceous units presentproportion to number of pilosebaceous units present Rosai claims these tumors attempt to differentiate Rosai claims these tumors attempt to differentiate
toward pilosebaceous units, but often this is not toward pilosebaceous units, but often this is not readily apparentreadily apparent
Often multiple tumorsOften multiple tumors Usually older adultsUsually older adults Slow and indolent, untreated cases may invade Slow and indolent, untreated cases may invade
subcutis, skeletal muscle and bone; facial tumors subcutis, skeletal muscle and bone; facial tumors may invade skull, nares, orbit or temporal bone; only may invade skull, nares, orbit or temporal bone; only 100 metastatic cases described, often associated 100 metastatic cases described, often associated with basal cell nevus syndrome or basosquamous with basal cell nevus syndrome or basosquamous histology, on sunlight-protected skinhistology, on sunlight-protected skin
Metastases are rare; 60% to regional lymph nodes, Metastases are rare; 60% to regional lymph nodes, also lung, liver, bonealso lung, liver, bone
BASAL CELL CARCINOMABASAL CELL CARCINOMA
neoplasmaneoplasma 8787
Risk factors:Risk factors: fair skin, blue eyes, fair skin, blue eyes, immunosuppression (higher incidence, more immunosuppression (higher incidence, more
aggressive tumors), aggressive tumors), xeroderma pigmentosumxeroderma pigmentosum
Also associated with Also associated with nevus sebaceus of Jadassohn, nevus sebaceus of Jadassohn, chronic venous stasis of lower leg, chronic venous stasis of lower leg, arsenic, X rays, arsenic, X rays, skin injury, chickenpox scars, skin injury, chickenpox scars, tattoos, hair transplant scars, tattoos, hair transplant scars, immunosuppressionimmunosuppression
Less common in children or young adults, Less common in children or young adults, sunlight-protected skin; rarely coexists sunlight-protected skin; rarely coexists with benign nevuswith benign nevus
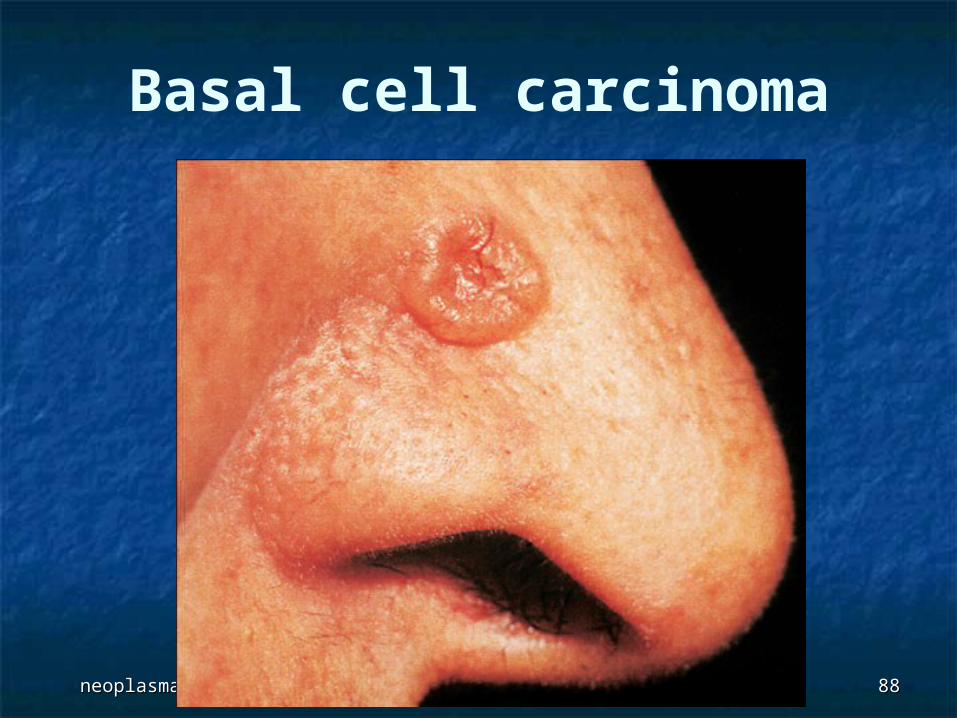
neoplasmaneoplasma 8888
Basal cell carcinoma
neoplasmaneoplasma 8989
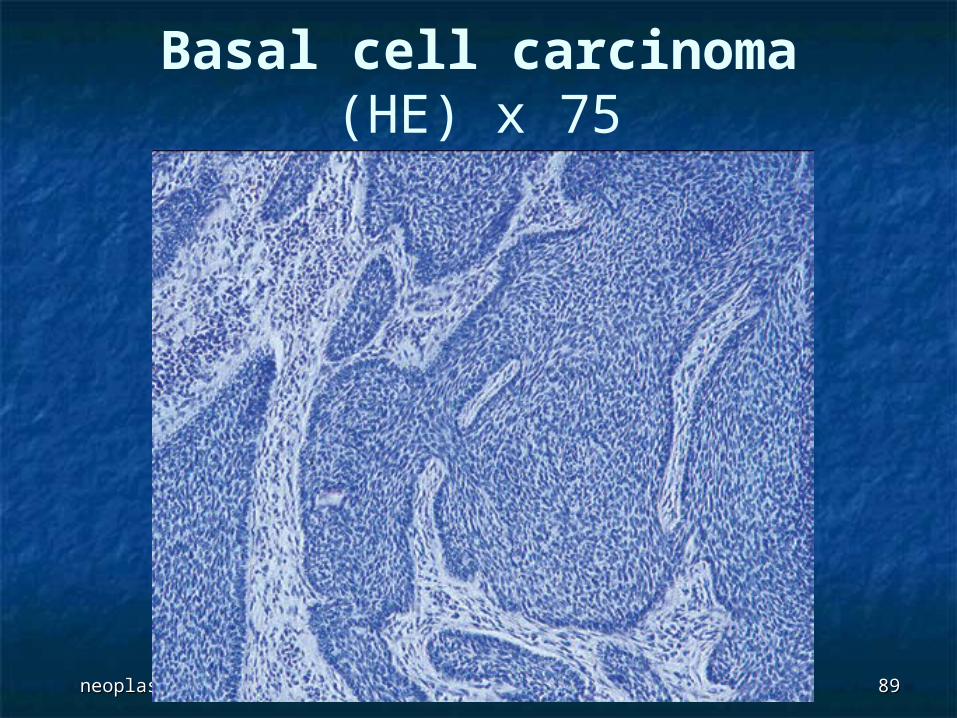
Basal cell carcinoma(HE) x 75
QUIZ QUIZ
neoplasmaneoplasma 9191
A 14-year-old girl presented with a 3-A 14-year-old girl presented with a 3-month history of multiple upper month history of multiple upper extremity nodules. Physical extremity nodules. Physical examination revealed examination revealed multiple multiple erythematous pigmented noduleserythematous pigmented nodules, 0.5 , 0.5 to 1 cm in diameter, slightly pruritic, to 1 cm in diameter, slightly pruritic, involving the upper limbs (Figure 1). A involving the upper limbs (Figure 1). A skin biopsy of a nodular lesion was skin biopsy of a nodular lesion was performed (Figure 2). performed (Figure 2).
MiniquizMiniquiz

neoplasmaneoplasma 9292
Figure 1 : Erythematous Figure 1 : Erythematous pigmented pigmented nodules of nodules of forearmsforearms
neoplasmaneoplasma 9393
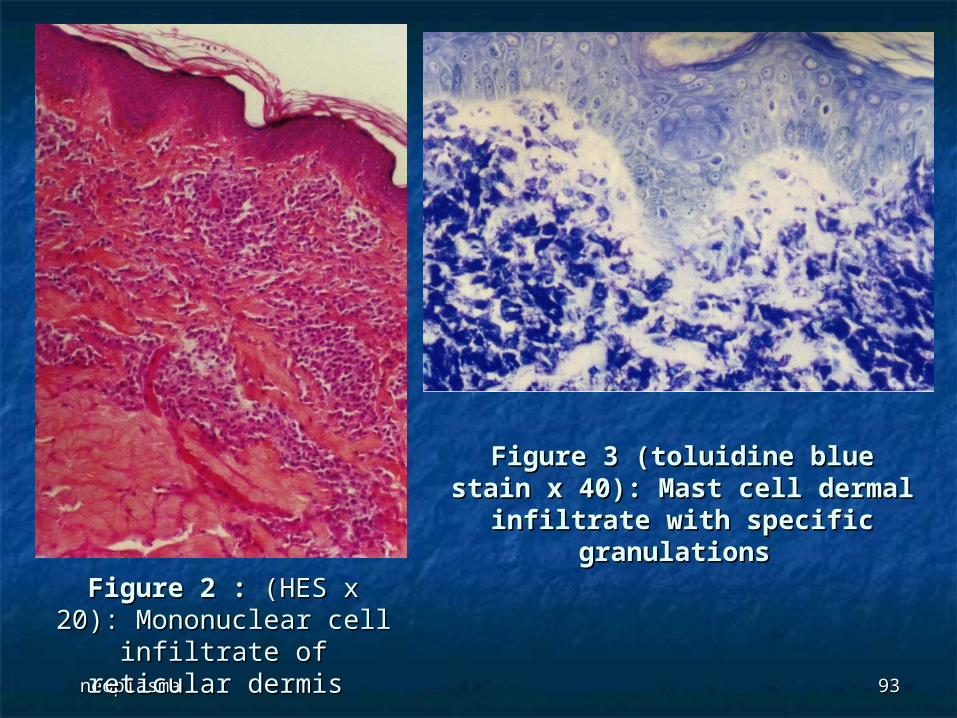
Figure 2 : Figure 2 : (HES x 20): (HES x 20): Mononuclear cell infiltrate Mononuclear cell infiltrate
of reticular dermis of reticular dermis
Figure 3 (toluidine blue stain x Figure 3 (toluidine blue stain x 40): Mast cell dermal infiltrate 40): Mast cell dermal infiltrate
with specific granulationswith specific granulations
Question :Question :
What is the diagnosis of this What is the diagnosis of this case ?case ?
Answer:Answer:
MastocytosisMastocytosis
neoplasmaneoplasma 9696
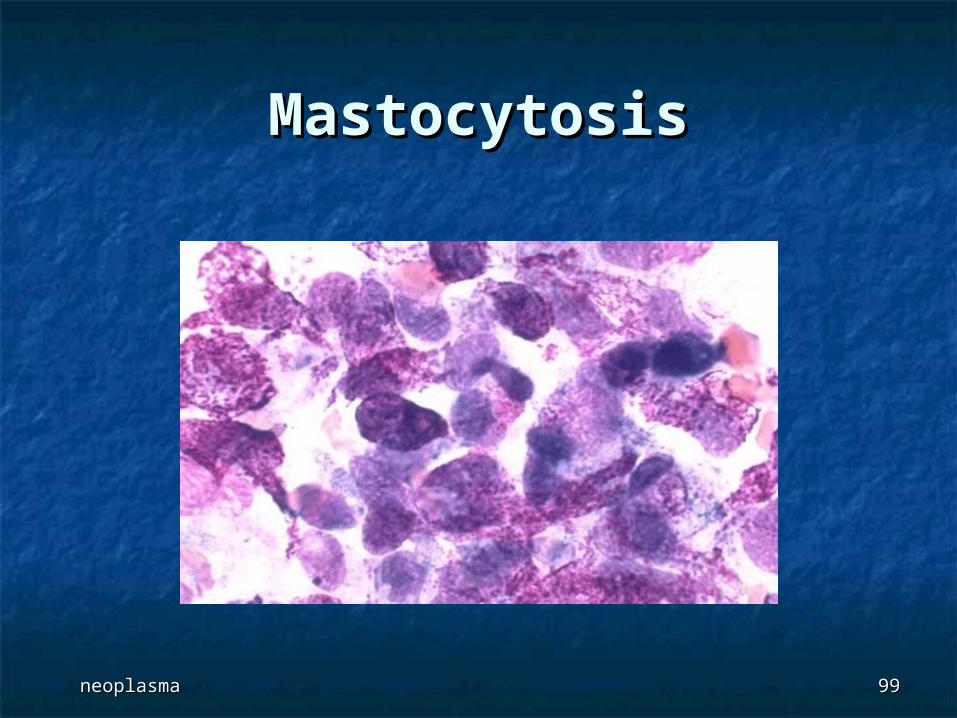
Mastocytosis (MC) is a rare, Mastocytosis (MC) is a rare, heterogeneous disorder, heterogeneous disorder, characterized by a marked increase in characterized by a marked increase in mast mast
cellscells in the skin and occasionally in the bone in the skin and occasionally in the bone marrow, liver, spleen, gastrointestinal tract, marrow, liver, spleen, gastrointestinal tract, and other various organ systems. and other various organ systems.
Mast cells are produced in the bone marrow Mast cells are produced in the bone marrow and contain and contain mediators for inflammatorymediators for inflammatory and and allergenic responses. When these cells are allergenic responses. When these cells are triggered, a degranulation event occurs in triggered, a degranulation event occurs in which mediators such as histamine, which mediators such as histamine, prostaglandins, leukotrienes, heparin, prostaglandins, leukotrienes, heparin, tryptase, and other chemicals are released tryptase, and other chemicals are released from the mast cell and into the systemic from the mast cell and into the systemic circulationcirculation
MastocytosisMastocytosis
neoplasmaneoplasma 9797
cutaneous mastocytosis is generally cutaneous mastocytosis is generally benign in children benign in children
urticaria pigmentosa (UP) is the most urticaria pigmentosa (UP) is the most common clinical form though common clinical form though descriptions of this entity should be descriptions of this entity should be expanded to include nodular forms. expanded to include nodular forms.
In childhood, in the absence of In childhood, in the absence of clinical symptoms suggesting clinical symptoms suggesting systemic involvement, detailed systemic involvement, detailed laboratory investigations are not laboratory investigations are not recommended.recommended.
MastocytosisMastocytosis
neoplasmaneoplasma 9898
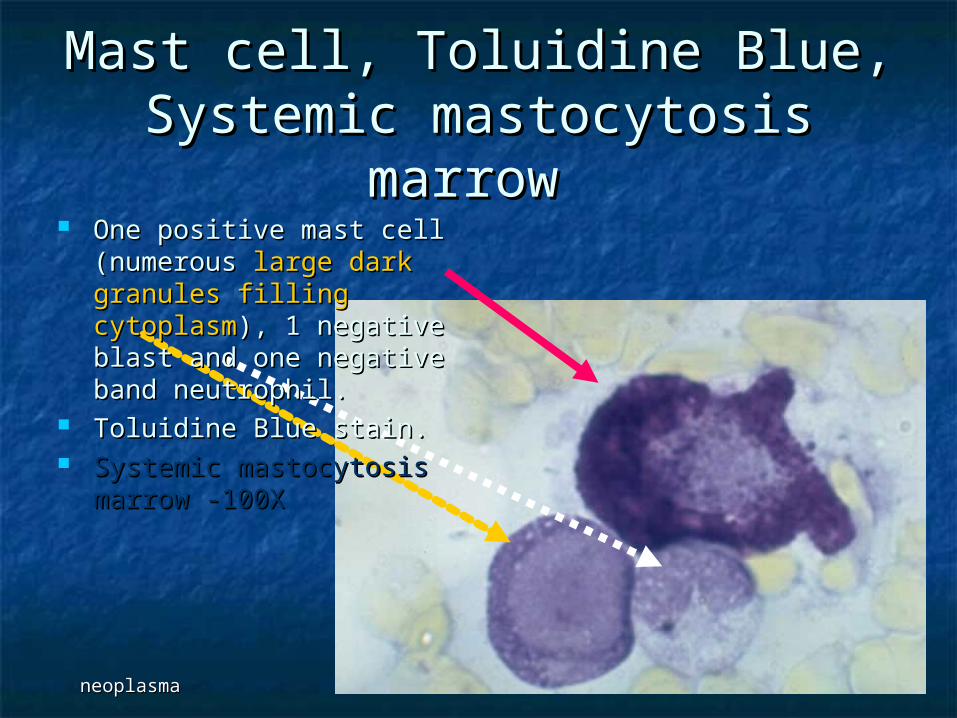
Mast cell, Toluidine Blue, Mast cell, Toluidine Blue, Systemic mastocytosis marrow Systemic mastocytosis marrow
One positive mast cell One positive mast cell (numerous (numerous large dark large dark granules filling cytoplasmgranules filling cytoplasm), ), 1 negative blast and one 1 negative blast and one negative band neutrophil. negative band neutrophil.
Toluidine Blue stain. Toluidine Blue stain. Systemic mastocytosis Systemic mastocytosis
marrow -100Xmarrow -100X
neoplasmaneoplasma 9999
MastocytosisMastocytosis
neurofibromatosis
neoplasmaneoplasma 101101
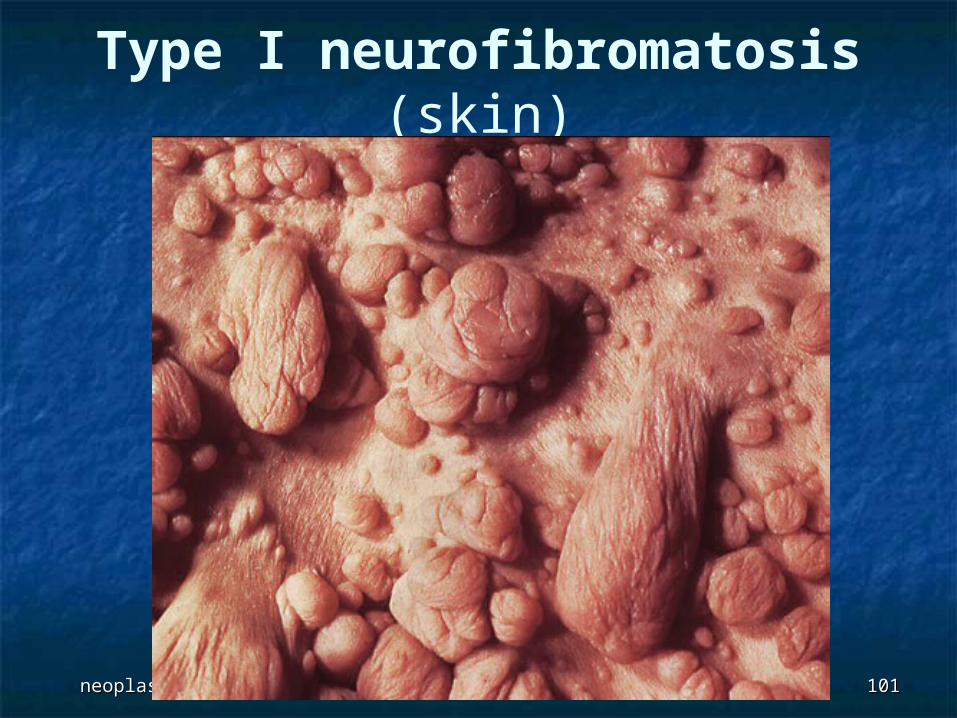
Type I neurofibromatosis (skin)
neoplasmaneoplasma 102102
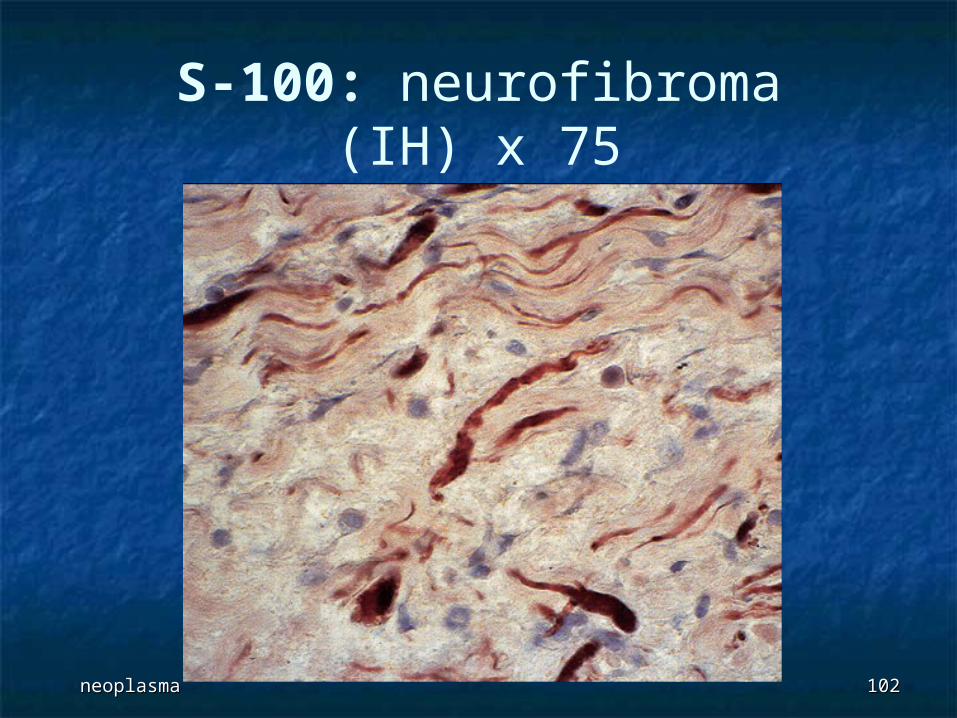
S-100: neurofibroma(IH) x 75