Embed Size (px)
Citation preview

Targeting Angiogenesis in the Treatment of Advanced-Stage Breast Cancer Breast cancer development and metasta-sis is dependent on the formation of new vasculature, making tumor angiogenesis a rational target for therapeutic interven-tion. Currently, several antiangiogenesis strategies are being evaluated in patients with metastatic breast cancer (MBC), and data from 3 trials were presented at the 28th Annual San Antonio Breast Cancer Symposium. The 2 primary strategies undergoing clinical investigation involve using agents specifically targeting vas-cular endothelial growth factor (VEGF), a key mediator of angiogenesis, or using receptor tyrosine kinase inhibitors which target VEGF receptors as well as other growth factor signaling pathways. Miller et al presented the results of the second interim analysis of E2100, a randomized phase III trial that compared the efficacy of weekly paclitaxel in combi-nation with bevacizumab, a humanized monoclonal antibody targeting VEGF, with paclitaxel alone in patients with previously untreated MBC.1 Results demonstrated that the addition of beva-cizumab to paclitaxel produced a sig-nificantly higher overall response rate (ORR) of 30% compared with 14% for the paclitaxel alone arm (P < 0.0001). Progression-free survival (PFS) was also significantly improved in the paclitaxel/
bevacizumab arm (median time to pro-gression, 11.4 months vs. 6.11 months; hazard ratio [HR], 0.51; P < 0.0001). A higher incidence of grade 3/4 adverse events, including hypertension (< 16% vs. 2%), bleeding (< 3% vs. 0), and pro-teinuria (2% vs. 0), was reported in the paclitaxel/bevacizumab arm. Burstein et al presented the results of a multicenter phase II trial that evaluated the efficacy of metronomic chemotherapy alone or in combination with bevacizumab in patients with advanced-stage breast cancer.2 Metronomic chemotherapy refers to administration of drugs in small doses on a frequent schedule for prolonged peri-ods. Preclinical data show that metronom-ic chemotherapy inhibits tumor growth primarily through antiangiogenic effects while simultaneously minimizing toxic-ity. In contrast, standard chemotherapy
entails administering drugs on a bolus schedule at maximum tolerated doses that necessitate breaks between treatments, potentially permitting repair of tumor microvasculature and tumor regrowth.3 The growth inhibitory effects of metro-nomic chemotherapy have been demon-strated extensively in preclinical tumor models and is now actively being investi-gated in the clinical setting.4,5 The present study is based on preclinical evidence that the efficacy of metronomic chemotherapy could be further improved upon combina-tion with an antiangiogenic agent.6 Eligible patients (N = 55) with stage IV breast cancer and no previous cyclophos-phamide or methotrexate or angiogenesis inhibitor therapy were enrolled in the study (Figure 1). Patients were random-ized to receive metronomic chemotherapy alone with cyclophosphamide/methotrex-
highlightsmeeting
Prepared by: Aarati Ranganathan, PhD; Sabeeha Muneer, PhD Reviewed by: Joyce A. O’Shaughnessy, MD
2005Highlights From:
The 28th Annual San AntonioBreast Cancer Symposium
San Antonio, TXDecember 2005
Figure 1: Metronomic Chemotherapy with or Without Bevacizumab in Advanced-Stage Breast Cancer: Treatment Schema
Metronomic CM
Cyclophosphamide(50 mg orally every day)
Methotrexate(2.5 mg orally twice a day
on days 1 and 2 every week)
Metronomic CM plus Bevacizumab
Cyclophosphamide50 mg orally every day
Methotrexate(2.5 mg orally twice a day
on days 1 and 2 every week)Bevacizumab
10 mg/kg intravenously every 14 days
• Stage IV breast cancer with metastasis
• Hormone receptor–positiveor hormone receptor–
negative disease• No previous chemotherapy,
oral cyclophosphamide or methotrexate, or angiogenesis
inhibitor therapy for MBC
Eligibility Criteria:
N = 55
RANDOMIZE
16 • Clinical Breast Cancer April 2006
MH 7.1.indd 2 5/4/06 9:04:18 AM
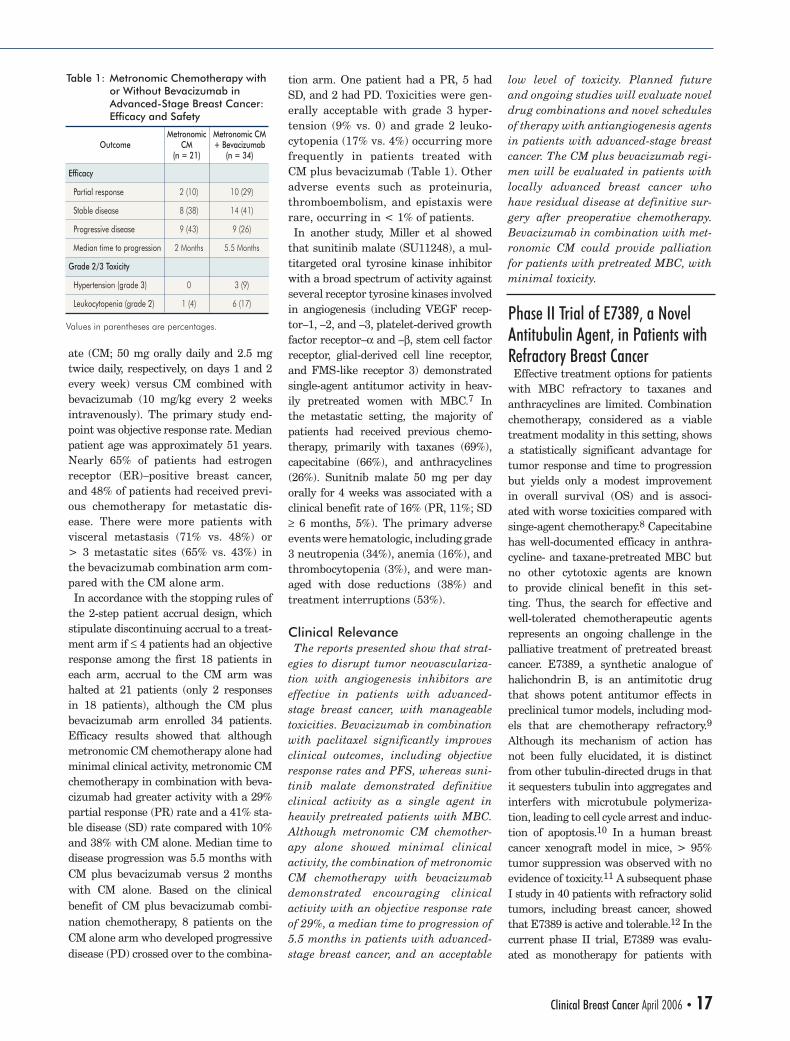
ate (CM; 50 mg orally daily and 2.5 mg twice daily, respectively, on days 1 and 2 every week) versus CM combined with bevacizumab (10 mg/kg every 2 weeks intravenously). The primary study end-point was objective response rate. Median patient age was approximately 51 years. Nearly 65% of patients had estrogen receptor (ER)–positive breast cancer, and 48% of patients had received previ-ous chemotherapy for metastatic dis-ease. There were more patients with visceral metastasis (71% vs. 48%) or > 3 metastatic sites (65% vs. 43%) in the bevacizumab combination arm com-pared with the CM alone arm. In accordance with the stopping rules of the 2-step patient accrual design, which stipulate discontinuing accrual to a treat-ment arm if ≤ 4 patients had an objective response among the first 18 patients in each arm, accrual to the CM arm was halted at 21 patients (only 2 responses in 18 patients), although the CM plus bevacizumab arm enrolled 34 patients. Efficacy results showed that although metronomic CM chemotherapy alone had minimal clinical activity, metronomic CM chemotherapy in combination with beva-cizumab had greater activity with a 29% partial response (PR) rate and a 41% sta-ble disease (SD) rate compared with 10% and 38% with CM alone. Median time to disease progression was 5.5 months with CM plus bevacizumab versus 2 months with CM alone. Based on the clinical benefit of CM plus bevacizumab combi-nation chemotherapy, 8 patients on the CM alone arm who developed progressive disease (PD) crossed over to the combina-
tion arm. One patient had a PR, 5 had SD, and 2 had PD. Toxicities were gen-erally acceptable with grade 3 hyper-tension (9% vs. 0) and grade 2 leuko-cytopenia (17% vs. 4%) occurring more frequently in patients treated with CM plus bevacizumab (Table 1). Other adverse events such as proteinuria, thromboembolism, and epistaxis were rare, occurring in < 1% of patients. In another study, Miller et al showed that sunitinib malate (SU11248), a mul-titargeted oral tyrosine kinase inhibitor with a broad spectrum of activity against several receptor tyrosine kinases involved in angiogenesis (including VEGF recep-tor–1, –2, and –3, platelet-derived growth factor receptor–α and –β, stem cell factor receptor, glial-derived cell line receptor, and FMS-like receptor 3) demonstrated single-agent antitumor activity in heav-ily pretreated women with MBC.7 In the metastatic setting, the majority of patients had received previous chemo-therapy, primarily with taxanes (69%), capecitabine (66%), and anthracyclines (26%). Sunitnib malate 50 mg per day orally for 4 weeks was associated with a clinical benefit rate of 16% (PR, 11%; SD ≥ 6 months, 5%). The primary adverse events were hematologic, including grade 3 neutropenia (34%), anemia (16%), and thrombocytopenia (3%), and were man-aged with dose reductions (38%) and treatment interruptions (53%).
Clinical Relevance The reports presented show that strat-egies to disrupt tumor neovasculariza-tion with angiogenesis inhibitors are effective in patients with advanced-stage breast cancer, with manageable toxicities. Bevacizumab in combination with paclitaxel significantly improves clinical outcomes, including objective response rates and PFS, whereas suni-tinib malate demonstrated definitive clinical activity as a single agent in heavily pretreated patients with MBC. Although metronomic CM chemother-apy alone showed minimal clinical activity, the combination of metronomic CM chemotherapy with bevacizumab demonstrated encouraging clinical activity with an objective response rate of 29%, a median time to progression of 5.5 months in patients with advanced-stage breast cancer, and an acceptable
low level of toxicity. Planned future and ongoing studies will evaluate novel drug combinations and novel schedules of therapy with antiangiogenesis agents in patients with advanced-stage breast cancer. The CM plus bevacizumab regi-men will be evaluated in patients with locally advanced breast cancer who have residual disease at definitive sur-gery after preoperative chemotherapy. Bevacizumab in combination with met-ronomic CM could provide palliation for patients with pretreated MBC, with minimal toxicity.
Phase II Trial of E7389, a Novel Antitubulin Agent, in Patients with Refractory Breast Cancer Effective treatment options for patients with MBC refractory to taxanes and anthracyclines are limited. Combination chemotherapy, considered as a viable treatment modality in this setting, shows a statistically significant advantage for tumor response and time to progression but yields only a modest improvement in overall survival (OS) and is associ-ated with worse toxicities compared with singe-agent chemotherapy.8 Capecitabine has well-documented efficacy in anthra-cycline- and taxane-pretreated MBC but no other cytotoxic agents are known to provide clinical benefit in this set-ting. Thus, the search for effective and well-tolerated chemotherapeutic agents represents an ongoing challenge in the palliative treatment of pretreated breast cancer. E7389, a synthetic analogue of halichondrin B, is an antimitotic drug that shows potent antitumor effects in preclinical tumor models, including mod-els that are chemotherapy refractory.9 Although its mechanism of action has not been fully elucidated, it is distinct from other tubulin-directed drugs in that it sequesters tubulin into aggregates and interfers with microtubule polymeriza-tion, leading to cell cycle arrest and induc-tion of apoptosis.10 In a human breast cancer xenograft model in mice, > 95% tumor suppression was observed with no evidence of toxicity.11 A subsequent phase I study in 40 patients with refractory solid tumors, including breast cancer, showed that E7389 is active and tolerable.12 In the current phase II trial, E7389 was evalu-ated as monotherapy for patients with
Table 1: Metronomic Chemotherapy with or Without Bevacizumab in Advanced-Stage Breast Cancer: Efficacy and Safety
Efficacy
Partial response
Stable disease
Progressive disease
Median time to progression
Grade 2/3 Toxicity
Hypertension (grade 3)
Leukocytopenia (grade 2)
OutcomeMetronomic
CM(n = 21)
2 (10)
8 (38)
9 (43)
2 Months
0
1 (4)
Metronomic CM+ Bevacizumab
(n = 34)
10 (29)
14 (41)
9 (26)
5.5 Months
3 (9)
6 (17)
Values in parentheses are percentages.
Clinical Breast Cancer April 2006 • 17
MH 7.1.indd 3 5/4/06 9:04:19 AM

anthracyline- and taxane-refractory breast cancer, the results of which were presented by Silberman et al at the 28th Annual San Antonio Breast Cancer Symposium and are summarized herein.13 In this phase II trial, eligible patients must have progressed on or within 6 months of receiving ≥ 2 previous chemotherapy regimens and must have been previously treated with an anthracycline and taxane. The treatment strategy was to administer a bolus dose of E7389 1.4 mg/m2 intrave-nously on days 1, 8, 15 of a 28-day cycle. However, the incidence of neutropenia on day 15 of the 28-day cycle required dose delays, necessitating the treatment of a new cohort of patients with a sched-ule of 1.4 mg/m2 on days 1 and 8 of a 21-day cycle. The primary endpoint was response rate. Because expression levels of β-tubulin isotypes have previously been associated with the sensitivity of breast cancer cell lines to E7389,14 a secondary objective of the study was to correlate expression of β-tubulin iso-types and related proteins with ORR (results are not reported here). The study accrued 71 patients in the 28-day cycle cohort and 33 patients in the 21-day cycle cohort. The median age of the study population was 54 years (range, 36-73 years). A majority (69%) of patients had received 4-14 previous chemother-apy regimens, whereas the other 31% had received 2-3 previous chemotherapy regimens, and 50% had received previous hormonal therapy. All patients had previ-ously received treatment with anthracy-cline- and taxane-based regimens. The baseline tumor histology showed that 66% of tumors were ER-positive, 36% were progesterone receptor (PgR)–posi-tive, and 9% were HER2 overexpressing, whereas 30% of tumors were ER, PgR, and HER2 negative. Myelosuppression was the major toxicity found to be associated with the admin-istration of E7389 in this study. Of the 48 patients in the 28-day cycle cohort assessed for safety, 22 patients (46%) expe-rienced grade 3/4 neutropenia with associ-ated febrile neutropenia in 2 patients (Table 2).13 Grade 3 dyspnea was noted in 4 patients, with 1 patient experiencing grade 4 toxicity. Other grade 3 toxicities included dehydration (8%), fatigue (2%), and arthralgias (4%). Peripheral grade 3 neuropathy was noted in 2 patients.
Initial tolerability assessments in the 26 patients in the 21-day cycle cohort who had completed ≥ 1 cycle treatment showed that 21 patients (81%) had an absolute neutrophil count (ANC) > 1000/μL on day 8, whereas on day 15, 46% of patients showed an ANC > 1000/μL and 8 patients required filgrastim support (Table 3).13 In treatment cycle 2, 18 of 20 patients (90%) had an ANC > 1000/μL on day 8, whereas 30% of patients showed an ANC > 1000/μL on day 15. At the time of this preliminary report, no dose modifica-tions had been required in patients on the 21-day cycle. In contrast, only 37% patients on the 28-day cycle did not need dose delays and/or adjustments, and 38% required leukocyte growth factor support during the first 2 cycles. Twelve of 65 evaluable patients on the 28-day cycle cohort showed a PR (18.5%), 2 of which are yet to be confirmed, with duration of response ranging from ≥ 55 days to ≥ 183 days. No complete responses have been reported. Further, disease stabi-lization was observed in 21 patients, whereas 32 patients had PD. The median PFS was 7 weeks. Efficacy data from patients treated with the 21-day schedule are pending.
Clinical Relevance In this phase II study, preliminary efficacy analysis showed that E7389 monotherapy is active in patients with
anthracycline- and taxane-pretreated MBC with an ORR of 19%. No other cytotoxic agent has demonstrated this degree of antitumor activity in this heavily pretreated population. However, significant hematologic toxicities neces-sitated modification of the 28-day treat-ment schedule. The optimized 21-day cycle appears to be better tolerated, and the delivery of E7389 on the day 1 and 8 schedule appears feasible over the first 2 cycles of therapy. Grade 3/4 neutropenia was observed in 46% of patients on the 28-day cycle cohort, although neurotox-icity, commonly associated with tubulin-targeting agents, was infrequent (grade 3, 4%). Further analysis of this study will include evaluation of the associa-tion of β-tubulin isotypes with response to therapy. Based on these results, addi-tional studies evaluating the efficacy and safety of E7389 monotherapy in patients with newly diagnosed and refractory breast cancer are warranted.
ABCSG 8 Trial: Five-Year Follow-upof an Adjuvant Anastrozole Switching Trial in Postmenopausal Women with Hormone-Responsive Early-Stage Breast Cancer In recent years, results from a num-ber of clinical trials have demonstrated superior disease-free survival with the inclusion of aromatase inhibitors (AIs) in adjuvant regimens versus tamoxifen alone in postmenopausal women with early-stage breast cancer.15-19 However, the designs of these trials differ in the treatment strategies used and the char-acteristics of patients included. For instance, the Arimidex®, Tamoxifen, Alone or in Combination (ATAC) trial
Table 2: Efficacy and Safety of E7389 Monotherapy in the 28-Day Cycle Cohort of Patients with Refractory Breast Cancer13
Safety (n = 48)*
Neutropenia
Febrile neutropenia
Dyspnea
Leukopenia
Dehydration
Neuropathy
Efficacy (n = 65)
Partial response
Stable disease
Progressive disease
Outcome
Grade 3
11 (23)
2 (4)
4 (8)
5 (10)
4 (8)
2 (4)
12 (19)
21 (32)
32 (49)
Grade 4
11 (23)
0
1 (2)
0
0
0
–
–
–
Number of Patients (%)
*Toxicity-induced dose reductions and/or delays were required in 63% of patients treated with E7389 on days 1, 8, and 15 on the 28-day cycle.
Table 3: Tolerability of E7389 Monotherapy in the 21-Day Cycle Cohort of Patients with Refractory Breast Cancer*13
Cycle 1 (n = 26)
Day 8
Day 15
Cycle 2 (n = 20)
Day 8
Day 15
Treatment Cycle
21 (81)
12 (46)
18 (90)
6 (30)
Number of Patients (%)
*ANC values > 1000/μL.
Meeting Highlights
18 • Clinical Breast Cancer April 2006
MH 7.1.indd 4 5/4/06 9:04:19 AM
compared primary adjuvant therapy with anastrozole versus tamoxifen for 5 years; the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, Arimidex®/Nolvadex® (ARNO) 95, and the Intergroup Exemestane Study (IES) compared switching to an AI from tamox-ifen with tamoxifen alone for 5 years; the MA.17 trial evaluated extending adjuvant therapy with letrozole after 5 years of tamoxifen; and the Breast International Group (BIG) 1-98 trial is comparing adju-vant therapy with letrozole alone, tamox-ifen alone, letrozole followed by tamoxi-fen, or tamoxifen followed by letrozole for 5 years. Although the benefit of AI therapy was observed in all the trials, the magnitude of benefit appears to vary between strategies. In the ABCSG 8 and ARNO 95 trials, patients received tamoxifen treatment for 2-3 years followed by anastrozole or continued on tamoxifen, to complete a total of 5 years of adjuvant endo-crine therapy.16 At a median follow-up of 28 months, the combined analysis data from these trials were reported. In the combined analysis, only events occurring after the switch were included.
However, in the ABCSG trial 8, random-ization occurred before the initiation of any endocrine therapy, allowing analysis of events occurring at any point during the adjuvant regimen. An update on the data from the ABCSG 8 trial after 3 years of therapy after switching to anastrozole versus continu-ing on tamoxifen and an analysis of all events occurring from the time of initial randomization were presented by Jakesz et al at the 28th Annual San Antonio Breast Cancer Symposium in 2005.20
Postmenopausal women (aged ≤ 80 years) with G1,2,x breast cancer who had ER- or PgR-positive disease were enrolled in this study. No previous chemotherapy was allowed. Patients were randomized at the time of entry to receive tamoxifen (20 mg daily) for 5 years or tamoxifen for 2 years followed by anastrozole (1 mg daily) for 3 years. The primary endpoint was event-free survival (EFS). Secondary endpoints included distant recurrence–free survival, OS, and adverse events. Of the 2926 patients treated, 1454 received tamoxifen and 1472 received tamoxifen followed by anastrozole. Seventy-four percent of patients had
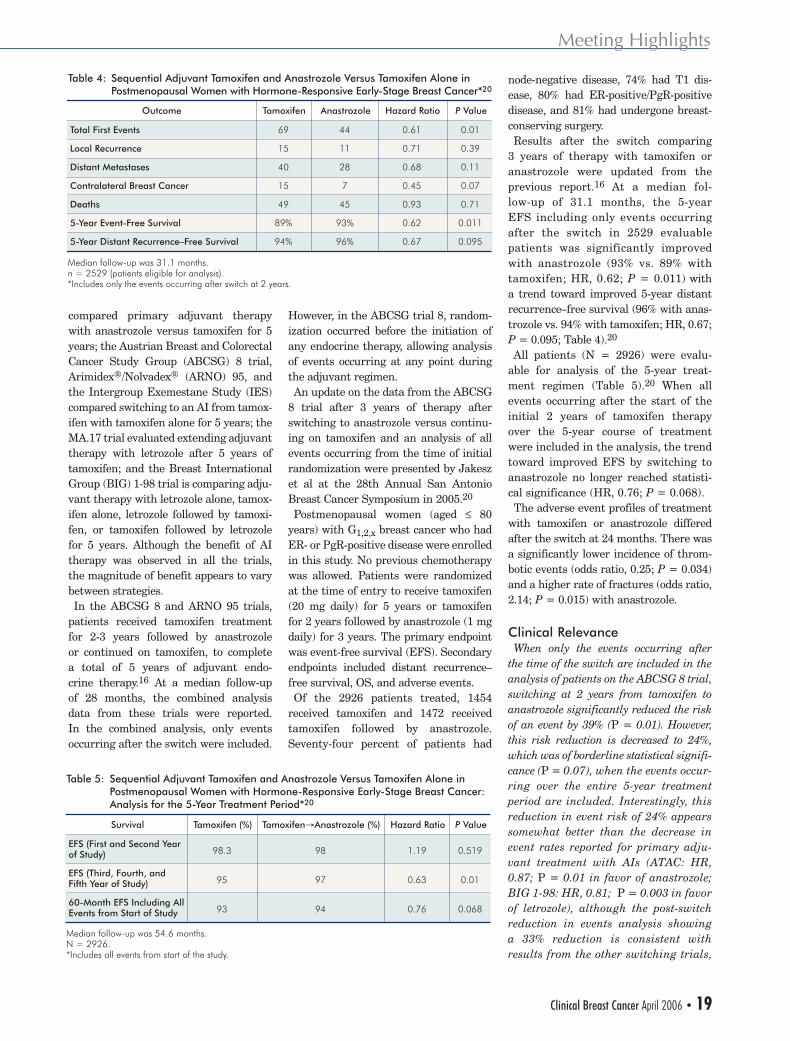
node-negative disease, 74% had T1 dis-ease, 80% had ER-positive/PgR-positive disease, and 81% had undergone breast-conserving surgery. Results after the switch comparing 3 years of therapy with tamoxifen or anastrozole were updated from the previous report.16 At a median fol-low-up of 31.1 months, the 5-year EFS including only events occurring after the switch in 2529 evaluable patients was significantly improved with anastrozole (93% vs. 89% with tamoxifen; HR, 0.62; P = 0.011) with a trend toward improved 5-year distant recurrence–free survival (96% with anas-trozole vs. 94% with tamoxifen; HR, 0.67; P = 0.095; Table 4).20 All patients (N = 2926) were evalu-able for analysis of the 5-year treat-ment regimen (Table 5).20 When all events occurring after the start of the initial 2 years of tamoxifen therapy over the 5-year course of treatment were included in the analysis, the trend toward improved EFS by switching to anastrozole no longer reached statisti-cal significance (HR, 0.76; P = 0.068). The adverse event profiles of treatment with tamoxifen or anastrozole differed after the switch at 24 months. There was a significantly lower incidence of throm-botic events (odds ratio, 0.25; P = 0.034) and a higher rate of fractures (odds ratio, 2.14; P = 0.015) with anastrozole.
Clinical Relevance When only the events occurring after the time of the switch are included in the analysis of patients on the ABCSG 8 trial, switching at 2 years from tamoxifen to anastrozole significantly reduced the risk of an event by 39% (P = 0.01). However, this risk reduction is decreased to 24%, which was of borderline statistical signifi-cance (P = 0.07), when the events occur-ring over the entire 5-year treatment period are included. Interestingly, this reduction in event risk of 24% appears somewhat better than the decrease in event rates reported for primary adju-vant treatment with AIs (ATAC: HR, 0.87; P = 0.01 in favor of anastrozole; BIG 1-98: HR, 0.81; P = 0.003 in favor of letrozole), although the post-switch reduction in events analysis showing a 33% reduction is consistent with results from the other switching trials,
Table 4: Sequential Adjuvant Tamoxifen and Anastrozole Versus Tamoxifen Alone in Postmenopausal Women with Hormone-Responsive Early-Stage Breast Cancer*20
Total First Events
Local Recurrence
Distant Metastases
Contralateral Breast Cancer
Deaths
5-Year Event-Free Survival
5-Year Distant Recurrence–Free Survival
Outcome
69
15
40
15
49
89%
94%
Tamoxifen
44
11
28
7
45
93%
96%
Anastrozole
0.61
0.71
0.68
0.45
0.93
0.62
0.67
Hazard Ratio
0.01
0.39
0.11
0.07
0.71
0.011
0.095
P Value
Median follow-up was 31.1 months.n = 2529 (patients eligible for analysis).*Includes only the events occurring after switch at 2 years.
Table 5: Sequential Adjuvant Tamoxifen and Anastrozole Versus Tamoxifen Alone in Postmenopausal Women with Hormone-Responsive Early-Stage Breast Cancer: Analysis for the 5-Year Treatment Period*20
EFS (First and Second Year of Study)
EFS (Third, Fourth, and Fifth Year of Study)
60-Month EFS Including All Events from Start of Study
Survival
98
97
94
Tamoxifen→Anastrozole (%)
98.3
95
93
Tamoxifen (%)
1.19
0.63
0.76
Hazard Ratio
0.519
0.01
0.068
P Value
Median follow-up was 54.6 months.N = 2926.*Includes all events from start of the study.
Meeting Highlights
Clinical Breast Cancer April 2006 • 19
MH 7.1.indd 5 5/4/06 9:04:20 AM
such as IES (HR, 0.6; P < 0.001 in favor of exemestane).15,17,19 These dif-ferences likely reflect differences in the patient populations, because patients with more aggressive disease that recurs during the first year or 2 have been excluded from the post-tamoxi-fen switching trials. Thus, it is not possible, based on currently available data, to determine the comparative effi-cacy of upfront treatment with an AI versus switching to an AI after an ini-tial period of tamoxifen. Results from studies such as BIG 1-98 and TEAM, which are directly comparing upfront AI therapy to tamoxifen-AI sequenc-ing strategies, will aid in determining the optimal strategy for the adjuvant endocrine treatment of various subsets postmenopausal women with hormone receptor–positive disease.
Subgroup Analysis of Oral Clodronate Therapy on Bone Turnover and Skeletal Metastasis in Patients with Primary Breast Cancer Bone is the most common site of metas-tasis in breast cancer. Activation of osteo-clastic bone resorption by paracrine fac-tors released by the tumor cells is the predominant mechanism of bone loss and adverse skeletal-related events of bone metastasis.21 Moreover, breast can-cer treatment such as hormonal therapy and chemotherapy can lead to accelera-tion of this process.22 Bisphosphonates are potent inhibitors of osteoclastic bone resorption and have effectively been used to reduce bone loss and progression of bone metastasis in advanced-stage breast cancer.23,24 In the adjuvant early-stage breast cancer setting, the potential ben-efit of bisphosphonate use is still unclear, with contradictory results obtained from clinical trials. Jaschke et al, at a follow-up of 8.5 years, showed that adjuvant clo-dronate treatment significantly improved OS (P < 0.01) in patients with primary breast cancer and micrometastasis to bone marrow.25,26 In contrast, Saarto et al showed no effect of clodronate treat-ment on the development of bone metas-tasis and a deleterious effect on OS and disease-free survival as a result of the incidence of nonskeletal metastasis.27
In a randomized, double-blind, pla-cebo-controlled study, 1069 assessable patients with operable stage I-III breast cancer were randomized to receive 2 years of oral clodronate (1600 mg per day) or placebo after appropriate pri-mary therapy (surgery, chemotherapy, radiation therapy, and hormonal thera-py). During the 5-year study period, clo-dronate therapy significantly reduced the risk of occurrence of bone metastases by 31% (HR, 0.692; P = 0.043) and improved OS by 23% (HR, 0.768; P = 0.048) in all patients compared with placebo.28 In the current study, the relationship between bone turnover response and incidence of bone metastases was ana-lyzed in a subset of 555 patients, the results of which were presented by McCloskey et al at the 28th Annual San Antonio Breast Cancer Symposium and are summarized herein.29
In this subgroup analysis, serum levels of amino-terminal propeptide of type I colla-gen (PINP), a marker of bone turnover, at baseline showed that PINP levels were identical in the clodronate and pla-cebo treatment groups. However, during the 2-year clodronate therapy, a 26% decrease in the median PINP level was observed in patients receiving clodro-nate compared with a 5% increase in the placebo group (P < 0.0001). The PINP levels returned to baseline within 1 year of discontinuing clodronate ther-apy. There was a trend toward higher median PINP values in postmenopausal women than in premenopausal women that did not reach statistical significance (37 mg/L vs. 34.5 mg/L; P = 0.07). Based on percentage changes between baseline and 1 year, patients were clas-sified into 3 bone turnover groups based
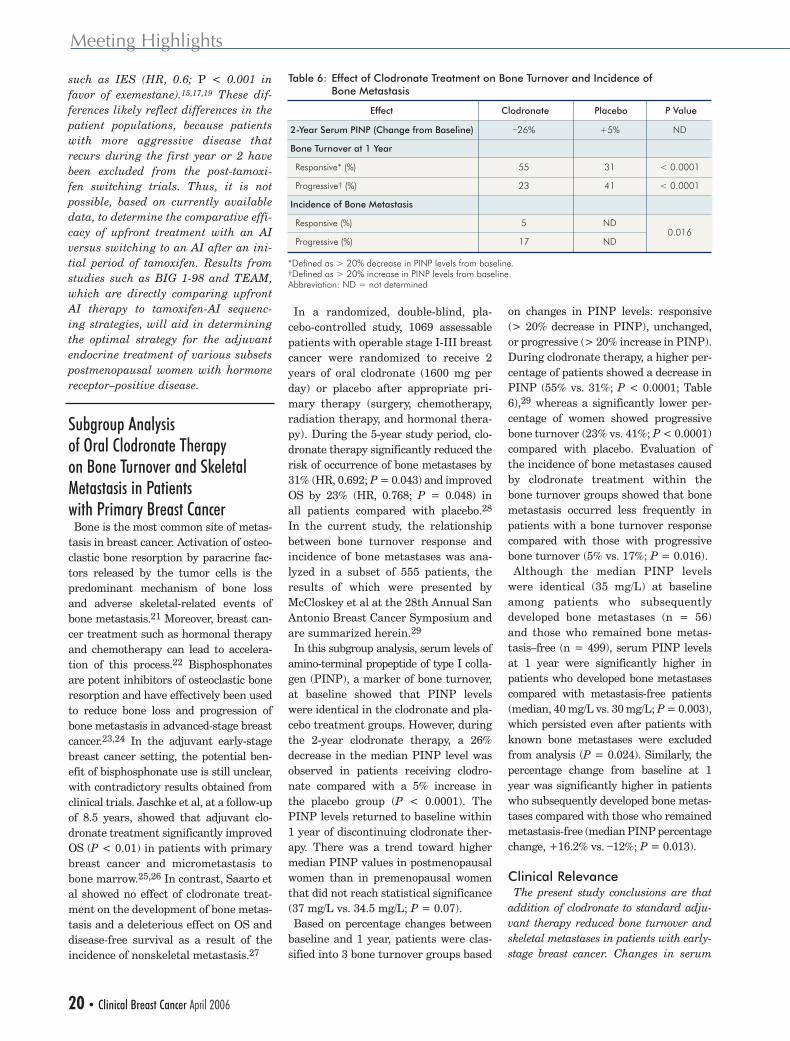
on changes in PINP levels: responsive (> 20% decrease in PINP), unchanged, or progressive (> 20% increase in PINP). During clodronate therapy, a higher per-centage of patients showed a decrease in PINP (55% vs. 31%; P < 0.0001; Table 6),29 whereas a significantly lower per-centage of women showed progressive bone turnover (23% vs. 41%; P < 0.0001) compared with placebo. Evaluation of the incidence of bone metastases caused by clodronate treatment within the bone turnover groups showed that bone metastasis occurred less frequently in patients with a bone turnover response compared with those with progressive bone turnover (5% vs. 17%; P = 0.016). Although the median PINP levels were identical (35 mg/L) at baseline among patients who subsequently developed bone metastases (n = 56) and those who remained bone metas-tasis–free (n = 499), serum PINP levels at 1 year were significantly higher in patients who developed bone metastases compared with metastasis-free patients (median, 40 mg/L vs. 30 mg/L; P = 0.003), which persisted even after patients with known bone metastases were excluded from analysis (P = 0.024). Similarly, the percentage change from baseline at 1 year was significantly higher in patients who subsequently developed bone metas-tases compared with those who remained metastasis-free (median PINP percentage change, +16.2% vs. –12%; P = 0.013).
Clinical Relevance The present study conclusions are that addition of clodronate to standard adju-vant therapy reduced bone turnover and skeletal metastases in patients with early-stage breast cancer. Changes in serum
Table 6: Effect of Clodronate Treatment on Bone Turnover and Incidence of Bone Metastasis
2-Year Serum PINP (Change from Baseline)
Bone Turnover at 1 Year
Responsive* (%)
Progressive† (%)
Incidence of Bone Metastasis
Responsive (%)
Progressive (%)
Effect
–26%
55
23
5
17
Clodronate
+5%
31
41
ND
ND
Placebo
ND
< 0.0001
< 0.0001
0.016
P Value
*Defined as > 20% decrease in PINP levels from baseline. †Defined as > 20% increase in PINP levels from baseline.Abbreviation: ND = not determined
Meeting Highlights
20 • Clinical Breast Cancer April 2006
MH 7.1.indd 6 5/4/06 9:04:21 AM

PINP levels were found to correlate with risk of developing skeletal metas-tases in patients treated with clodronate and, thus, might be a potential clinical marker for response to therapy. The role of bisphosphonates in early-stage breast
cancer, the optimal duration of their use, and the optimal timing of initiation are not known and need to be defined before oral bisphosphonates are administered with the goal of reducing the inci-dence of bone metastasis. Randomized
phase III trials including AZURE and National Surgical Breast and Bowel Project B-34 are under way to evaluate the clinical benefit of including zoledro-nate and clodronate, respectively, in the treatment of early-stage breast cancer.
1. Miller KD, Wang M, Gralow J, et al. A randomized phase III trial of paclitaxel versus paclitaxel plus bevacizumab as first-line therapy for locally recurrent or meta-static breast cancer: a trial coordinated by the Eastern Cooperative Oncology Group (E2100). Breast Cancer Res Treat 2005; 94(suppl 1):S6 (Abstract #3).
2. Burstein HJ, Spigel D, Kindsvogel K, et al. Metronomic chemotherapy with and without bevacizumab for advanced breast cancer: a randomized phase II study. Breast Cancer Res Treat 2005; 94(suppl 1):S6 (Abstract #4).
3. Kerbel RS, Kamen BA. The anti-angiogenic basis of metronomic chemotherapy. Nat Rev Cancer 2004; 4:423-436.
4. Nicolini A, Mancini P, Ferrari P, et al. Oral low-dose cyclophosphamide in meta-static hormone refractory prostate cancer (MHRPC). Biomed Pharmacother 2004; 58:447-450.
5. Colleoni M, Rocca A, Sandri MT, et al. Low dose oral methotrexate and cyclophospha-mide in metastatic breast cancer: antitu-mor activity and correlation with vascular endothelial growth factor levels. Ann Oncol 2002; 13:73-80.
6. Klement G, Baruchel S, Rak J, et al. Continuous low-dose therapy with vinblas-tine and VEGF receptor-2 antibody induces sustained tumor regression without overt toxicity. J Clin Investig 2000; 105:R15-R24.
7. Miller KD, Burstein HJ, Elias AD, et al. Phase II study of SU11248, a multitargeted tyro-sine kinase inhibitor (TKI) in patients (pts) with previously treated metastatic breast cancer (MBC). Breast Cancer Res Treat 2005; 94(suppl 1):S61 (Abstract #1066).
8. Carrick S, Parker S, Wilcken N, et al. Single agent versus combination chemotherapy for metastatic breast cancer. Cochrane Database Syst Rev 2005; 2:CD003372.
9. Jordan MA, Kamath K, Manna T, et al. The primary antimitotic mechanism of action of the synthetic halichondrin E7389 is sup-pression of microtubule growth. Mol Cancer Ther 2005; 7:1086-1095.
10. Towle MJ, Salvato KA, Budrow J, et al. In vitro and in vivo anticancer activities of syn-thetic macrocyclic ketone analogues of hali-chondrin B. Cancer Res 2001; 61:1013-1021.
11. Towle MJ, Agoulnik S, Kuznetsov G, et al. In vivo efficacy of E7389, a synthetic analog of the marine sponge antitubulin agent halichondrin B, against human tumor xeno-grafts under monotherapy and combination therapy conditions. Proc Am Assoc Cancer Res 2003; 44:A2749.
12. Synold TW, Morgan RJ, Newman EM, et al. A phase I pharmacokinetic and target vali-dation study of the novel anti-tubulin agent E7389: A California Cancer Consortium Trial. J Clin Oncol 2005; 23:200s (Abstract #3036).
13. Silberman SL, O’Shaughnessy J, Vahdat L, et al. E7389, a novel anti-tubulin, is safe and effective in patients with refrac-tory breast cancer. Proc Am Soc Clin Oncol 2005; 94(suppl 1):S60 (Abstract #1063).
14. Agoulnik S, Kuznetsov G, Tendyke K, et al. Sensitivity to halichondrin analog E7389 and hemiasterlin analog E7974 correlates with ßIII tubulin isotype expression in human breast cancer cell lines. J Clin Oncol 2005; 23:138s (Abstract #2012).
15. The ATAC Trialists group. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. Lancet 2005; 365:60-62.
16. Jakesz R, Jonat W, Gnant M, et al. Switching of postmenopausal women with endocrine-responsive early breast cancer to anastrozole after 2 years’ adjuvant tamoxi-fen: combined results of ABCSG trial 8 and ARNO 95 trial. Lancet 2005; 366:455-462.
17. Coombes RC, Hall E, Gibson LJ, et al. A randomized trial of exemestane after two to three years of tamoxifen therapy in post-menopausal women with primary breast cancer. [Published erratum in N Eng J Med 2004; 351:2461]. N Eng J Med 2004; 350:1081-1092.
18. Goss PE, Ingle JN, Martino S, et al. Randomized trial of letrozole following tamoxifen as extended adjuvant therapy in receptor-positive breast cancer: updated findings from NCIC CTG MA.17. J Natl Cancer Inst 2005; 97:1262-1271.
19. Thurlimann B, Keshaviah A, Coates AS, et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 2005; 353:2747-2757.
20. Jakesz R, Gnant M, Greil R, et al. The benefits of sequencing adjuvant tamoxifen and anastrazole in postmenopausal women with hormone-responsive early breast can-cer: 5 year analysis of ABCSG trial 8. Breast Cancer Res Treat 2005; 94(suppl 1):S10 (Abstract #13).
21. Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportuni-ties. Nature Rev Cancer 2002; 2:584-593.
22. Lipton A. Toward new horizons: the future of bisphosphonate therapy. Oncologist 2004; 9:38-47.
23. Body JJ, Diel IJ, Lichinitzer M, et al. Oral ibandronate reduces the risk of skeletal complications in breast cancer patients with metastatic bone disease: results from two randomized, placebo-controlled phase III studies. Br J Cancer 2004; 90:1133-1137.
24. Pavlakis N, Stockler M. Bisphosphonates for breast cancer. Cochrane Database Syst Rev 2002; 1:CD003474.
25. Jaschke A, Bastert G, Solomayer EF, et al. Adjuvant clodronate treatment improves the overall survival of primary breast can-cer patients with micrometastasis to bone marrow – a longtime follow-up. Proc Am Soc Clin Oncol 2004; 23:9 (Abstract #529).
26. Diel IJ, Solomayer EF, Costa SD, et al. Reduction in new metastasis in breast can-cer with adjuvant clodronate treatment. N Engl J Med 1998; 339:357-363.
27. Saarto T, Bomqvist C, Virkkunen P, et al. Adjuvant clodranate treatment does not reduce the frequency of skeletal metastasis in node-positive breast cancer patients: 5-year results of a randomized controlled trial. J Clin Oncol 2001; 19:10-17.
28. Powles T, McCloskey E, Kurkilahti M, et al. Oral clodronate for adjuvant treatment of operable breast cancer: results of a ran-domized, double-blind, placebo-controlled multicenter trial. Proc Am Soc Clin Oncol 2004; 23:9 (Abstract #528).
29. McCloskey EV, Paterson AHG, Powles TJ. Effects of oral clodronate (BONEFOS) therapy on bone turnover and skeletal metastases in women with primary breast cancer. Breast Cancer Res Treat 2005; 94(suppl 1):S6 (Abstract #43).
References
Meeting Highlights
Clinical Breast Cancer April 2006 • 21
MH 7.1.indd 7 5/4/06 9:04:21 AM