Embed Size (px)
Citation preview

PIGMENT METABOLISM
PRESENTER - Dr SHREYA PRABHU
MODERATOR - Dr ANISHA T S
1

INTRODUCTION
PIGMENTS are colored substances, some of which are normal
constituents of cell, whereas others are abnormal and accumulate
in cells only under special circumstances.
They absorb visible light within a narrow band between 400-800
nm.
Thus pigments greatly differ in origin, chemical constitution, and
biological significance.
They can be organic or inorganic compounds that remain insoluble
in most solvents
2

CLASSIFICATION
A)ENDOGENOUS PIGMENTS
1) HEMATOGENOUS PIGMENTS
a. Hemosiderin
b. Hemoglobin
c. Bilirubin
d. Porphyrins
2) NON HEMATOGENOUS PIGMENTS
a. Melanin
b. Lipofuscins
c. Chromaffin
d. Pseudomelanosis
e. Dubin-Johnson pigment
f. Ceroid-type lipofuscins
g. Hamazaki-Weisenberg bodies
3

B)EXOGENOUS PIGMENTS
Inhaled pigments
Ingested pigments
Injected pigments
C)ARTIFACT PIGMENTS
Formalin
Malaria
Schistosome
Mercury
Chromic oxide
Starch
4

ENDOGENOUS
PIGMENTS
5

HEMOSIDERINS
Hemoglobin derived, GOLDEN YELLOW to BROWN granular intracellular
pigments.
They contain iron in the form of ferric hydroxide that is bound to a protein
framework
Formed by aggregates of ferritin (iron complexed to apoferritin) found
especially within the phagocytes of the bone marrow, spleen, liver where the
break down of senescent RBC takes place.
Excessive storage of hemosiderin(hemosiderosis) occurs in situation where
there is excessive breakdown of red cells or systemic overload of iron
6

7
HEMOSIDEROSIS
LOCALISED GENERALISED
LOCAL TISSUES PARENCHYMAL DEPOSISTS
(Macrophages, fibroblasts, endothelial (Liver, Kidney, Pancreas. Heart, Skin)
cells and alveolar cells) RED CELL DEPOSISTS
(Liver, Spleen, Bone marrow)
Examples: Examples:
1.Hemorrhage in tissues 1.Acquired Hemosiderosis
2.Black eye 2.Hereditary Hemosiderosis
3.Brown induration lung 3.Excessive dietary intake (Bantu’s
4.Infraction disease)

8

DEMONSTRATION OF HEMOSIDERIN AND
IRON
PERLS’ PRUSSIAN BLUE REACTION FOR FERRIC IRON:
Considered to be first classical histochemical reaction.
Treatment with an acid ferrocyanide solution will result in the unmasking of
ferric iron in the form of the hydroxide, Fe(OH)3, by dilute hydrochloric acid.
The ferric iron reacts with a dilute ferrocyanide solution to produce an insoluble
blue compound, ferric ferrocyanide (prussian blue)
FIXATION:
Avoid the use of acid fixatives. Chromates will also interfere with the
preservation of iron
9

10SECTIONS:
Works well on all types of section, including resin
FERROCYANIDE SOLUTION:
1% aqueous potassium ferrocyanide 20 ml
2% aqueous hydrochloric acid 20 ml
Freshly prepared just before use
METHOD:
Take a test and control section to water
Treat sections with the freshly prepared acid ferrocyanide solution for 10-30 minutes
Wash well in distilled water
Lightly stain the nuclei with 0.5% aqueous neutral red or 0.1% nuclear fast red
Wash rapidly in distilled water
Dehydrate, clear, and mount in synthetic resin
RESULTS:
Ferric iron Blue
Nuclei Red

11
A SECTION OF LIVER FROM A PATIENT WITH HEMOCHROMATOSIS
STAINED FOR FERRIC IRON WITH PERLS’METHOD. FERRIC IRON IS
STAINED BLUE

12

LILLIE’S METHOD FOR FERRIC AND FERROUS IRON
Ferric iron dark Prussian blue
Ferrous iron dark Turnbull’s blue
Nuclei Red
HUKILL AND PUTT’S METHOD FOR FERROUS AND
FERRIC IRON
Ferrous iron Red
Nuclei Blue
13

15
A SECTION OF PLACENTA TREATED WITH LILLIE’S METHOD FOR
FERROUS IRON. FERROUS IRON IS STAINED DARK BLUE

HEMOGLOBIN
HEMOGLOBIN is a basic conjugated protein bound to globin and is the red
pigment component, responsible for the transportation of oxygen and carbon
dioxide.
Heme is composed of protoporphyrin, a substance built up from pyrrole rings
and combined with ferrous iron.
Histochemical demonstration of the ferrous iron is only possible if the close
binding in the heme molecules is cleaved
17

As Hb is normally present within red blood cells its
demonstration is not necessary.
Outside its normal position in RBC, Hb may be found free in
areas of recent hemorrhage, in macrophages.
The pathological conditions like casts in the lumen of renal
tubules in cases of hemoglobinuria or active
glomerulonephritis.
18

DEMONSTRATION OF HEMOGLOBIN
Methods demonstrate the enzyme, Hemoglobin peroxidase,
which is reasonably stable and withstands short fixation and
paraffin processing.
This peroxidase activity was demonstrated by the Benzidine-
nitroprusside methods ( Lepehne-Pickworth Benzidine
Trchnique), but because of the carcinogenicity of benzidine, these
methods are not recommended.
Tinctorial method, The amido black technique and the Kiton
red-Almond green technique are worth noting
19

20
LEUCO PATENT BLUE METHOD
Hemoglobin peroxidase Dark Blue
Nuclei Red

BILE PIGMENTS
23

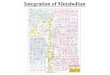
24Heme Biliverdine Bilirubin
(unconjugated)
Bilirubin–albumin complex
(Uptake by liver)
Conjugated
bilirubin Bilirubin-diglucuronide
in intestine Urobilinogen
StercobilinogenUrobilinogen
In kidney
Urobilin
Excretion in urine
Stercobilin
Excretion in feces
20% absorptionEnterohepatic
circulation
80% Intestine
oxygenase
Bilirubin
reductase
Heme
Glucuronyl
transfersae

BILE PIGMENTS
Bilirubin (conjugated+unconjugated), biliverdine, hematoidin-
together refered to as Bile pigments
They are chemically and physically distinct with solubility in
water and alcohol
Bilirubin is the orange-yellow pigment, a toxic waste product
in the body.
It is extracted and biotransformed mainly in the liver, and
excreted in bile and urine.
25

HEMATOIDIN-
Virchow first described in sites of old hemorrhage
Related to bile pigments but differ
Thought that heme has undergone a chemical change within these areas- led to it being trapped- preventing transportation to liver
Extracellular yellow-brown crystals and amorphous masses within old hemorrhagic areas
Microscopically- appear as bright yellow pigment in sections of old splenic infarcts, old hemorrhagic areas of brain or infarcted tissues
26

Microscopical examination of any liver sections that contains bile
pigments will almost certainly reveal a mixture of biliverdine and
both conjugated and unconjugated bilirubin
In H&E stained sections- bile if present-
seen as small yellow brown globules within bile canaliculi- indicating
obstruction
Within hepatocytes (they need to be distinguished from Lipofuscin)
Conditions- Prehepatic/ Hepatic/ Post hepatic
27

28

29
Intracellular
Cholestasis,
Bile pigments in
The cytoplasm
Fig: CHOLESTASIS

30
BILE PLUG (arrow) showing expansion of bile canaliculus by bile

DEMONSTRATION OF BILE PIGMENTS:
Need arises in the histological examination of liver where
distinguishing from lipofuscin is of significance
Both appear yellow-brown in H&E paraffin sections
Bile pigments are not autofluorescent and fail to rotate the
plane of polarized light, whereas Lipofuscin is autofluorescent
Most common method- Modified Fouchet Technique
31

MODIFIED FOUCHET’S (HALL) TECHNIQUE
(FOR LIVER BILE PIGMENTS)
32
RESULTS-
Bile pigments emerald to blue green
Muscle yellow
Collagen red

35

OTHER TECHNIQUES
GMELIN TECHNIQUE-
Only method that shows identical result with liver, gallbladder bile and
hematoidin.
Method- Deparaffinized sections of tissue treated with nitric acid and
changing color spectrum is produced around pigment deposits
Red Purple Green
KUTLIK’S TECHNIQUE-
Method-Sections treated with ferric iron solution
Result- Bilirubin- Green on pale yellow background
36

PORPHYRIN PIGMENTS
Normally occur in tissues in small amounts.
Considered to be precursor of the heme portion of Hb
PORPHYRIAS are rare pathological conditions that are
disorders of the biosynthesis of porphyrins and heme
Found most abundantly in liver
No method for demonstration other than Orange-red
fluorescence which they give with UV light
Porphyrins and bile pigments both give positive Gmelin
reaction
37

Porphyrin pigment-
Appears as dense dark brown pigment
In fresh frozen section exhibits a brilliant red fluorescence
that fades rapidly with exposure to ultraviolet light.
In paraffin sections and viewed using polarized light,
shows as bright red in color with centrally located, dark
maltese cross
38

39

MELANIN
Melanin (melas= black), serves protective function- absorbs UV light
In melanocytes, tyrosine DOPA Melanin
Melanin is the brown-black, non-hemoglobin derived pigment
Skin-
It is synthesised in the melanocytes which are present in the basal cells of the
epidermis
Stored in the form of cytoplasmic granules in the phagocytic cells called the
melanophages in inflammatory conditions, present in the upper dermis
Benign nevus, Malignant melanoma
40
tyrosinase oxidase

Eye-
Found in choroid, ciliary body, iris
Melanomas (rare)
Brain-
In substantia nigra, macroscopically visible as black streak on both sides of
mesencephalon
Also in meninges (sooty appearance)
Parkinson’s disease this area is reduced
41

DISORDERS OF PIGMENTATION
HYPERPIGMENTATION:
GENERALISED- Addison’s disease, Chloasma
FOCAL- Café au lait spots, Peutz jegher’s syndrome (peri oral),
Melanosis coli, Melanotic tumors
HYPOPIGMENTATION:
GENERALISED- Albinism (tyrosinase activity of melanocytes genetically
defective)
FOCAL- Leucoderma ( form of partial albinism), Vitiligo
ACQUIRED FOCAL- leprosy, healing of wounds, DLE, radiation
dermatitis
42

43
PERIORAL HYPERPIGMENTATION

44
ALBINISM VITILIGO
HYPOPIGMENTATION

45

46
MALIGNANT MELANOMA

METHODS FOR MELANIN
Reducing methods- Fontana silver method, Schmrol’s
reaction
Enzyme methods
Fluorescent methods
Immunohistochemistry
Solubility and bleaching characteristics
47

MELANIN AND ITS
PRECURSORS:
Are capable of reducing both
silver and acid ferricyanide
solutions
MELANINS:
Completely insoluble in most
organic solvents
Bleached by strong oxidizing
agents
Powerful reducing agents
48

REDUCING METHODS
PRINCIPLE-
Melanin’s argentaffin property- that is the reduction of
ammonical silver solutions to form metallic silver without the
need for a separate reducing agent.
Melanin is also Argyrophilic, melanin is colored black by
Silver impregnation methods
Reduce ferricyanide to ferrocyanide with production of
Prussian blue in the presence of ferric salts
49

50MASSON-FONTANA METHOD

51
MELANIN PIGMENT IN CELLS OF MALIGNANT MELANOMA,FONTANA-MASSON STAIN

SCHMORL’S REACTION:
Melanin Dark blue
Nuclei Red
LILLIE’S FERROUS ION UPTAKE REACTION:
Melanin Dark green
Nuclei Red
LILLIE’S NILE BLUE METHOD:
Melanin Dark blue
Lipofuscin Dark blue
Nuclei Red
52

SECTION OF SKIN STAINED BY SCHMORL’S REAGENT POSITIVE FOR
MELANIN
53

54

55

ENZYME METHODS
Cells that are capable of producing melanin can be
demonstrated by DOPA method
These methods are those of
Bloch and Laidlaw and Blackberg for tissue sections
Bloch and Rodriguez and McGavran for tissue blocks
58

SOLUBILITY AND BLEACHING METHODS
Melanins are insoluble in organic solvents
Due to tight bound it has with its protein component
Use of strong oxidising agents will bleach melanin (slow, 16
hours)
Method of choice- Peracetic acid
59

FORMALIN-INDUCED FLUORESCENCE
Certain aromatic amines like 5-HT, Dopamine, Epinephrine,
Norepinephrine, Histamine- show yellow fluorescence when
exposed to formaldehyde
Useful when demonstrating Amelanotic melanoma
Results- Melanin precursor cell- Weak yellow fluorescence
60

LIPID PIGMENTS/CHROMOLIPIDS
Have lipid characteristics
These are:
1. Lipofuscins
2. Ceroid
3. Alcoholic hyaline
4. Lipochromes
5. Pseudomelanosis pigment
64

LIPOFUSCINS
Wear and tear pigment/ Brown atrophy pigments/ abnutzung pigments
Produced by oxidation process of lipids and lipoproteins with aging
Yellowish brown intracellular pigment
M/E- coarse golden brown granular pigment, accumulates in central part
of the cells around the nuclei.
These are formed by slow progressive oxidation process, thus reactions
vary according to the degree of oxidation present in the pigment
65

Found in:
Atrophied cells of old age
Hepatocytes
Cardiac muscle cell (brown atrophy of heart)
Inner reticular layer of normal adrenal cortex
Testis, in interstitial cells of Leydig (gives tissue brown color)
Ovary
Edge of cerebral haemorrhage or infarct
66

67

68

69

70

71

DEMONSTRATION OF LIPOFUSCINS
Periodic acid- schiff method
Schmorl’s ferric-ferricyanide reduction test
Long ziehl-Neelsen method
Sudan black B method
Gomori’s aldehyde fuchsin technique
Masson-Fontana silver method
Churukian’s silver method
Lillie’s Nile blue sulfate method
73

74

CEROID
It is a mixture of Lipofuscin like pigment, probably represents it in an
early stage of formation
Occurs in
• Atheroma
• Alcoholic cirrhosis
Occurs as globules of yellow material within macrophages
Differs from lipofuscin by negative Schmorl reaction
Exhibits autofluorescence-
• greenish yellow in frozen sections
• Brownish yellow in paraffin sections
75

ALCOHOLIC HYALIN
Hyaline eosinophilic material, irregular to round mass
(Mallory bodies) near the nuclei of liver cells in chronic
alcoholics
Represent enlarged, distorted, degenerated mitochondria
Affinity towards acid fuchsin and eosin
MALLORY’S HEMALUM-PHLOXINE METHOD-
Alcoholic hyalin- red
Nuclei- blue
76

77

PSEUDOMELANOSIS PIGMENT
Pseudomelanosis condition in which a dark brown, melanin-
like pigment is found in macrophages in the mucosae of the
large bowel and appendix
Stains blue-green in the ferric-ferricyanide reduction test
78

79
PSEUDOMELANOSIS PIGMENT

OTHER ENDOGENOUS PIGMENTS
CHROMAFFIN:
Normally found in adrenal medulla as dark brown, granular material. Occur in
tumors of adrenal medulla- pheochromocytoma
Demonstrated by Schmorl’s reaction, Lillie’s Nile blue A, the Masson-Fontana,
PAS technique
DUBIN-JOHNSON PIGMENT:
Found in liver of patients of Dubin-Johnson syndrome- brownish black, granular,
intracellular pigment, situated in the centrilobular hepatocytes
HAMAZAKI-WEISENBERG BODIES:
Small, yellow brown spindle shaped structures in sinuses of lymph nodes in
patients with sarcoidosis
80

EXOGENOUS PIGMENTS
81

Introduced in the body by- Inhalation /
Ingestion /Inoculation
Broadly classified as
1. Inhaled pigments (Carbon)
2. Ingested pigments (Lead)
3. Injected pigments (Tattooing)
Majority of these pigments are infact colorless, some are
inert and unreactive
82

TATTOO PIGMENT
Tattooing is a form of localized, exogenous pigmentation of the skin.
Pigments like India Ink, Cinnabar, Carbon inocluated are phogocytosed
by dermal macrophages, in which they reside for the remainder of the life.
Pigments do not usually evoke any inflammatory response
Examples-
Tattooing by pricking the skin with dyes
Prolonged use of ointments containing mercury
Dirt left accidently in a wound
83

84

CARBON
Most commonly seen mineral in tissue.
Commonly found in lung and adjacent lymph nodes of urban dwellers and tobacco smokers
MAIN SOURCE- Car exhausts, smoke from domestic and industrial chimneys.
Black pigmentation of the lung (Anthracosis) is result of massive depostion of carbon in coal workers.
Macroscopically lungs appears almost Black. Lung disease is known as Coal workers pneumoconiosis ( found in association with silica found with coal and other mineral ores)
85

86The pigment particles on inhalation are trapped by the thin film of mucus in the nose,
pharynx, trachea and bronchi
Small amount reaches alveoli and taken up by alveolar macrophages
Some of the pigment-laden macrophages are coughed out via bronchi, while some settle in the
interstitial tissue of the lung and in the respiratory bronchioles and pass into lymphatics to be
deposited in the hilar lymph nodes
Carbon is extremely unreactive and inert and fails to be demonstrated with the
conventional histological stains and histochemical methods.
The site and nature of carbon deposits make identification relatively easy.
It may be confused with melanin deposition but treatment with bleaching agents will
show carbon unaffected, whereas melanin will be dissolved.

87
ANTHRACOSIS LUNG

88

SILICA
In the form of silicates is associated with the majority of all
mined ores, also abundant in stone and sand and industries
involved in grinding stone or sand blasting.
Mine workers inhale large quantities of silica that can give
rise to the disease SILICOSIS.
Silicosis consists of diffuse, nodular, whorled proliferation of
fibrous tissue surrounding the tiny doubly refractile silica
crystals when examined by polarized light.
89

Silica is unreactive thus not demonstrated by histological
stains and histochemical methods.
It is anisotropic (birefringent) when examined using polarized
light.
HEMATITE LUNG-
Mining hematite (ferric oxide) from quartz ores
Silica from quartz play major role
Iron in hematite lung fail to give Prussian blue reaction unless treated
before with 40% HCl
90

91

92

ASBESTOS
Special form of silica used as a fire resistant and insulating material.
Type of asbestos fibers that cause pulmonary disease are called AMPHIBOLES.
Dangerous type is CROCIDOLITE. Fibers are 5-100 µm long and only 0.25-0.5
µm in diameter and can collect in the alveoli at the periphery of lung.
Fibers are anisotropic but fail to show birefringence when appear as asbestos
body
ASBESTOS BODY – Characteristically beaded, yellow- brown, dumb-bell shaped
in lung sections. The proteinaceous coat contains hemosiderin and is positive with
Perls’ Prussian blue.
93

941) In case where asbestosis is suspected but no asbestos fibres or bodies are demonstrable
lung tissue from lower lobes can be digested with 40% sodium hydroxide.
Resultant tissue sludge is then centrifuged and washed in water
Smears from the deposit are made and examined using polarized light
2) Thick paraffin sections of lung tissues are mounted on glass slides coated with an adhesive
The sections are dewaxed and mounted unstained and then examined using polarised light
(Many thick sections may be needed before a positive result is seen)
DEMONSTRATION OF ASBESTOS FIBRES

95

96

LEAD
Environmental pollution due to Lead has been greatly reduced
Lead pipes that carried much of the domestic water supply have been replaced and lead in
paint, batteries and gasoline has also been reduced
Lead poisoning cases are rare and usually diagnosed biochemically using the serum
In chronic lead poisoning, excessive amounts can be deposited within many tissues,
particularly bone and kidney tubules
Demonstrated by various methods- Rhodizonate method (popular), Sulfide silver of
Timm, the unripened hematoxylin technique of Mallory and Parker, but neither of these is
specific for Lead.
97

RHODIZONATE METHOD
RESULTS:
Lead salts Black
Background Green
98

101

BERYLLIUM AND ALUMINUM
BERYLLIUM is used in the manufacture of fluorescent light tubes and gains
access to the body by inhalation or traumatization of the skin
A foreign body granuloma is formed.
These bodies usually give a positive reaction with Perls’ Prussian blue.
ALUMINUM rarely seen in tissues but gains access to the body in similar
way to Beryllium
It can also be found in bone biopsies from patients on regular hemodialysis
for chronic renal failure
102

SOLOCHROME AZURINE METHOD FOR BERYLLIUM AND ALUMINUM
RESULTS:
Solution A: Aluminum and Beryllium Blue
Solution B : Beryllium only Blue-Black
Nuclei Red
104

105ALUMINON METHOD FOR ALUMINUM
RESULTS-
Aluminium Red
Background Green

SILVER
Rarely seen in the skin of silver workers as a result of
industrial exposure
Resultant permanent Blue-Gray pigmentation is called
Argyria and is marked in Sun exposed areas
Now commonly seen as localized change in mouth (amalgam
tattoo)
In unstained and H&E sections the silver appears as fine
dark brown or black granules, particularly in basement
membranes and sweat galnds.
106

RHODANINE METHOD
METHOD:
Paraffin sections to distilled water
Incubate sections in rhodanine solution at 37˚C for 24 hours
Wash well in distilled water
Mount in glycerin jelly
RESULTS:
Silver deposits Reddish- brown
107

108
SIVER PIGMENT- RHODANINE METHOD

ARTIFACT
PIGMENTS
109

This group of pigments comprises:
Formalin
Malaria
Schistosome
Mercury
Chromic oxide
Starch
110

FORMALIN PIGMENT
a/k/a ACID HEMATIN, formed after several weeks in specimens by the interaction of acidic formaldehyde solutions with blood.
Traces of formic acid are formed by oxidation, which decreases the quality of nuclear staining and leaches out hemosiderin resulting in formation of formalin pigment.
COLOR- Brown or Brownish-Black deposit in tissues (product of degradation of hemoglobin, settles out as an insoluble product, extracelluarly)
MORPHOLOGY- Vary, commonly seen as microcrystalline deposit that is anisotropic(birefringent).
111

The deposit is usually present in blood rich tissues such as
spleen, blood vessels, hemorrhagic lesions.
Fixation of these organs for long period will tend to increase
the amount of formalin pigment formed. Under these
conditions it is advisable to change the fixative on regular
basis.
Use of Buffered neutral formalin will help to minimize the
problem of formalin pigment deposition.
112

113
Section of Kidney showing formalin pigment

REMOVAL OF FORMALIN
PIGMENT BEFORE STAINING
PICRIC ACID METHOD: Treat sections in saturated solutions of picric
acid for 5 minutes to 2 hours.
SCHRIDDE’S METHOD: Treat sections for 30 minutes with a mixture of
200 ml of 75% alcohol and 1 ml of 25-28% liquor ammonia. Wash in
water.
VERCAY’S METHOD: Treat sections for 10 minutes with a mixture of
100 ml of 80% alcohol and 1 ml of aqueous potassium hydroxide. Wash
in water.
114

LILLIE’S METHOD: Treat sections for 1-5 minutes with a
mixture of 50 ml of 75% acetone, 50 ml 3% hydrogen
peroxide and 1 ml of 28% ammonia water followed by
washing in 70% alcohol and then in running water.
KARADASEWITSCH’S METHOD: Treat sections for 30
minutes to 1 hour with a mixture of 100 ml of 70% ethyl
alcohol and 1 ml of 28% ammonia water. Wash in water.
115

MALARIAL PIGMENT
Morphologically similar to formalin pigment exhibits birefringence.
It is formed within or in the region of RBC that contain the parasite
The pigment sometimes may be so dense that can obscure the vision of
parasite in RBC
Pigment can also seen in the phagocytic cells that ingest the infected RBC’s.
Thus should examine for Kupffer cells of liver, the sinus lining of lymph nodes
and spleen, and within phagocytic cells of bone marrow.
116

117MALARIAL PIGMENT
IN PLACENTA IN SPLEEN

EXTRACTION OF MALARIAL PIGMENT
REAGENT-
Removed with saturated alcoholic picric acid for 12-24 hours
PROCEDURE-
1. Bring sections to water.
2. Place the sections in alcoholic picric acid
3. Rinse sections in 90% alcohol
4. Rinse sections in 70% alcohol
5. Place sections in tap water
6. Stain with H&E or other routine stain
118

MERCURY PIGMENT
Pigment seen in the tissues that have been fixed in the mercury containing
fixatives (‘B5’, Heidenhain’s, Zenker’s fluid)
MORPHOLOGY-
Varies, usually seen as Brownish black, extracellular crystal, monorefringent
(birefringent when formalin fixed tissue has been secondarily fixed in formal
mercury)
120

121
SECTION OF KIDNEY SHOWING MERCURY
PIGMENT

122
REAGENTS:
1. Lugol’s iodine 1 g, Potassium iodide 2 g, distilled water 100 ml
2. 5% aqueous Na2S2O3 (sodium thiosulphite)
METHOD:
1. Bring sections to water
2. Place in Lugol’s iodine for 15 minutes
3. Wash in water
4. Place in thiosulfate for 3 minutes
5. Wash in water
6. Stain with H&E or other technique
NOTE:
Advisable to not remove mercury pigment with iodine solutions prior to staining with gram’s method as
the connective tissue will take up crystal violet and then resist acetone decolorization.

123SCHISTOSOME PIGMENT:
Occasionally seen in tissue sections infested with Schistosomes.
Pigment tends to be chunky, properties similar to formalin and malarial pigments.
CHROMIC OXIDE:
Pigment rarely seen. Presents as fine yellow-brown particulate deposit,
monorefringent and extracellular in tissues fixed in chromic acid or dichromate
containing fixatives.
Removed from tissues by treatment with 1% acid alcohol.
STARCH:
Pigment introduced by talcum powder from the gloves of surgeon/ nurses/
pathologists.
It is PAS and Gomori Methamine Silver Positive and produce Maltese cross
configuration when polarised.

REFERENCES
1. Kumar v, Abbas K A, Aster C J. Cellular responses to stress and toxic insults: Adaptation, Injury and death. In: Kumar v, Abbas K A, Aster C J, editors. Robbins and cotran pathological basis of disease. 9th ed. New delhi : Elsevier ; 2014
2. Strayer S D, Rubin E.cell adaptaion, cell injury and cell death. In: Rubin R, Strayer S D, editors. Rubin’s Pathology: clinicopathological foundations of medicine. 6th ed. China: Lippincott Williams and Wilkins;2012
3. John D Bancroft, Marilyn Gamble, Pigments and Minerals: Theory and Practice of Histological techniques. 6th Edition
4. Ivan Damjanov, James Linder, Anderson’s Pathology, 10th edition
5. Lynch’s medical Laboratory Technology
6. Principles and interpretation of laboratory practices in surgical pathology, Shameem Shariff, Amrit Kaur Kaler
124

125
THANK YOU