Embed Size (px)
Citation preview
PIGMENT DISPERSION SYNDROME
Dr. Aditi Singh
Described by : Sugar and Brown 1949
Pigment dispersion syndrome (PDS) and pigmentary
glaucoma (PG) :
two successive stages of the same disease process
characterized by –
disruption of the iris pigment epithelium
and deposition of the dispersed pigment granules
throughout the anterior segment
EPIDEMIOLOGY
Young
Myopic
Male
Experiences blurry vision or eye pain after exercise
PATHOPHYSIOLOGY
Concave iris contour that allows apposition of its
posterior surface to the zonular bundles.
Friction between zonules and the peripheral iris - cause
of the pigment liberation.
Reverse pupillary block mechanism may exist : “flap
valve,”
Accumulation of pigment granules in the intertrabecular
meshwork
Increases resistance of aqueous egress elevating IOP
Elevating IOP.
Exercise (jogging, playing basketball, and bouncing
during dancing) can cause the release of pigment
as a result of pupillary movement.
Pharmacologic pupillary dilation - may result in
significant pigment liberation into the anterior
chamber.
This pigment liberation may be accompanied by
IOP increase.
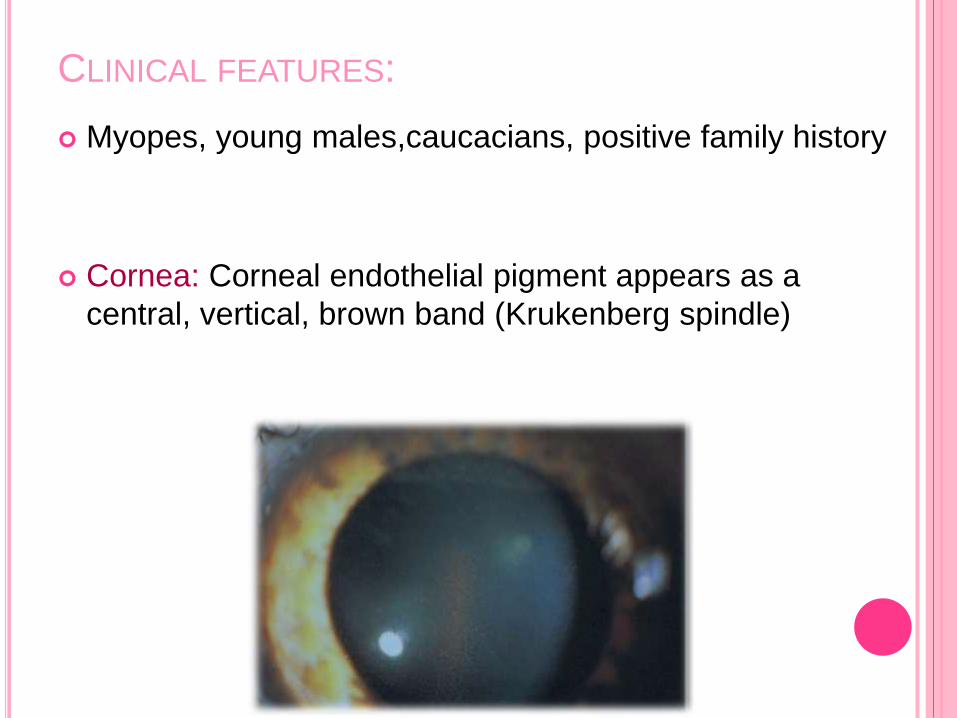
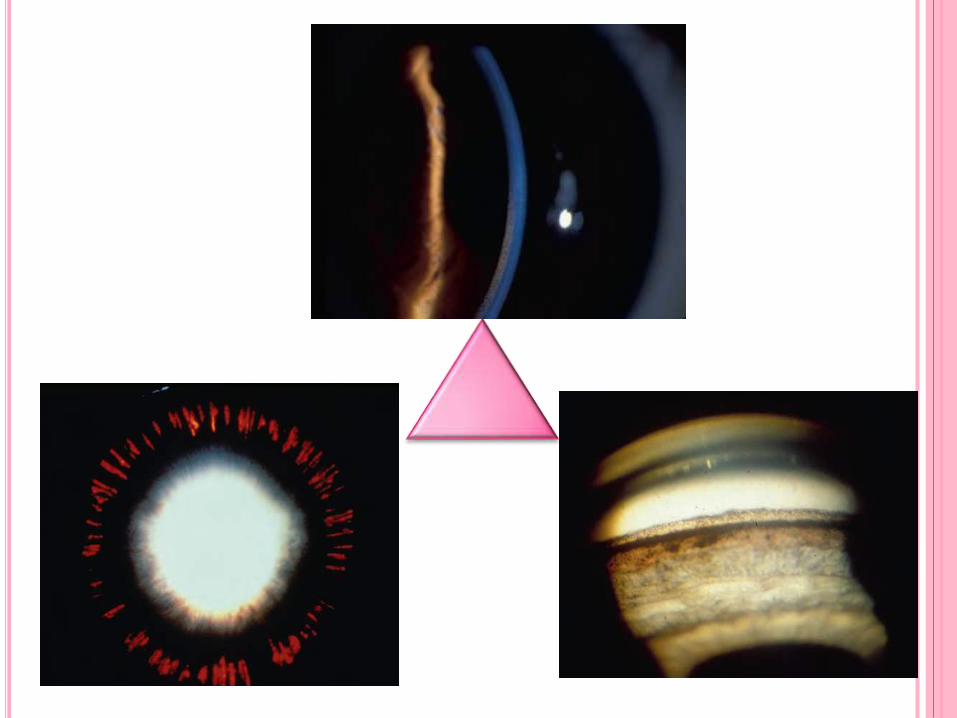
CLINICAL FEATURES:
Myopes, young males,caucacians, positive family history
Cornea: Corneal endothelial pigment appears as a
central, vertical, brown band (Krukenberg spindle)
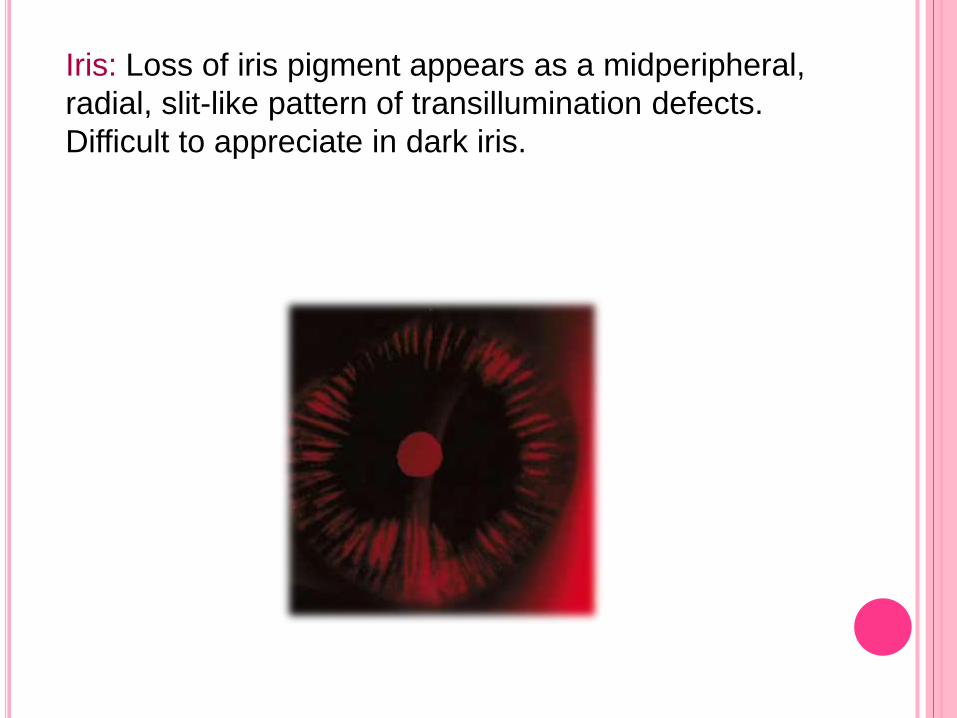
Iris: Loss of iris pigment appears as a midperipheral,
radial, slit-like pattern of transillumination defects.
Difficult to appreciate in dark iris.
Lens / Zonules : Interrupted lines on the posterior
peripheral surface of the lens – Zentamayer ring or
Scheie’s stripe.
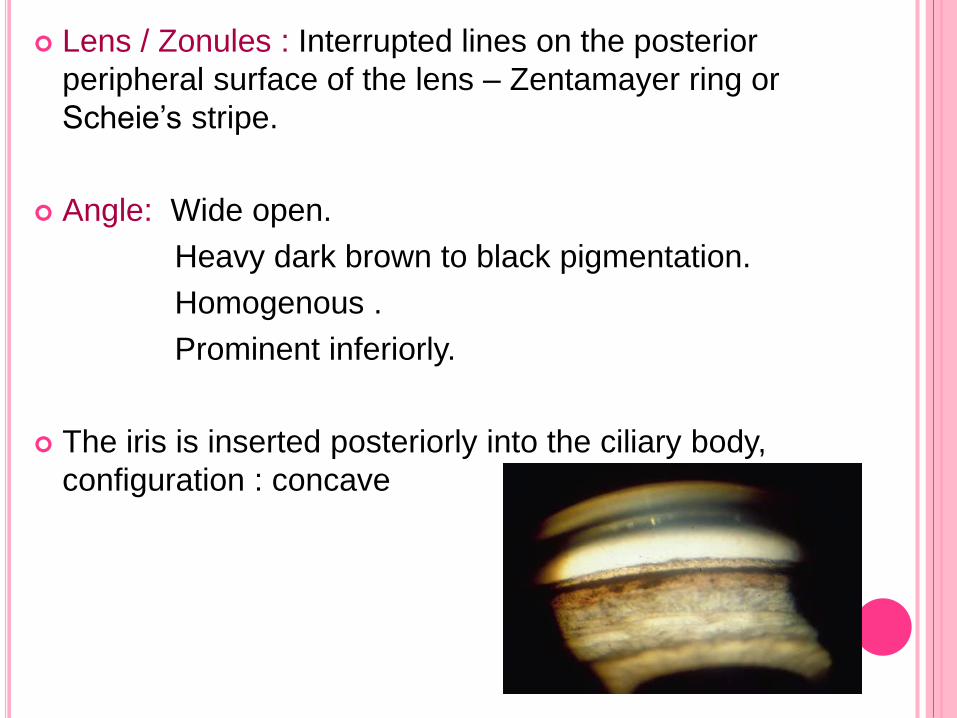
Angle: Wide open.
Heavy dark brown to black pigmentation.
Homogenous .
Prominent inferiorly.
The iris is inserted posteriorly into the ciliary body,
configuration : concave
Posterior segment:
lattice degeneration - 20% of patients
retinal breaks- 11.7%
rhegmatogenous retinal detachments
requiring surgery may occur in 3.3%
oOptic nerve examination:
Size , PPA, RNFL defect, disc h’ges, NRR thinning
TEMPORAL EVOLUTION OF PDS
Conversion of PDS to PG – slow and may take years
slow spontaneous resolution irreversible damage to angle
transillumination defects may disappear,
the IOP may return to normal,
the trabecular meshwork pigmentation may decrease.
Pigment reversal sign ( burned out )
DIFFERENTIAL DIAGNOSIS
Disorders causing anterior segment pigment dispersion :
exfoliation syndrome (XFS),
diabetes,
herpetic eye disease,
iris pigment epithelitis,
radiation,
trauma,
iris pigment epithelial cysts,
ciliary
body cysts,
iris nevus, and
melanoma or melanocytoma of
the anterior and posterior segment
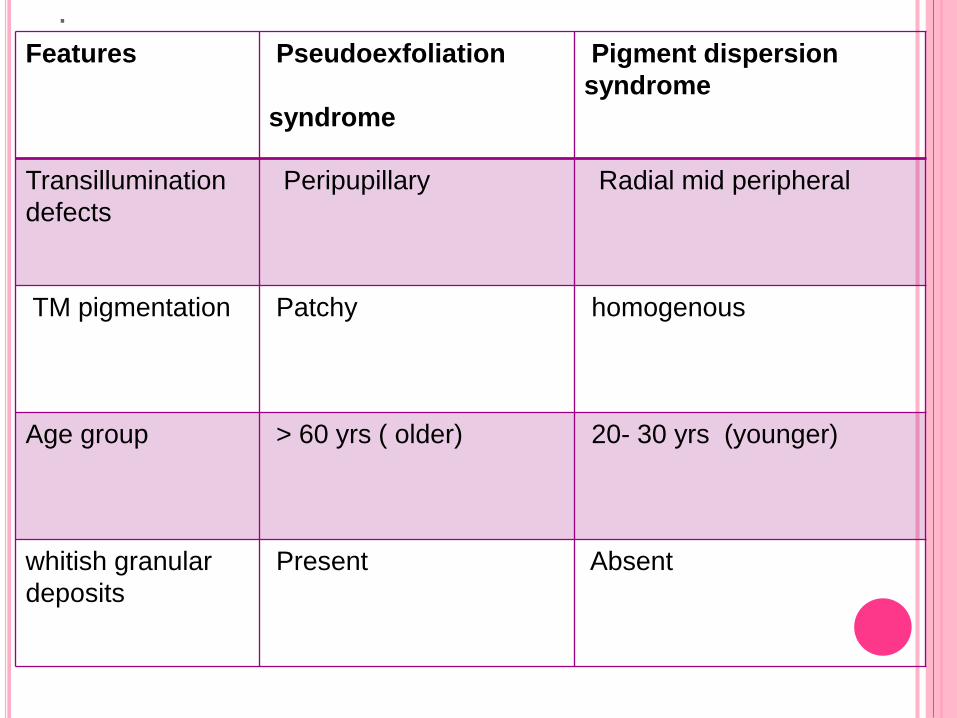
.Features Pseudoexfoliation
syndrome
Pigment dispersion
syndrome
Transillumination
defects
Peripupillary Radial mid peripheral
TM pigmentation Patchy homogenous
Age group > 60 yrs ( older) 20- 30 yrs (younger)
whitish granular
deposits
Present Absent
TREATMENT
The treatment of PDS/PG is aimed at reversing the iris concavity, preventing pigment release, and therefore lowering IOP.
Miotics:
reverses the iris concavity and eliminates iridozonularcontact.
Tension over the scleral spur, miotics increase aqueous outflow through the trabecular meshwork.
Low-concentration pilocarpine.
Peripheral retina should be examined carefully
Prostaglandin analogues: Increasing uveoscleral
outflow.
Agents that lower IOP by reducing aqueous production
hypothetically –
may diminish the rate of clearance of the pigment from
the trabecular meshwork, possibly exacerbating the
disease process.
these agents may inhibit relative pupillary block, which
is therapeutic in PDS.
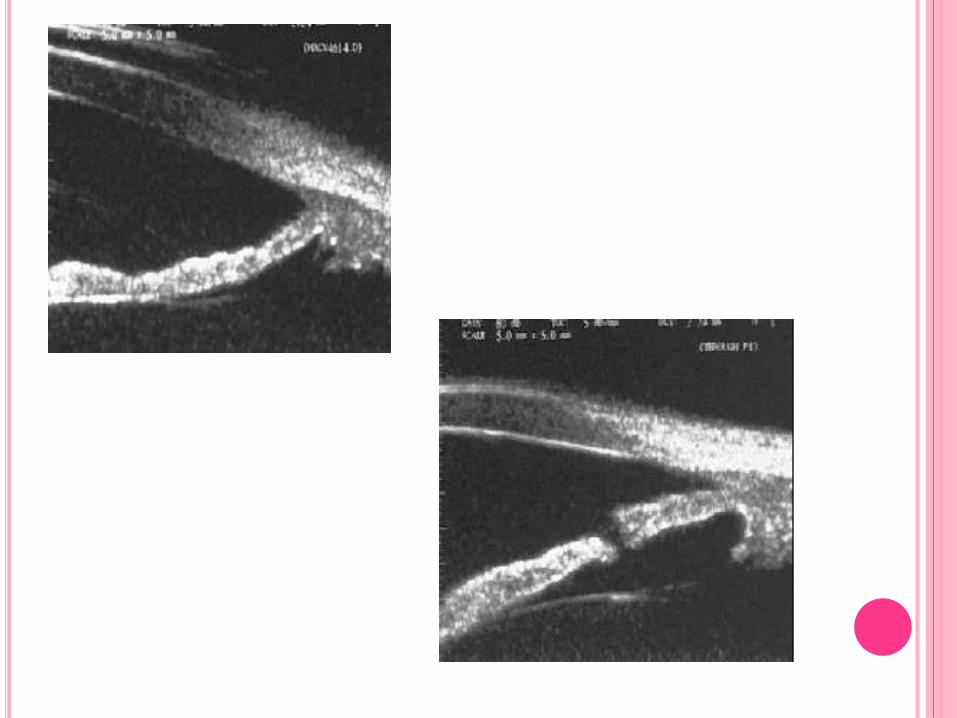
LASER IRIDOTOMY
Equalizes pressures between the anterior and posterior chambers,
Flattens the iris,
Eliminates iridozonular contact, and
Occasionally decreases further liberation of pigment
Proper patient selection.
Ideally, patients should still be in the pigment liberation stage.
In young patients with iris concavity, active release of pigment and ocular hypertension, LI may be of benefit for years.
Argon laser trabeculoplasty and selective laser
trabeculoplasty
Alternative treatments to lower IOP, mostly in young
pigmentary glaucoma patients.
The success rate of argon laser trabeculoplasty
(ALT) in PG is greater in younger patients than in
older ones and decreases with age
Trabeculectomy :
Not responding to medical / laser therapy.
MMC to be used in lower concentration for lesser
time.
Outcomes comparable /better than of POAG












![Pigment Dispersion Syndrome and Pigmentary Glaucoma · [5]. Aqueous veins have a length of approximately 1 mm and a diameter of approximately 50µm [11]. According to Poiseuille’s](https://img.pdfslide.us/doc/110x75/5ffb387c6bdd851059308fb6/pigment-dispersion-syndrome-and-pigmentary-5-aqueous-veins-have-a-length-of-approximately.jpg)