Embed Size (px)
Citation preview
A case report : NHL & AIHA,a diagnostic dilemma
Dr. Abu Yousuf Md. NazimHMO,Dept. of HaematologyD.M.C.H.Dhaka-1200
Name : Mr. Humayun Kabir
Age : 35 years
Sex : Male
Religion : Muslim
Occupation: Emplyee
Address : Mymensingh
Date of Admission: 10.04.2012
Date of examination: 10.04.2012
Ward no: 217
Bed no : 18
Particulars of the patient
A case report….• Mr. Humayun Kabir, a married man of 35 years old, resides in Mymensingh, has
referred to the Haematology department of this hospital from a private clinic with a diagnostic dilemma ,whose chief complaints were -
• Fever (High grade ; usually at night)
• With Night sweat,
• Productive cough & moderate respiratory distress,
• Pallor & generalized fatigability,
• Sore throat & anorexia,
• Multiple nodular swellings in neck, axilla & groin,
• Mild to moderate Pain in the center of abdomen & feeling of a mass near Left flank
• He has been suffering from all these complaints for last 4 months.
History of present illness
According to the patient’s statement he was apparently well 4months back and able to perform his ordinary physical activity, then he developed high grade fever, usually got worse at night with night sweats & the highest recorded temperature was 103⁰F, . He also complaints of gradual pallor appearance with generalized fatigability, at the beginning weakness and fatigue ness were associated with exertion but now a days he got exhausted even after ordinary physical activity. He has sore throat & has lost appetite and subsequently he has lost weight by apprx. 10 kg by last 4 months. He also found multiple painless nodular swellings in neck, axilla & inguinal regions which are nodular, painless, firm in consistency and a mass near his left flank for the same period. He was transfused >15 units of fresh whole blood by last 4months. He was admitted in a private clinic at first later referred to our hospital. With all these complaints he has got admitted in DMCH for further evaluation and better management.
History of past illness: No significant past medical history
Immunization history: Immunized as per EPI scheduleFamily history: He is the1st issue of his parents. Other
sib are normal & has no history of such type of disease Personal history: Non-smoker and no other bad habitsSocioeconomic condition: He belongs to middle class
familyDrug history: Not allergic to any kind of drug. He took
chemotherapy (ABVD regimen), oral antibiotic and antipyretic for his illness.
Transfusion History: He received >15 units of fresh whole blood by last 4 months.
History of past illness
His circumcision was uneventful. He had no history of skin rash, painful joint swelling or prolonged bleeding after minor trauma before this illness.He was normotensive, non diabetic, non asthmatic. He had no history of tuberculosis, contact with TB patient or no history jaundice & hepatitis.
• He was transfused with several units of fresh whole blood but in vain.
• Initially lymph node (from axillary lymph node) biopsy report infers as Hodgkin’s disease, hence he received 2 cycles of ABVD regimen D1 & D21.
• Later review of the same slide revealed as NHL and he has been given CHOP-14 regimen as treatment protocol because of highly aggressive nature of the tumor.
• So, there is a diagnostic dilemma while hematologist and the pathologist are stick to their diagnosis.
• So immunohistochemistry (CD 3, LCA, CD 20) was sent and reports negative.
Appearance : Ill looking Body built : AverageDecubitus : On choice Anaemia : Severe(+++)Jaundice : Mild (++)Cyanosis : AbsentOedema : (+)
Dehydration : AbsentClubbing : AbsentKoilonychia : AbsentLeuconychia : AbsentOral cavity : Healthy
General examination
Conjunctival haemorhage : Present in the left eyeNeck rigidity : AbsentBony tenderness : PresentLymphnode : Palpable cervical, axillary and
inguinal nodes. Size about 3-4cm, non-tender, firm in consistency and freely mobile
Purpuric rash : Not present. Pulse : 90 beats/minBP : 130/70 mm of HgTemperature : 101 °FRespiratory rate : 26 / min
Oral cavity : NormalAbdomen proper Inspection : Abdomen was scaphoid in shape.
No visible peristalsis and engorged vein. Umbilicus was centrally placed and everted and .
Palpation : Abdomen - Soft and non tender Liver - Just palpable Spleen - palpable(4cm below subcostal margin) Kidney - Not ballotable Fluid thrill – Absent
Shifting dullness- Present Percussion : Tympanic Shifting dullness- Absent Auscultation : Bowel sound present
Alimentary system
Inspection-
Shape of the precordium-normal
Visible pulsation- absent
Engorged vein, scar mark, pigmentation- absent Palpation-
Apex beat- left 5th intercostal space just lateral to
midclavicular line
Left parasternal heave, palpable P2, any thrill- absentAuscultation
1st & 2nd heart sounds are audible and normal in
intensity and character. No murmur or any other added
sound
Cardiovascular system
Respiratory system
Inspection : Movement of chest –not restricted. Bilaterally symmetrical. No visible vein or scar mark Palpation : Trachea –normal in position
Apex beat – left 5th ICS just medial to mid clavicular line
Percussion : Resonant Auscultation : Breath sound - Vesicular No added sound
Nervous system
All motor and sensory functions along with all jerks
and reflexes were normal
Salient features
Provisional diagnosis
Differential diagnosis
Differential diagnosis
LymphomaAplastic anaemiaDisseminated TBKala- azarMalariaTropical Sprue
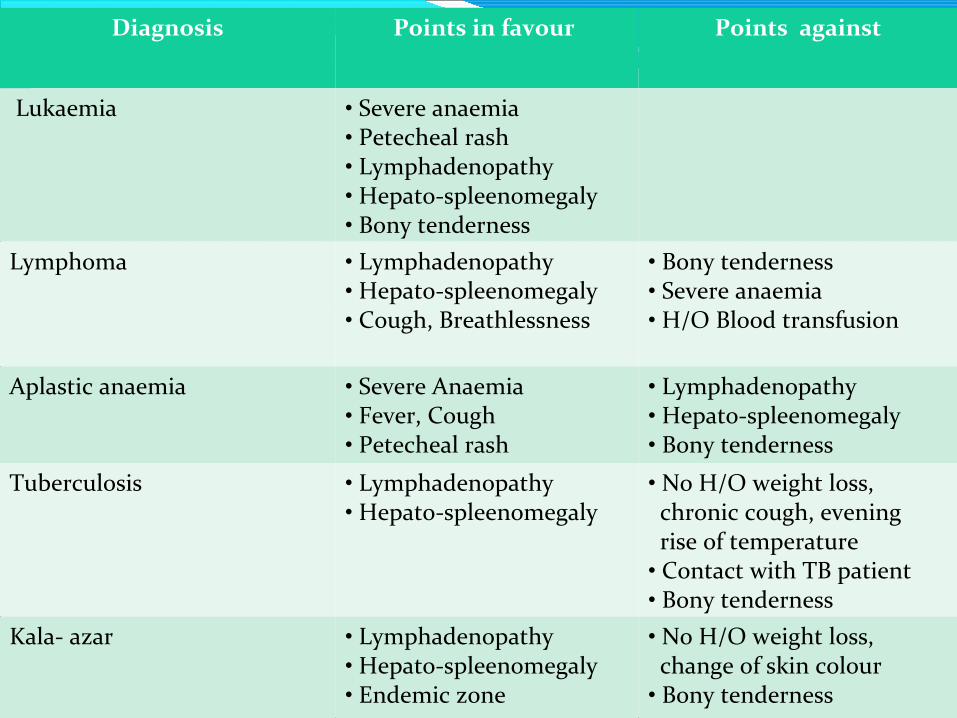
Diagnosis Points in favour Points against
Lukaemia • Severe anaemia• Petecheal rash• Lymphadenopathy• Hepato-spleenomegaly• Bony tenderness
Lymphoma • Lymphadenopathy• Hepato-spleenomegaly• Cough, Breathlessness
• Bony tenderness• Severe anaemia• H/O Blood transfusion
Aplastic anaemia • Severe Anaemia• Fever, Cough• Petecheal rash
• Lymphadenopathy• Hepato-spleenomegaly• Bony tenderness
Tuberculosis • Lymphadenopathy• Hepato-spleenomegaly
• No H/O weight loss, chronic cough, evening rise of temperature• Contact with TB patient• Bony tenderness
Kala- azar • Lymphadenopathy• Hepato-spleenomegaly• Endemic zone
• No H/O weight loss, change of skin colour• Bony tenderness
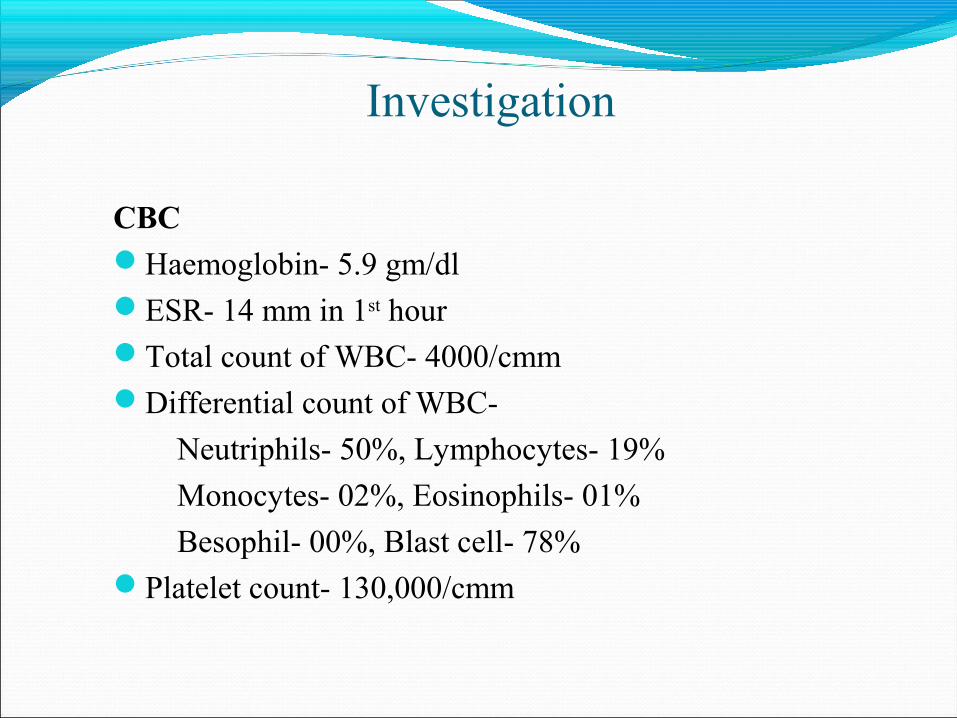
Investigation
CBCHaemoglobin- 5.9 gm/dl ESR- 14 mm in 1st hourTotal count of WBC- 4000/cmmDifferential count of WBC-
Neutriphils- 50%, Lymphocytes- 19%
Monocytes- 02%, Eosinophils- 01%
Besophil- 00%, Blast cell- 78%Platelet count- 130,000/cmm
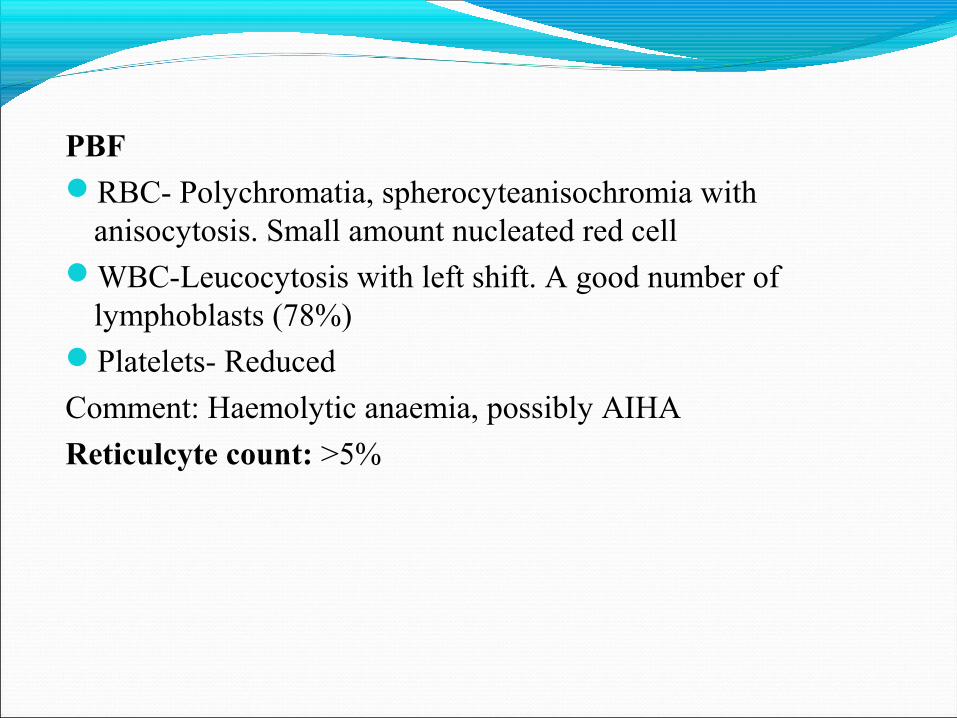
PBFRBC- Polychromatia, spherocyteanisochromia with
anisocytosis. Small amount nucleated red cell WBC-Leucocytosis with left shift. A good number of
lymphoblasts (78%)Platelets- Reduced
Comment: Haemolytic anaemia, possibly AIHA
Reticulcyte count: >5%
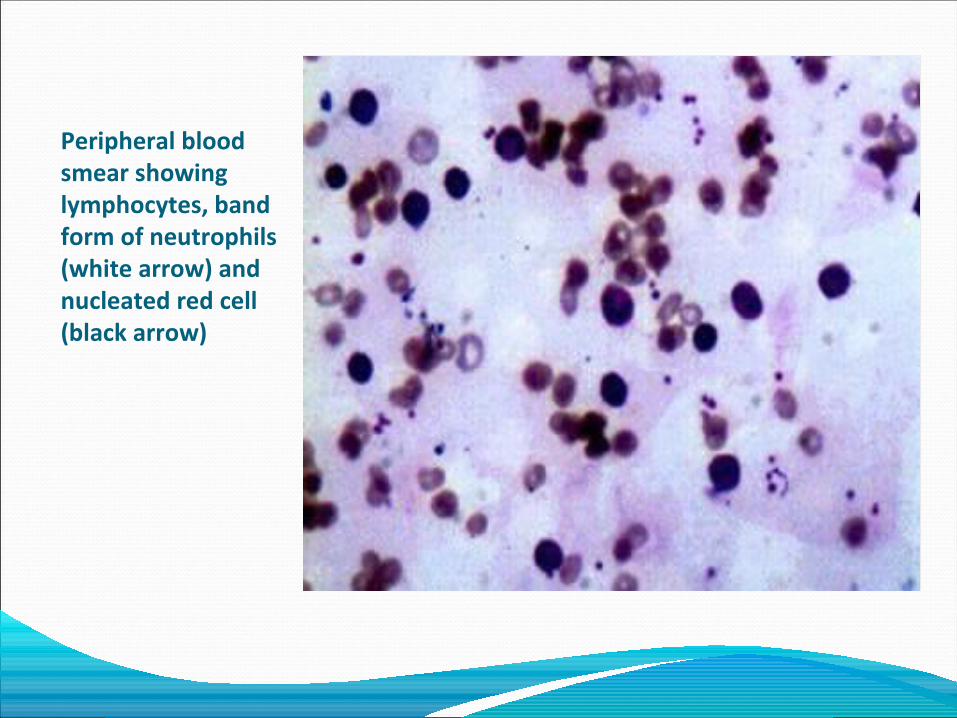
Peripheral blood smear showing lymphocytes, band form of neutrophils (white arrow) and nucleated red cell (black arrow)
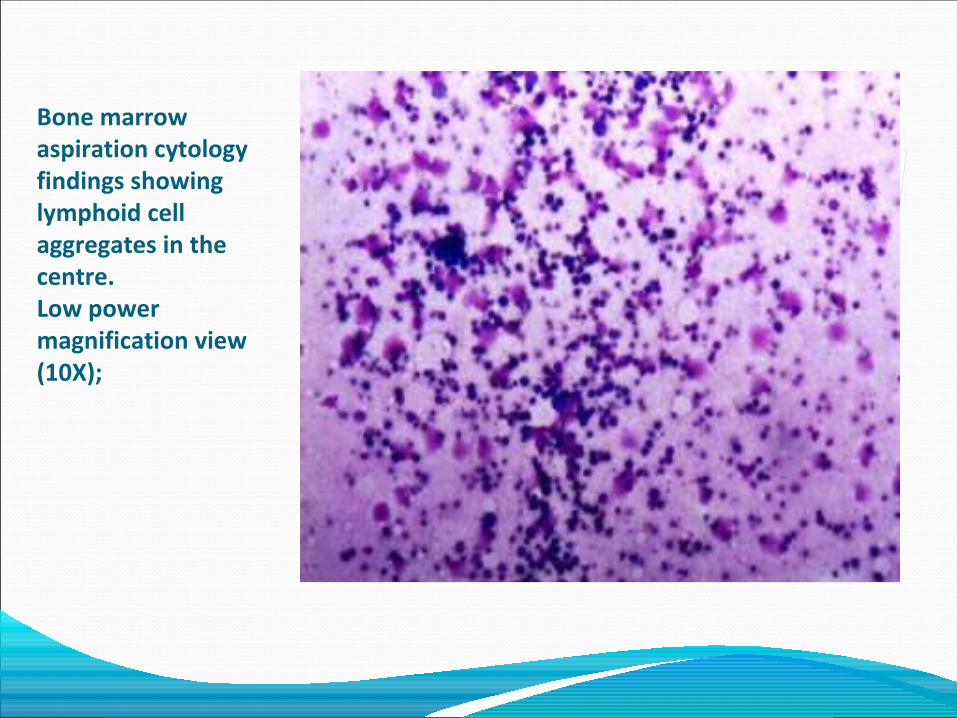
Bone marrow aspiration cytology findings showing lymphoid cell aggregates in the centre. Low power magnification view (10X);
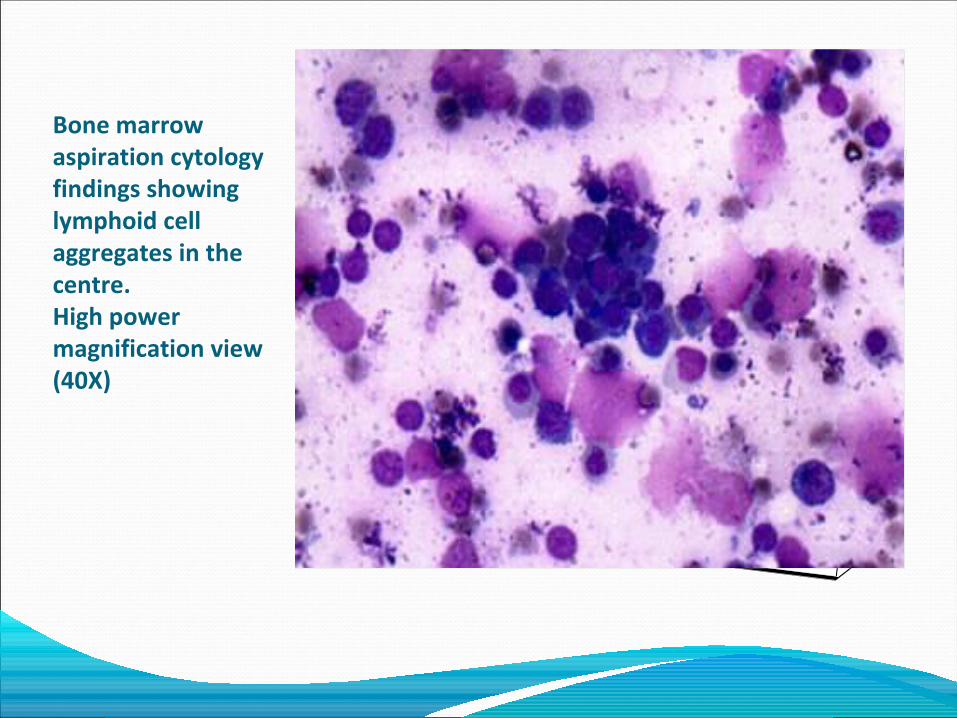
Bone marrow aspiration cytology findings showing lymphoid cell aggregates in the centre. High power magnification view (40X)
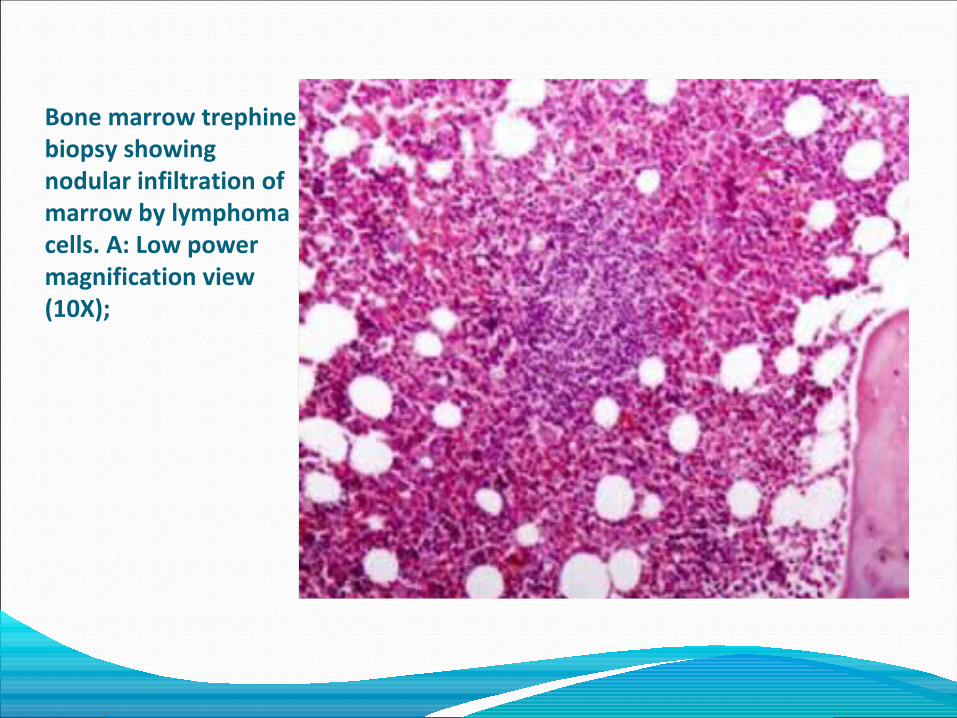
Bone marrow trephine biopsy showing nodular infiltration of marrow by lymphoma cells. A: Low power magnification view (10X);
Pathogenesis of AIHA
Autoimmune diseases are characterized by loss of tolerance to self antigens and include a broad variety of conditions like autoimmune hemolytic anemia (AIHA), systemic lupus erythematosus, rheumatoid arthritis, Sjogren’s syndrome, inflammatory bowel disease etc. The concurrence of autoimmune diseases with malignancy is well documented. One such association is AIHA occurring with non-Hodgkin’s lymphoma (NHL). The exact pathogenesis of this association is still speculative. AIHA is relatively uncommon disease and most often idiopathic. NHL arising from lymphoid tissue refers to a heterogeneous group of malignancies with varied clinical and biological features.
Diagnosis of Lymphoma
• Clinical features• Laboratory findings
Diagnosis of Lymphoma
• Clinical presentation– Generalized Lymphadenopathy – Splenomegaly– B symptoms ( Fever, night sweats, itching etc)– Abnormal laboratory findings (Cytopenia)– Extranodal presentation
Diagnosis of Lymphoma
• Investigations for diagnosis and classification
CBC & PBF
Lymph node biopsy
Leukemia/lymphoma
Making the Dx
Immunophetype/
CytogeneticsWHO Classification
Tissue biopsy/ cytology
Making the Dx
Diagnosis of Lymphoma
• Laboratory investigations for staging
Bone marrow
Radiology
Biochemistry
Aspiration & biopsy
Xray, CT, PET, USG
LDH
Diagnosis of Lymphoma
• Additional investigations
Virology HBV, HCV, HIV, HTLV
Cytology Body fluid
FNAC Transformation, Not Dx
Staging of Lymphoma
Cotswold-modified Ann Arbor classification
I Single LN region (I) or one extralymphatic site (IE)II ≥2 LN regions, same side of the diaphragm (II) or local extralymphatic extension + ≥ 1 LN regions same side of the diaphragm (IIE)III LN regions on both sides of the diaphragm (III), which may be accompanied by local extralymphatic extension (IIIE)IV Diffuse involvement of ≥ 1 extralymphatic organs or sites
Treatment of LymphomaCotswold-modified Ann Arbor classification
Suffix:A: No B symptomsB :Presence of at least one of the following: Unexplained weight loss
10% baseline during 6 months before staging; Recurrent unexplained fever 38°C; Recurrent night sweats
X :Bulky tumor is defined as either a single mass of tumor tissue >10 cm in largest diameter or a mediastinal mass exceeding one-third of the maximum transverse transthoracic diameter
Treatment of LymphomaInternational Prognostic IndexPrognostic factors Age older than 60 y Performance status of 2 or higher LDH level greater than X1 normal Extra nodal sites of 2 or more Stage III or IV
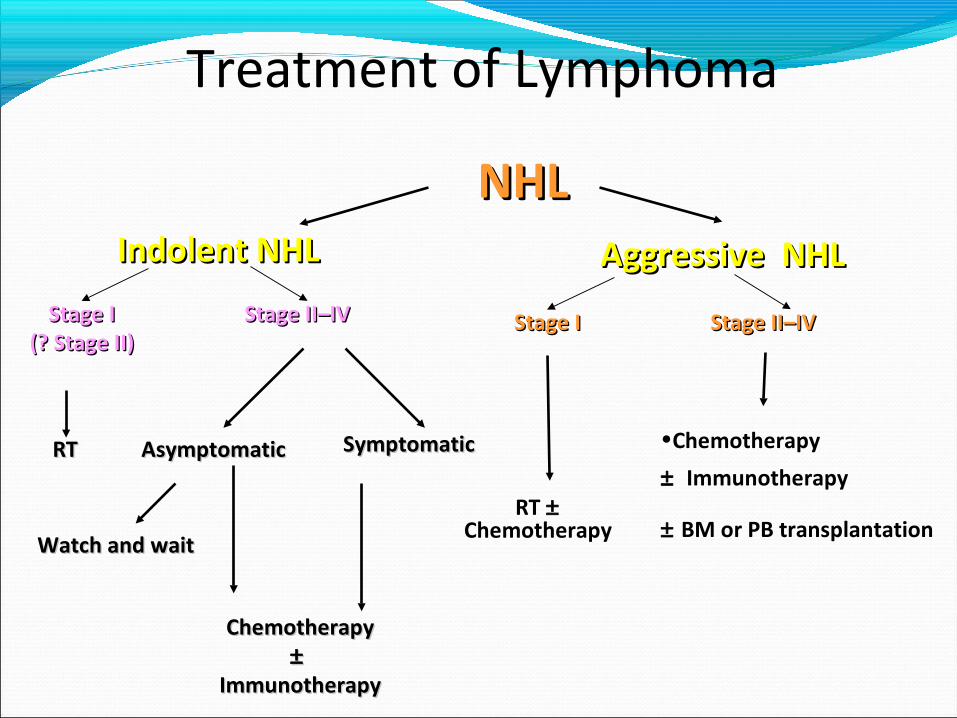
Treatment of Lymphoma
NHLNHL
Stage IStage I(? Stage II)(? Stage II)
Stage II–IVStage II–IV
RTRT SymptomaticSymptomaticAsymptomaticAsymptomatic
ChemotherapyChemotherapy±±
ImmunotherapyImmunotherapy
Watch and waitWatch and wait
Indolent NHLIndolent NHL
Stage IStage I Stage II–IVStage II–IV
RT ± Chemotherapy
Aggressive NHLAggressive NHL
•Chemotherapy
± Immunotherapy
± BM or PB transplantation
Treatment of LymphomaIndolent lymphoma Follicular lymphoma 22%
Small lymphocytic lymphoma 6%
Marginal zone B-cell lymphoma, MALT type 5%
Marginal zone B-cell lymphoma, nodal type 1%
Lymphoplasmacytic lymphoma 1%
Treatment of Lymphoma
Diffuse Large B-Cell Lymphoma (DLBCL) Stage I disease Non-bulky disease and no adverse risk factors (elevated LDH, PS <2) should receive 3-4 cycles of R-CHOP followed by involved site radiotherapy (ISRT)Patients with bulky disease should receive 6-8 cycles of R-CHOP. Radiotherapy should be considered for residual mass at the completion of treatment.
Treatment of Lymphoma
Diffuse Large B-Cell Lymphoma (DLBCL) Stage II-IV Disease Following the GELA study and subsequent NICE guidance, patients with CD20 positive DLCBL stage II-IV disease should now be offered 6-8 cycles of R-CHOP as first line treatment
CHOP vs R-CHOP (3.5 vs 8.4 years)
Treatment of Lymphoma
Follicular Lymphoma Criteria for delaying treatment (GELF17)All of the following:
Maximum diameter of disease 7 cmFewer than 3 nodal sitesNo systemic symptomsSpleen 16 cm on CTNo significant effusionsNo risk of local compressive symptomsNo circulating lymphoma cellsNo marrow compromise
Treatment of Lymphoma
Follicular Lymphoma: Rx option Watch and wait CVP ± R ( R- ↑CR but ?OS) Oral alkylating agents, i.e chlorambucil Fludarabine ± R
Treatment of Lymphoma
Mantle Cell Lymphoma :Distinct subtype of B-cell NHL. The majority of patients are over the age of 60 usually presenting with advanced stage disease. Conventional CHOP chemotherapy offers 75% overall response rate (ORR), 7% complete response (CR) rate but most patients relapse within 2 years.
Treatment of Lymphoma
Mantle Cell Lymphoma :CD5+ and CD43+, but CD10− and CD23−t(11;14) (q13;q32)CHOP±R (No ↑OS)FC/FCRHyperCVADAutologus BMT
Treatment of Lymphoma
Burkitt’s Lymphoma/ALL- L3 :Tumour lysis syndrome is a particular risk High risk of CNS disease/relapse and intrathecal treatment.High-intensity chemotherapy regimens have been developed for Burkitt’s lymphoma resulting in a 60-70% long-term survival rate.
Treatment of Lymphoma
Lymphoblastic Lymphoma\Leukaemia :ALL like treatment
Treatment of Lymphoma
T cell Lymphoma : (15%)AggressiveCommon type – Peripheral T-Cell lymphoma –NOS Angioimmunoblastic T cell lymphoma ATL
Common in Asia (Japan)HTLV infectionTreatment involved antiviral drugs
Treatment of Lymphoma
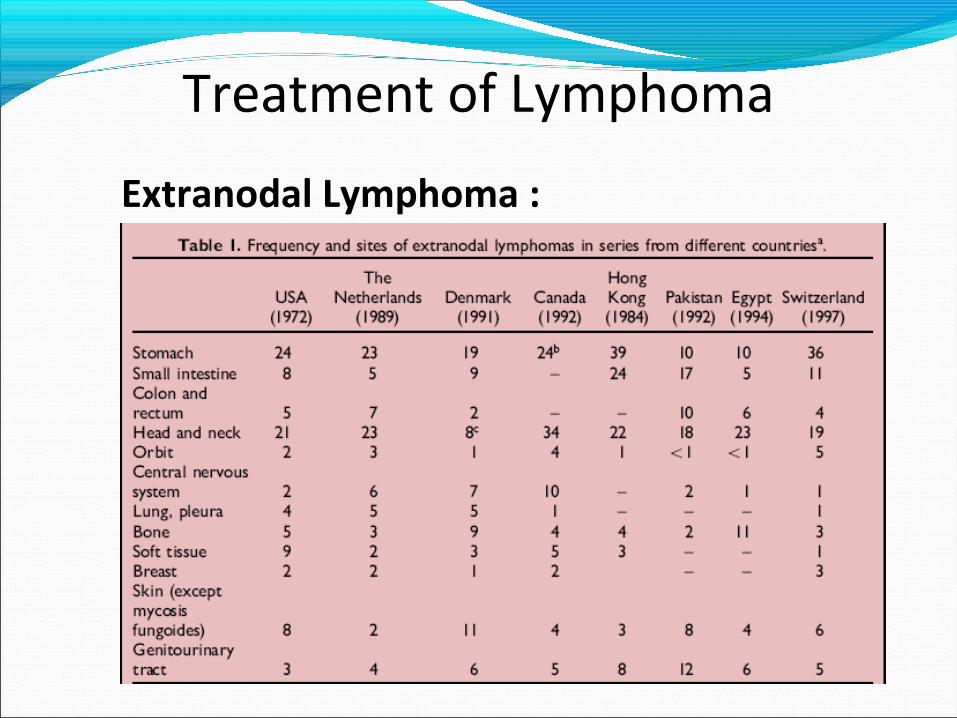
Extranodal Lymphoma :
Treatment of Lymphoma
Extranodal Lymphoma :Gastric MALT LymphomaDLCL of GITNon gastric MALT LymphomaPrimary cutaneous lymphoma Primary CNS lymphomaPrimary effusion lymphomaExtranodal T/NK cell lymphoma, nasal type
Treatment of Lymphoma
Marginal Zone\Gastric MALT Lymphoma :Non-bulky gastric disease (stage IE-II) should be treated with H.pylori eradication therapy for 3 weeks and then restaged at 3 months post-therapy (earlier if symptomatic). This treatment can be followed up with chlorambucil for up to 6 courses
Commonly/typically presenting as SLsSMZL SL-u HCL LL B-PLLT-LGL Hepatosplenic T-cell lymphoma
Primary splenic presentations of nodal lymphomas
MCL FL DLBCL-not otherwise specifiedT-cell/histiocyte-rich large B-cell lymphoma
Treatment of Lymphoma
Splenic Lymphoma : Unexplanied splenomegaly -36-48%
Commonly/typically presenting as SLsSMZL SL-u HCL LL B-PLLT-LGL Hepatosplenic T-cell lymphoma
Primary splenic presentations of nodal lymphomas
MCL FL DLBCL-not otherwise specified
T-cell/histiocyte-rich large B-cell lymphoma
Treatment of Lymphoma
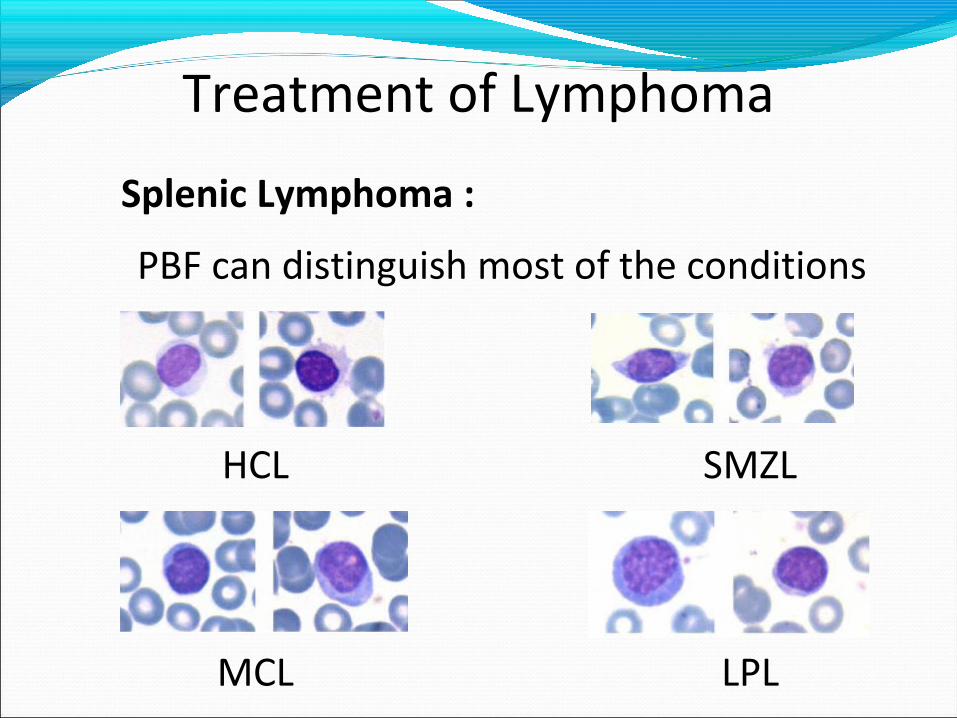
Splenic Lymphoma :
PBF can distinguish most of the conditions
HCL SMZL
MCL LPL
Treatment of Lymphoma
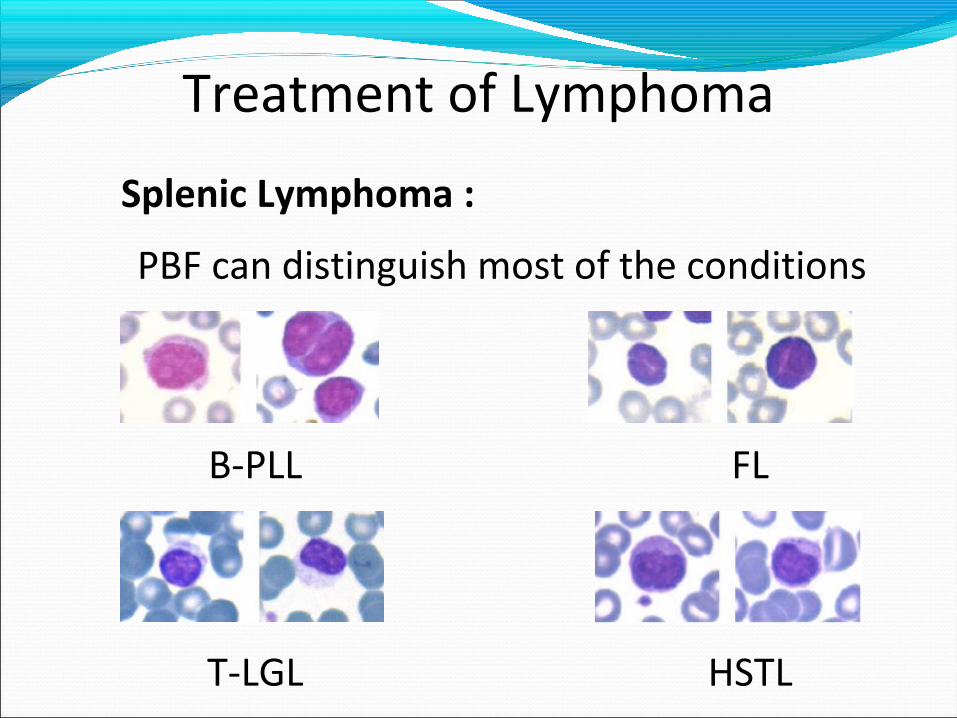
Splenic Lymphoma :
PBF can distinguish most of the conditions
B-PLL FL
T-LGL HSTL
Treatment of Lymphoma
Lymphoma in pregnancy :Aggressive lymphoma:
First trimester- termination prior to the commencement of chemotherapy should be offered.
After 32 weeks- it may be possible to delay treatment until safe delivery of the child is possible.
Indolent : Usually delayed
Treatment of Lymphoma
Lymphoma in pregnancy :Aggressive lymphoma:
First trimester- termination prior to the commencement of chemotherapy should be offered.
After 32 weeks- it may be possible to delay treatment until safe delivery of the child is possible.
Indolent : Usually delayed
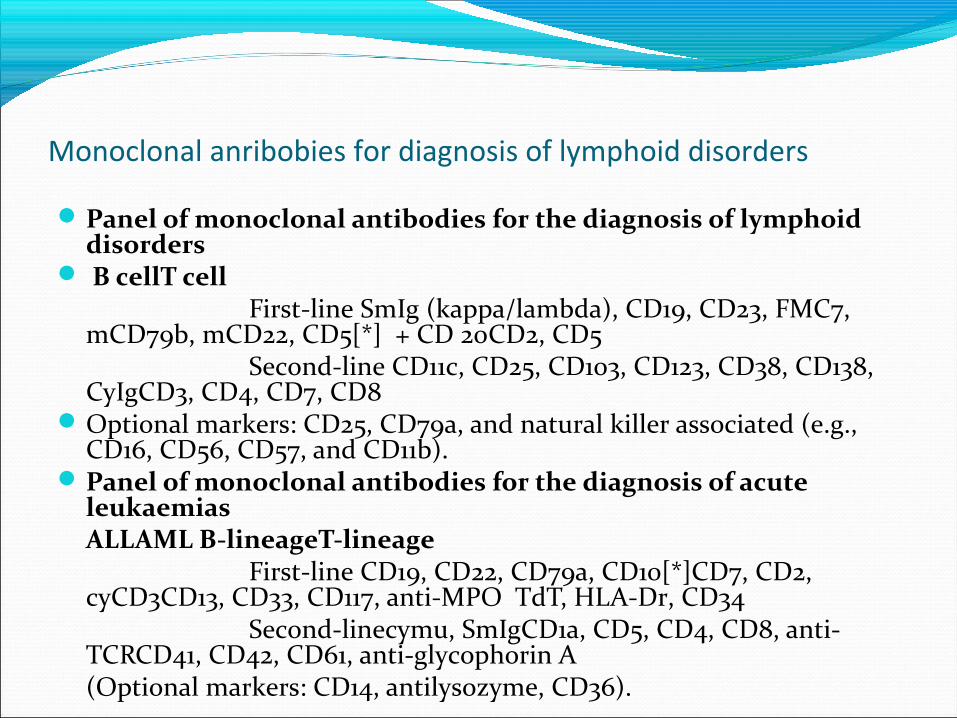
Monoclonal anribobies for diagnosis of lymphoid disorders
Panel of monoclonal antibodies for the diagnosis of lymphoid disorders
B cellT cellFirst-line SmIg (kappa/lambda), CD19, CD23, FMC7,
mCD79b, mCD22, CD5[*] + CD 20CD2, CD5Second-line CD11c, CD25, CD103, CD123, CD38, CD138,
CyIgCD3, CD4, CD7, CD8Optional markers: CD25, CD79a, and natural killer associated (e.g.,
CD16, CD56, CD57, and CD11b). Panel of monoclonal antibodies for the diagnosis of acute
leukaemias ALLAML B-lineageT-lineage
First-line CD19, CD22, CD79a, CD10[*]CD7, CD2, cyCD3CD13, CD33, CD117, anti-MPO TdT, HLA-Dr, CD34
Second-linecymu, SmIgCD1a, CD5, CD4, CD8, anti-TCRCD41, CD42, CD61, anti-glycophorin A(Optional markers: CD14, antilysozyme, CD36).
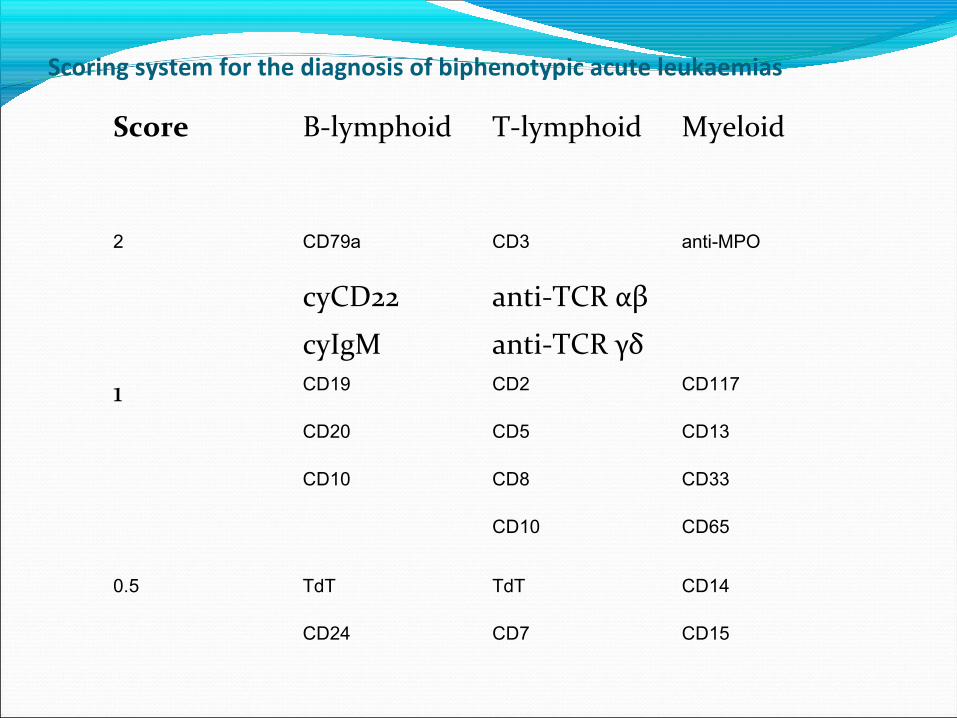
Scoring system for the diagnosis of biphenotypic acute leukaemias Score B-lymphoid T-lymphoid Myeloid
2 CD79a CD3 anti-MPO
cyCD22 anti-TCR αβ
cyIgM anti-TCR γδ
1 CD19 CD2 CD117
CD20 CD5 CD13
CD10 CD8 CD33
CD10 CD65
0.5 TdT TdT CD14
CD24 CD7 CD15
Thank you



























![Jaal-Nazim Uddin [Banglapdf.net Exclusive]](https://img.pdfslide.us/doc/110x75/577c80d61a28abe054aa5da0/jaal-nazim-uddin-banglapdfnet-exclusive.jpg)
