Embed Size (px)
Citation preview

PERDARAHAN AKUT PERDARAHAN KRONIS
H E M O L I T I K
ANEMIA
dr. FX Hendriyono,SpPK
27 Maret 2008

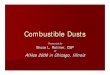
Acute blood loss
Bleeding
Post hemorrhagic anaemia (normocytic
anaemia)
Thrombocytopenia
Plasma volume RBC mass
Thrombocytosis Leukocytosis Neutrophilia
Haemodilution after 24
hourErythropoiesis
activity
BM hiperplasia
Reticulocytosis polychromatophilia RBC macrocytosis
Phase I (day 1-3)
Hypovolumic stage
Phase II (day 3-5)
Regeneration stage

Anemia of Chronic Disease
Anemia in :- Chronic inflammation, malignancy, post extensive trauma / surgery- Take place > 2 month
Mechanism :1. Phagocytic cells release apolactoferrin binds Fe2. RBC life span 3. Marrow failure (EPO )
Lab :Iron normalStores

Anemia of Chronic Disease
Fe storesRES

Endotoksin
Antigen Tantangan fagosit
Protein fase akutAbsorbsi besi Interleukin-1 Leukositosis Feritin serum Demam
Sintesis feritin
Besi Perubahan membran
Besi serum Ambilan Aktivitas fagosit eritrosit dan metabolisme Penglepasan
Eritropoesis Umur eritrositDefisiensi Fe
Soluble factor (s)
Hambatan eritropoesis
Eritropoetin Sel T
Mekanisme defisiensi besi pada ACD

ACD Anemia Kombinasi defisiensi besi
Hb Jarang < 9 g/dL Bervariasi Bervariasi
MCV & MCHC Normal / Selalu rendah Selalu rendah rendah ringan
Besi serum Rendah Rendah Rendah
DIBT (TIBC) Normal / Selalu tinggi Bervariasi, rendah ringan sering batas
atas normal
Feritin > 25ug/L, < 12ug/L Sering < 12 ug/Lsering > 50 ug/L
Besi SUTUL Normal atau tinggi Kosong Kosong
Sideroblas (%) Kurang Sangat kurang Sangat kurang
Respon besi Tidak ada Baik Sebagian
Perbandingan hasil laboratorium antara ACD dan anemia defisiensi besi

Anemia of Chronic Disease

Haemolytic anaemia

Haemolytic anaemia
Rate of RBC destruction
RBC production
Reticulocyte counts
Reticulocytosis in haemolytic anaemia

EXTRAVASCULAR HAEMOGLOBIN DEGRADATION
Macrophage
Haemoglobin Heme + globinplasma protein and amino acid pool
Biliverdin + CO + Fe transferrin + Fe Bone marrow
lungs
Bilirubin
plasma albumin
Bilirubin-Albumin (unconjugated)
liver
Bilirubin diglucuronide (conjugated)
bile duct to duodenum
Urobilinogen Blood
stool Urobilinogen (urine)
kidney
Urobilinogen + stercobilinogen

INTRAVASCULAR HAEMOGLOBIN DEGRADATIONFree Hb in blood
Haptoglobin (102 mg/dL)
Hgb-haptoglobin liver (catabolism same as extravascular)
Hb
in excess of haptoglobin
Methaemoglobin
globin amino acid pool
Heme (Fe+
++)
haemopexinhaemopexin-heme
albuminmethemalbumin
albumin
heme
RE cells in liver
dimers
kidney
Urine haemoglobin
Urine haemosiderin
tubular reabsorption

CAUSED OF HAEMOLYTIC ANAEMIAS
Intrinsic Causes(Congenital)
1. Haemoglobinopathies
(S, C, D)
2. Thalassaemia
3. Unstable haemoglobins
4. Enzyme deficiencies (that is, G-6-PD)
5. Hereditary spherocytosis
6. Hereditary haemolytic ovalocytosis
Extrinsic Causes(Acquired)
1. Autoimmune
2. Drug associated, that is, methyldopa, penicillin
a. Warm antibodies
b. Cold antibodies
3. Snake venoms
4. Parasitism (malaria)
5. Microangiopathic haemolytic anaemic
6. Hypersplenism
7. Isoimmune

LABORATORY OF HAEMOLYTIC ANAEMIAS
BLOOD FILM
Microspherocyte : 1. Autoimmuno haemolytic anaemia=AIHA
2. Hereditary spherocytosis
3. Haemoglobinopathies : HbC
4. Hipersplenisme
MCV N
MCH N
MCHC
AIHASpherocyte

A : normal
B : spherocytosis
Osmotic fragility test
A
B

A : congenital non-spherocytic anaemias
B : spherocytosis
Osmotic fragility test

LABORATORY
• RBC abnormalities
Sel target : HbC
Fragmented RBC : schistocytes
burr cells
helmet cells (MAHA)
• Plasmodium
HbC Helmet cells Burr cellsP. falciparum

LABORATORY
BONE MARROW
Erythroid hyperplasia : rubrisit predominant
Iron stores : negative / or

G-6PD deficiency
• X-linked disorders, heterozygote females only
rarely have significant haemolysis
• Haemolysis cause by infection, acidosis, drugs & toxins
• Red blood cells membrane oxidation
• Precipitation of haemoglobin Heinz bodies
• PB smear bite cells
• In acute haemolytic episode G-6PD activity
maybe normal

G-6PD Deficiency
NADPH : nicotinamide adenine dinucleotide phosphate GSSH : glutathione oxidized form G-6PD : glucose-6 phosphate dehydrogenase

• RBC in PNH are abnormally sensitive to
lysis to complement
• Diagnosis can be made by :
1. Abnormal lysis of RBC by acidic serum (Ham’s tests)
2. Hypotonic medium solution (Sugar water test)
Paroxymal nocturnal haemoglobinuria (PNH)



ANTIGLOBULIN TESTS (COOMB’S TEST)
Direct antihuman globulin tests (DAT)
Indirect antihuman globulin tests (IDAT)

LABORATORY DIAGNOSIS OF NORMOCYTIC ANAEMIA
OTHER HAEMOLYTIC ANAEMIAS
Parasites
Hypersplenism
Microangiopathic
haemolysis
Hereditary
spherocytosis
Paroxysmal noctural
haemoglobinuria
Enzyme deficiencies
Drug or toxin
Haemoglobinopathies
AUTO IMMUNO HAEMOLYTIC ANAEMIA
Erythroblastosis
foetalis
Transfusion
reaction
Collagen
vascular
disease
OTHER
Renal disease
Infection
Malnutrition
Aplastic
anaemia
Radiation
MYELOPHTHISIC
Tumor
Myelofibrosis
Infection
Leukaemia
BLOOD LOSS ANAEMIA
REPLACEMENT OF NORMAL
MARROW ELEMENTS
DECREASED CELLULARITY
HYPERCELLULAR ERYTHROID HYPERPLASIA
HYPERCELLULAR ERYTHROID HYPERPLASIA
POSITIVE
POSITIVE
NEGATIVE NEGATIVE
NEGATIVE
INCREASED
REDUCED
NORMOCYTIC ANAEMIA
INTERPRETATIONLABORATORY TEST
PERIPHERAL SMEAR
RETICULOCYTE COUNT
BLOOD IN STOOL OR OTHER SOURCE OF BLEEDING IDENTIFIED
ANTIHUMAN GLOBULIN (COOMBS’TEST)
BONE MARROW AND BONE MARROW BIOPSY
DIAGNOSIS

INDICATION FOR BONE MARROW BIOPSY
1. Suspected aplastic anaemia
2. Suspected myelofibrosis3. Suspected aleukaemic
leukaemia4. Suspected metastatic
tumor
5. Suspected miliary granulomatus infection
6. Suspected malignant lymphoma
Tumor metastasisAplastic anaemia (biopsy)
Aplastic anaemiaAcute leukaemia

NORMOCYTIC NORMOCHROMIC ANAEMIA & RETICULOCYTOPENIA
• Reduced proliferative erythroid cells1. Renal disease2. Infections, inflammation, malignancy3. Protein malnutrition4. Aplastic anaemia5. Marrow replacement (myelophtisic)
a. Tumorb. Leukaemiac. Fibrosisd. Infection (chronic granuloma)
6. Toxin, poison, radiation, drugs7. Endocrine disorders (thyroid disease)

LABORATORY
BLOOD FILM1. Anaemia myelophthisic
invasion with tumor cell or
increased in fibrotic tissues (myelofibrosis)
infection with TBC
• Moderate to marked anisocytosis &
poikilocytosis tear drop cellsNRBC Leukoerythroblastic
• WBC count normal or elevated picture
Shift to the left, including blast cells
• BM biopsy

Tear drop cells Metastasis Bronchial carcinoma cells in
bone marrow

2. Acute or chronic infection
• PMN increased
• Shift to the left
• Classic changes of infection : toxic granulation, Dohle bodies, vacuolisation & pyknotic nucleus
Dohle bodies Toxic granule
Shift to the left
Bacteria & Vacuole
Pyknotic

3. Aplastic anaemia
Clinical features :
• Bleeding, bruising, infection, lethargy, shortness of breath, no adenopathy and hepatosplenomegaly
Diagnostic Criteria :
1. Severe aplastic anaemia
Hypocellular marrow and two of the following three criteria :
• Absolute reticulocyte count < 40,0000 / L
• Absolute neutrophil count < 500 / L
• Platelet count < 20,000 / L
2. Very severe aplastic anaemia
• Absolute neutrophil count < 200 / L

BONE MARROW
BM aspiration
• Leukaemia, myelophthisic anaemia, aplastic anaemia
granuloma, infection
• BM biopsy
NORMOCYTIC NORMOCHROMIC ANAEMIA & RETICULOCYTOSIS