Embed Size (px)
DESCRIPTION
Citation preview

Multiple Myeloma

Definition and epidemiology
• Multiple myeloma (MM) is a low-grade Non-Hodgkin Lymphoma ,which is a result of proliferation of malignant clone of Pl cells in bone marrow, where they induce osteolytic lesions and produce monoclonal Ig components.
• MM accounts for 10-15% of hematologic neoplasm and about 1% of all cancer.
• The disease affects elderly people, 70% of myeloma patients are over 60 years of age and 90% are over 50 years old.

Biology of Pl cell disorders
• Plasma cells are terminally differentiated cells of the B lymphocyte lineage. Mature B Ly express on their surface the antibody that serves as receptor for specific antigen (Ag). When they encounter this Ag , they are stimulated to proliferate and differentiate, which leads to development of memory B cells and plasma cells. The Pl cells is highly specialazed to produce and secrete large amount of the same antibody . They are normally incapable of dividing and are thought to have a relatively short lifespan of several weeks. Pl cells develop both in the lymph nodes, where they are found predominantly in the medullary cords, and in the bone marrow. Pl cell have typical immunophenotype- CD38, CD 78, HLA-DR +, but have lost the surface Ags typical of B Lys

Biology of plasma cell disorders
• Chronic B-cell Ag stimulation and other cellular oncogenic events lead to clonal neoplastic Pl cell transformation. The resulting clone fails to respond to apoptotic stimuli . This results is piling up of a clone of Pl cells with marked overproduction of a single antibody that appears in the plasma as M-component ( monoclonal Ig or M-protein). Therefore MM is rather a result of a failed apoptosis of mature cells than of an excessive proliferation of precursors.

Biology of Pl cell disorders
• The bone marrow microenvironment has also important role in MM. The growth of myeloma cells is highly dependent of IL-6 produced by bone marrow stromal cells. IL-6 production is stimulated by myeloma cells. Another factor that appears to be important in the growth of myeloma cells is vascular endothelial growth factror (VEGF) which increase the angiogenesis.

Biology of Pl cell disorders
• Cause of the bone disease in MM- local activation of osteoclasts by the clonal Pl cells. This activation is due to the release of chemokines of the clonal PL cells and stromal cells such as IL-1, TNF, IL-6, macrophage inflammatory protein ( MIP). MIP is associated with the upregulation of RANKL ( receptor activation of NF-kappabeta ligand) and downregulation of OPG( osteoprotegerin, a natural antagonist of RANKL). Overexpression of RANKLis associated with increased generation of osteoclast from monocyte precursors.

Role of M-component
• M-protein could be intact immunoglobulin( IgG, IgA, rarely-IgD and IgE) and part of Ig molecule- free light chains kappa or lambda. Large concentration of IgG or dimerization of IgA could be the reason for hyperviscosity syndrome. M-protein sometimes has anti-I Ab specificity and causes cold agglutinin hemolytic anemia ( rarely) or antimyelin activity and could lead to peripheral neuropathy.Free light chains pass through the glomerular basement membrane , accumulate in the kidney parenchyma resulting in renal disfunction. Some light chains have the propety to accumulate as amyloid deposits in various organs.

Neoplastic Pl cell
suppression of normal hemopoesis
Paraprotein-monoclonal IgIgG, IgA+lambda or kappa chains or only light chain production-Bence-Jones myeloma
OAF- (Ils, TNF,MIF)
Bone destruction-lytic bone lesions,pathological fractures, osteoporosis Ca level
Hyperviscositysyndrome
Renal failureamyloidosis
li
Lightchains
anemia
neutropenia Thrombocytopenia
Bacterialinfections bleeding
SupressedNormal Ig production

Variants
• IgG, IgA, Bence-Jones myeloma; IgD and IgE- extremely rare
• Smouldering MM: > 10% atipical plasma cells, > 3 g M component, no skeletal lesions, no renal involvement. Slow progressing disease; treatment is not needed.Thorough follow-up.
• Plasma cell leukemia: young subjects, > 20% plasma cells in the peripheral blood, adenomegalies, hepato-splenomegaly, short survival.
• Non-secretory MM: < 1% of all MM, with no M component in the serum. Diagnosis: identification of the M component in the cells by immuno-hystochemestry.
• Solitary Plasmocytoma: histologic evidence of a tumor consisting of plasma cells in bones or lung,nasopharynx, without marrow plasma cell infiltration nor M component; 50% of patients survive > 10 y.

Clinical manifestation
• bone pain, pathological fractures• Symptoms of anemia- fatigue, pallor, palpitations, shortness of breath• Renal failure – causes: high Ca level, light chain deposition in renal
tubules; amyloidosis-rare complication- nephrotic syndrom; renal infections.
• Severe infections- causes: neutropenia, suppressed humoral immunity- low production of normal Igs
• Bleeding- causes: thrombocytopenia, abnormal platelet function, abnormal coagulation-the paraprotein covers the platelets’ surface and absorbs the clothing factors and interferes with their functions.
• Hyperviscosity syndrome- esp. IgA , - headache, blurred vision, bleeding, coma
• Hypercalcemia- thirst, headache, poliuria,weakness, coma• Neurological symptoms- peripheral polineuropathies , radiculopathy-
compression from large tumor mass or vertebral fracture, spinal cord compression
• Amyloydosis- rare complication

Laboratory studies
• ESR, exception-Bence-Jones myeloma
• Anemia, leukopenia, thrombocytopenia-not obligatory
• serum protein, serum alb. NB- Bence-Jones myeloma and non-secretory myeloma- normal protein level
• Abnormal renal function- serum creat, uric acid, urea- not obligatory
• Abnormal coagulation-not obligatory
• Serum Ca- not obligatory
• proteinuria

Laboratory studies
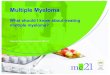
• Serum electrophoresis- screening method for detection of Pl cell disorders. It reveals
monoclonal component (narrow band peak: “church spike”) is found in 98% of patients, in serum, urine or both
• Immunoelectrophoresis- determines the class of Ig / IgG, IgA, IgD, IgE, IgM/ and the type of the light chain / lambda or kappa?

ELECTROPHORETIC FRACTIONATION OF MYELOMA SERUM
3 444444444
4
444
5 6 7
ALB 1
4
4
2
31 2 4 5 6 7 n
MYELOMA
...

Diagnosis
• І Plasmacytoma on tissue biopsy • II = Bone marrow with greater than 30% plasma cells • III = Monoclonal globulin spike on serum protein electrophoresis,
with an immunoglobulin (Ig) G peak of greater than 35 g/L or an IgA peak of greater than 20 g/L, or urine protein electrophoresis (in the presence of amyloidosis) result of greater than 1 g/24 h
• a = Bone marrow with 10-30% plasma cells • b = Monoclonal globulin spike present but less than category III • c = Lytic bone lesions • d =Depressed normal Igs• The diagnosis of MM requires at least 1 major and 1 minor
criterion or at least 3 minor critaria including both a and b

Diagnosis
Immunohistochemistry and flow cytometry- when the percentage ofPl cells in marrow aspirate or biopsy is not greatly increased- Pl cells react with monoclonalAb to CD138(immunohistochemistry) and CD 38( flow cytometry), monoclonality is also proved with monoclonalAb directed against kappa and lambda light chains.
Cytogenetics/FISH - detection of chromosomal abnormality is also proof of a clonal disorder. The most frequent chromosomal abnormalities are del13, translocations involving the IgH locus on 14q. t(4,14), t( 14,16), del13 have bad prognosis.

Diferential Diagnosis
• Other Pl cell disorders- MGUS ( monoclonal gammapathy of uncertain significance), Waldenstrom disease
• Bone methastasis –breast, prostatic Ca• Hyperparathyreoidism• Other reasons for renal failure-ex. chronic
glomerulonephritis.

Staging • Salmon-Durie staging system for multiple myeloma12 • Stage I
– Hemoglobin level greater than 10 g/dL – Calcium level less than 12 mg/dL – Radiograph showing normal bones or solitary plasmacytoma – Low M protein values (ie, IgG <5 g/dL, IgA <3 g/dL, urine <4
g/24 h)• Stage II
– Findings that fit neither stage I nor stage III criteria• Stage III
– Hemoglobin level less than 8.5 g/dL – Calcium level greater than 12 mg/dL – Radiograph showing advanced lytic bone disease – High M protein value (ie, IgG >7 g/dL, IgA >5 g/dL, urine >12
g/24 h)• Subclassification A involves a creatinine level less than 2 g/dL. • Subclassification B involves a creatinine level greater than 2 g/dL. • Median survival is as follows:
– Stage I, >60 months – Stage II, 41 months – Stage III, 23 months

Staging
• ISS ( International Staging System)• 1 – Beta 2 microglobulin <3,5mg/l and alb>35g/l- overal
survival (OS) 62 months• 2- Beta2 m<3,5mg/l and alb<35g/l or Beta2m>3,5mg/l
but<5,5 mg/l and alb>35g/l- OS 44 months• 3- beta2m>5,5 mg/l- OS 29 months

Treatment
• MM responds poorly to traditional multidrug therapy. • 1. Melphalan + Prednisone- was the gold standart for treatment- 50-
60% of patients have partial response,complete remission is rare, the duration of the response is about 1 years and the OS – about 3 y.
• 2.VAD , M2 , C-VAMP protocols- rapid induction response, but do not prolong OS
• 3. Newer therapies- Intensive treatment with autologous stem cell rescue- intensive chemotherapy- high-dose melphalan with or without total body irradiation,followed be autologous stem cell rescue ( ASCR) -12-18 months gain in OS

Treatment
• 4.Newer chemotherapy drugs for MM- • a/Thalidomide- immunomodulatory drug, suppresses the
angiogenesis, is given alone or in combination with traditional chemotherapy. Improve the response rate and extend the OS to 51 months. It is considered the new gold standard first –line treatment for elderly patients not eligible for ASCR. Side effects- sensory neuropathy, increased risk of thrombembolism.
• b/ Lenalidomide- analog of Thalidomide, less neurotoxic• c/Bortezomib ( Velcade)-side effects- peripheral
neuropathy and myelossupression

Management of Complications
• UREMIA: rehydratation, diuretics,steroids,antibiotics if renal infection is suspected, hemodialysis if these measures fail.
• HYPERCALCEMIA: rehydratation, steroids, bisphosphonates, diuretics.
• PARAPLEGIA: decompressive laminectomy, radiotherapy, chemotherapy.
• BONE LESIONS: if painful and localised, chemo or local radio-therapy, analgetics, biphosphonates.
• SEVERE ANEMIA: transfusions, erytropoetin
• HYPERVISCOSITY SYNDROME: plasmapheresis, correction of hypercalcemia.
• BLEEDING: platelet concentrates, fresh frozen plasma• INFECTIONS: antibiotic treatment