Embed Size (px)
DESCRIPTION
Citation preview

ƒ“œŠŠ
Ž››ŽŽƒ
Hard work is like stairs and luck like a lift. Lift may fail but stairs will
definitely take you to the top

Multiple Myeloma
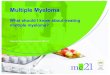
Multiple myeloma represents a malignant proliferation of plasma cells derived from a single clone. The terms multiple myeloma and myeloma may be used interchangeably. The tumor, its products, and the host response to it result in a number of organ dysfunctions and symptoms of bone pain or fracture, renal failure, susceptibility to infection, anemia, hypercalcemia, and occasionally clotting abnormalities, neurologic symptoms, and manifestations of hyperviscosity.

Nevous System
Nevous System
CherstRecurrentinfections
CherstRecurrentinfections
BloodBlood
KidneysKidneys
BonesBones
MyelomaMyeloma

Etiology
The cause of myeloma is not known.Myeloma occurred with increased frequency in those exposed to the radiation of nuclear warheads in World War II after a 20-year latency.A variety of chromosomal alterations have been found in patients with myeloma but no common molecular pathogenesis has yet emerged.Myeloma has been seen more commonly than expected among farmers, wood workers, leather workers, and those exposed to petroleum products.The neoplastic event in myeloma may involve cells earlier in B cell differentiation than the plasma cell. Circulating B cells bearing surface immunoglobulin that share the idiotype of the M component are present in myeloma patients.Interleukin (IL) 6 may play a role in driving myeloma cell proliferation; a large fraction of myeloma cells exposed to IL-6 in vitro respond by proliferating. The IL-6 dependency of myeloma is controversial.

Pathogenesis of Multiple Myeloma

Main clinical features
Bone pain Fracture (due to lytic bone lesions)Renal failureSusceptibility to infectionAnemiaHypercalcemiaoccasionally clotting abnormalitiesNeurologic symptomsManifestations of hyperviscosity

Why Bone Pain
Bone pain is the most common symptom in myeloma, affecting nearly 70% of patients. The pain usually involves the back and ribs, and unlike the pain of metastatic carcinoma, which often is worse at night, the pain of myeloma is precipitated by movement. Persistent localized pain in a patient with myeloma usually signifies a pathologic fracture. The bone lesions of myeloma are caused by the proliferation of tumor cells, activation of osteoclasts that destroy bone, and suppression of osteoblasts that form new bone. The osteoclasts respond to osteoclast activating factors (OAF) made by the myeloma cells.[OAF activity can be mediated by several cytokines, including IL-1, lymphotoxin, macrophage inhibitory factor (MIP)-1 , and tumor necrosis factor (TNF)]. However, production of these factors decreases following administration of glucocorticoids or interferon

Why bleeding and clotting disorders in Multiple Myeloma
Bleeding/clotting disorders are due to Interference with clotting factors, antibody to clotting factors, amyloid damage of endothelium, platelet dysfunction, antibody coating of platelet, therapy-related hypercoagulable defects

Why Renal Failure
Renal failure due to hypercalcemia, light chain deposition, amyloidosis, urate nephropathy, drug toxicity (nonsteroidal anti-inflammatory agents, bisphosphonates) and contrast dye

Why easy fatigability
Easy fatigue is due to anemia which occurs as a result of bone marrow infiltration, production of inhibitory factors, hemolysis, decreased red cell production, decreased erythropoietin levels

Why recurrent infections
Recurrent infections occur due to hypogammaglobulinemia, low CD4 count and decreased neutrophil migration

Why Neurologic symptoms
Neurologic symptoms are due to hyperviscosity, cryoglobulinemia, amyloid deposits, hypercalcemia, nerve compression, anti-neuronal antibody, POEMS syndrome and therapy-related toxicity

What is POEMS Syndrome
POEMS means
Polyneuropathy
Organomegaly
Endocrinopathy
Multiple myeloma
Skin changes

Representative patterns of serum electrophoresis

Multiple myeloma (marrow).

Bony lesions in multiple myeloma

Treatment of Multiple Myeloma
About 10% of patients has very slow progression of disease over many years. Such patients only require antitumor therapy when the disease becomes symptomatic with development of anemia, hypercalcemia, progressive lytic bone lesions , or recurrent infections. Patients with solitary bone plasmacytomas and extramedullary plasmacytomas may be expected to enjoy prolonged disease-free survival after local radiation therapy to a dose of around 40 Gy. Other patients respond well to systemic chemotherapy as Melphalan.Patients with symptomatic and/or progressive myeloma require therapeutic intervention. In general such therapy is of two sorts: systemic therapy to control the progression of myeloma, and symptomatic supportive care to prevent serious morbidity from the complications of the disease. Therapy can significantly prolong survival and improve the quality of life for myeloma patients.

Treatment
The initial standard treatment for newly diagnosed myeloma is dependent on whether or not the patient is a candidate for high-dose chemotherapy with autologous stem cell transplant.In patients who are transplant candidates, alkylating agents such as melphalan should be avoided since they damage stem cells. High-dose pulsed glucocorticoids have been used either alone (dexamethasone 40 mg for 4 days every 2 weeks) or in combination VAD chemotherapy (vincristine, 0.4 mg/d in a 4-day continuous infusion; doxorubicin, 9 mg/m2 per day in a 4-day continuous infusion; dexamethasone, 40 mg/d for 4 days per week for 3 weeks) for initial cytoreduction.

Major syndromes complicating marrow transplantation

?
VOD, venoocclusive disease; GVHD, graft-versus-host disease; HSV, herpes simplex virus; CMV, cytomegalovirus; VZV, varicella-zoster virus. The size of the shaded area roughly reflects the risk of the complication.