-
7/26/2019 Multiple Myeloma Final
1/69
MULTIPLE
MYELOMA
-
7/26/2019 Multiple Myeloma Final
2/69
Multiple Myeloma
Multiple myeloma is a disseminated
malignancy of monoclonal plasma cells
that accounts for 15% of all hematologic
cancers. Multiple myeloma is a disease with a wide
clinical spectrum, ranging from the
condition known as MGUS to the most
aggressive form, plasma cell leukemia .
-
7/26/2019 Multiple Myeloma Final
3/69
Monoclonal Gammopathy ofUnknown Signicance (MGUS)
haracteri!ed "y an accumulation of "one marrow
plasma cells derived from a single a"normal clone .
M#$rotien in Serum &'g(). and(or
*one marrow colonal plasma cells+1'%.
o related organ or tissue impairment-no end organdamage,or
impairment or symptoms.
-
7/26/2019 Multiple Myeloma Final
4/69
Monoclonal Gammopathy ofUnknown Signicance (MGUS)
*enign or a premalignant condition .
/he risk of transformation has "een estimated at
1% per year /he long period of sta"ility supports annual
monitoring with serum electrophoresis and "lood
counts.
-
7/26/2019 Multiple Myeloma Final
5/69
Smoldering AsymptomaticMyeloma
M#$rotien in Serum 0 &'g().
and(or
*one marrow colonal plasma cells 1'%. o related organ or tissue
impairment -no end
organ damage or impairment or symptoms.
-
7/26/2019 Multiple Myeloma Final
6/69
Smoldering AsymptomaticMyeloma
2ntermediate form of myeloma . 3isk of transformation to
multiple myeloma is much
higher than in MGUS -5#1'% per year.
-
7/26/2019 Multiple Myeloma Final
7/69
Multiple Myeloma
M#$rotien in Serum 0 &'g().
and(or
*one marrow colonal plasma cells 1'%.
$lus re4uires one of following -CRABriteria.
Calcium levation -11.5g(dl.
Renal insufficiency -reatinine 6mg(dl.
Anemia -7". + 1'g(dl or 6g(dl+normal.
Bone disease -)ytic or 8steopenic.
-
7/26/2019 Multiple Myeloma Final
8/69
Solitary lasmacytoma of !one"
Solitary "one lesion due to plasma cell tumor.
ormal Skeletal Survey.
ormal *one marrow plasmacytosis. o 9nemia, 7ypercalcemia or
3enal disease.
$reserved levels of uninvolved immunoglo"ulins.
-
7/26/2019 Multiple Myeloma Final
9/69
lasma cell leukemia
$lasma cell leukemia is a very rare variant of multiple
myeloma, where the proliferation of plasma cells is
not confined to the "one marrow "ut may "e detectedin the
peripheral "lood.
arries a very poor prognosis with median survival of
only & to : months.
-
7/26/2019 Multiple Myeloma Final
10/69
-
7/26/2019 Multiple Myeloma Final
11/69
#pidemiology
Gender
Men are affected more fre4uently than women
-1.;imately ::years.
Race
More common in *lacks.
-
7/26/2019 Multiple Myeloma Final
12/69
#tiology and $isk %actors
o predisposing factors for the development of
multiple myeloma have "een confirmed.
Environment
o Radiation exposure
o Occupational exposure -agricultural, chemical,
metallurgical, ru""erplant, pulp, wood and paper
workers, and leather tanners.o Chemical exposure to
formaldehyde,
epichlorohydrin,
-
7/26/2019 Multiple Myeloma Final
13/69
&he 'nitial orkup
CBCwith differential count and platelet count.
Routine serum chemistry -e.g., calcium, "lood urea nitrogen,
creatinine,al"umin.
Bone marrow aspirate and trephine biopsyor biopsy of mass if
solitary lesion
lonality, immunophenotype and cytogenetic studies, plasma
cell
la"eling inde>to assess plasmacytosis.
M-Protien Assessment
erum protein electrophoresis and immunofi!ation to defineprotein
type.
erum free light chain"
#$-hour urine protein% electrophoresis% and immunofi!ation "
&uantitative serum 'g levels"
-
7/26/2019 Multiple Myeloma Final
14/69
&he 'nitial orkup
(eletal survey
Prognostic )actors
? Beta-#-microglobulin "
? erum albumin"
? C reactive protein *CRP+"
? ,actate dehydrogenase *,.+ levels"
/hole-body 01 )-fluorodeo!yglucose *)G+positron
emissiontomography *PE2+3C2 scan"
MR' is an e!cellent tool for evaluation of spinal
cord compression3impingement
-
7/26/2019 Multiple Myeloma Final
15/69
eripheral *lood
/he peripheral "lood smear may reveal a
normocytic, normochromic anemia with
rouleau> formation.
$lasma cells may also "e seen.
-
7/26/2019 Multiple Myeloma Final
16/69
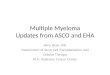
ormal plasma cells help
protect the "ody from germs
and other harmful
su"stances
Myeloma cells make
anti"odies called M proteins
and other proteins. /hese
proteins can collect in the
"lood, urine, and organs
-
7/26/2019 Multiple Myeloma Final
17/69
!one Marrow *one marrow e>amination usually reveals an
increased number of plasma cells*4056+"
2mmaturity of the plasma cells is evident with the
presence of prominent nucleoli -@myeloma cellsA.
/hese cells are strongly positive for C71% C071,
and cytoplasmic immunoglobulin.
/he pattern of "one marrow involvement in plasma
cell myeloma may "e macrofocal. 9s a result, plasmacell count
may "e normal when an aspirate misses the
focal aggregates of plasma cells that are "etter
visuali!ed radiographically or on direct needle "iopsy.
-
7/26/2019 Multiple Myeloma Final
18/69
Monoclonal roteins
2gG -:'%.
2g9 -6'%.
2gB -6%.
2g -+ '.1%.
light#chain C or D only -1E%.
*i#clonal + 1% of patients.
on#secretory disease + 5%.
-
7/26/2019 Multiple Myeloma Final
19/69
+steolytic ,esions
Multiple osteolytic lesions ='%. Single osteolytic lesions or
diffuse osteoporosis 15%.
ormal skeletal radiographs in 15%.
)esions are most commonly seen in the Skull
Ferte"rae
3i"s
$elvis
$ro>imal long "ones.
/he use of M32 indicates that skeletal a"normalities
e>ist in nearly all patients with myeloma.
-
7/26/2019 Multiple Myeloma Final
20/69
-ypercalcemia
lassified "ased on total serum and ioni!ed
calcium levels, as followscision is an indication for
radical
3/, which can significantly reduce local recurrence
rates. )ocal lymph nodes are only included in the
target volume if they are clinically involved.
-
7/26/2019 Multiple Myeloma Final
32/69
Multiple Myeloma&reatment
/he main options for therapy includeamethasone -F9B was the
standard induction
therapy in upfront patients who were candidates for 7B/.
2n the last 1' years, induction regimens dramatically
changed following the onset of thalidomide, "orte!omi",
and lenalidomide.
Melphalan is not usually recommended for people who
are canidate for renal transplant. /his is "ecause it is
often difficult to collect a sufficient number of
healthy stem cellsfor transplantation
-
7/26/2019 Multiple Myeloma Final
39/69
&halidomime4e0amethasone
2halidomide was the first @novelA agent to "e
tested in frontline setting. /he use of thalidomide
plus de>amethasone -2hal-e! has "een studied
in four randomi!ed trials.
9ll studies have demonstratedthat /hal#Be>
regimen was superior to ?=6 ;RR.
-
7/26/2019 Multiple Myeloma Final
40/69
Bortezomib-Based Induction Regimens
2n the last 5 years, "orte!omi" also
reached the frontline setting and various
phase 22 and phase 222 clinical trials were
conducted -7arousseau et al. 6'':,6''ER 3osinol et al. 6''=. /he
833
ranges from :'% to E5% with 15% to
6'% 3s.
-
7/26/2019 Multiple Myeloma Final
41/69
,enalidimide4e0amethasone
,enalidomide-3ev is also undergoing first lineevaluation.
3ev#Be> regimen was studied in
attempt to improve the /hal#Be> regimen,"ased
on the assumption that lenalidomide is more
effective and less neuroto>ic than thalidomide.
/wo large randomi!ed trials, one conducted "y
8G -3akumar et al. 6'1' and the other "y
SN8G -Tonder et al. 6''=,have shown that themaority of patients
respond to induction with
3ev(Be> -;RR of 1# and 196 with a 3 rate of
;O66%, respectively.
-
7/26/2019 Multiple Myeloma Final
42/69
&hree4rug $egimens
2hree-rug Regimens
9s all new drugs have shown e>cellent feasi"ility
and efficacy com"ined with Be> as inductiontherapy.
/he most promising three#drug induction regimen
might "e the com"ination of borte@omib with
Rev3e! *
-
7/26/2019 Multiple Myeloma Final
43/69
&ypes of &ransplant
#utologous transplantation< the stem cells areo"tained from
the individual with multiple myeloma.
Most commonly recommended.
#llogeneic transplantation< the stem cells or "one
marrow are o"tained from a donor with a tissue typematching that
of the patient. /his type of transplantation
carries very high risks and is not recommendedfor most
individuals with multiple myeloma.;'% mortality rate.
"$ngeneic transplantation< the stem cells or "one
marrow are o"tained from an identical twin of the
individual. /his is the optimal form of transplantation
although few people with multiple myeloma have an
identical twin who can serve as a donor.
-
7/26/2019 Multiple Myeloma Final
44/69
rocedure
'nitial therapy with a regimen such as len(de>a or
thali(de>a given for three tofour months.
Granulocyte colony-stimulating factor-G#S are given to stimulate
the
production of stem cells.
Stem cell are collected thru plasmaphoresis .
.arvested
Cryopreserved
-
7/26/2019 Multiple Myeloma Final
45/69
rocedure
9fter an individual recovers from the stem cell
collection, he or she is given high-dose
chemotherapywith melphalan -6''mg(m6to killas many of the
malignant plasma cells as possi"le.
$reviously collected stem cells are thawed and
returnedto the patient.
-
7/26/2019 Multiple Myeloma Final
46/69
4elayed &ransplantation"
9lternatively, after stem cell collection standard
chemotherapy with melphalan -or similar drugs
given to achieve a plateau phase"
At the time of relapse, high doses of melphalan
-or similar drugs are given.
/he previously collected stem cells are returned to
the patient.
-
7/26/2019 Multiple Myeloma Final
47/69
&andem &ransplant
Bou"le autologous transplantation -two
consecutive autologous
transplantations may "e more effective
than single autologous transplantation ifthe first transplant
has not produced
a complete or near complete
response"/he second transplantation
is usually performed within si> months of
the first.
-
7/26/2019 Multiple Myeloma Final
48/69
#5ecti/eness
9"out 0 to # percent of individuals die
from complications related to
transplantation. 7owever, compared
with chemotherapy alone, autologousstem cell transplantation is
more likely to
produce a response, and is associated
with 0#-month longer survival
compared to chemotherapy alone"
-appro>imately 5= versus ;; months
ti t 3 t #li i*l f A t l
-
7/26/2019 Multiple Myeloma Final
49/69
atients 3ot #ligi*le for AutologousStem .ell
&ransplantation
:ewer regimens for the treatment of MM.
2halidomide3 de!amethasone
9 dose of 1'' mg $8 daily at night is as effective, "ut
with fewer neuropathic effects, than higher doses. MP2 -cycle
fre4uency is every ; weeks
? Melphalan< ; mg(m6 daily on days 1 through =
? $rednisone< ;' mg(m6 daily on days 1 through =
? /halidomide< 1'' mg daily at night
Rev3e!-cycle fre4uency is every ; weeks
? 3evlimid -lenalidomide< 65 mg $8
? Be>amethasone< ;' mg $8 weekly
-
7/26/2019 Multiple Myeloma Final
50/69
&he doselimiting side e5ects
:eurologic-somnolence, peripheral
neuropathy for thalidomide .
.ematosuppression-mainly throm"ocytopenia
for lenalidomide.
*oth agents are teratogenicand
thrombophilic.
-
7/26/2019 Multiple Myeloma Final
51/69
6elcade (*orte7omi*) regimens
-
7/26/2019 Multiple Myeloma Final
52/69
4oselimiting sidee5ects
Bose#limiting side effects of "orte!omi" are
Peripheral neuropathy -predominantly sensory .
.ematosuppression-esp. throm"ocytopenia.
+lder chemotherapy regimens for
-
7/26/2019 Multiple Myeloma Final
53/69
+lder chemotherapy regimens forMM
MP-cycle fre4uency is ; to : weeks
? Melphalan< 1' mg(m6 $8 on days 1 through ;
? $rednisone< :' mg(m6 $8 on days 1 through ;
-
7/26/2019 Multiple Myeloma Final
54/69
lateau phase
hemotherapy is usually continued until multiple
myeloma enters a stable *plateau+ phase"
/he plateau phase is reached when the myeloma
"ecomes sta"le and shows no signs ofprogressing.
9lthough this phase is usually temporary, it typically
lasts si! months or longer.
;ccurs in about one half of individuals after
chemotherapy.
9chieving this phase usually reuires at least si!
or more cycles of treatment.
-
7/26/2019 Multiple Myeloma Final
55/69
$emission maintenance &herapy
"teroi!s for maintenance
/wo large, randomi!ed trials have shown that
glucocorticoid maintenance prolongs the
duration of remission and improves life
e!pectancy"
/he SN8G used prednisone -5' mg every other
day. /he 2 anadain trial contained de>amethasone
-;' mg daily for ; days every ; weeks.
-
7/26/2019 Multiple Myeloma Final
56/69
$emission maintenance &herapy
hali!omi!e
/he 2M #': study evaluated maintenance
therapy with thalidomide plus pamidronate
-9redia compared with pamidronate alone orwith o"servation only
following tandem
autologous transplantation. uperior event-
free survival and overall survival were
reported in the cohort receiving thalidomideplus
pamidronate.
Borte@omib
urrently under study as a maintenance
-
7/26/2019 Multiple Myeloma Final
57/69
Refractory and relapsed, refractory disease
9ppro>imately 1'% to 15% of patients
with newly diagnosed multiple myeloma
are unresponsive to induction therapy.
Moreover, virtually all patients whorespond initially will
relapse.
-
7/26/2019 Multiple Myeloma Final
58/69
&reatment +ptions
Con&entional chemotherap$
Al(ylating agents% alone or in combination,
have "een effective in appro>imately one#third of
patients with F9B#refractory disease.
hali!omi!e
/halidomide has an esta"lished role in therapy for
refractory(relapsed multiple myeloma, with 756 ofpatients
achieving at least 956 reduction in
paraprotein levels. 3emissions o"tained are
dura"le
-
7/26/2019 Multiple Myeloma Final
59/69
&reatment +ptions
'igh!ose chemotherap$
7igh#dose melphalan and stem cell
rescue should "e offered to patients who
have deferred the transplant initially.:ovel agents
enali!omi!e
)enalidomide has greater potency thandoes thalidomide.
Borte@omib
-
7/26/2019 Multiple Myeloma Final
60/69
-
7/26/2019 Multiple Myeloma Final
61/69
Supporti/e care
Bedrestis often necessary "ecause of the painful "ony
lesions or fractures. *edrest, however, further promotes
"one deminerali!ation, which may lead to hypercalcemia.
Bisphosphonates $amidronate, ' mg 2F over 6 hours, or Toledronic
acid,
; mg 2F over 15 minutes given monthly are indicated for
all patients with stage 22 or 222 MM -and perhaps stage 2 as
well./hese agents have significantly decreased the incidence
of skeletal complications in this disease.
2t is important to recogni!e that these agents occasionally
are associated with renal dysfunction.
-
7/26/2019 Multiple Myeloma Final
62/69
Supporti/e care
ental procedures, such as root canal or
e>traction of teeth, may "e associated
with infection or destruction of the aw
-osteonecrosis in patients treated withintravenous
bisphosphonates.
9ccordingly, patients should avoid such
procedures, if possi"le, while taking these
agentsR any needed dental proceduresshould "e performed
beforethese agents
are started.
-
7/26/2019 Multiple Myeloma Final
63/69
Supporti/e care
Calcium and vitamin deficiencies
occur in many patients with myeloma and
serum calcium levels may also be
reduced with bisphosphonate treatment./hus, oral calcium -1,'''
mg daily and
vitamin B -E'' 2U daily is recommended.
Monitoring of serum calcium is necessary,
however, "ecause occasionally patient maydevelop
hypercalcemia.
-
7/26/2019 Multiple Myeloma Final
64/69
Supporti/e care
.ydration" $atients must "e repeatedly reminded
to drink # to 7 , of liuids daily to promote
urinary e>cretion of light chains, calcium, and uric
acid. /his simple reminder has "een shown toimprove survival
greatly in some studies.
'nfections are the foremost cause of death in
patients with MM-Bue to lack of opsoni!ation.2nfections must "e
investigated and treated
urgently. 2F2G therapy should "e considered in
cases of recurrent, life#threatening infections
-
7/26/2019 Multiple Myeloma Final
65/69
Supporti/e care
Renal failure /he treatment of impaired kidney function is aimed
at the
specific underlying cause"
/reatment usually includes intravenous fluids.
Prednisonecan indirectly lower "lood calcium levels.
Allopurinol, a drug that can lower "lood levels of uric
acid.
$atients are advised to stay well-hydratedand should drink
enough fluid to produce three liters of urine daily if they
have
*ence ones proteinuria .
/hey should also avoid using :A's and contrast media
Some patients may "e candidates for hemodialysis treatment
-
7/26/2019 Multiple Myeloma Final
66/69
$egimes Used 'n $enal %ailure
/halidomide(Be>a
F9B
Falcade (Be>a )inilidamide(Be>a
-
7/26/2019 Multiple Myeloma Final
67/69
-
7/26/2019 Multiple Myeloma Final
68/69
$ole of #!$&
/he most common use of 3/ in the
management of plasma cell tumors is for
palliative treatment of "ony disease -relief
of compression of spinal cord cranialnerves, or peripheral
nerves.
2t has "een estimated that appro>imately
;'% of patients with multiple myeloma will
re4uire palliative 3/ for "one pain at sometime during the
course of their disease
-
7/26/2019 Multiple Myeloma Final
69/69
$ole of #!$&
Nhen 3/ is given for pain due to
disease involving a long "one, a local
field suffices. 2t is unnecessary to treat
the entire "one . Boses of 1' to 6' Gy -in five to 1'
fractions are effective, although the pain
relief is often partial .