Embed Size (px)
DESCRIPTION
guiding the procedure is key.
Citation preview

Francesco Maisano
San Raffaele Scientific Institute and University HospitalMilano

First case performed in 1991
Over 1500 published cases accumulated worldwide
About 15 yrs follow-up Technically simple and
reproducible Versatile Criticized by some surgeons
Did not apply correctly Used only as a bailout

Alfieri O et al. JTCVS 2001
Performed in diverse clinical settings: High risk patients Complex anatomy Functional MR
Used to correct anterior and posterior lesions
Annuloplasty has been added whenever possible (90%)

Alfieri O et al. JTCVS 2001; Maisano F et al. EJCTS 1998
Free
dom
from
re
oper
atio
nR
ecur
renc
e of
MR
/ M
S 5 yrs follow-up of 82 pts with severe
Barlow’s disease and bileaflet prolapse
Overall Etiology subgroups

Debonis et al. JTCVS 2005
years
14121086420
Fre
ed
om
fro
m r
eo
pe
ratio
n
1,00
,90
,80
,70
,60
,50
,40
,30
,20
,10
ALP: 96,6 ± 1,74%PLP: 96.2 ± 2.0%
E2E offers the same results as conventional techniques
n.s.
MayoMayo
ClevelandCleveland

The suture must incorporate the diseased segment(s) completely
Respect symmetry Suture lenght should be kept to the
minimum effective to correct MR in order to avoid stenosis
Depth of suture bites is variable according to the nature of the MR

Maisano F et al. EJCTS 1998

Stenosis / Gradients
Suture dehiscence
Role of annuloplasty

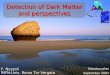
Hemodynamics are not influenced by a two orifice configuration of the valve
Pressure gradients are related to the sum of the two orifices area
0
2
4
6
8
(mmHg)
Double (1:1) Double (1:2)Single Q = 11 l/minArea = 2.25 cm2
Maisano F et al. EJCTS 1999

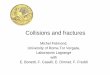
Stresses on the suture are maximum at diastole
Stresses depend on annular size
Redaelli et al. J. Biomechanics 2001
- 647
- 520
- 394- 267
- 140
- 134
+ 113+ 240
+ 367
+ 493
+ 620+ 747
+873
+1000
SI (kPa)

Annuloplasty has been routinely added to the Alfieri procedure Absence of annuloplasty is associated with increased stresses on the
suture and on the valve structures Absence of annuloplasty may be associated with accelerated failure
(but not in multivariate analysis)
- 647- 520 - 394- 267- 140 - 134+ 113+ 240+ 367+ 493+ 620+ 747+873+100
0
SI (kPa)
Alfieri et al. JTCVS 2001, Maisano et al JTCVS 2003, Nielsen et al Circulation 2005

Maisano F et al. Eurointervention 2006


Guide
Steerable sleeve
Clip delivery handle
Stabilizer
Atrial Septum

Enrollment Population nEVEREST IFeasibility (completed)
Registry patients 55
EVEREST IIRandomized n=244
Roll-in Randomized ClipRandomized Surgery
6017288
EVEREST II High Risk Registry 78
Total enrolled 453



79 pts

SURGERY FREE
76/104
Surgery After Clip Implanted (n = 20)• 15 (75%) Repairs (0 - 562 days)
• 5 (25%) Replacements
Surgery After No Clip (n = 8)• 5 (63%) Repairs
• 3 (37%) Replacements
71% Repaired

Applicable only to central MR originating from A2-P2
Not applicable in case of wide prolapse
Not applicable in case of annular dilatation
mid esophageal 120°
mid esophageal 90°
mid esophageal 120°
Maisano F, et al Am J Cardiol 2007;99:1434–1439
SL AL
<10% of current surgical candidates

When performed according to surgical principles, the E2E technique provides results at least non inferior to other surgical techniques
Precision of the repair is mandatory for efficacy and durability Pt selection + include all diseased segments + respect symmetry
Patients with normal annular function may undergo ringless repair, although lower durability may be expected
Percutaneous approach is feasible also in FMR Addition of annuloplasty should be an option also
for percutaneous patients

66 aa, maschio, 64 Kg, 164 cm, BSA 1.7 m2, BMI 24
IM 4+, FE 15-20%, PAPs 75 mmHg, disfunzione VDx, IT 3+
1994 IMA anteriore; 2001 PTCA e successivo CABG (LIMA—LAD);
successive plurime PTCA con stents medicati
2005 AlloTx di midollo per AML, inizia CsA
2006 stenting a. carotide comune e interna destra
1/2008: recidiva di IMA per trombosi intrastent POBA su LAD
4/2008 EPA PM-ICD biv
AAA sottorenale; CCS II, NYHA II, labile compenso emodinamico
Anamnesi-1 Paziente n. 1Paziente n. 1