Embed Size (px)
DESCRIPTION
Citation preview

Proceedings of the Ispat General Hospital
YEAR 2011
Ispat General Hospital,
Rourkela Steel Plant, Rourkela

Proceedings of the
Ispat General Hospital
Editor
Dr R N Mohapatra
Reviewers Publicity
Dr A M Acharya Mr J C Mohapatra
Dr C M Rao Mr R Kumar
Dr K C Mohanta Ms A Satpathy
Dr N K Behera
Dr P Mishra
Dr (Mrs) Prativa Behera
Dr R B Pattnaik
Dr S Mohanty
Dr S K Mishra
Dr S K R Prusty
Dr S N Mohapatra

Message
I am extremely happy to learn that 'Proceedings of Ispat General Hospital' is
being revived after a gap of nearly two decades.
The current edition that heralds a new beginning will surely lay the
foundations for making this journal more meaningful for practicing Doctors.
In fact, with the fast changing scenario in the medical sphere, such
publications have immense value for meeting the education and training
needs of upcoming medical professionals besides providing the basis for
fresh research.
In recent times Ispat General Hospital, administered by Rourkela Steel Plant,
has not only grown in stature as a treatment centre for complicated aliments
but has also established itself as a centre for medical education with the
introduction of post graduate courses (DNB). I am sure this publication will
be of enormous help to the DNB students both as a source of learning and
also a platform to publish their achievements.
I extend my hearty congratulations to the dedicated team of Doctors of Ispat
General Hospital for taking up this endeavour and wish this publication a
grand success in the current edition as well as in future.
S. N. Singh(CEO, RSP & I/c RMD)


Ispat General HospitalRourkela-769005
Dr S.K.Mishra,Director In-Charge,
Medical & Health Services,SAIL, RSP, Rourkela
Acknowledgement We would like to place on record our deep sense of gratitude to our
Managing Director, Shri S N Singh who has constantly encouraged us to
develop as professionals and bring about improvements in every activity
connected to health care. We are particularly grateful to him for his
unstinted support, guidance and encouragement that made this issue of
'The Proceedings of IGH' see the light of the day.
This publication is an endeavour to once again present the efforts and
achievements of the dedicated medical professionals at Ispat General
Hospital before the medical fraternity. The erudite authors of the articles
have contributed significantly in making the proceedings a valuable
compendium truly worth perusing and preserving. The reviewers have also
rendered a commendable service by fine-tuning and adding value to the
content. We sincerely acknowledge the efforts of the authors as well as the
reviewers.
We are also grateful to the Public Relations Department for their support
at each stage of this project, right from conceptualization to coordination
with the publishers, and giving the finishing touches.
The publishers patiently stood by us during the several revisions while
adding their innovative ideas to enhance the quality of this publication. They
deserve our sincere thanks.
Finally I wish to place on record my grateful thanks to all my colleagues for
the generous help and support that they have bestowed at every stage of this
publication.

• Editorial 03
Review Article
• Diabetic nephropathy 04Kishore C Mahanta
Original Papers
• Prevalence of phage types & biotypes among Salmonella Typhi 13and Salmonella Paratyphi A isolates from Rourkela, OrissaSeshadri S Bhattacharya, Usha Das
• Predictions of Length of Hospital stay of malaria patients 17Saroj K Mishra, Narayan P Sahoo, Kishore C Mahanta, Rajalaxmi Mishra
Case reports
• Peutz- Jeghers Syndrome presenting as acute intestinal obstruction 21due to Jejunal Intussusception in an adult male Amulya M Acharya, Sishir R Dash, Manoja K Panigrahi
• Necrotising fasciitis in neonate – case report 25Radhanath Satpathy, Nimain C Nanda, Pitabas Mishra, Rajan K Behera,Pinaki Panigrahi
• Squamous cell carcinoma & basal cell carcinoma with xeroderma 28pigmentosa – a rare presentationAruna M Minz, Niranjan K Behera, Rabi R Panda, Sanghamitra Satpathy,Prativa K Behera, Usha Das
• Multiple brain metastases due to occult Papillary Carcinoma 31of thyroid gland: A Case Report
Rabindra N Mohapatra, Sudhi R Pradhan , Rabi R Panda, Pushpa Kumari, Saropani Hembram
• Unusual case of severe Sepsis 34Rajyabardhan Pattnaik, Sanjib Mohanty, Sradhananda Mohapatra
Clinical imaging
• Choanal Stenosis with single nostril -a rare Case 37Paramananda Rath, Nimai C Nanda, Pitabas Mishra, Sidhesh C Mishra
Residents' Section
• Accidental Breakthrough 39Suman Behera, Pallavi Agarwal
• Practice paper 40
• Down The Memory Lane 44
• Instructions for the Authors 46
• Ispat General Hospital : An Overview
Contents

3
“20,000 liver transplants needed annually in India, only 110 donors in 2009”. This was the news
1headline on April 01 2010 .
Throughout the world, main resources of donor 2, 3
organs are the brain dead patients. But, the sorry state in our country is mainly due to reluctance to accept the concept of brain death, both by the physicians as well as general public. Causes of this reluctance may be due to several reasons related to physicians themselves and relatives of the
2deceased as well. According to Pathak et al., some of the factors responsible for this may be
• Lack of understanding the concept.• Special emotional attachment to the dead
person• Loss of confidence in medical practice• Ethical questions related to earlier organ
transplant procedure• Perceived insufficient participation of
government and medical associations.Concept of clinical death in the form of loss of observable cardio respiratory failure has undergone a sea change due to widespread use of mechanical ventilators that prevent respiratory
3arrest . In 1968, ad hoc committee at Harvard Medical School defined irreversible coma, or brain death, as unresponsiveness and lack of receptivity, the absence of movement and breathing, the absence of brain-stem reflexes, and coma whose
3cause has been identified.
In India, The Transplantation of Human Organs Act, 1994 (Central Act 42of 1994), lays down the definition of death thus: 'Deceased person ' means in whom permanent disappearance of all evidence of life occurs, by reason of brain stem death or in a cardio-pulmonary sense at any time after live birth has taken place. It goes on to state that 'brain-stem death' means the stage at which all functions of the brain stem have permanently and irreversibly ceased. Once brain-stem death has been diagnosed by an authorized committee using specified criteria, the dead person's organs can be removed for transplantation provided legally valid
3, 4consent for this is available.
Continuation of critical care support after brain death, drains out the resource crunch critical care departments of life saving resources, manpower and finance. In fact, it puts a lot of burden on the family members physically, financially and emotionally, for an outcome which is unattainable. In addition, keeping life saving equipments engaged for a brain dead patient may deprive another critically ill patient whose condition is reversible. We, the physicians, should understand that there is no recovery after brain death. We can explain relatives of the deceased that putting their patient on life support system is futile; rather his viable organs can alleviate the disease in a person who can otherwise lead a normal healthy life. In an Indian scenario, the relatives of the deceased can be emotionally appealed that some part of their near and dear ones will still be surviving in the recipient's body.
The purpose of this Editorial is not to go into the intricacies of brain death, rather to sensitise medical professionals and public regarding the fact that brain death is ultimate end of one's journey in this Earth.
It is time to educate ourselves and the public, to assist in understanding the concept of brain death. It is particularly true in hospitals, where load on critical care department is very high.
References:
1. Zee News.Com, uploaded on Thursday, April 01, 2010, 00.03
2. Pathak MK, Tripathy SK, Agrawal P, Chaturvedi R, Yadav S. Clinical Criteria for Diagnosis of Brain death and its Medico-Legal applications (A Review Study). IndMedica-Medico-Legal update.2006; 6(2):3-6
3. Golia AK, Pawar M. The diagnosis of brain death. Indian J Crit Med 2009;13:7-11
4. Pandya SK. Brain death and our transplant law. Paper presented at: The seventh National critical care congress CCCON; 2001 Jan 2-7; Bangalore
Rabindra N.MohapatraDeptt. of Neurosurgery
Address for communication :
Sr. Deputy director, Neurosurgery,
Ispat General Hospital, Rourkela-769005, India
e-mail: [email protected]
Brain Death, its impact on organ donation and resources of critical care units
Editorial

4
Diabetic Nephropathy
Kishore C Mahanta
Deptt. of Internal Medicine Address for communication :Dr K.C. Mohanta,
Senior Deputy Director,
Ispat General Hospital, Rourkela -769005, INDIA
Email: [email protected]
ABSTRACT
Introduction:-
Diabetes has become the common single cause of
Chronic Kidney disease (CKD) leading to End-Stage
Renal Disease (ESRD) in most countries: this is due
to the fact that diabetes, particularly type 2 is
increasing in prevalence and that diabetic
patients are living longer with proper medication.
About 20-30% of patients with type 1/ type 2
diabetes develop evidence of nephropathy.
Recent studies have now demonstrated that the
onset and course of diabetic nephropathy can be
delayed to a very great extent by several
interventions, but these interventions have their
greatest impact if instituted at a very early course
of development of this complication. Recently
there has been a lot of developments in the
treatment of End Stage Renal Failure.
There is a silent epidemic of type 2 diabetes world
over. It is predicted that India will be the diabetic
capital of the world by 2020. With growing
population of type 2 diabetes, the prevalence of
diabetic nephropathy is on the rise. In fact diabetic
nephropathy is the single most common cause of
End Stage Renal Disease (ESRD) today.
Besides patients' miserable sufferings, it
consumes greater financial resources than non
diabetic ESRD. Diabetic ESRD patients do poorly
on dialysis and mortality is higher. There is a
spectrum of co-morbidities such as CV disease,
brain stroke, blindness, gangrene etc which are to
be dealt with while treating such patients with
Renal Replacement Therapy (RRT).
There has been some evidence to suggest that
genetic predisposition to hypertension may
predispose to development of diabetic 1
nephropathy. Pre diabetic individuals, with
impaired glucose tolerance, frequently have
hypertension as one facet of metabolic syndrome.
Genetic factors combined with metabolic and
hemodynamic alterations induce renal damage in
susceptible individuals.
The exact cause of diabetic nephropathy is
unknown, but it is believed that uncontrolled high
blood sugar leads to the development of kidney
damage, especially when high blood pressure is
also present. Not all persons with diabetes
develop this condition.
Each kidney is made up of hundreds of thousands
of filtering units called nephrons. Each nephron
has a cluster of tiny blood vessels called a
glomerulous. Together these structures help
remove waste from the body. Too much blood
sugar can damage these structures, causing them
to thicken and become scarred. Slowly, over time,
more and more blood vessels are destroyed. The
kidney structures begin to leak and protein
(albumin) begins to pass into the urine.
Persons with diabetes who have the following risk
factors are more likely to develop this condition:
• African American, Hispanic, or Americans of
Indian origin
• Family history of kidney disease or high
blood pressure
• Poor control of blood pressure
• Poor control of blood sugars
• Type 1 diabetes before age 20
• Smoking, Alcoholism
• Abnormal lipid levels
Causes:
Review Articles

5
Diabetic nephropathy generally goes along with
other diabetic complications including high blood
pressure, retinopathy and blood vessel changes
(vasculopathy).
The pathophysiology of diabetic nephropathy m a n i f e s t s h i s t o l o g i c a l l y a s d i a b e t i c glomerulosclerosis and is characterized by glomerular basement membrane thickening and mesangial expansion with increased extracellular matrix deposition. Mesangial expansion in diabetic glomerulosclerosis may be considered the result of an imbalance between mesangial matrix protein production and degradation, favor ing matr ix protein accumulat ion. Overproduction of mesangial matrix proteins may be the result of glomerular hypertension and/or hyperglycemia-driven synthesis of prosclerotic
Pathophysiology:
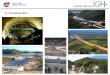
Fig 1. Graphic presentation of the natural history of diabetic glomerulosclerosis. Initially there is glomerular hyper
filtration and microalbuminuria. Microalbuminuria is followed by macroalbuminuria (dipstick positive
proteinuria), the onset of macroproteinuria heralds the beginning of a relentless decline in GFR at the rate
approximately 1ml/mt/month (at a BP of 140/90 mm hg). If GFR is 70ml/mt at onset of macroalbuminuria
and dialysis is indicated at a GFR of 10ml/mt, 65 months would pass from the onset of proteinuria to the need
for renal replacement therapy. The goal of therapy is to slow the rate of loss of GFR. Reducing the rate of loss
of GFR from 1 ml/minute/month to 0.5 ml/min/month would translate into a doubling of the time for the
need for dialysis (130 months). Modified from Molitch, Diabetes Care 17:756, 1994.
cytokines such as transforming growth factor-B, 2,3angiotensin II, and/or other growth factors.
Alternatively, elevated glucose levels may inhibit matrix protein degradation through non-enzymatic glycosylation and/or through the
4 inhibition of protein degradative pathways. Thus, the mediators of mesangial expansion constitute reasonable therapeutic targets when crafting a treatment strategy for diabetic nephropathy. Understanding the natural history of diabetic glomerulosclerosis is important to design therapeutic interventions, as well as gauging responses to therapy. In this regard, Parving demonstrated the deleterious effect of hypertension on renal function in proteinuric
5,6 diabetics. Of equal or greater value in that report was the demonstration of the expected rate of loss of glomerular filtration rate (GFR) over time, in patients with diabetic nephropathy.

6
Figure 1. is a schematic summary of the natural
history of diabetic glomerulosclerosis, and
demonstrates the relationship between
albuminuria and the loss of GFR over time. The
model is based on the following assumptions: (a)
all macroscopic (dipstick positive) proteinuria is
preceded by a phase of microalbuminuria
(microalbumin 30-300 mg/day); (b) the
appearance of dipstick positive proteinuria
heralds the beginning of a linear, irreversible loss
of GFR; and (c) GFR is lost, on average, at the rate
of 1 ml/min/month.
Clinical diagnosis of diabetic nephropathy
Symptoms :
Examination and Tests
Early stage diabetic nephropathy has no
symptoms. Over time, the kidney's ability to
function starts to decline. Symptoms develop late
in the disease and may include:
• Fatigue
• Foamy appearance or excessive frothing of
the urine
• Frequent hiccups
• General ill feeling
• Generalized itching
• Headache
• Nausea and vomiting
• Poor appetite
• Swelling of the legs
• Swelling, usually around the eyes in the
mornings; general body swelling may
occur with late-stage disease
• Unintentional weight gain (from fluid
buildup)
The earliest clinical evidence of renal involvement
in diabetes is the presence of small amount of
albumin in urine (30-300mg/24 hrs). This is
labeled microalbuminuria. Protein may appear in
the urine for 5 to 10 years before other symptoms
develop. In type 1 Diabetes 80%, who develop
microalbuminuria, will develop macroproteinuria
and around 50% will eventually develop ESRD. In
type 2 Diabetes 20-40% of patient with
microalbuminuria develop overt proteinuria and
only about 20% go on to develop ESRD. However
presence of microalbuminuria in addition to
being a manifestation of renal involvement, is also
a marker of cardiovascular risk. Patients with
sustained microalbuminuria need to be
aggressively managed for cardiovascular risk 7
factors as well.
Screening in individual with type I diabetes should
begin after 5 years disease duration. In type 2 DM,
screening should begin at diagnosis, there after
for the presence of microalbuminuria should be
performed annually.
Screening for microalbuminuria can be
performed by three methods:-
1. Measurement of albumin to creatinine
ratio (ACR) in a random spot collection
2. 24 hr collection with creatinine, allowing
the simultaneous measurement of
creatinine clearance.
3. Screening with reagent tables or dipstick
for microalbumin have sensitivity 95% and
specificity93%. Reagent strips only
indicate concentration and do not correct
the creatinine as the spot albumin-7
creatinine ratio does.
1. Microalbuminuria – Random ACR 30-300
mg on 2 out of 3 occasion
2. Macroalbuminuria- Random ACR >300 mg
or positive protein dipstick
3. Diabetic nephropathy Estimated GFR < 60
ml/min for at least 3 months.
Screening of microalbuminuria is invalid in
following conditions:
In uncontrolled hyperglycaemia, febrile illness,
following strenuous exercise, uncontrolled
hypertension or heart failure and presence of
urinary infection as all these conditions can cause 7transient proteinuria.
High blood pressure often goes along with
diabetic nephropathy. One can have high blood
pressure that develops rapidly or is difficult
to control.
SCREENING FOR MICROALBUMINURIA:-
Definitions :-

7
Laboratory tests that may be done include:
• BUN
• Serum creatinine
The levels of these tests will increase as kidney
damage gets worse. Other laboratory tests that
may be done include:
• 24-hour urine protein
• Blood levels of phosphorus, calcium,
bicarbonate, PTH, and potassium
• Hemoglobin
• Hematocrit
• Protein electrophoresis - urine
A kidney biopsy confirms the diagnosis. However,
clinical diagnosis can be done without a biopsy if
the following three conditions are met with:
1. Persistent protein in the urine
2. Diabetic retinopathy
3. No other kidney or renal tract disease
A biopsy may be done, however, if there is any
doubt in the diagnosis.
Diabetics with heavy proteinuria, but lacking the
disease for a sufficient period of time and/or
retinopathy, may require renal biopsy. These
p a t i e n t s m a y s u f f e r f r o m p r i m a r y
glomerulopathies such as membranous 8
nephropathy, or other glomerular diseases.
Diabetic glomerulopathy is the most common
cause of nephrotic syndrome. Thus, early in the
course of the disease, the serum creatinine is
normal despite heavy proteinuria (> 3 grams/24
hours). In this regard, a diabetic patient
presenting with elevated serum creatinine in the
absence of macroscopic proteinuria should
suggest additional diagnostic possibilities (such as
other glomerulopathies) . The diagnostic utility of
proteinuria is less useful in patients treated with
angiotensin converting enzyme inhibitors (ACEi)
or angiotensin II receptor blockers (ARBs), since
both classes of drugs are known to reduce 9,10
glomerular proteinuria.
MEDICAL THERAPY OF DIABETIC NEPHROPATHY :
The medical therapy of diabetic glomerulo-
sclerosis includes strict control of blood glucose
levels, aggressive blood pressure control,
angiotensin II inhibition, and dietary protein
restriction. Additional therapeutic targets include
microalbuminuria and macroproteinuria. An
approach to each of these parameters is discussed
below.
1. Tight blood glucose control
The DCCT (Diabetes Control and Complications
Trial) demonstrated the importance of tight blood
glucose control in slowing the development of 13
proteinuria in Type 1 diabetics. In this regard,
patients randomized to tight glucose control
(HbA1C levels < 6.5%) versus regular control (8-
9%), demonstrated 39 and 54% lower rates of
development of microalbuminuria and
macroalbuminuria, respectively, over the two
years of the trial.
Similarly the UKPDS(United Kingdom Prospective
Diabetes Study) in Type II diabetes showed a 25%
risk reduction in microvascular complication in
the intensively treated group.
2. Blood pressure control
Hypertension in diabetic patient may be due to
coexisting “essential” hypertension, or due to
myriad of other secondary causes, such as renal
vascular disease. Isolated systolic hypertension
has been attributed to the loss of elastic
compliance of atherosclerotic large vessels. Both
systolic and diastolic hypertension markedly
accelerates the progression of diabetic
nephropathy and aggressive antihypertensive
management is able to greatly decrease the rate
of fall of GFR. Appropriate antihypertensive
intervention can significantly reduce mortality
from 94 to 45% and a reduction in the need for
dialysis and transplantation from 73 to 31% 16
years after development of overt nephropathy.
Choice of antihypertensive therapy:-
One needs to be careful about:-
- Use of ACEI and ARBs as these may lead to
hyperkalemia in patients of advanced renal
insufficiency,
- ACEI are contraindicated in bilateral renal
artery stenosis and in pregnancy.

8
- Beta blockers are contraindicated in
peripheral vascular disease.
Targets for blood pressure control:-
• <130/80 mm hg in absence of proteinuria
• <125/75 mm hg in presence of proteinuria.
3. Angiotensin II inhibition : The ACE inhibitor
trial in diabetic nephropathy was the first
randomized, placebo controlled trial that
showed the beneficial effect of ACE inhibitors
i n t h e t r e a t m e n t o f d i a b e t i c 11 glomerulosclerosis. Subsequent studies have
confirmed this observation for both ACE 10,12 inhibitors and ARBs. Most agree that ACEI
a re f i rst l ine therapy for d iabet i c 10
glomerulosclerosis, but ARBs are regarded by 10 some as equivalent. The beneficial effect of
angiotensin II inhibition may result from:
a) a decline in glomerular hypertension (with 13slowing of mesangial expansion)
b) a reduction in proteinuria (with an
expected decrease in proteinuria-14
associated prosclerotic events), and/or
c) a decrease in angiotensin II stimulated 15,16
TGF-ß synthesis.
4. Dietary protein restriction : In some reports,
dietary protein restriction has been shown to 17slow the loss of GFR in proteinuric diabetics,
although the data are not conclusive. Protein
restricted diets (0.6-0.8 g/kg body wt/day)
decrease glomerular hypertension, the
production of prosclerotic cytokines, 18
proteinuria, and glomerulo-sclerosis, and
remain a viable therapeutic option for
compliant patients.
5. Microalbuminuria : Microalbuminuria
predates the development of macroscopic
proteinuria. Macroscopic proteinuria is a 14major risk factor for progression to ESRD, thus
measures to reverse microalbuminuria may
retard development of clinical nephropathy.
Patients with microalbuminuria treated with
ACEi demonstrate slower progression to 6
macroproteinuria and renal failure. American
Diabetic Association (ADA) guidelines suggest
assessing for microalbuminuria (normal < 30
mg/24 hours or less 30 mcg/mg creatinine for
a spot urine collection) at the time of diagnosis
in all type 2 diabetics, in all type I diabetics with
disease duration > 5 yrs, and annually 19 thereafter in both groups. Early and
aggressive therapy of microalbuminuria, taken
along with angiotensin II inhibition, is
expected to slow disease progression.
6. Macroproteinuria
Heavy proteinuria is a risk factor for progressive 20renal failure, 16 including diabetic nephropathy.
There is abundant evidence that abrogating
proteinuria with dietary and antihypertensive 21
interventions, and/or ACE inhibitors, 1 and/or 22,23 ARBs, results in a slower loss of GFR in
proteinuric states. In this regard, combination
therapy with both ACE inhibitors and ARBs may 24
provide benefit over ACE inhibitors alone.
Finally, nephrotic diabetics treated with ACE
inhibition, and exhibiting a reduction in
proteinuria to < 1 gm / day, demonstrated stable 25
renal function for up to 8 to 15 years. Taken
together, therapeutic measures directed at
reducing macroscopic proteinuria would be
expected to slow the progression of diabetic
nephropathy, and angiotensin II inhibition is the
mainstay of therapy for attaining that goal.
Other aspects of treatment : Treatment of
progressive renal disease includes prevention of
renal osteodystrophy with sodium and phosphate
restriction and use of phosphate binders,
treatment and prevention of anaemia etc.
Avoidance of nephrotoxic drugs in proteinuric
diabetic patients will prevent form onset of acute
kidney injury.
Radiocontrast media are nephrotoxic in diabetic
nephropathy and careful hydration is mandatory
in these cases if it is done.

9
SPECIAL CONSIDERATIONS
Insulin metabolism in CKD : Unutilized insulin is
excreted by kidney normally which accumulates
in CKD. So if we fail to reduce insulin dose as
kidney disease progresses, patients will
experience hypoglycaemia. So reducing insulin
dose and switching to short acting insulin
analogues is recommended in this situation. It is
recommended to avoid long acting Insulins in CKD
patients.
Oral antidiabetic drug: 97% of the most
commonly used oral antidiabetic drug Metformin
is excreted by normal kidney within 12 hrs. In CKD
it will accumulate and lead to lactic acidosis, a
serious condition.
So metformin should be stopped when the eGFR is 2<35 ml/mt/1.73 m correlates to serum creatinine
o f a p p rox m i m ate l y 1 . 7 m g / d l . O l d e r
sulfonylurea(SU) are excreted mainly through
kidney. Only 10% of second line SU are excreted by
kidney but are long acting and may accumulate in
CKD, so we must be cautious while using these.
Meglitinides and Thiazolidinediones are not
excreted by kidneys. These do not cause
hypoglycaemia.
Monitoring glycaemic control in CKD : As kidney
disease develops, the turnover of red blood cells
becomes abnormal. Usually there is prolonged life
span of RBCs, perhaps because the person is
anaemic. So hemoglobin has more time to
become glycated. In such conditions HbA1 in c
kidney disease may be falsely high. Hb may also be
carbamylated with some of the waste products,
which accumulate in uremia and these
compounds will interfere with the measurement
of HbA1 . This is one more reason for HbA1 to be c c
falsely high. Correction of anaemia may lead to 26decrease HbA1 level.c
Renal replacement therapy:
1. Hemodialysis : Hemodialysis and peritoneal
dialysis are the two forms of dialysis used to treat
diabetic patients with end stage renal disease.
Survival analysis shows the two modalities are 27
comparable with regard to patient outcome.
However, when compared to non-diabetics,
diabetic patients on dialysis do substantially 28
worse, with five-year survival rates as low as 5% 29 for elderly type 2 diabetics. With meticulous
management, others have shown three-year 28 survival rates as high as 58%. .The reasons for
poor survival rates relate to the high incidence of
preexisting cardiovascular disease, late referral
both for predialysis care, as well as vascular access
placement, malnutrition, and co-existing vascular
problems (in particular, peripheral vascular 28disease with associated ischemic toes and feet).
Furthermore, diabetes and smoking have been
shown to be significant risk factors for
atherosclerotic heart disease in dialysis patients, 30
similar to what is seen in the general population.
The anemia of chronic renal disease may further
complicate the course of patients with significant
coronary artery disease. Taken together, these
data suggest that the survival of diabetic patients
on hemodialysis may be optimized with
aggressive attention to risk factors for
card iovascu lar d i sease (hypertens ion ,
dyslipidemia, smoking, etc.), awareness and
therapy of diabetic foot problems, and early
nephrology referral (as GFR falls or with
progressive proteinuria) for vascular access
placement and anemia management.
2. Peritoneal dialysis : The second option for renal
replacement therapy in diabetic patients with
ESRD, is peritoneal dialysis. When compared to
hemodialysis, fewer patients are treated with
peritoneal dialysis. Patients opting for peritoneal
dialysis tend to be healthier and more involved in
their medical care. While no clear survival
advantage for peritoneal or hemodialysis has
been demonstrated, patients treated with
peritoneal dialysis may experience labile blood
glucose levels (attributed to the high glucose
concentrations inherent to PD dialysate) and
increased risk of malnutrition (secondary to 31
excessive protein losses in dialysate effluent).

10
3. Transplantation : By far the best treatment for
ESRD from diabetes is kidney transplantation.
Kidney transplantation in diabetics with end-stage
renal disease may include kidney transplantation
a l o n e , o r c o m b i n e d k i d n e y - p a n c re a s
transplantation. The former treats renal failure,
the latter both renal failure and diabetes. Patient
survival following kidney transplantation without
a pancreas has consistently been demonstrated to
be superior to any form of dialysis. Data from the
Organ Procurement and Transplantation Network
reported one-, three-, and five-year patient
survival rates for transplanted diabetics of 90, 79 32
and 66%, respectively. This compares to a two
year survival rate in diabetic patients on 29
hemodialysis of 58%. The improved survival of
renal transplant patients over those treated with
hemodialysis must be interpreted in light of the
fact that they are selected for transplantation,
whereas patients with extensive co-morbidities
tend to remain on dialysis. Living donor
transplants confer an allograft survival advantage
over cadaveric donors, with three-year allograft
survival rates of 88 and 78% for living and 32cadaveric donor transplants, respectively.
However, both modalities are superior to dialysis
with three year patient survival rates of 3 2
a p p r o x i m a t e l y 8 8 - 9 4 % . P r e e m p t i v e
transplantation is renal transplantation that is
performed prior to instituting dialysis. Preemptive
transplantation may confer a survival advantage
that is superior to transplanting patients on
dialysis. In this regard, the time spent on dialysis
prior to transplantation portends worse survival
rates for patients. For example, in patients on
dialysis < 6 months, 12-24 months, or >48 months
had mortality rates of 21%, 41%, and 72%, 33,34,35 respectively. A similar trend for allograft
survival was seen in cadaveric transplants
performed in patients receiving hemodialysis for
more than two years prior to the transplant. In
those studies, the allograft survival rate was only 3639% after ten years.
Summary
The rising incidence of diabetes means that
clinicians can expect to find an increased rate of
diabetic nephropathy, and increasing numbers of
patients requiring renal replacement therapy.
Understanding the natural history of diabetic
nephropathy, the early recognition of diabetic
complications, and timely initiation of therapy to
slow progression are cornerstones in the
management of this condition. Aggressive
treatment of hyperglycemia and hypertension,
the use of angiotensin II inhibitors, and timely
therapy of micro and macroproteinuria are
essential features of optimal therapy. For patients
reaching end stage renal failure, renal
replacement options include dialysis and kidney
transplantation, with transplantation conferring a
substantial survival advantage.
References:
1. Strojek K et al, Nephropathyof type 2
diabetes: Evidence for hereditary factor.
Kidney Int. 51:1602-1607,1997.
2. Hostetter T, Rennke H, Brenner B. The case
for intrarenal hypertension in the
initiation and progression of diabetic and
other glomerulopathies. Am J Med. 1982;
72:375.
3. Ziyadeh F, Han D. Involvement of
transforming growth factor-b and its
receptors in the pathogenesis of diabetic
nephropathy. Kidney Int . 1997; 52:S7-S11.
4. Brownlee M. Biochemistry and molecular
cell biology of diabetic complications.
Nature. 2001; 414(6865):813-20.
5. Parving H, Smidt U, Andersen A, Svendsen
P. Early aggressive antihypertensive
treatment reduces rate of decline in
kidney function in diabetic nephropathy.
Lancet.
1983; 1:1175-1179.
6. Parving HH. Diabetic nephropathy:
prevention and treatment. Kidney Int.
2001; 60(5):2041-55.

11
7. Anjali, Jacob J J, Nephropathy in Diabetes; thpractical guide to Diabetes Mellitus: 4
Edn.;146-148
8. Carstens S, Hebert L, Garancis J, Piering W,
Lemann Jr J. Rapidly progressive
glomerulonephritis superimposed on
diabetic glomerulosclerosis: recognition
and treatment. JAMA. 1982; 247:1453-
1457.
9. Brenner BM. Regarding: “Management of
glomerular proteinuria: a commentary.” J
Am Soc Nephrol. 2004; 15(5):1354-5;
discussion 1356-7.
10. Lewis E, Hunsicker L, Bain R, Rohde R. The
effect of angiotensin converting enzyme
inhibition in diabetic nephropathy. N Engl J
Med. 1993; 329:1456-62.
11. Lewis EJ, Lewis JB. ACE inhibitors versus
angiotensin receptor blockers in diabetic
nephropathy: is there a winner? J Am Soc
Nephrol . 2004; 15(5):1358-60.
12. Hostetter T. Prevention of end-stage renal
disease due to type 2 diabetes. N Engl J
Med. 2001; 345:910-911.
13. Zatz R, Bunn B, Meyer T, Anderson S,
Rennke H, Brenner B. Prevention
o f d i a b e t i c g l o m e r u l o p a t h y b y
pharmacolog ica l amel iorat ion of
glomerular capillary hypertension.
J Clin Invest. 1986; 77:1925.
14. Wilmer WA, Rovin BH, Hebert CJ, Rao SV,
Kumor K, Hebert LA. Management of
glomerular proteinuria: a commentary. J
Am Soc Nephrol. 2003; 14(12):3217-32.
15. Nahman N, Kronenberger J, Sferra T, Clark
K. Transcriptional activation of the TGF-b
gene by angiotensin II: implications for
fibronectin biosynthetic pathways
in human mesangial cells. J Amer Soc
Nephrol. 1997; 8:522A.
16. Siegert A, Ritz E, Orth S, Wagner J.
Differential regulation of transforming
growth factor receptors by angiotensin II
and transforming growth factor-beta1 in
vascular
smooth muscle. J Mol Med . 1999;
77(5):437-45.
17. Zeller K, Whittaker E, Sullivan L, et al. Effect
of restricting dietary protein on the
progression of renal failure in patients with
insulin-dependent diabetes mellitus.
N Engl J Med. 1991; 324:78-84.
18. Klahr S, Levey AS, Beck GJ, et al. The effects
of dietary protein restriction and blood-
pressure control on the progression of
chronic renal disease. Modification of Diet
in Renal Disease Study Group [see
comments]. N Engl J Med . 1994;
330(13):877-84.
19. Molitch ME, DeFronzo RA, Franz MJ, et al.
Nephropathy in diabetes. Diabetes Care.
2004; 27 Suppl 1:S79-83.
20. Breyer JA, Bain RP, Evans JK, et al.
Predictors of the progression of renal
insufficiency in patients with insulin-
dependent diabetes and overt diabetic
nephropathy.
The Collaborative Study Group. Kidney Int.
1996; 50(5):1651-8.
21. Peterson JC, Adler S, Burkart JM, et al.
Blood pressure control, proteinuria, and
the progression of renal disease. The
Modification of Diet in Renal Disease
Study.
Ann Intern Med. 1995; 123(10):754-62.
22. Parving HH, Lehnert H, Brochner-
Mortensen J, Gomis R, Andersen S, Arner P.
The effect of i rbesartan on the
development of diabetic nephropathy in
patients with type 2 diabetes. N Engl J
Med. 2001; 345(12):870-8.
23. Lewis EJ, Hunsicker LG, Clarke WR, et al.
Renoprotective effect of the angiotensin-
receptor antagonist irbesartan in patients
with nephropathy due to type 2 diabetes.
N Engl J Med. 2001; 345(12):851-60.

12
24. Jacobsen P, Andersen S, Rossing K, Jensen
BR, Parving HH. Dual blockade of the renin-
angiotensin system versus maximal
recommended dose of ACE inhibition in
diabetic nephropathy. Kidney Int. 2003;
63(5):1874-80.
25. Wilmer WA, Hebert LA, Lewis EJ, et al.
Remission of nephrotic syndrome in type 1
diabetes: long-term follow-up of patients
in the Captopril Study. Am J Kidney
Dis. 1999; 34:308-14.
26. Mashall S etal, Chronic kidney Disease in
Diabetics: Current best practice and
possibilities for future. Novonordisk
Diabetes Update. Proceedings 2009; 21-28
27. Locatelli F, Pozzoni P, Del Vecchio L. Renal
replacement therapy in patients with
diabetes and end-stage renal disease. J Am
Soc Nephrol. 2004; 15 Suppl 1:S25-9.
28. Schwenger V, Zeier M, Ritz E. How can the
poor outcomes for diabetic dialysis
patients be improved? Semin Dial. 2004;
17(3):186-7.
29. Koch M, Kutkuhn B, Grabensee B, Ritz E.
Apolipoprotein A, fibrinogen, age, and
history of stroke are predictors of death in
dialysed diabetic patients: a prospective
study in 412 subjects. Nephrol Dial
Transplant. 1997; 12(12):2603-11.
30. Cheung AK, Sarnak MJ, Yan G, et al.
Atherosclerotic cardiovascular disease
risks in chronic hemodialysis patients.
Kidney Int. 2000; 58(1):353-62.
31. Xue JL, Everson SE, Constantini EG, et al.
Peritoneal and hemodialysis: II. Mortality
risk associated with initial patient
characteristics. Kidney Int. 2002;
61(2):741-6.
32. Organ Procurement and Transplantation
Network. www.optn.org/latestData/
rptStrat.asp. 2004.
33. Meier-Kriesche HU, Port FK, Ojo AO, et al.
Effect of waiting time on renal transplant
outcome. Kidney Int. 2000; 58(3):1311-7.
34. Mange KC, Joffe MM, Feldman HI. Effect of
the use or nonuse of long-term dialysis on
the subsequent survival of renal
transplants from living donors. N Engl
Med. 2001; 344(10):726-31.
35. Kasiske BL, Snyder JJ, Matas AJ, Ellison MD,
Gill JS, Kausz AT. Preemptive kidney
transplantation: the advantage and the
advantaged. J Am Soc Nephrol. 2002;

13
Original Papers
Prevalence of phage types & biotypes among Salmonella Typhi and Salmonella Paratyphi A isolates from Rourkela, Orissa.
Seshadri S Bhattacharya, Usha Das
Deptt. of Microbiology,
Address for communication :SS Bhattacharya
Deptt. of Microbiology, Ispat General Hospital, Rourkela, Orissa.
Email: [email protected]
ABSTRACT
Key words
Introduction
Aim of this study was to highlight the changes in prevalence of phage types encountered among Salmonella isolates from Rourkela. Besides S. Typhi as the main causative agent of enteric fever, S. Paratyphi A has also been emerging with increasing rate as the other causative agent of enteric fever from different parts of India including Rourkela. This retrospective study was carried out between September 2005 and August 2006 with 1454 patients attending out-patient-departments (OPD) and wards of Ispat General Hospital, Rourkela, India. Phage typing and biotyping was performed for randomly chosen isolates of S. Typhi (N=36) and S. Paratyphi A (N=12). A distinctive change has been noticed in the prevalence of phage types compared to their prevalence pattern reported earlier. Phage type 40 was the most commonly encountered phage among S. Typhi isolates followed by type E1. Susceptibility testing was performed for all 112 isolates of Salmonella including 48 strains chosen randomly for phage typing and biotyping. Though 4-5% of Salmonella isolates showed resistance to ciprofloxacin, they were highly sensitive to both aminoglycos ides and th ird generat ion cephalosporins. Diversity among the phage types encountered among S. Typhi isolates was probably due to the diverse origin of those phages. Salmonella enteric serotype Typhi is the most commonly occurring causative agent of
1.2enteric fever in India.
Prevalence; Phage typing; Biotypes; Randomly chosen; Susceptibility testing; Diversity.
Salmonella enteric serotype Typhi is the most commonly occurring causative agent of enteric
1,2 fever in India However, isolation of Salmonella enterica serotype Paratyphi A causing the same disease have been reported with an increasing
3,4 trend. In Rourkela, we have been reporting 5
S.Typhi causing enteric fever since 1996, whereas isolation of S.Paratyphi A causing the same disease has been encountered in this place since
62002.
Phage typing is a major means of epidemiological tracing as strains within a particular serotype may be differentiated into a number of phage types, and may help to define groups of persons who have been infected with the same strain from the same source. Again, combination of biotyping with phage typing gives a finer discrimination of strains in tracing out the source of infection. The use of phage typing and biotyping for epidemiological tracing had been documented
1since 1982 in different parts of India.
Phage typing and biotyping of both Salmonella Typhi and Salmonella Paratyphi A had been
6,7 reported from Rourkela in 2006 and 2007. There was a noticeable change in the prevalence pattern of phage types encountered among S.Typhi isolates in 2005-2006 in comparison to the phage types found in 2004-2005. In this retrospective, hospital based study, we have highlighted the changes in the prevalence pattern of phage types and biotypes among the Salmonella isolates chosen randomly. The susceptibility pattern of Salmonella isolates including the typed strains have also been reported in this communication.
This study was conducted between September 2005 and August 2006. A total of 1454 patients attending out-patient departments (OPDs) and wards of Paediatric and Medicine departments of Ispat General Hospital , Rourkela, Orissa,
.
Materials & methods

14
suspected of having enteric fever or pyrexia of unknown origin (PUO) were included in this study.
A total of 1454 blood samples were included in
this study. Irrespective of repeat sample we have
taken into account only one sample from each
patient. Only positive isolation was considered for
the patients having both positive and negative
results.
Clinical samples of blood were collected in brain
heart infusion broth with sterile precautions and 0
incubated aerobically at 37 C for 48 hours. Three
subcultures were done on blood agar, MacConkey
agar and Salmonella-Shigella agar and incubated 0
aerobically at 37 C for 18-24 hours. In negative
cases subcultures were done for one week.
Isolation of S. Typhi and S. Paratyphi A was 8established by conventional methods.
Identification of these two serotypes was
established by biochemical and serological testing 8,9
with factor sera. Antibiotic susceptibility testing
was performed by Kirby Bauer disk diffusion 10
method, with the modifications recommended
by the National Committee for Clinical Laboratory 11 Standards (NCCLS). Antimicrobials agents tested
were ampicillin, co-trimoxazole, chloromycetin,
gentamicin, amikacin, ciprofloxacin, cephotaxime
and ceftriaxone.
Randomly selected strains of both S. Typhi and
S. Paratyphi A were sent to the National
Salmonella Phage Typing Centre, Lady Hardinge
Medical College, New Delhi, India, for phage
typing and biotyping.
Out of 1454 patients, 1052 were children (72.35%)
and remaining 402 were adults (27.65%). Among
Results
Host organism Phage type Biotype No. of isolates
S. Typhi A I 5
(N=27) D1 I 1
E1 I 17
E9 I 1
J1 I 3
S. Paratyphi A 4 II 3
(N=24) 6 II 21
Table 1. Phage types encountered among S. Typhi ans S. Paratyphi
A isolates in Rourkela between September 2004 and August 2005.
the patients, 768 were males (52.81%) and 686
were females (47.19%).
Of 1454 patients, 112 were positive for Salmonella
isolates giving a per cent positivity of 7.70. Of 112
Salmonella isolates, 92 were S. Typhi strains and
remaining 20 were S. Paratyphi A strains. Almost
75 per cent of isolates were from pediatric
population, among which 52.38% were boys and
47.62% were girls.
In 2004-2005, the predominant phage type
encountered among S. Typhi strains was E1,
followed by phage type A (Table 1). In the present
study (2005-2006), predominant phage type
encountered among S. Typhi isolates was 40,
which itself is a rare and exotic phage type in India.
Second most common phage type of S. Typhi
isolates in this study was E1 and number of Vi-
Negative strains was 4 (Table 2). In both the
studies mentioned, the predominant phage type
found among S. Paratyphi A strains was type 6,
followed by phage types of either 4 or 1.
Host organism Phage type Biotype No. of isolates
S. Typhi A I 1
(N=36) D1 I 1
E1 I 8
J1 I 2
40 II 19
USV-2 II 1
Vi-Negative I 4
S. Paratyphi A 1 II 1
(N=12) 6 II 11
Table 2. Phage types encountered among S. Typhi and S. Paratyphi
A isolates in Rourkela between September 2005 and August 2006.
Antibiotics S. Typhi (%) S. Paratyphi A(%)
(N=92) (N=20)
Ampicillin 82 (89.13) 11 (55)
Co-trimoxazole 74 (80.43) 11 (55)
Chloramphenicol 85 (92.39) 12 (60)
Gentamicin 90 (97.82) 19 (95)
Amikacin 91 (98.91) 20 (100)
Ciprofloxacin 88 (95.65) 19 (95)
Cephotaxime 91 (98.91) 20 (100)
Ceftriaxone 91 (98.91) 19 (95)
Table 3. Susceptibility pattern of S. Typhi and S. Paratyphi
A isolates in Rourkela between September 2005 and August 2006.

15
phage type 40, which itself is a rare and exotic
phage type of S. Typhi in India. It is worth
mentioning that two more rare and exotic phage
types of multi-drug resistant (MDR) S. Typhi
strains, namely type 51 and type 28, caused
outbreaks in Kolkata and Mumbai respectively,
but in case of phage type 40, most of the strains
were not multi-drug resistant. Emergence of Vi-
negative strains among S. Typhi isolates in
Rourkela was another important finding during
the same time.
Till date, not many study-reports are available
regarding phage typing and biotyping of S.
Paratyphi A. A study among the patients (coming
from Indian subcontinents) in Kuwait reported
that 66% of S. Paratyphi A isolates belonged to 13 phage type I. Another study from Nagpur also
showed that the prevalent phage type among S.
Paratyphi A isolates from the local population was 14
type I. The most commonly encountered phage
type of S. Paratyphi A isolates from Rourkela was
type 6, a finding which hardly got any other
contemporary reference in India. From 1992 to
2003, commonest biotype of S. Paratyphi A in 13,14,15 India was type I, but in our study all the
phages of S. Paratyphi A belonged to biotype II.
The commonest biotype encountered among
S. Typhi strains isolated from Kolkata, Nagpur and 12,16,17 Ludhiana was type I, but in our study, biotype I
accounted for 44.4% of S. Typhi isolates and
remaining 55.6% were biotype II.
Susceptibility pattern to ampicillin and
chloramphenicol were very encouraging for 5,6,7 S.Typhi isolates as reported earlier, though it
was not that much inspiring for S.Paratyphi A
isolates in this study. In this study, differences in
per cent susceptibility between S. Typhi and
S. Paratyphi A isolates for ampici l l in,
chloramphenicol and ciprofloxacin were
statistically significant (P<0.05), whereas for the
rest of the antimicrobials tested, differences in per
cent susceptibility were found insignificant
(P>0.05). Although 4-5% resistance to
ciprofloxacin among Salmonella isolates was a
matter of concern, very high susceptibility of
those strains to aminoglycosides (gentamicin and
amikacin) and third generation cephalosporins
1,12
Most of the phage types of S. Typhi isolates
belonged to biotype I, except for phage type 40
and USV-2. All the phage types of S. Paratyphi A
isolates belonged to biotype II (Table 2).
Ampicillin and chloramphenicol sensitivity among
S. Typhi isolates was found very high in our study,
though 40-45% of S. Paratyphi A isolates showed
resistance to these antimicrobials (Table 3).
Isolates of both S. Typhi and S. Paratyphi A showed
remarkably high susceptibility to gentamicin and
amikacin. Resistance to ciprofloxacin was 4-5%
among the isolates of S. Typhi and S. Paratyphi A.
Susceptibility to cefotaxime and ceftriaxone was
very high among the isolates of both S. Typhi and
S. Paratyphi A (Table 3).
Randomly chosen strains of both S.Typhi and S.
Paratyphi A for phage typing and biotyping were
also found remarkably sensitive to the
antimicrobials used in our study. Out of 36 isolates
of S. Typhi, only 2 strains showed resistance to
ciprofloxacin and 1 strain resistant to
cephotaxime. Out of 12 strains of S. Paratyphi A
randomly chosen for phage typing and biotyping,
only 3 strains showed resistance to ampicillin, co-
trimoxazole and chloramphenicol. Interestingly,
all these 3 MDR strains of S. Paratyphi A belonged
to phage type 6.
Phage typing is one of the most important means
of epidemiological tracing. In 1982-89, the order
of frequency of phage types in north and central
India was A, E, O, while in south the second
predominant phage type was O. From 1990
onwards , E1 became the most commonly phage
type except in south India, where phage type O
was the predominant type. In 1992, the order of
frequency had become E1, O, A throughout the
country. However, there was hardly any report of
phage type O from any part of the country since 121994.
In our findings of phage types encountered among
S. Typhi strains from Rourkela, E1 was the most
commonly occurring phage type in 2004-2005
and second-most common phage type in
2005-2006. One strikingly different finding in
2005-2006 study was the highest occurrence of
Discussion
1

16
(cephotaxime and ceftriaxone) was highly
encouraging, and can be used judiciously in case
of ciprofloxacin resistance.
A diversity among phage types of S. Typhi isolates
has been noticed, though in case of S. Paratyphi A,
mostly phage type 6 was encountered. This
diversity of phage types observed in this eastern
part of India might be due to the diverse origin of
these phage types. The diversity of origin of these
phages again may be due to the migration of
population to and from Rourkela, an industrial
(steel) township, with respect to other parts of the
country. Further studies are required regarding
the epidemiological tracing especially for the
exotic phage type 40 of S. Typhi isolates.
References
1. Pillai PK, Prakash K. Current status of drug
resistance and phage types of Salmonella
typhi in India. Indian J Med Res 1993; 97:
154-158.
2. Sanghavi SK, Mane MP, Niphadkar KB.
Multidrug resistant Salmonella serotypes.
Indian J Med Microbiol 1999; 17(2): 88-90.
3. Sood S, Kapil A, Dash N, Das BK, Goel V and
Seth P. Paratyphoid fever in India. Emerg
Infect Dis 1999; 5: 483-484.
4. Chandel DS, Chaudhary R, Dhawan B,
Pandey A, Dey AB. Drug-resistant Salmonella
enterica serotype Paratyphi A in India.
Emerg Infect Dis 2000; 6: 420-421.
5. Bhattacharya SS, Das Usha. Occurrence of
Salmonella typhi infection in Rourkela,
Orissa. Indian J Med Res 2000; 111 : 75-76.
6. Bhattacharya SS, Das Usha. A sudden rise in
occurrence of Salmonella paratyphi A
infection in Rourkela, Orissa. Indian J Med
Microbiol 2007; 25 : 78-79.
7. Das Usha, Bhattacharya SS. Antibiogram,
phage typing & biotyping of Salmonella
Typhi & Salmonella Paratyphi a from
Rourkela, Orissa. Indian J Med Res 2006; 124
: 109-111.
8. Sleigh JD, Duguid JP. Salmonella. In: Collee
JG, Fraser AG, Marmion BP, eds. Practical
6
thMedical Microbiology. 13 ed. Edinburg :
Churchill Livingstone, 1984: 456-81.
9. Baron EJ, Peterson LR, Finegold SM. Bailey , th
and Scott s Diagnostic Microbiology. 9 ed.
St. Louis, Missouri : Mosby, 1994 : 362-85.
10. Bauer AW, Kirby WM, Sherris JC and Truck
M. Antibiotic susceptibility testing by a
standardized single disc method. Am J Clin
Pathol 1996; 45 : 493-6.
11. National Committee for Clinical Laboratory
Standards. Performance standards for thantimicrobial disc susceptibility tests, 6 ed.
Approved standard M2-A6. Wayne, Pa :
National Committee for Clinical Laboratory
Standards; 1997.
12. Saha MR, Palit A, Chatterjee NS, Dutta P,
Mitra U and Bhattacharya SK. A prospective
study of phage types & biotypes of
Salmonella enterica serotype Typhi isolated
from hospitalized children in Kolkata, India.
Indian J Med Res 2003; 117 : 201-204.
13. Panigrahi D, Chugh TD, West PWJ, Dimitrov
TZ, Groover S and Metha G. Antimicrobial
susceptibility, Phage typing and Plasmid
profile of Salmonella enterica serotype
paratyphi A strains isolated in Kuwait. Med
Princ Pract 2003; 12: 252-255.
14. Tankhiwale SS, Agrawal G, Jalgaonkar SV. An
unusually high occurrence of Salmonella
enterica serotype Paratyphi A in patients
with enteric fever. Indian J Med Res 2003;
117: 10-12.
15. Chopra GS, Basu SK and Bhattacharya SR.
Present Phage types and Antibiotic
susceptibility of Salmonellae. Indian J Pathol
Microbiol 1992; 4 : 345-350.
16. Agarwal V, Brahmne RB, Dhanvijay AG,
Jalgaonkar PD, Pathak AA, and Saoji AM.
Antibiogram, phage types and biotypes of
Salmonella Typhi isolated in Nagpur. Indian J
Med Res 1992; 95: 14-16.
17. Kumar R, Aneja KR, Punia AK, Roy P, Sharma
M and Gupta R. Changing pattern of
biotypes, phage types and drug resistance of
Salmonella Typhi in Ludhiana during 1980-
1999. Indian J Med Res 2001; 113: 175-180.

17
Abstract
Introduction:
Malaria is a major cause for hospital admissions in the tropical regions, but there is no objective tool to predict the length of hospital stay (LOS). Analyzing 700 hospitalized patients, a simple equation was devised. LOS was equal to ½ [5+ 5 x Severe anemia + 1 x Jaundice +2 x acute renal failure+3 cerebral malaria + 1 x Type of therapy]; where, presence of the complication is 1 and absence=0 ; Type of therapy : oral anti malaria therapy=1, parenteral =2, and any ICU intervention (ventilator, dialysis etc)=3 . The Length of hospital stay of a malaria patient can be estimated easily and rapidly by a simple formula, which does not require sophist icated investigations. It can be calculated at the time of admission as well as during the course of the disease.
When a patient is admitted to a hospital the most important concern is the survival. The subsequent question which arises in the mind of the health care providers, patients or their relatives, as well as the administrators is the duration of hospital stay of the patient. In malaria prone areas, many of the hospital beds in the referral centres are occupied by patients with malaria. The cost of treatment depends on several factors, one of these being the period of stay. A simple scoring system was devised by Mishra et al to predict the
1 survival of the malaria patients. A large number of the beds are occupied by these patients, during the peak transmission period, making it a major administrative problem. The LOS of admitted patients is one of the indicators of bed occupancy, planning and rotation of staff deployment, etc and
2-4the resource utilization. (Kazembe et al. 2006;
Velip et al. 2006; Van Houdenhoven et al. 2007)
Similarly, from the point of view of the health care
providers and administrators, no tool is available to predict the length of stay for the malaria cases. When confronted by a questioning/ inquisitive relative, the treating doctor only extends a rough estimate depending on his own experience, which is purely subjective. In practical situation, the statements are variable for different doctors and thus totally confusing to the relatives.
In the present study, it is attempted to identify various determinants on LOS, and to develop a mathematical model which can be used objectively for each patient admitted to a hospital. We tried to make it simple and easy to remember. It is attempted that it must be calculated rapidly and must not require too many lab data.
a. Hospital: Ispat General Hospital is situated in Sundargarh district of Orissa. It is a 685 bed hospital under of a Public sector steel plant.
b. It has eleven bed Critical care units. There are facilities for haemodialysis, peritoneal dialysis, blood banking, 24 hour emergency, haematology and biochemical laboratory etc.
c. Catchment area: Patients come from urban areas of Rourkela as well as surrounding villages, forested areas, mining localities etc.
d. Subjects: All patients admitted to the Internal Medicine Dept of Ispat General Hospital, Rourkela with confirmed malaria.
The study has two parts: (a) analysis of the malaria and (b) Multiple regression analysis.
In the first phase, database was collected prospectively in a format which includes age, sex, demographic data, treatment received before admission, biochemical and hematological reports, presence of seizures, treatment details, and the outcome. All those who expired were
Material & Methods:
Predictions of Lengths of Hospital stay of malaria patients
Address for communication :
Dr SK Mishra
Director, Ispat General Hospital,
Rourkela -769005, INDIA
Email: [email protected]
Original Papers
Saroj K MishraDeptt. of Internal MedicineKishore C MahantaDeptt. of Internal MedicineRajalaxmi Mishra Deptt. of Mathematics,Sushilavati Govt. Womens College, Rourkela
Narayan P SahooDeptt. of Anaesthesia

18
Determinants
Entitled
Sex
Residence area
Acute renal failure
Cerebral malaria
Severe anemia
Jaundice
Complications
Level of treatment
Characteristics
EntitledNE
MaleFemales
RuralUrban
Sr Creatinine >3mg/dlSr Creatinine < 3mg/dl
GCS <10GCS >10
Hb<5.1 GHB>5 g/dl
Bil >3mg/dlBil < 3 mg/dl
UncomplicatedSingleMultiple
Oral drugsParenteral (QBH/AS)
No of patients
433267
512188
257443
29671
61639
18620
139561
390181129
115585
LOS (± SD)
3.99(±2.00)4.95(±2.95)
4.29 (±2.39)4.52(±2.61)
4.62(±2.75)3.91 (±1.73)
8.66 (±4.45) 4.17(±2.14)
7.41(±2.11)4.06(±2.08)
5.89(±2.65)4.37(±2.46)
5.81(±3.33)3.99(±2.03)
2.87(±1.68)4.33(±1.68)6.78(±3.53)
2.97(±21.18)4.62(±2.54)
P value
0.000*
0.299
0.000
0.000
0.000
0.027
0.000
0.000
0.000
Table 1. Characteristics of malaria patients and LOS
excluded from the study. 700 patients with complete data were analysed.
Student's t test was used to differentiate between male vs female; adult vs children; Rural vs urban; patients with acute renal failure (sr Creatinine >3 mg/dl), jaundice (sr Bilirubin > 3 mg/dl), severe anemia (Hb < 5 gm/dl) or cerebral malaria (unarousable coma or GCS <10).
The statistical analysis was done by using OpenEpi version 2.2.1 (2010), an Open Source Epidemiologic Statistics for Public Health, Version 2.2.1. www.OpenEpi.com, accessed on 18 June 2010 The difference is considered to be significant if p < 0.05.
In the second phase Multiple Regressions was performed to find out the relationship of the above parameters and to get a linear equation.
Statistics:
LOS was 8.66 (±4.45) days in presence of acute
renal failure, 7.41(±2.11) days in patients with
cerebral malaria, and 5.89 (±2.65) in presence of
severe anaemia and 5.81 (±3.33) in patients with
jaundice. LOS was longer in patients, who have
come from rural areas, but there was no
difference in males vs females.
After the determinants were identified, a linear
It will be in the form of
LOS = a x + a x + a x + a x + …… + C1 1 2 2 3 3 4 4
In the study we collected the data of those adult patients who survived and were discharged from the hospital. 700 surviving patients were analysed for the prediction of length of hospital stay. Out of these, 188 were females and rest were males.
Observations:
62% were entitled patients (either employees or their dependants, or retired employees of the steel plant: all of these get free medical treatment) and 38% were from different walks of life, including people from villages, township and traders. These patients were treated in the hospital on payment basis. Their income and socio economic conditions varied widely. 60% were from urban areas, and others were from suburbs or villages.
The comparisons of length of stay in different
groups are depicted in the Table-1. As it appears,
the length of stay was significantly longer in
patients with severe anemia, acute renal failure,
cerebral malaria and jaundice.
Thus LOS was 2.87(±1.68) days when the patient
was having uncomplicated malaria, which went
on increasing in presence of complications. Thus

19
patients are concerned regarding the length of stay in a tertiary care hospital and the cost associated with it. We searched the literature to find out the studies related to LOS in malaria patients. But there were only two studies cited in the MEDLINE by Kazembe et al. 2006 and Velip et
2,3 al. 2006. However, several studies have been carried out by Mounsey et al. 1995;. Bannwartet al., 1999; Arrahamyan et al. 2006; Clark et al., 2007 and Diringer et al., 2004 to predict the LOS in other clinical conditions viz, very low weight neonates in nursery, sepsis in ICU settings,
5-9patients after coronary surgery etc.
In a retrospective study in Spain, 1920 episodes of community-acquired pneumonia (CAP) in 27 community hospitals were analyzed by Cabre et
10al. (2007) for inter-hospital variability in length of
hospital stay (LOS), mortality and readmission rates. The overall adjusted LOS (mean+/-S.D.) was
10.0+/-9.8 days. LOS increased according to the Pneumonia Severity Index (PSI) risk class: 7.3 days for class I to 11.3 days for class V (P<0.001).
2Velip et al. (2006) from Goa described the determinants of LOS in malaria patients. The study indicated the importance of altered sensorium, presence of liver involvement, duration of therapy
equation was developed by using multiple regressions.
LOS = 2.441+ 2.565 Severe anemia + 0.447 Jaundice +0.993 acute renal failure
1.405 cerebral malaria +0.657 Level of therapy
The equation was made modified to make it simple and ready to use at bedside.
Thus,
LOS = 2.5+ 2.5 Severe anemia + 0.5 Jaundice +1 acute renal failure
1.5 cerebral malaria + 0.5 Type of therapy
Where, the severe anemia, jaundice, acute renal failure, cerebral malaria are considered as present=1, or absent=0; and level of treatment is oral anti- malaria treatment with chloroquin or quinine =1, parenteral artemisinine or quinine =2,
and any ICU intervention (ventilator, dialysis etc)=3.
Malaria being a disease mostly in the developing countries, the treatment is availed at different levels: (a) at home, (b) at the nearby health facilities and (c) referral centre for severe malaria cases; where the patient is shifted to a hospital far away from own place of residence. Relatives of
Discussion
Factors
Entitled or not
Residence
Severe anemia
Cerebral malaria
Jaundice
Acute renal failure
Level of therapy
Beta
0.186
0.106
2.565
1.405
0.447
0.993
0.657
P value
0.323
0.428
0.000
0.000
0.028
0.006
0.000
LOS= 2.441+ 2.565 Severe anemia + 0.447 Jaundice +0.993 acute renal failure
1.405 cerebral malaria +0.657 Level of therapy
simplifying the equation for ready bedside use
LOS = 2.5+ 2.5 Severe anemia + 0.5 Jaundice +1 acute renal failure
+ 1.5 cerebral malaria + 0.5 Level of therapy
or,
LOS = ½ [5+ 5 x Severe anemia + 1 x Jaundice +2 x acute renal failure
+3 x cerebral malaria + 1 x Level of therapy]
Where, presence =1 , and absence = 0 for severe anemia, jaundice, acute renal failure and cerebral malaria.
For level of therapy oral chloroquin or quinine =1, parenteral artemisinine or quinine =2, and any ICU intervention (ventilator, dialysis etc)=3
Table-2.: Multiple regression showing influence of factors on LOS

20
before admission as influencing factors. But a major flaw of the study was that most of the patients were uncomplicated ones. PUBMED search did not show studies on determination of LOS in severe malaria cases. Similarly publications are not available from any tertiary care hospital which manages both uncomplicated and complicated cases.
Some of the parameters in our study were similar to the Goa study. However, we have not been able to find any difference among the males and females, urban vs rural on LOS. But, as expected the LOS is higher in patients with any or more complications. It was noted that all complications are not similar, and they influence the survival in a different weighted capacity. Similarly they also influence the LOS.
When a very sick malaria patient is managed in critical care unit or high dependency unit, survival is the most important concern. In a previous study, Mishra et al. (2007) proposed a simple prediction rule for the survival of the patients with severe malaria by assigning 1,2,3 and 4 to A (anemia), B
(BUN↑ ), C (cerebral malaria) and D (Dyspnoea/ ARDS) respectively. The malaria score for adults (MSA) ranges from 0 to 10. The mortality was 2% for MSA 0 – 2; 10% for MSA 3–4, 40% for MSA 5–6 and 90% for MSA 7 or more. The sensitivity is 89.9% and positive predictive value is 94.1% when 5 is taken as the cut off value.
In the present one, we derived a very simple prediction rule for the LOS. It does not involve sophisticated data collection, estimation or analysis. Still it extends valuable information, which will be helpful to the clinicians. In addition, the formula can be used to modify the result/ prediction in the course of time if any new complication arises.
However, we have analyzed the data of only one year, and that too only among the adults. It is proposed that such studies may be undertaken among children too. It should also be validated in cohorts from different geographical regions.
Acknowledgement: We extend sincere thanks to the staff of IGH and malaria research Unit.
Funding: None, Conflict of interest: None
References:
1. Mishra SK, Panigrahi P, Mishra R, Mohanty S. Prediction of outcome in adults with severe falciparum malaria- a new scoring
system. Malaria Journal, 2007; 6:24. doi: 10.1186/ 1475-1875-6-24.
2. Velip AP, Kulkarni MS, Motghare DD, Vaz FS. Determinants of hospital stay among malaria patients at a tertiary care hospital in Goa. J Communic Dis, 2006; 38: 115-117
3. Kazembe LN, Kleinschmidt I, Sharp BL. Patterns of malaria-related hospital admissions and mortality among Malawian children: an example of spatial modelling of hospital register data Malaria Journal 2006, 5:93 doi:10.1186/1475-2875-5-93
4. Van Houdenhoven M, Nguyen TD, Eijkemans MJ, Steyerberg EW, Tilanus HW, Gommers D, Wullink G, Bakker J, Kazemier G.Optimizing intensive care capacity using individual length-of-stay prediction models. Crit Care. 2007 27; 11 :R42
5. Mounsey JP, Griffith MJ, Heaviside DW, Brown AH, Reid DS. Determinants of LOS in ICU and in hospital after coronary artery surgery. Br Heart J, 1995; 73: 92-98.
6. Arrahamyan L, Demirchyan A, Thomson ME, Hovaguimian H. Determinants of morbidity and ICU stay after coronary surgery. Asian Cardiovasc Thorac Ann, 2006; 14: 114-118.
7. Bannwart BC, Rebello cerebral malaria, Sadeck LSR, Pontes MD, Ramos JLA, Leone C. Prediction of Length of Hospital Stay in Neonatal Units for Very Low Birth Weight Infants. J Perinatology, 1999; 19: 92-96
8. Clark DE, Lucas FL, Ryan LM. Predicting hospital mortality, length of stay, and transfer to long-term care for injured patients. J Trauma, 2007 ;62:592-600.
9. Diringer MN, Reaven NL, Funk SE, Uman GC. Elevated body temperature independently contributes to increased length of stay in neurologic intensive care unit patients. Crit Care Med. 2004 ;32 :1489-95.
10. Cabre M, Bolivar I, Pera G, Pallares R; Pneumonia Study Collaborative Group. Factors influencing length of hospital stay in community-acquired pneumonia: a study in 27 community hospitals. Epidemiol Infect. 2004 Oct;132(5):821-9.Velip AP, Kulkarni MS, Motghare DD, Vaz FS. Determinants of hospital stay among malaria patients at a tertiary care hospital in Goa. J Communic Dis, 2006; 38: 115-117

21
Peutz- Jeghers Syndrome presenting as acute intestinal
obstruction due to Jejunal Intussusception in an adult maleAmulya M Acharya
Sishir R Dash
Manoja K Panigrahi
Deptt. of Surgery
Address for communication :Dr A.M.Acharya, Sr Deputy Director,
Deptt. of Surgery, Ispat General Hospital, Rourkela, Odisha, India
Email:[email protected]
ABSTRACT
Key words:
Introduction:
Peutz – Jeghers syndrome (PJS) is a rare familial
a u t o s o m a l d o m i n a n t d i s o r d e r w i t h
hamartomatous polyposis of G I Tract and melanin
pigmentation around mouth, oral mucosa , lips
and digits. Most common symptoms are
recurrent pain abdomen, anaemia and blood in
stool. Presentation of frank intussusception and
intestinal obstruction in adults is uncommon. We
are reporting a case of Indian adult male
presented to us in acute intestinal obstruction due
to jejuno jejunal intussusception. There were
multiple polyps in the small gut and one large
polyp of 4cm x 8cm was the lead point in triggering
the intussusception. Histopathology confirmed
them as hamartomatous polyps typically seen in
Peutz- Jeghers syndrome. As it is unusual to see
such rare case in clinical practice and scarcity of
literature, we feel to report this for the benefit of
clinicians and students. Awareness of the disease
is helpful for proper diagnosis, early management
and follow up with genetic counseling to the
patient and his family.
Peutz, Jeghers,PJS, polyposis, intestinal polyps,
melanin pigmentation, intussusception
Adult intussusception is rare and do not present
the symptoms of red currant jelly stool that is seen 1 in children. Very rarely multiple intestinal polyps
seen in the familial disorder Peutz- Jeghers
syndrome (PJS) with the typical muco- cutaneous
pigmentation around mouth, oral mucosa lips
and digits. The most common symptoms are
recurrent pain abdomen, anemia, malena and
hematochezia. Here we are reporting a case of PJS
presented as acute intestinal obstruction due to
jejunal intussusception in an Indian adult male.
We are providing some clinical photographs,
histopathology report and added discussion
available from the scarce literature which may be
of educational importance.
A 58 years old Indian male was admitted in the
surgical ward with sudden onset of severe
abdominal pain associated with vomiting of three
days duration. He was found afebrile, anemic and
dehydrated. Pulse 98/min, BP 100 / 70 mm Hg.
Abdomen was distended with diffuse tenderness
and guarding. An ill defined soft immobile mass
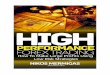
(15 x 8 cm) was palpable in the epigastrium. Some
bluish black pigmentation was seen over his
buccal mucosa but could not be correlated with
the acute abdominal condition (Fig.1).
Case report:
Figure 1: Bluish-black pigmentation over buccal mucosa.
Case reports

22
One large polyp of 3.5cm with a 8cm stalk was
found on per rectal examination (Fig.2).
Biochem reports were normal except low protein
(total protein 4g and albumin 1.9g). X-Ray
abdomen showed few air-fluid levels. Ultrasound
of abdomen revealed two concentric echo
structures with classical target sign suggestive of
intussusception (Fig.3a, 3b). Emergency
laparotomy was taken up with a provisional
diagnosis of acute intestinal obstruction.
Laparotomy revealed jejuno-jejunal intussuscep-
tion about one foot distal to duodeno-jejunal
flexture involving two feet long segment of
jejunum. Multiple polyps were seen on the
involved jejunum. There was one large polypoidal
mass of 4cmx8cm which was the lead point in
triggering the intussusceptions (Fig.4a,b).
About two feet of jejunum involving the
intussusception and having multiple polyps was
excised and end to end anastomosis done
followed by rectal polypectomy. Rest of the small
and large gut was thoroughly palpated and found
to be normal. Patient recovered uneventfully.
Histopa-thology of resected jejunum with polyps
showed branching of smooth muscles arising from
muscularis mucosae into the stroma of columnar
and goblet cells which are typical hamartomatous
changes seen in Peutz- Jeghers syndrome (Fig.5).
There was no evidence of atypia or malignancy.
Lymph nodes showed reactive hyperplasia.The case was finally diagnosed as Peutz-
Jeghers syndrome with unusual presentation of
acute intestinal obstruction duo to adult
intussusception.
Figure 2Rectal polyp 3.5cm with 8cm long stalk
Figure 3a US abomen showing target sign of intussusception.
Figure 3b Intussuscipien inside intussusceptum.
Figure 4a Multiple polyps in jejunum.

23
Follow up investigations were carried out. His
upper GI endoscopy and colonoscopy did not
reveal any polyp. Ba-meal follow through was
normal. We could not do the genetic study due to
lack of facilities.
The patient and his family members are now in
regular follow up.
Peutz- Jeghers syndrome (PJS) is a familial disorder
with two distinct features, (a) multiple
hamartomatous polyps of GI tract and (b) melanin
pigmentation around mouth, oral mucosa and
digits. The syndrome first described by Jan Peutz
in 1921 and later published in detail by Harold 2
Jegher in 1949 . First case was reported by 3 A.K.Basu in 1952. The disease is an autosomal
Discussion:
dominant disorder occurs due to subtle loss of 4 chromosome 19p 13.3 due to defect in serine/
threonine kinase gene (STK11/LKB 1). Sporadic
PJS can rarely occur.
The incidence of PJS is one in 60,000 – 3,00,000
population and not specific to any sex or race. The
polyps in PJS most commonly found in jejunum,
ileum; but can occur in any part of GI tract. The
melanin spots found small flat, brown or dark blue
and commonly found around the mouth, lips, and
buccal mucosa. The pigmented spots may fade
after puberty.
Different associated anomalies have been 5reported in PJS. Dormandy et al reported polyps
in bladder, renal pelvis, bronchus and nose . Rarely
polyps in ureter, gallbladder and CBD may occur.
Even ovarian cyst adenoma and Sertoli tumor of
testes are reported.
Small intestine obstruction and intussusception
occurs in 43% cases of Peutz-Jeghers syndrome
but usually seen in children. In our case an adult
male presented with frank jejuno-jejunal
intussusception and intestinal obstruction due to
an unusual large polyp of 4x8 cm. Very few such 6,7 cases have been reported from India. Malignant
potential of GI tract is very high in these patients,
as reported by various investigators. Giardiello8
et al found 93% cumulative risk of developing
cancer (15.2 fold relative risk, RR) by the age
64years The relative risks (RR) for cancer formation in PJS in relation to general population
are: Small intestine (RR 520), stomach (RR 96),
pancreas (RR 132), colon (RR 84), oesophagus (RR
57), ovary (RR 27), lungs (RR 17), uterus (RR 16)
and breast (RR15).
Giardiello and Trimbath published a review of PJS
and recommended the following management 9.and follow up
• Polypectomy of isolated polyps > 1cm in
stomach, colon
Morbidity and Mortality:
Management:
Figure 5 Branching of smooth muscle into the stroma of the epithelium.
Figure 4b large polypoidal mass which had triggered the intussusception.

24
Resection of intestine segment having
confluence of polyps
• Resection anastomosis for intussusception
• Intra operative push enteroscopy and
polypectomy of >1cm polyps.
1. Annual physical exam. of breast, abdomen,
pelvis( ovary), testes
2. US for pancreas, ovaries, testes annually
3. Mammography / MRI, Pap smear every year
4. Annual complete blood cell count
5. Ba-meal follow through every 2 year
6. EGD & colonoscopy every 2 year
7. Genetic counseling and screening from birth
of all first-degree relatives.
PJS is a rare familial disease involving multiple
polyps of GIT and mucocutaneous pigmentation
around mouth, lips, oral mucosa and digits.
Common C/F are recurrent pain abdomen,
anemia, GI bleeding. Acute Intestinal Obstruction,
Intussusception are common complications.
Development of cancer is relatively high. Early
diagnosis and proper M/M can reduce
complications. Genetic counseling & screening of
family members should be done as there is high
risk of development of cancer.
REFERENCES :
1. Agha FP, Intussusception in adult. Am J
Roentgenol 1986 March;143(3): 527-31
•
9Recommended follow up:
CONCLUSION:
2. Jeghers H, McKusick VA et al. Generalised
intestinal polyposis and melanin spot s of
oral mucosa, lips and digits. N Eng J Med
1949; 241: 993-1005, 1031-6.
3. Basu, A. K.: Familial intestinal polyposis with
pigmentat ion of sk in and mucous
membrane. Lancet 1952, 2: 586-587.
4. Hemminki A, Tomlinson I, Markie D, et al
Localization of susceptibility locus for Peutz-
Jeghers syndrome to 19p using comparative
genomic hybridization and targeted linkage
analysis . Nat Genet 1997; 15: 87-90
5. Dormandy TL, Gastrointestinal polyposis
with mucocutaneous pigmentation ( Peutz-
Jeghers syndrome) N Engl J Med 1957; 256:
1141-6
6. Saxena PK, Arora RK, Mehta, Singh HH.
Peutz-Jeghers syndrome with unusual
features (a case report). J Postgrad Med
1986 ;32:236-8
7. Thakker HH,Joshi A,Despande A, Peutz
Jeghers syndrome presenting as jejuno ileal
intussusception in an adult male: A case
report. Cases J,2009 Aug 2:8865
8. Giardiello FM, Brensinger JD, Tersmette AC ,
Vary high risk of cancer in familial Peutz-
Jeghers syndrome. Gastroenterology , Dec
2000;119(6): 1447-53.
9. Giardiello FM, Trimbath JD, Peutz- Jeghers
syndrome and management recommen-
dations. Cin Gastroenterol Hepatol,2006; 4:
408-15.
10. Clava D,Howe JR. Hamartomatous polyposis
syndrome. Sur Clin North Am 2008 Aug;
88(40) : 779-817

25
Pitabas Mishra Deptt. of Paediatrics
Address for communication :Dr. R. Satpathy, Sr. Consultant,
UNMC NICHD Research Network Email: [email protected]
Radhanath Satpathy UNMC NICHD Research Network
Nimain C Nanda Deptt. of Paediatrics
Rajan K BeheraDeptt. of Surgery
Pinaki PanigrahiProfessor and Director, Center for Global Health and DevelopmentCollege of Public Health , University of Nebraska Medical Center, USA
Abstract:
Keyword:
Introduction:
Necrotising Fasciitis (NF) is relatively a rare disease
found in adults. When occur in neonates, its
outcome is usually fatal. Two rare cases of
Necrotizing fasciitis (NF) have been reported with
possible rare association of trisomy.
Necrotising Fasciitis, Neonate
Necrotising fasciitis (NF), otherwise known as the
Flesh Eating Disease, is a term that describes a
disease condition of rapidly spreading infection
usually located in fascial plane of connective tissue 1that results in tissue necrosis . Although the
condition was described earlier, Dr B Wilson 2termed the condition in 1952 . The disease occurs
infrequently and almost can occur in any part of
the body. The spread of infection can be so fast
that it is difficult to stop it with both antimicrobial
drugs and surgery. It is predominantly an adult
disorder. When it occurs in children the course is
usually fatal. Less than a 100 Neonatal NF cases
have been reported in literature. The purpose of
this communication is to report two rare cases of
neonatal NF with fatality.
Case-1 (Figure1) Baby of SA was admitted to
hospital with a big area of ulceration on the back
of 3 days duration. The baby was delivered
normally in hospital and was weighing 2.8 kg. Early
neonatal period was uneventful. It was all along
breastfed. On Day-15, baby had fever and was
crying inconsolably. Next morning, mother
noticed an area of redness on the back that rapidly
spread all over the lower half of the back with
ulceration. On examination, baby was febrile,
irritable, sucking from mother, pink with features
of trisomy and had no other focal sign of infection
than an ulcerated area of 6x4 cm, seen being
surrounded by deep brown dead tissue on the
back. The floor of the ulcer was showing muscles
of the back and oozing of pus. Margin was much
irregular and was looking like punched out ulcer. It
was treated with combination antibiotics, daily
dressing of wound and wound debridement as
and when necessary. Total count was
6400/cm,Hb-14.5/dl, and blood group was B+ve.
Blood culture and wound swab culture did not
reveal any organism. Though, baby improved with
therapy, parents took discharge against medical
advice on D10 and the baby expired at home
after 3 days.
Case-2 (Figure2) Baby of BS, was admitted to
hospital on Day 11 with complaints of unable to
take feed properly, ulceration of mouth of 2 days
duration and a swelling on the back with bluish-
Necrotising Fasciitis In Neonates – Case Report
Case Reports

26
Figure 1 Showing lesion on back
red discoloration and painful to touch of one day
duration. He was born in hospital to a multi-para
mother by normal vaginal delivery and cried soon
after birth. There was premature rupture of
membrane for a week. There was no maternal
fever or any other sickness. Soon after birth, baby
was fed breast milk and had some oral ulceration. 0 On examination baby was febrile (temp 102 F),
lethargic, pale and weighing 2.8kg. Heart rate was
140 and respiration rate was 44/minute. There
was jaundice but no cyanosis. All peripheral
pulsations were felt and capillary refill time was
less than 4 seconds. Ears and anterior fontanel
were normal. Oral thrush was there. A big bluish
red discolored area was on the back measuring
nearly 3''X4” size without any ulceration or oozing
(Fig-2). It had an area of central fluctuation. A
many vesico-pustular lesions were detected on
the peri-umbilical area and back on gluteal region.
Cardiovascular and respiratory systems and
abdominal examination were normal. Neonatal
reflexes were poorly elicitated. Necessary
investigations were done and pulse oxymetry
showed 95 to 99% saturation.
The baby was put on combination antibiotics
(Cefrtriaxone and amikacin) and managed in
pediatric ward. Surgeons saw the baby and
aspirated sero-sangunous fluid on D-2. Baby
continued to be febrile, sick and had abdominal
distention. Wound sloughed out and a raw area
developed by D-4. Vital signs were unstable and
baby was put on IV fluid and pressure amines. By
D-5 there was edema, fever, respiratory distress,
refusal to feed and abdominal distension.
Vancomycin was added to the regimen and
continued for 2weeks. The skins including the
deep tissue were shredded (Fig-2) and wound
debridment was done, the area affected was daily
cleaned and dressed, dead tissues were removed.
Anemia, edema and fever continued for long time
and the baby was somewhat better by 3 weeks
hospital stay.
During the course of stay, the baby continued to
have fever all the time and sick. There was edema
of limbs, abdominal distension and conjugated
hyperbilirubinemia. As the baby developed
anemia and low general condition, it received two
units of blood transfusion. Both medical and
surgical management and crisis management n d
continued for 22 days. On 22 day of
hospitalization, baby had cardiac arrest and could
not be revived.
Necrotising fasciitis is a rare condition in neonates.
Terms like necrotising fasciitis, myonecrosis, and
necrotising adipositis refer to classification by depth of infection. Type 1(polymicrobial) and type
2 (monomicrobial) infections refer to classification based on microbial cause. Historically, necrotizing
infections were classified according to anatomical sites. Fournier gangrene (involving the perineum)
and Ludwig's angina (involving sub-mandibular and sublingual spaces) are examples. These
infections were named after the physicians who
1first described those . NF is frequently
attributable to secondary infections. They are like
omphalitis, mammitis, balanitis, postoperative
complications, and bullous impetigo, and may be
Discussion
Figure 2 Early changes on the back

27
associated with diabetes mellitus, necrotising 3enterocolitis, immunodeficiency, malnutrition
and septicemia. Both the babies were neonates
and were diagnosed in hospital at the interval of
five years, proving the rarity of the condition. If it is
not suspected, the diagnosis is missed. The most
common site of involvement in pediatric patients
is the abdominal wall followed by the thorax, back, 4
extremities with head and neck as unusual sites .
In our case, classically neonates had the back
involvement.
The initial skin presentation ranges from a minimal
rash to erythema, oedema, induration or cellulitis.
These lesions spread rapidly. The overlying skin
may later develop a violaceous discolouration,
peau d'orange appearance, bullae, or necrosis.
Our second case (Fig-2) had the classical
presentation and was detected and treated from ndthe 2 day of occurrence. Continued fever and
tachycardia was seen in both the cases. Marked
tissue oedema, rapid progression of inflammation
and signs of systemic toxicity were seen in the
second case. Death occurred before surgery or
shortly after surgical intervention as a result of
bacter ia l infect ion with sept ic shock,
disseminated intravascular coagulation and/or
multiple organ failure. Our second case died due
to multi-organ failure. Empirical antibiotics to
cover (Cephalosporin and aminoglycoside) gram
positive and negative organism were used, to start
with. Subsequently vancomycin has been used in
second case. We had two different cases, one
presented while skin shredding has occurred (Fig-1)
and the other at the onset of the disease (Fig-2).
Case one, with medico-surgical management had
stable vital signs but died at home on discharge
against medical advice, whereas case two had all
complications of neonatal sepsis and did not
survive after a long duration of hospital stay, thus
showing the fatality.
Early diagnosis and aggressive surgical treatment
reduces risk; however, it is often difficult and
patients are treated for simple cellulitis until they
rapidly deteriorate. Prompt diagnosis with 5
aggressive therapy improves survival . Antibiotic
therapy is mandatory and early surgical
exploration and debridement is critical to ensure a
good outcome. Microbiologically, until blood
culture results are available, wide spectrum
coverage with intravenous antibiotics is started.
These antibiotics should cover S pyogenes, S
aureus, and Gram-negative aerobes and
anaerobes as clinically indicated. Group A Beta
hemolytic streptococci (GABHS) has been
reported widely as a single pathogen. Appropriate
therapy includes IV Penicillin150 000u/kg/day in 4
divided doses, Clindamycin 40mg/kg/day in 4
divided doses and Vancomycin40mg/kg/day in 3-64 divided doses .
References:
1. Medicine Net.com- assessed on 26.10.2010
2. Hsieh WS, Yang PH, Chao HC, Lai JY. Neonatal
necrotizing fasciitis: a report of three cases and
review of the literature. Pediatrics 1999;
103:e53.
3. Antonio FM, Pedro GC; C DM, Carola DM; Luz
Orozco-C, Tamayo-S; Ramon RM Necrotizing
Fasciitis, Report of 39 Pediatric Cases, Arch
Dermatol. 2002; 138: 893-899.
4. Kothari PR and Kulkarni B, Neonatal
Necrotizing Fascitis, Indian Pediatrics: 2004,
41:1070-71
5. Moss RL, Musemeche CA, Kosloske A M.
Necrotising fasciitis in children: prompt
recognition and aggressive therapy improve
survival. J Pediatr Surg 1996 ; 31:1142–6.
6. Textbook of Pediatric Infectious Diseases, 6th
Edition, Saunders, Philadelphia 2009; pg79-791

28
Case Reports
Abstract :
Keywords:
Introduction:
Xeroderma pigmentosum with squamous cell
carcinoma and basal cell carcinoma is rarely
reported. A 22 years female having Xeroderma
Pigmentosum presented with ulcerated and
blacklish pigmented lesion on Sun exposed area of
body. Histopathological examination of the three
different skin biopsy showed squamous cell
carcinoma, basal cell carcinoma & initial phase of
Xeroderma pigmentosum. Case is being
presented because of the rare association of these
tumors with Xeroderma pigmentosum in Indian
scenario. It is also observed for the first time in
IGH, Rourkela.
Xeroderma pigmentosum, squamous cell
carcinoma, basal cell carcinoma
Xeroderma Pigmentosum (XP) is a rare genetically
heterogenous autosomal recessive disorder
resulting from the defect in DNA repair
mechanism i.e. Nucleotide Excision Repair (NER).
It is characterized by photosensitivity, pigmentary
changes, premature skin ageing and various
cutaneous and internal malignancies at an early
age. XP was first described by Herba and Kaposi in 1
1874. It occurs with an estimated frequency of
1:250,000 in US and somehow more common in
2Japan i.e. 1: 40,000 but in Indian scenario its
frequency is not yet calculated because of its
rarity. To our knowledge, dual malignancy i.e.
Squamous Cell Carcinoma (SCC) and Basal Cell
Carcinoma (BCC) associated with XP is rarely
reported in India.
Here we report a case of XP with different stages
of skin manifestations.
22 year female presented with various pigmented
lesion on face and hand (Fig1). Pigmented lesion
on face was since childhood. On examination she
had an ulcerated lesion over forehead with rolled
CASE REPORT:
Squamous cell carcinoma & basal cell carcinoma with
xeroderma pigmentosa – a rare presentation
Aruna M Deptt. of Pathology
Minz Niranjan K of Dermatology
BeheraDeptt.
Rabi R of Pathology
Panda Deptt.
Sanghamitra of Pathology
SatpathiDeptt.
Prativa K of Pathology
BeheraDeptt.
Usha of Microbiology
DasDeptt.
Address for communication : Dr. Aruna Mukti Minz, Specialist,
Department of Pathology,
Ispat General Hospital, Rourkela
e-amil : [email protected]
Fig1. Pigmented lesions on face

29
out border clinically diagnosed as BCC,
hypertrophied lesion on cheek clinically
diagnosed as actinic keratosis and scarring lesion
on right hand clinically suggestive of SCC. She also
had photophobia .The lesions were progressive
and getting aggravated after sun exposure. Family
history was not significant. Systemic examination
was unremarkable and intelligence was normal.
Skin biopsies were taken from the face and hand
lesions. Histopathological examination showed
three different lesions. Biopsy from cheek showed
features suggestive of first stage of skin changes of
XP i.e. hyperkeratosis, thinning of stratum
malpighi with hyper-pigmentation (F-2), biopsy
from forehead showed features of BCC (F-3) and
biopsy from hand showed features of well 4differentiated SCC. (F-4).
Xeroderma Pigmentosum is a rare inherited
disease. The incidence is approximately 1:250,000
in US and somehow more common in Japan i.e. 2 1:40,000. The defect is autosomal recessive
genetic defect in which NER enzymes are mutated
leading to reduction in or elimination of NER.
There are seven groups of XP i.e. XPA to XPH and
one more type which is XP variant. Out of these 3 XPA is common and XPE is rare. XP patients are at
a high risk for developing skin cancers at an early
age as compared to normal individual and these
cancers are commonly BCC, SCC & malignant
melonoma. In our case, the patient had both BCC
and SCC. The disease typically passes through
three stages. The first stage appears after the age
of six months characterized by different
erythema, scaling and freckle like area of
increased pigmentation on the sun exposed areas.
The second stage is characterized by skin atrophy,
telangiectasis and mottled hyper-pigmentation.
The third stage is presented by numerous
malignancies including SCC, BCC, malignant
melanoma and fibrosarcoma. These cancers may
present as early as 4-5 years of age. As our case
had two varieties of malignancies i.e. SCC and BCC,
she progressed to the third stage of the disease.
Occular problem occurs in 80% cases includes
photophobia, conjunct iv i t is , ectropion
symblephoron with ulceration and malignancies.
Our patient had Photophobia.
Discussion:
Fig 3. Basal Cell Carcinoma (H&E)
stFig2. 1 Stage of Skin Changes of XP
Fig 4. Squamous Cell Carcinoma (H&E)

30
References:
1. Hebra F, Kapsosi M. On diseases of the Skin
including the exanthemata. Vol.3 ( translated by
W.Tay) London: The new Syderham Society
1874;252-8.
2. Robbins JH, Kraemer KH, Lulzner MA, Festoff
BW, Coon HG. Xeroderma Pigmentosum, an
inherited disease with Sun sensitivity, multiple
Cutaneous neoplsia and abnormal DNA repair.
Ann intern Med 1974; 80:221-48.
3. J.I.Harper, R.C.Trembath . Genetics and
Genodermatosis in : Rooks Text book of th
Dermatology.7 Edn. Blackwell 2004; 12.56-
12.61.
4. Lever WF , Schaumberg-Lever G. Congenital
Diseases. In: Lever WF, Schawmberg-Lever G. eds. th
Histopathology of Skin. 9 Edn. Philadelphia: JB
Lippincott 2005; 147-148.
Neurological problems are seen in nearly 20% of
cases which includes microcephaly & Mental
Retardation (MR). De Sanctis cacchione syndrome
refers to the combination of XP & MR and 3cerebellar ataxia, hypogonadism and dwarfism.
In our case, she had absolutely normal
intelligence. Prenatal diagnosis can be made by
amniocentesis.
Xeroderma pigmentosum is a progressive disease
and patient dies due to complications of various
malignancies. So the management of XP patient
needs protection from sunlight by every possible
means. Early and adequate excision &
radiotherapy of all tumors are preferred. Our case
was referred to higher centre for Radiotherapy.
The relatives of known cases must be screened to
detect any genetic defect at early possible stage.
Editorial Declaration
Copy right of the manuscripts, letters and photographs published in the
'Proceedings of Ispat General Hospital' is vested with the contributors of
the material. "Authors and contributors are free to publish or present
their research work anywhere else only under intimation to the editors of
this publication.

31
Case reports
Abstract :
Keywords:
Introduction:
Case History:
Brain metastases from papillary thyroid
carcinoma (PTC) are extremely rare with a
frequency of only 0.1 to5 percent. Mostly they are
first detected during the course of treatment of
PTC. With the publication of case reports of brain
metastases from clinically silent PTC and
importance of tissue diagnosis to treat this
condition, as it may need radio iodine therapy,
intense thyroid work-up may be needed, in brain
metastases, with unknown primary.
metastases brain, papillary carcinoma thyroid,
silent, occult, unknown primary.
Papillary thyroid carcinoma rarely spreads to 1brain. We, here, report a case of extensive brain
metastases with undetectable primary and
clinically normal thyroid gland. Due to recent
publications, detail thyroid work-up with different
imaging modalities in conjunction with fine
needle aspiration cytology led to suspicion of PTC.
It was corroborated by the tissue diagnosis of
brain lesion. Incidentally, more than 20 countable
metastatic lesions in the brain, is being reported
for the first time.
A 52 years married lady presented at
Neurosurgery department of our hospital with
complaints of weakness of left upper limb for two
months and headache off and on for the same
period. She further revealed that she was having
tingling sensation on her left side limbs at times.
Her higher functions were normal. She was having
gross papilledema on both sides but rest of her
cranial nerves were normal. Her power around
the left shoulder joint, elbow was grade 3/5, at the
wrist and grip of same side was grade 2/5.There
was spasticity in left upper limb but no additional
movements. No sensory deficit could be detected
in her body including her left upper limb, though
she was complaining of tingling sensation. Deep
tendon reflexes were normal all over except in left
upper limb, where they were exaggerated. Her
cortical and cerebellar functions as well as gait
were normal. All other systems, including the
thyroid gland, were normal on clinical
examination. Her hemogram, biochemical reports
and ski gram of cervical spine were within normal
limit. Her computerized tomogram (CT) of the
brain showed multiple ring enhancing lesions
distributed in both the hemispheres and
cerebellum (Figure1). Magnetic Resonance (MR)
imaging and spectroscopy suggested secondary
deposits in brain. With the provisional diagnosis
of multiple metastases of brain, attempt was
made to find out the primary lesion.
Accordingly, she was again examined thoroughly
and investigated with ski gram and CT scan of
Address for communication :Dr.R.N.Mohapatra,
Neurosurgery Department,
Rourkela-769005, India.
e-mail: [email protected]
Multiple brain metastases due to occult Papillary Carcinoma of
thyroid gland: A Case Report
Rabindra N Mohapatra Deptt. of Neurosurgery
Sudhiranjan Pradhan Deptt. of Radiology
Saropani HembramDeptt. Neurosurgery of
Rabiratna PandaDeptt. of pathology
Pushpa Kumari, Deptt. of Ophthalmology

32
chest, ultrasonic examination of abdomen and
pelvis, all of which were unrevealing. Her
mammary glands were normal. On suspicion, she
was advised ultrasonic examination of thyroid,
though the gland was clinically normal. It revealed
one solid nodule of size 6 millimeter (mm) in
diameter on right lobe and the other one on left
side, which was cystic and of same size.
Ultrasound guided fine needle aspiration cytology
(FNAC) was done from both the lesions. FNAC
from the solid nodule was suspicious of papillary
carcinoma.
Thyroid scanning with radio iodine revealed a cold
nodule on right lobe but a normal brain. To clinch
the diagnosis, craniotomy and excision of 2 lesions
from right frontal lobe was done. The excised
specimen was sent for histopathology study,
which revealed predominantly papillary
architecture with evidence of malignancy (Fig2).
The lady was referred to a premier oncology
center for consideration of radiotherapy (RT).
While she was undergoing radiation therapy her
general condition deteriorated and she withdrew
her consent, for thyroidectomy and radio iodide
therapy, (after receiving 30 Gy RT over 10 sittings).
She had undergone Tco4-thyroid scan, which
revealed photon deficient area in both the lower
poles of thyroid, diffuse increased tracer
concentration in both hemispheres of brain.
These were highly suggestive of PTC with
metastatic deposit in brain. At the end of 3
months, the lady is having good cognitive
function, weakness of left half of body improv ed,
needs support to walk and to carry out her day to
day activities. She is on steroid and prophylactic
anticonvulsant only.
Discussion : PTC is the most common thyroid 1, 2, 3
neoplasm. Distant metastases occur in only 5
to 14% cases. The most common sites for distant
metastasis of PTC are the lungs, followed by the
bone. Brain metastasis from PTC is extremely 1, 2, 3, 4, 5
rare. Total 23 cases are reported in literature.1 CT scan, MRI and MR spectroscopy all may help
to diagnose metastases in brain, but they cannot
help to identify the primary lesion. As PTC is not
known to cause metastases to brain, frequently
detail work-up of thyroid gland is neglected, when
it is clinically silent. Ultrasonic examination of the
thyroid gland followed by FNAC may help to clinch
the pathology, as in our case. Radio Iodine uptake
is very rare in brain metastases from PTC, probably
due to the poor penetration of blood brain barrier 6by the radio isotope. Tco-4 thyroid scanning may
support the diagnosis.
Surgery, radiotherapy, and radioactive iodine
therapy are the available modalities for treatment
of PTC with brain metastases, along with total 1,7
thyroidectomy. But these modalities are
dependent on tissue diagnosis. If primary disease
can be detected initially, it may be possible to
avoid craniotomy and treat the primary disease
early.
Figure1. Contrast enhanced CT scan of brain shows multiple enhancing ring lesions in brain with
surrounding oedema.
Figure2. Histopathology of the brain lesion in low power magnification shows prominent
papillary architecture

33
Median survival of thyroid malignancy, once brain
metastases have occurred varies between 4.7 to 7, 89.4 months.
Metastases from papillary carcinoma of thyroid,
though rare, are being reported by different
authors. When brain metastases are detected
from unknown primary, thyroid gland should be
investigated in detail for the primary lesion
because treatment modalities may be different in
this type of disease. We found ultrasonic
examination followed by fine needle aspiration
cytology to be fruitful procedure in this regard.
References:
1. Saleh FA, Abdullah SA, Wafa AS .Abdullah ST.
Cerebellar mass as a primary presentation of
papillary thyroid carcinoma: case report and
literature review. Head & Neck Oncology
2009; 1:23doi:10.1186/1758-3284-1-23
2. Erem C, Hacihasanoglu A, Sari A, Reis A,
Alhan E, Cobanoglu U, Onder Ersöz H, Ukinç
K. Intrathyroideal papil lary thyroid
carcinoma presenting with a solitary brain
metastasis. Endocrine 2004;25(2): 187-93
3. Jianyi Li, Kenneth D Aldape, Gregory N
Fuller,Suzanne Z Powell. Metastatic Papillary
Thyroid Carcinoma in Brain: Report of Three
Cases. The FASEB Journal 2008; 22:706-25.
4. Tsuguhito O, Yukihiro B, Masamichi H,
Nobuyoshi T, Yasushi T, Yoshio K , Masakiyo F.
Papillary Carcinoma of the Thyroid with
Distant Metastases to the Cerebrum: a Case
Report. Japanese Journal of Clinical
Oncology 2001; 31:112-5
5. Brunicardi FC, Andersen DK, Billiar TR, Dunn
DL, Hunter JG, Matthews JB, Pollock RE,
Schwartz SI: Schwartz's Principles Of Surgery.
8th edition. New York: McGraw-Hill; 2005.
6. Misaki T, Iwata M, Kasagi K, Konishi J. Brain
metastasis from differentiated thyroid
cancer in patients treated with radioiodine
for bone and lung lesions.
Ann Nucl Med 2000;14:111-4.
7. Biswal B M, Bal CS, Singh MS, Padhy AK, Rath
GK. Management of intracranial metastases
of differentiated carcinoma of thyroid.
Journal of Neuro-Oncology 1994, 22:77-81
8. Chiu AC, Delpassand ES, Sherman SI.
Prognosis and treatment of brain metastases
in thyroid carcinoma.
J Clin Endocrinol Metab 1997; 82:3637-42.
Key to the Practice Paper
1c, 2b, 3d, 4b, 5b, 6b, 7e, 8b, 9a, 10b, 11a, 12a, 13a, 14a, 15b, 16c, 17a, 18b, 19a, 20b, 21b, 22a, 23a, 24b, 25a,
26b, 27a, 28c, 29d, 30a, 31e, 32a, 33b, 34a, 35d, 36d, 37a, 38d, 39d, 40b, 41a, 42c, 43c, 44d, 45b, 46c, 47d

34
Abstract:
Key words:
Introduction:
Treatment of sepsis is often difficult and
challenging. The problem is aggravated in diabetic
patients. The treatment is based broadly on
diabetic control, broad spectrum antibiotic
therapy, ventilator support, dialysis and other
supportive therapy, may not be sufficient for the
recovery of the patient. Mortality in sepsis with 1
multi-organ failure is around 65%. We report one
unusual case of severe sepsis which ultimately
responded to anti-fungal treatment.
Sepsis, Diabetes, Antifungal.
Sepsis in cases of diabetes has poor outcome.
Diabetic patients are immunocompromised
hence multi organ involvement is much more
frequent then in non diabetics. Infection or
inflammation leads to poor glycemic control which
perpetuates severe infection leading to sepsis and
multi organ failure. Patients treated in ICU with broad
spectrum antibiotics and on ventilator support are
more prone for opportunistic infection like yeast, 2,3fungus, etc.
We report such a case of diabetes mellitus with
severe sepsis who ultimately responded to
empirical anti fungal treatment after adequate
antibiotic therapy and organ support treatment
failed to resolve her condition.
Case Report: A 44 year old female a known case of
Type II diabetes mellitus, hypertension,
hypothyroid was admitted with history of fever,
loose motion for last three days. Fever was not
associated with chills or rigor. It was intermittent
type and low grade. The loose motion was watery
and six to seven times a day. There was no history
of cough, vomiting, itching. At the time of
admission her GCS was 15, pulse 102/ minute
regular, all peripheral pulses were well felt, BP-
80/60 mm Hg, chest was clinically clear, heart
sounds were normal. She was admitted to general
ward. Her hypotension did not respond to fluid
challenge and her sensorium deteriorated, so she
was shifted to ICU. Her chest x-ray showed
shadowing in the left lower zone. She developed
acute renal failure .So she had a central line placed
and fluid replacement was done with frequent
measurement of the central venous pressure. She
was intubated and ventilated in pressure
controlled mode. In spite of adequate fluid
replacement her urine output decreased and
hypotension persisted. So she was put on
inotrope support and peritoneal dialysis started
and continued for 40 two litre exchanges with
indwelling time of 20 minutes for each exchange.
All the investigation reports are in the table no: 1
Unusual case of severe Sepsis
Rajyabardhan PattnaikCritical Care Unit,
Sanjib MohantyDeptt. of Internal Medicine
Sradhananda MohapatraDeptt. of Internal Medicine
Address for correspondence:Dr. Rajyabardhan Pattnaik ,
Critical Care Unit, Ispat General Hospital,
Rourkelae-mail : [email protected]
Case Reports

35
DateInvest 22/8 24/8 27/8 29/8 2/9 5/9 7/9 9/9 12/9 15/9 17/9 21/9
Hb 10.6 10 8.7 7.8 9.2 4.6 11.9 11.3
TLC 5700 18800 22000 34200 34300 19900 35900 13500 13100 10000
FBS 62 300 168 94 198 176 156 204 191 159 172 144
Urea 72 76 41 86 96 44 22
Creat 3.5 4.7 2.9 3.4 2.9 1.6 1.1 1.1 1
Na 125 136 134 137 147 148 150 148 137
K 3.8 3.7 3.4 4.4 3.3 2.8 2.2 2.2 5 3.8
Mg 1.4 2.8 1.8
Bill 1.3 0.8 0.5 0.5
SGPT 40 40 41 31
Platelet 10000 80000 88000 190000 200000
CXR LF LZ Opcty Intnsty Lf MiniOpct perst decrsd pl effsn
Table1. Sequential investigations and their results
Fig3. Skiagram showing shadowing of lungs
so inotropes were stopped. Her blood sugar was
well controlled with intermediate insulin. She had
received six units of whole blood and six units of
platelet rich plasma during her hospital stay for
her anemia and thrombocytopenia. All care was
taken to correct her electrolyte imbalance. In spite
of good glucose control, improvement of anemia
and correction of electrolyte imbalance and
improvement of sensorium she could not be
weaned off from ventilator and had persistent
leucocytosis. As she needed prolonged ventilation
and tracheostomy was done on day five of
ventilation. Her nutrition was improved with
enteral feeding. Her antibiotics were upgraded
but still she could not be weaned off from
ventilator and leucocytosis persisted. There was
radiological deterioration of the chest shadowing.
In spite of two weeks broad antibiotic therapy
patient's respiratory effort was poor and
leucocytosis persisted. So empirical antifungal
started with caspofungin with loading dose of
70mg followed by 50mg daily for six days. There
was dramatic improvement of respiratory effort
and general well being. She was given T' piece trial thon 4 day of anti-fungal treatment and tolerated it
very well. Her tracheostomy was closed on the
During peritoneal dialysis her blood pressure
improved and she started passing adequate urine,
Fig 4. Skiagram shows resolution of chest pathology

36
next day (total 17 days). She was ventilated for 22
days out of 30 days of hospital stay. She was
discharged with a diagnosis of Type-II DM,
hypertension, hypothyroidism, acute renal failure
(peritoneal dialysis was done), sepsis fungal
pneumonia. She was followed up for next 4
months without any complications.
Fungal infection now a days has become a
common cause of infection worldwide.
Candidemia is associated with one of the highest
rate of mortality of any bloodstream infection.
The common risk factors for Candida infections
are previous antimicrobial administration,
prolonged corticosteroid therapy, cancer,
chemotherapy, neutropenia, extensive intra-
abdominal surgery or burn, mechanical
ventilation or admission to ICU indwelling CVP 4,5
line, TPN and haemodialysis .
Anti-fungal agents are Amphoterecin B, Azoles,
and Echinocandins. Amphoterecin B works on the
cell membrane of the fungi and increases
membrane permeability leading to leakage of the
cytoplasm and fungal cell depth. The adverse
effects include nephrotoxicity. Azoles works on
the cell membranes by inhibiting fungal
cytochrome P-450 leading to accumulation of
toxic steroles. There is also much drug interaction
with this drug. But echinocandins, specifically
Caspofungin, disrupts cell wall glucan formation
through non competitive inhibition of the enzyme
complex - (1, 3)-D-glucan synthase, present in
most pathogenic fungi and essential for fungal cell
wall formation. It leads to osmotic instability and 5, 6
ultimate lysis of fungal cell wall and is less toxic 6, 7, 8
with a good safety profile .
A bedside scoring system for early antifungal
treatment in non-neutropenic critically ill patient
with candida colonisation will be helpful. The
variables are multifocal candida species
colonization score 1, surgery on ICU admission
score 1, TPN score 1, severe sepsis score 2. If the
total score is more than 2.5 it helps intensivists to
select patients who will benefit from anti fungal 9
administration.
In our case the risk factor were diabetes mellitus,
broad spectrum antibiotics and prolonged
Discussion:
ventilation. Since the patient could not be weaned
off from ventilator and there was persistent
leucocytosis, the diagnosis of fungal infection was
entertained. Since the patient had acute renal
failure treatment with Amphotericin infusion was
ruled out. So Caspofungin was administered. The
dramatic recovery after caspofungin therapy is a
proof that the patient was having opportunistic
fungal infection which responded well to
antifungal treatment.
References:
1. Todi S, Chatterjee S, Sahu S , Bhattacharyya M.
Epidemiology of severe sepsis: An update
Critical care 2010:14 (suppl 1): 382.
2. Edmond MB, Wallace SE, McClish DK et.al.
nosocomial bloodstream infections in United
States hospitals; A 3 year analysis. Clin infect
Dis 1999;29:239-244.
3. Pfaller MA, Jones RN, Doem GV and the
SENTRY participant group ; Bloodstream
infections due to Candida species ; SENTRY
antimicrobial surveillance program in North
America and Latin America 1997-1998.
Antimicrob Agents Chemother 2000;44:747-
751.
4. Garber G. An overview of fungal infection.
Drugs 2001;61(suppl 1):1-12.
5. Blumberg HM, Jarvis WR, Soucie JM et al and
the NEMIS study group. Risk factor for
candidal bloodstream infection in surgical
intensive care unit patients: Clin Infect Dis
2001; 33: 177-186 Debono M et.al antibiotic
that inhibits fungal cell wall development.
Annu Rev Microbial 1994;48:471-497.
6. Debono M et.al antibiotic that inhibits fungal
cell wall development. Annu Rev Microbial
1994;48:471-497.
7. Keating GM, Jarvis B, Caspofungin, Drugs
2001;61:1121-1129.
8. Sawistowska, Schroder ET, Kerridge D, Perry H.
Echinocandin inhibition of 1,3,-b-D-glucan
Synthase from candida albicans. FEBS Lett
1984; 173: 134-138.
9. Leon C. A bedside scoring system for early
antifungal treatment in non neutropnic
critically ill patients. Crit Care Med
2006;34.730-737.

37
Abstract
Key words
Case Report
Chonal stenosis and atresia is often seen in
immediate neonatal period and presents with
respiratory distress.However single nostril as an
associated anomaly with choanal stenosis has not
yet been reported. In Ispat general hospital
one newborn was delivered with such anomaly
and resusciated successfully.
Choanal stenosis, Single nostril
In Ispat General Hospital,Rourkela a male baby
weighing 2000 gm was delivered to a primi
mother who had an uneventful antenatal
outcome. The baby had respiratory distress with
retraction of chest noticed immediately after
birth. On examination, the baby had a single
nostril. A nasal catheter could pass only ½ to 1
centimetre through the nostril. Some degree of
nasal obstruction was suspected. Even after
frequent suctioning of throat respiratory distress
persisted and baby became cyanosed after few
minutes and started crying. As the baby cried,
cyanosis was relieved and he became pink and
quiet (fig-1, 2, 3). Such repeated attacks of
cyanosis which was being relieved after crying
continued to occur. A diagnosis of choanal atresia
was suspected. The baby was transferred to the
nursery. An oral airway was inserted and secured
to the cheeks with tape (fig-4).This relieved the
respiratory distress.
Address for communication :
Dr. P Rath, Sr. Consultant,Deptt. of Pediatrics and Neonatology,
Ispat General Hospital,Rourkela, Email: [email protected]
Figure 1 Immediately after delivery baby
Clinical imaging
Figure 2 Developing cyanosis
Figure 3 Cyanosis relieved after crying
Sidhesh C MishraDeptt. of E.N.T.
Paramananda Rath, Nimain C Nanda, Pitabas MishraDeptt. of Pediatrics and Neonatology
Choanal Stenosis with single nostril a rare Case

38
Figure 4 airway has been secured
He was kept on IV fluid for two days and then was
given gavage feeding. Congenital defects like
Treacher Collins syndrome, palatal abnormalities,
colobomas, tracheoesophageal fistula, and
congenital heart disease were excluded clinically.
Direct visualization through an otoscope couldn't
demonstrate anything abnormal. Plain radiograph
(antero-posterior view) of nasal and paranasal
region were carried out to rule out any septal
anomaly. A lateral radiograph of head with radio
opaque dye pushed through the nostril showed a
stenotic area (fig-5 arrow marked) in the choanal
region. But the dye could pass through the
stenotic area when pushed with pressure. A
diagnosis of Choanal Stenosis was confirmed.
Baby stayed for ten days in nursery and then was
referred to the pediatric surgeon for reconstructive
surgery which was done successfully.
Choanal atresia was first reported in 1830 and is
often seen in newborn period and occurs in 1 in 1
5000 to 8000 live births .It is usually associated
with anomalies likeCHARGE (Coloboma, Heart
defect, Atresia choaenae, Retardation of growth
and genital anomalies), polydactyly, nasal-
auricular and palatal deformities and other cranial 2anomalies . However single nostril associated
with choanal tenosis has not yet been reported.
Newborn babies usually don't have mouth
breathing.In choanal atresia they try to breath
through mouth.When they close their mouth or
are breast fed respiratory distress and cyanosis
occurs. Choanal atresia can be unilateral or
bilateral(20%) and may be associated with other
anomalies stated above.
Diagnosis of choanal atresia is done by
• Typical clinical presentation.
• Direct visualization of the atretic area by
otoscope.
• Taking a radiograph while pushing
radioopaque dye through nasal opening-
atretic or stenotic area can be visualized.
• CT scan can delineate extent of obstruction.
Definitive treatment of choanal atresia/Stenosis
includes
• Transnasal resecn tion by a laser beam.
• Definitive surgical reconstruction.
• Till surgical correction baby's airway to be
maintained by an oral airway and nutrition
maintained by gavage feeding.
• In our case in addition to repair of stenotic
segment cosmetic repair of the nostril was
also needed.
References
1. Pirsig W.Surgery of choanal atrsia in infants
and children:historical notes and updated
reviews,Int J pediatr otorhinolaryngology
II:153,1986
2. Brown K,Rodriguez K,Brown O E.Cummings thOtolaryngology , 4 edition. pp,4099-4109
Discussion
Figure 4 Airway has been secured

39
Residents Section
Accidents in medicine: The idea sends chills down your spine as you conjure up thoughts of
misdiagnoses, mistakenly prescribed drugs, and wrongly amputated limbs. Yet while accidents
in the examining room or on the operating table can be regrettable, even tragic, those that occur
in the laboratory can sometimes lead to spectacular advances, life-saving treatments, and
Nobel Prizes.
A seemingly insignificant finding by one researcher leads to a breakthrough discovery by
another; a physician methodically pursuing the answer to a medical conundrum over many
years suddenly has a "Eureka" moment; a scientist who chooses to study a contaminant in his
culture rather than tossing it out stumbles upon something entirely new.
The story behind the chance discovery of the anti-malarial drug quinine may be more legend
than fact, but it is nevertheless a story worthy of note. The account that has gained the most
currency credits, a South American Indian with being the first to find a medical application for
quinine. According to legend, the man unwittingly ingested quinine while suffering a malarial
fever in a jungle high in the Andes. Needing desperately to quench his thirst, he drank his fill from
a small, bitter-tasting pool of water. Nearby stood one or more varieties of cinchona, which
grows from Colombia to Bolivia on humid slopes above 5,000 feet. The bark of the cinchona,
which the indigenous people knew as quina-quina, was thought to be poisonous. But when this
man's fever miraculously abated, he brought news of the medicinal tree back to his tribe, which
began to use its bark to treat malaria.
Since the first officially noted use of quinine to fight malaria occurred in a community of Jesuit
missionaries in Lima, Peru in 1630, historians have surmised that Indian tribes taught the
missionaries how to extract the chemical quinine from cinchona bark. In any case, the Jesuits'
use of quinine as a malaria medication was the first documented use of a chemical compound to
successfully treat an infectious disease. To this day, quinine-based anti-malarials are widely used
as effective treatments against the growth and reproduction of malarial parasites in humans.
For all those would-be Nobel Prize-winners, remember the one trait that tied all these lucky
strikers together: openmindedness. As the American physicist Joseph Henry once noted, "The
seeds of great discoveries are constantly floating around us, but they only take root in minds well
prepared to receive them."
Quinine
Keep that mind open
ACCIDENTAL BREAKTHROUGHCompiled by :
Suman Behera (Intern)
Pallavi Agarwal (Intern)

40
1. Transitional epithelium is found in
a. thyroid gland
b. distal urethra
c. Ureter
D. small intestine
2. Narrowest part of male urethra is
A. membranous urethra
b. external urinary meatus
c. penile urethra
d. glandular urethra
3. Red nucleus is a part of
a. Thalamus
b. Pons
c. Cerebellum
d. Mid brain
4. Which is not a part of stomach?
a. Fundus
b. Neck
c. Body
d. Pylorous
5. How many lobes are there in left lungs?
a. 1
b. 2
c. 3
d. 4
6. Iron is absorbed in which part of GI tract
a. stomach
b. duodenum
c. jejunum
d. ileum
7. Vit B12 deficiency can occur in
a. ileal resection
b. strict vegetarians
c. parietal cell atrophy
d. total gasrectomy
e. all of the above
8. Which of the following statements is false
for brain death?
a. respiration should have ceased
permanently
b. heart beat should have ceased
permanently
c. reflex spinal movement of limbs may
be present
d. pupils should have no reaction to light
9. pulmonary vein carries
a. oxygenated blood from lungs to heart
b. oxygenated blood from heart to lungs
c. de oxygenated blood from lungs to heart
d. deoxygenated blood from heart to lungs
10. Nephron is seen in
a. central nervous system
b. kidney
c. spleen
d. liver
11. Mid diastolic murmur is classically seen in
a. mitral stenosis
b. aortic stenosis
c. aortic regurgitation
d. mitral regurgitation
12. Axons of a neuron carry impulse
a. away from the cell body
Residents Section
Practice paper
This practice paper is designed to incite intrusiveness amongst all the doctors and particularly for doctors
desirous to take part in different examinations. Though key to the question paper is given elsewhere, all
are requested to verify the answers from standard text books.
Please choose the most appropriate answer to each question.

41
b. low calcium level
c. a marker of Kalazar
20. In AP view of chest, relative position of
tube and film to the chest are as follows
a. Film is kept anterior and tube is
posterior
b. Tube is kept anterior and film is
posterior
c. Both tube and film are kept on the same
side of chest
21. Risk of radiation is highest with
a. X-ray
b. CT scan
c. MRI
d. ultrasound
22. Most probable diagnosis of the image
below is
a. hydrocephalus
b. encephalocele
c. meningocele
d. microcephaly
23. Which of the following phenotype
describes Bombay blood group?
a. hh
b. HH
c. Ao
d. Bo
b. towards the cell body
c. does not carry impulse
13. pH of vagina is
a. acidic
b. alkaline
c. neutral
13. Billirubin level is estimated
a. to know blood viscosity
b. to know liver function
c. to study pulmonary function
d. to know lipid metabolism
14. Autonomic nervous system deals with all of
the followings except
a. skeletal muscle contraction
b. cardiac function
c. pulmonary function
d. digestive function
15. Largest cell in human body is
a. spermatozoa
b. ovum
c. neutrophil
d. RBC
16. PNDT act deals with
a. drug trading
b. protecting the secrecy of patients
c. sex determination of foetus
d. narcotics
17. In emergency, dying declaration can be
taken by the treating doctor himself
a. true
b. false
18. All of the followings are neoplastic
disorders except
a. glioma
b. antibioma
c. neuroblastoma
d. nephroblastoma
19. Hypokalemia is
a. low potassium level

42
24. Sudden onset, intense headache with neck
stiffness should be investigated
immediately to rule out SAH by
a. lumbar puncture
b. CT scan of brain
c. MRI of brain
d. AP view of skull
25. Two scientists were awarded Noble prize
for their work on one vitamin. Name that
vitamin.
a. Vit B12
b. Vit C
c. Vit B6
d. Vit E
26. All of the followings are signs of upper
motor neuron except
a. up going plantar
b. flaccid muscle tone
c. exaggerated deep tendon reflexes
d. abolished superficial reflex
27. Classical lucid interval is described in
a. extradural hematoma
b. subdural hematoma
c. sub arachnoid hemorrhage
d. ventricular hemorrhage
28. Which of the following statements is false
for TIA?
a. it should be taken seriously because it
heralds major episode ahead
b. it allows time to detect treatable causes
and treat them
c. patient should be counseled only
and asked to report immediately if next
attack occurs.
29. Cauda equine syndrome due to any acute
compression should be considered as
surgical emergency because if delay occurs
a. patient may suffer from permanent loss
of bladder and bowel control
b. permanent motor weakness in lower
limbs and lifelong disablity
c. it may invite litigation
d. all of the above
30. Which of the following act of a doctor does
not make him liable under CPA?
a. Not accepting a cold patient for treatment
b. Fixing surgery at a later date after
accepting the patient for treatment
c. foreign body left in abdomen during
surgery due to the fault of the assisting
nurse.
d. not performing a life saving surgery
because no one is available to sign the
consent form.
31. Which of the following may create problem
for a surgeon under the CPA.
a. consent for surgery taken by the ward
sister
b. consent taken on a printed format used
in the hospital for all surgical patients
(blanket consent)
c. consent signed by the husband of a
40 year old lady
d. consent signed by the father of a 25 year
old newly recruited executive of SAIL.
e. all of the above
f. none of the above
32. Trachea bifurcates at which level?
a. D2
b. D3
c. D4
d. D5
33. Choice of treatment in organo-phospherous
poisoning is
a. PAM
b. atropine
c. neostigmine
d. none of the above
e. all of the above
34. Most dreaded complication of falciparum
malaria is
a. cerebral malaria
b. jaundice
c. association with pregnancy
d. bleeding from nose and gums

43
after full recovery plan for surgery
c. careful and expectant observation
d. conservative
42. which of the followings is most confirmatory
for pregnancy
a. urinary presence of HCG
b. morning sickness
c. ultrasonic observation of cardiac activity
of foetus
d. enlargement of mammary glands
43. Post partum period is the period
a. 2 weeks following delivery
b. 4 weeks following delivery
c. 6 weeks following delivery
d. 8 weeks following delivery
44. All of the followings are complications of
duodenal ulcer except
a. perforation
b. bleeding
c. obstruction
d. malignancy
45. which of the following condition is painful
a. hemorrhoids
b. fissure in ano
c. rectal polyp
d. malena
46. smoking is harmful in all of the following
condition except
a. Berger's disease
b. bronchial asthma
c. ulcerative colitis
d. coronary artery disease
47. Which of the followings are signs of fracture?
a. pain
b. swelling
c. deformity
d. all of the above
35. ACE inhibitors are contraindicated in
a. hypertensive encephalopathy
b. intracerebral hemorrhage
c. acute M.I.
d. bilateral ischemic kidney
36. Which statement is true for Type 2 diabetes?
a. they have insulin deficiency from birth
b. it affects persons above forty only
c. initial treatment is insulin
d. none of the above
e. all of the above
37. Which of the following condition is most
serious?
a. acute MI
b. stable angina
c. unstable angina
d. all are equally serious
38. Treatment of choice in pulse less VT is
a. amiodorone
b. verapramil
c. adenosine
d. DC shock
39. Thrombolysis is contraindicated in
a. non-ST elevation MI
b. unstable angina
c. stable angina
d. all of the above
e. none of the above
40. Life span of corpus luteum is
a. 12 days
b. 14 days
c. 16 days
d. 10 days
41. Management of ruptured ectopic pregnancy is
a. resuscitation and surgery should go side
by side without delay
b. blood transfusion, management of shock,
For Key to Practice Paper, Please see page-33.

44
Pandit Nehru in Ispat general Hospital
Doctors of IGH 1962
Down The Memory Lane

45
A page from the 'proceedings of IGH' published in 1981
Down The Memory Lane

46
1. Letter of submission signed by all the authors
2. Type of articles- Original article -2000 words, case reports- 800 words, guide line of IGH for
management of emergency cases 2500 words, article of historical interest -500 words, case reports
in Image -200 words, Review articles on invitation.
3. Figures - Maximum 2 colour photographs per 500 words except case report in images where 4
photographs can be submitted.
4. Three copies of manuscript with copies of illustrations attached to each.
5. Title page
Title of manuscript
Full name(s) and department(s)
Name, Address, Telephone, and e-mail address of corresponding author (first author).
Number of pages, number of figures and number of tables.
6. Abstract (objectives, methods, results, conclusion) along with title, and key words
7. Article proper (double spaced on A/4 size paper) with reference no. immediately following the
description as superscript.
8. Acknowledgements (separate sheet).
9. References (double spaced, separate sheet, Vancouver style).
Maximum number of references for Original articles - 15,Guide lines-15,Case reports - 6, Article of
historical interest or true stories which can inspire young doctors -5.Case reports in images- 5
10. Each table on separate sheet.
11. Figures/diagrams on separate sheet.
12. Photographs in envelope appropriately marked.
13. Legends on separate sheet
14. Since proceedings of IGH is our in house publication, articles are not copyright protected by this
publication. Authors can publish their articles in other journals as per the prevailing rules of RSP.
15. Statement regarding Ethics Committee Approval and informed consent from subjects.*
16. CD's / DVD's of the article if article is submitted in hard copies
1. Online submission is encouraged and preferred.
18. e-mail: [email protected]
Instructions for the Authors

Rourkela Steel Plant, was the first integrated steel plant in the Public Sector in India. This vision of
Pandit Nehru, the first ‘Temple’ of modern India, began to take shape in the mid-fifties. To
cater to the health need of the massive inflow of workforce to Rourkela a modest beginning was
made in the form of a small medical centre in 1955. In 1956 a First- Aid centre was started in the Steel
Plant and in the year 1959, the building, which houses the present day Ispat General Hospital
(IGH), came into existence.
As the years passed IGH kept pace with times and technology adding new facilities to its repertoire.
Today IGH is a 700-bedded state of the art hospital with a pool of 125 competent doctors and 612
paramedics. It extends treatment to more than 9 lakh people at its outpatient department, on an
average, in a year. In the inpatient department more than 30 thousand persons get treated annually
out of which about 40% are non-entitled patients.
The hospital has facilities in super specialities like neurosurgery, burn and plastic surgery. The
hospital also provides lifesaving interventions like dialysis, pacemaker implantation and
chemotherapy. Total hip and knee replacement, brain and spinal cord surgery, urological
procedures are routinely taken up apart from laparoscopic and open surgical procedures in
Surgery and Obstetrics department. Laser surgery and phaco-emulsification in Ophthalmology and
bronchoscopic surgery in ENT department make this hospital one of its kind in the entire state of
Odisha.
IGH is equipped with many modern investigating facilities like 3rd generation CT scan, 1.5 Tesla MRI
machine and sophisticated laboratory medicine department comprising Pathology, Microbiology
and Biochemistry departments. Nuclear medicine and blood transfusion facilities greatly facilitate
the treatment of patients.
On the research front, IGH is a WHO recognized research centre for Malaria and the faculty
members of IGH are regularly invited to impart training in other countries. The hospital is equipped
with a molecular laboratory for research work. Paediatric department of the hospital is participating
in research work in the international field in neonatal infection control. Contribution of the hospital
to the future generations of medical professionals is also immense as most of the research work is
published in international medical journals.
This premier hospital is also recognised for imparting post graduate training in most of the
disciplines of medical science. The performance of the students of this Institution is highly
satisfying – an eloquent testimony to the quality of training they are receiving here.
At present Ispat General Hospital caters to the complete health needs of employees of the steel
plant and their family members. Citizens of Rourkela and nearby districts too reach out to the
hospital. Besides, people of Jharkhand, Chhattisgarh and Madhya Pradesh make IGH their health
destination from time to time.
Ispat General Hospital which has redefined health care in the region epitomises concern and
commitment.
Ispat General Hospital: An Overview

ROURKELA STEEL PLANT