Embed Size (px)
Citation preview
CHRONIC TRAUMATIC ENCEPHALOPATHY
Gary Oh
WHAT IS CTE?
A progressive neurodegenerative disease caused by repetitive head trauma
Full-contact athletes and Military
ATHLETICS
First described in 1928 when Dr. Harrison Martland with boxers. “Punch Drunk” later termed dementia pugilistica.
Athletes, mostly retired, have struggled in their later years with depression, substance abuse, anger, memory/motor disturbances, and suicide
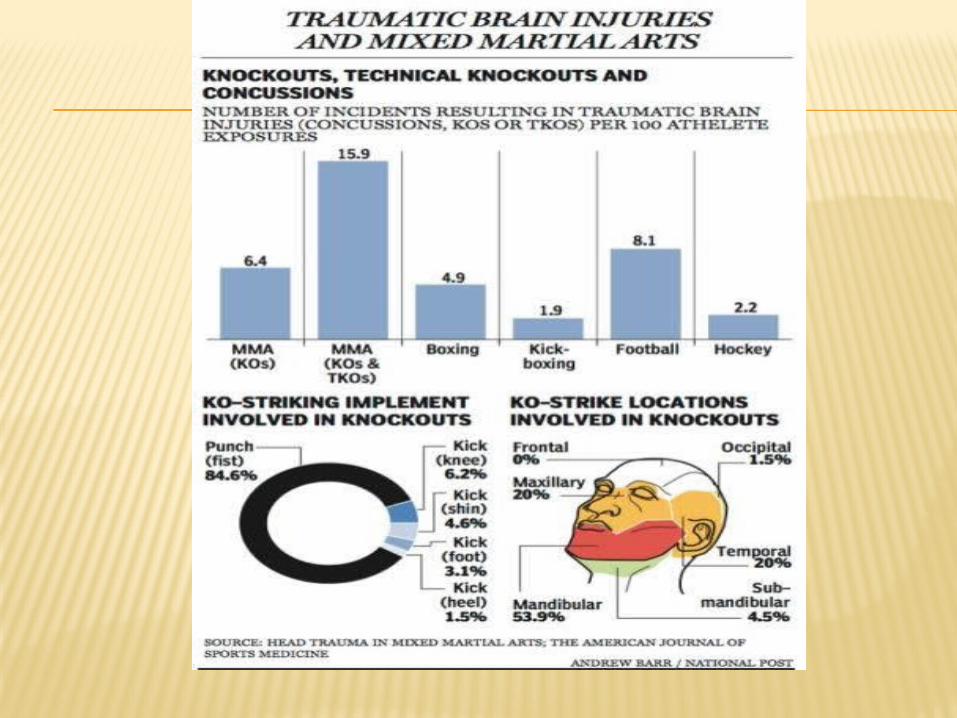
Documented in ice hockey, wrestling and Mixed Martial Arts.
MILITARY
Soldiers returning from the battle with brain injuries from blast trauma causing closed head injury
First appreciated in World War I as shell shock. Currently classified as mild traumatic brain injury (TBI).
CTE may yet play an undefined role in PTSD, postconcussive syndrome, post-traumatic headache, chronic neurocognitive impairment, post traumatic dementia.
CTE is uniquely difficult to study because all clinical examinations are post-mortem and must be done retrospectively through interviews conducted with family members of the deceased.
EPIDEMIOLOGY
90% of all brain injuries are concussion or mild traumatic brain injury (1.5 million USA annually)
Common occurrence in athletes (100-300,000 annually in football alone and underreported)
The Defense and Veterans Brain Injury Center estimates that approximately 270,000 blast exposures have occurred over the past decade
CLINICAL PRESENTATION
<3 mo concussion, >3 mo PCS, persisting or permanent PCS consider CTE
Onset often starts later in the lives of athletes after individual has removed themselves from competition (x=26-76 yo)

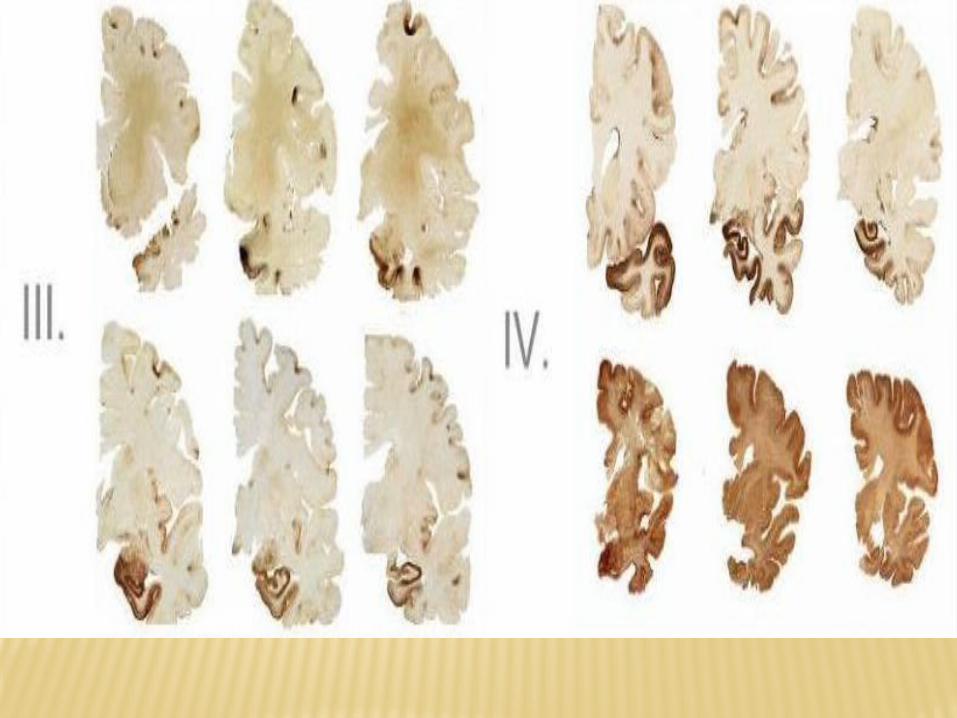
McKee 2009 Proposed 4 stages: First: Headache and loss of attention /
concentration. Perivascular tau NFT in frontal and lateral deep sulci cortices
Second: Depression and mood swings, explosivity, loss of attention and concentration, headache and short-term memory loss. Neurofibrillary tangles were found in superficial cortical layers adjacent to the focal epicenters and in the nucleus basalis of Meynert and locus coeruleus
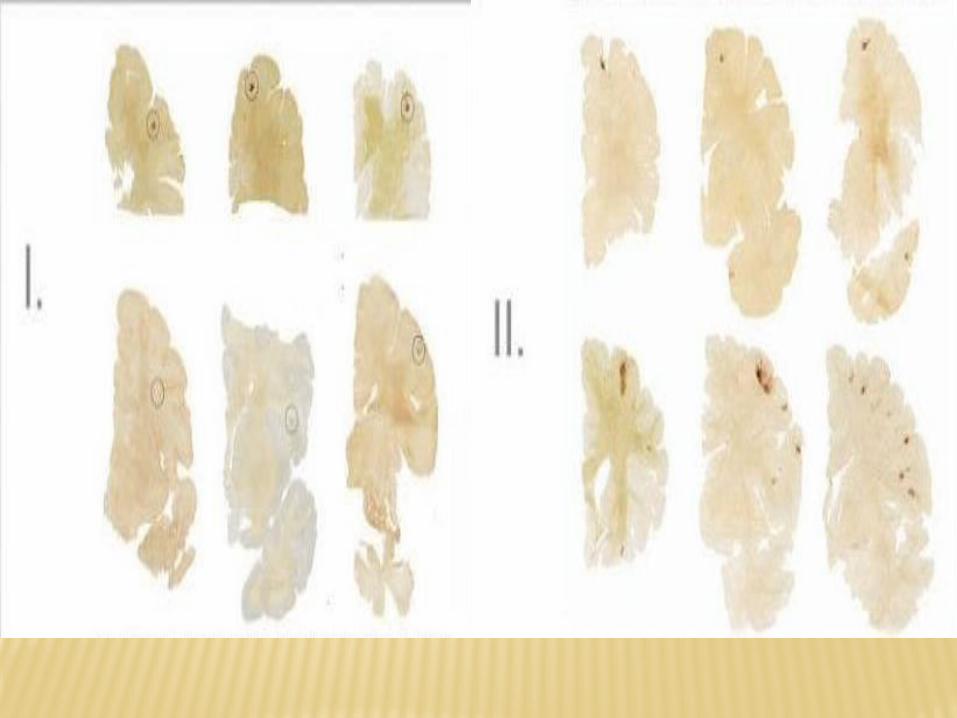
Third: Continued cognitive impairment (memory loss, executive dysfunction, loss of attention and concentration, depression, explosivity and visuospatial abnormalities).
Mild cerebral atrophy, septal abnormalities, ventricular dilation, a sharply concave contour of the third ventricle and depigmentation of the locus coeruleus and substantia nigra.
Microscopically, there was dense tau pathology in medial temporal lobe structures (hippocampus, entorhinal cortex and amygdala) and widespread regions of the frontal, septal, temporal, parietal and insular cortices, diencephalon, brainstem and spinal cord
Fourth: Demented with profound short-term memory loss, executive dysfunction, attention and concentration loss, explosivity and aggression. Most also showed paranoia, depression, impulsivity and visuospatial abnormalities
Further cerebral, medial temporal lobe, hypothalamic, thalamic and mammillary body atrophy, septal abnormalities, ventricular dilation and pallor of the substantia nigra and locus coeruleus.
Microscopically, tau pathology involved widespread regions of the neuraxis including white matter, with prominent neuronal loss and gliosis of the cerebral cortex and hippocampal sclerosis
PATHOPHYS
Repetitive traumatic brain injury from the acceleration/deceleration forces of closed head impacts (coup-countercoup)
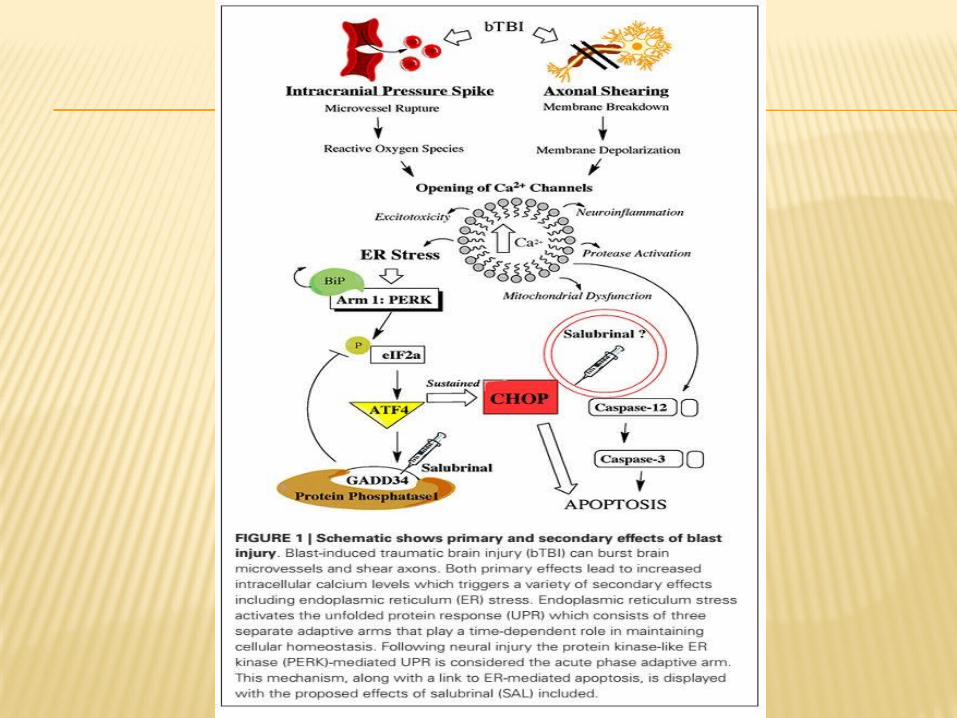
High-speed decelerations may also cause mechanical and chemical injury to the long axons resulting in traumatic/diffuse axonal shearing/tearing plus arteriole and capillary endothelial damage (BBB breakdown and Microglial Immunoexcitotoxicity)
Subsequent acute inflammation and neurodegeneration of axons (Tangled Tau). Acutely rapid axonal swelling, perisomatic axotomy, and Wallerian degeneration.
Chronic inflammation perpetuates damage long term over the next decades.
BBB BREAKDOWN
CSF fluid enters the brain parenchyma along the Virchow–Robin spaces surrounding penetrating arteries, might explain some of the tendency toward perivascular nests of tau-immunoreactive NFT.
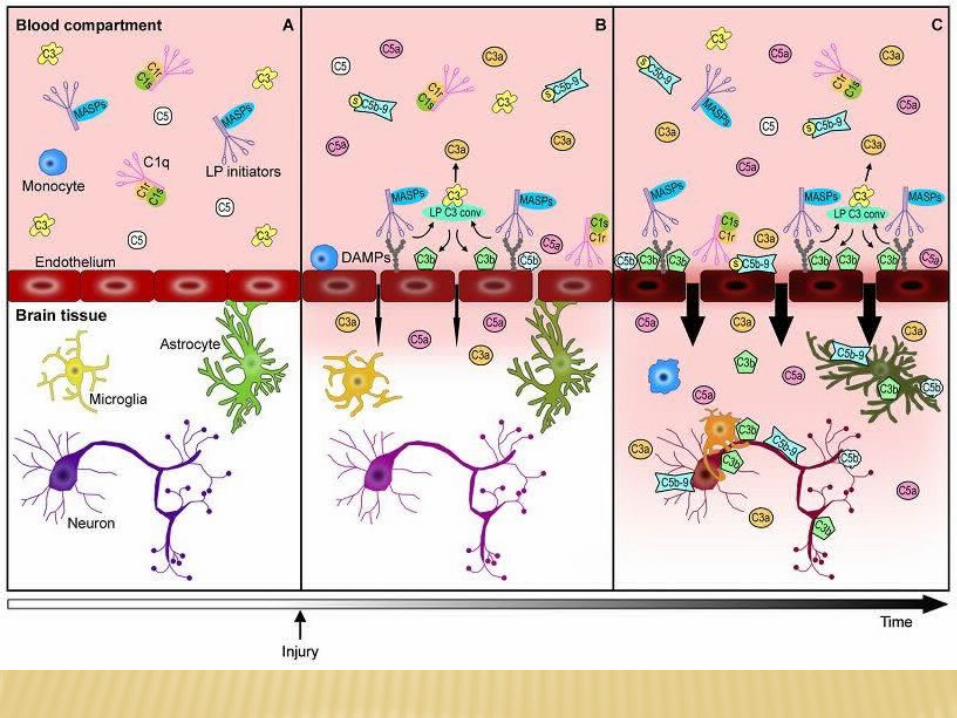
BBB breakdown leads to inflammatory cytokines (C3b C5a) penetrating CNS and activating microglia which further damage brain parenchyma.
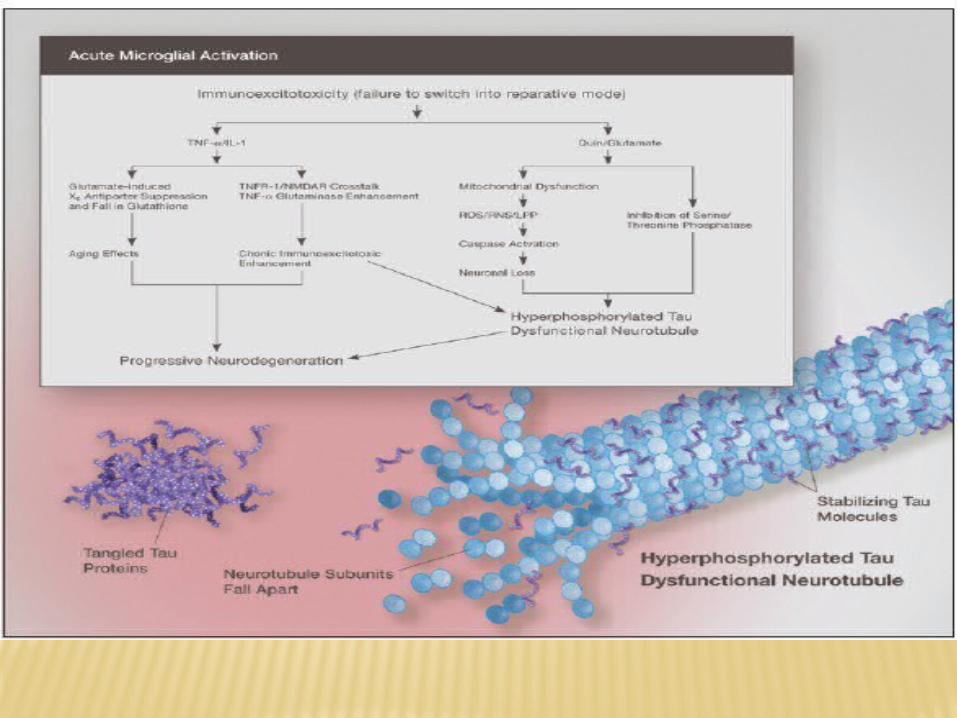
MICROGLIAL IMMUNOEXCITOTOXICITY Continued head trauma releases toxic
levels of cytokines, chemokines, immune mediators, and excitotoxins (glutamate, aspartate, and quinolinic acid).
Excitotoxins inhibit phosphatases, which results in hyperphosphorylated tau and eventually microtubule dysfunction and neurofibrillary tangle deposition perivascularly.
Damage induced Ca2+ influx and ER stress triggers release of caspases and calpains. This further enhances tau phosphorylation, misfolding, shortening, and aggregation as well as cytoskeleton failure with dissolution of neurofilaments and microtubules
Synergy between inflammatory cytokines and glutamate excitotoxicity worsen neurodegeneration
This multi-punch combination increases oxidative stress and nitrogen intermediates that interfere with glutamate clearance keeping the injury response high
TAU TANGLES
Tau is primarily associated with microtubules in axons, where it is neither toxic nor associated with neurofibrillary pathology
Brain trauma causes tau to become dissociated from microtubules in axons (via Ca2+ influx, glutamate excitotoxicity and kinase activation) mediating intracellular tau hyperphosphorylation, misfolding, aggregation and proteolytic cleavage
CHRONIC INFLAMMATION
As the brain grows older, microglial activation compounds with weaker mitochondrial functioning, neuronal and glial dystrophy, higher levels of inflammation, and lifetime exposures to environmental toxins
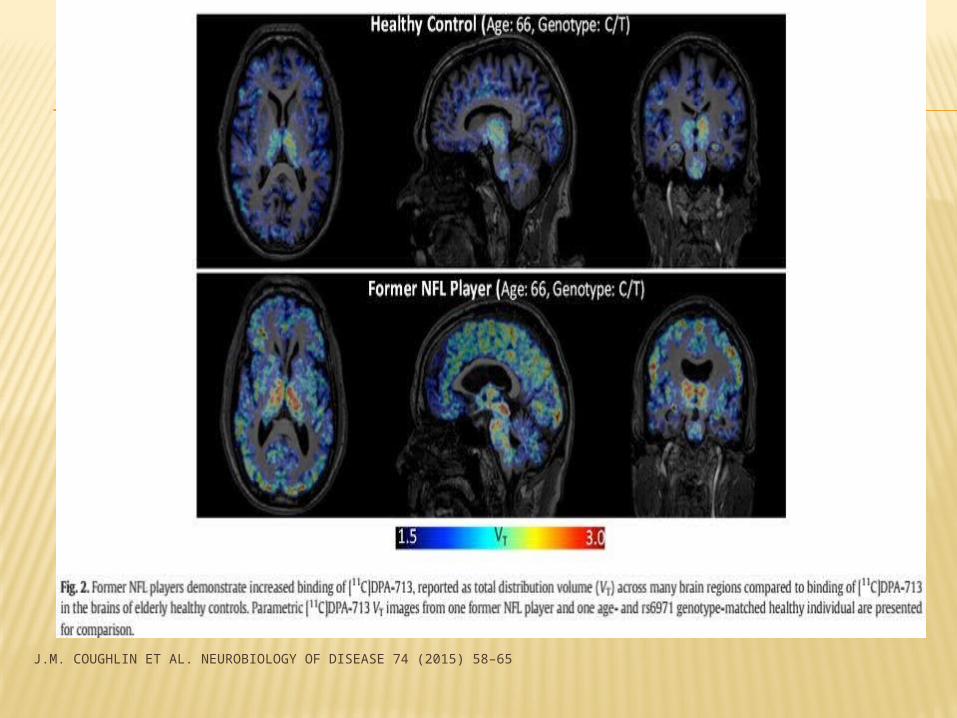
J.M. COUGHLIN ET AL. NEUROBIOLOGY OF DISEASE 74 (2015) 58–65
GROSS PATH
Extensive atrophy in both cerebral hemispheres (particularly in the frontal, temporal and parietal lobes) as well as subcortical structures including the olfactory bulbs, thalamus, mammillary bodies, brainstem, and cerebellum.
Enlargement of the lateral and third ventricles
Thinning of the corpus callosum Reduction in brain mass
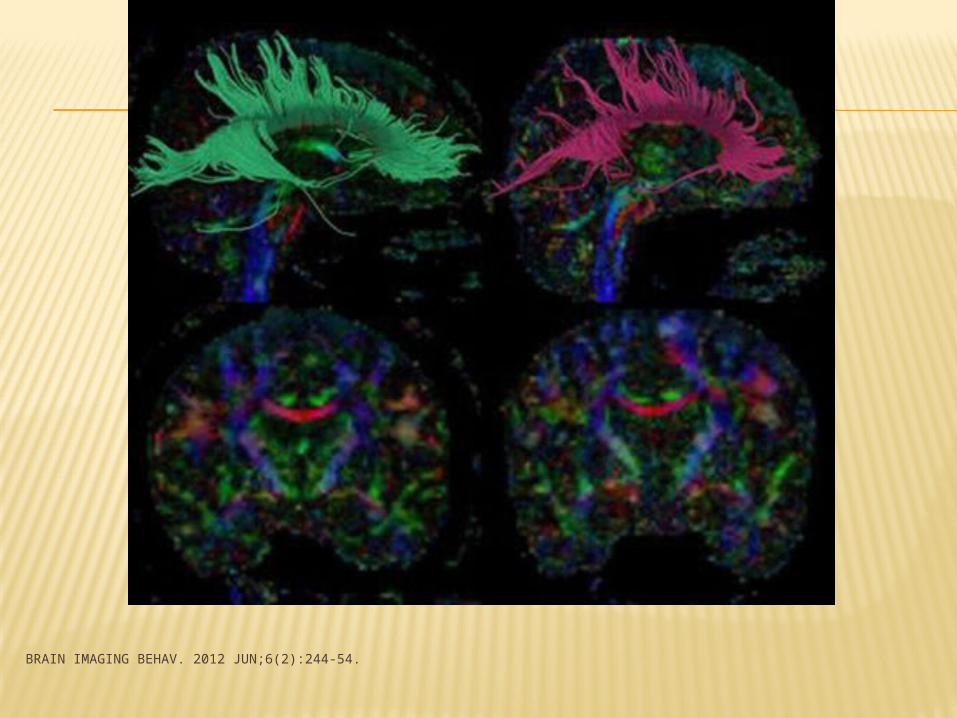
BRAIN IMAGING BEHAV. 2012 JUN;6(2):244-54.
MICROPATH
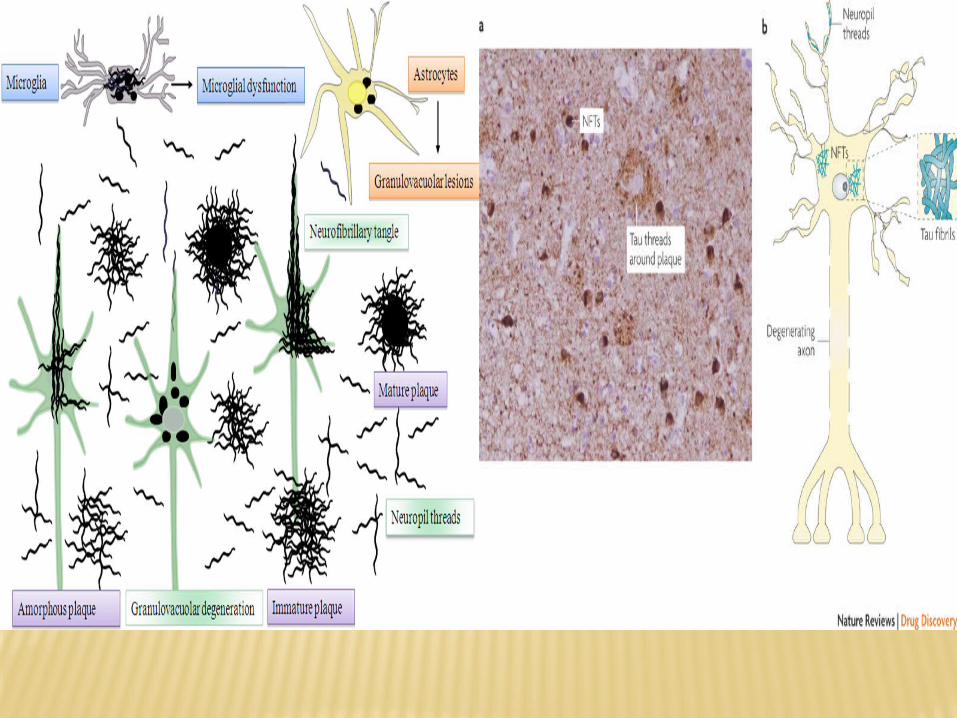
Abnormalities in Tau protein deposition is a hallmark of CTE.
The basic feature of CTE is the presence of sparse, moderate, or frequent band-shaped, flame-shaped small globose and large globose neurofibrillary tangles (NFTs) in the brain accompanied by sparse, moderate, or frequent neuropil threads (NTs)
NFT clusters are generally denser in CTE and they form at the depths of randomly distributed superficial cortical laminae, perivascular around small blood vessels
Beta-amyloid (Aβ) deposition is an inconsistent finding in CTE (Very common in Alzheimer’s Dz)
PROGNOSIS
One of the key features of CTE is that the disease continues to progress decades after the activity that produced traumatic injury has stopped.
It is most likely that multiple pathological cascades continue to exert their effects throughout the individual’s lifetime once they are triggered by repetitive trauma
The longer the survival after the initial events and the more severe the original injuries, the greater the severity of the neurodegeneration.
It is clear that neuronal loss, cerebral atrophy, and ventricular enlargement all increase with longer survival and greater exposure to repetitive trauma
REFERENCES Abdul-Muneer, P. M., Schuetz, H., Wang, F., Skotak, M., Jones, J., Gorantla, S., et al. (2013). Induction of oxidative and nitrosative damage leads to cerebrovascular inflammation in an animal model of
mild traumatic brain injury induced by primary blast. Free Radic. Biol. Med. 60, 282–291. Abdul-Muneer, P. M., Chandra, N., and Haorah, J. (2014). Interactions of oxidative stress and neurovascular inflammation in the pathogenesis of traumatic brain injury. Mol. Neurobiol. doi:
10.1007/s12035-014-8752-3. [Epub ahead of print] Arun, P., Abu-Taleb, R., Oguntayo, S., Tanaka, M., Wang, Y., Valiyaveettil, M., et al. (2013). Distinct patterns of expression of traumatic brain injury biomarkers after blast exposure: role of compromised
cell membrane integrity. Neurosci. Lett. 552, 87–91. Baugh CM et al. Chronic Traumatic Encephalopathy: Neurodegeneration following Repetitive Concussive and Subconcussive Brain Trauma, Brain Imaging Behav. 2012 Jun;6(2):244-54. R. L. Blaylock and J. Maroon, “Immunoexcitotoxicity as a central mechanism in chronic traumatic encephalopathy-a unifying hypothesis,” Surgical Neurology International, vol. 2, article 107, 2011. Chen, Y., Huang, W., and Constantini, S. (2013a). Concepts and strategies for clinical management of blast-induced traumatic brain injury and posttraumatic stress disorder. J. Neuropsychiatry Clin.
Neurosci. 25, 103–110. doi: 10.1176/appi. neuropsych.12030058 Chen, Y., Huang, W., and Constantini, S. (2013a). Concepts and strategies for clinical management of blast-induced traumatic brain injury and posttraumatic stress disorder. J. Neuropsychiatry Clin.
Neurosci. 25, 103–110. Coughlin JM. Neuroinflammation and brain atrophy in former NFL players: An in vivo multimodal imaging pilot study. Neurobiology of Disease 74 (2015) 58–65 D. H. Daneshvar, C. M. Baugh, C. J. Nowinski, A. C. McKee, R. A. Stern, and R. C. Cantu, “Helmets and mouth guards: the role of personal equipment in preventing sport-related concussions,” Clinics in
Sports Medicine, vol. 30, no. 1, pp. 145– 163, 2011 S. T. DeKosky, M. D. Ikonomovic, and S. Gandy, “Traumatic brain injury—football, warfare, and long-term effects,” New England Journal of Medicine, vol. 363, no. 14, pp. 1293–1296, 2010 Diaz-Arrastia R, Baxter VK: Genetic factors in outcome after traumatic brain injury: what the human genome project can teach us about brain trauma. J Head Trauma Rehabil 2006, 21:361 –374. Benjamin Falcon, Annalisa Cavallini, Conformation Determines the Seeding Potencies of Native and Recombinant Tau Aggregates J Biol Chem. 2015 Jan 9; 290(2): 1049–1065. Farrell-Carnahan, L., Franke, L., Graham, C., and McNamee, S. (2013). Subjective sleep disturbance in veterans receiving care in the veterans affairs polytrauma system following blast-related mild
traumatic brain injury. Mil. Med. 178, 951– 956. M. Fourtassi, A. Hajjioui, A. E. Ouahabi, H. Benmassaoud, N. Hajjaj-Hassouni, and A. E. Khamlichi, “Long term outcome following mild traumatic brain injury in Moroccan patients,” Clinical Neurology and
Neurosurgery, vol. 113, no. 9, pp. 716– 720, 2011. B. E. Gavett, R. A. Stern, and A. C. McKee, “Chronic traumatic encephalopathy: a potential late effect of sportrelated concussive and subconcussive head trauma,” Clinics in Sports Medicine, vol. 30, no.
1, pp. 179–188, 2011 Goldstein et al. Alzheimer's Research & Therapy 2014, 6:64, Considerations for animal models of blast-related traumatic brain injury and chronic traumatic encephalopathy Hughes DG, Jackson A, Mason DL, et al. Abnormalities on magnetic resonance imaging seen acutely following mild traumatic brain injury: Correlation with neuropsychological tests and delayed
recovery. Neuroradiology 2004;46:550–58 Jordan BD: Genetic influences on outcome following traumatic brain injury. Neurochem Res 2007, 32:905–915. Jordan BD. Chronic Traumatic Encephalopathy and Other Long-term Sequelae. Continuum (Minneap Minn) 2014;20(6):1588–1604 Kay AD, Day SP, Kerr M, et al. Remodeling of cerebrospinal fluid lipoprotein particles after human traumatic brain injury. J Neurotrauma 2003;20:717–23. Kraus MF, Susmaras T, Caughlin BP, et al. White matter integrity and cognition in chronic traumatic brain injury: a diffusion tensor imaging study. Brain 2007;130:2508–19. Mahley RW, Huang Y: Apolipoprotein E sets the stage: response to injury triggers neuropathology. Neuron 2012, 76:871 –885. H. S. Martland, “Punch drunk,” Journal of the American Medical Association, vol. 91, pp. 1103–1107, 1928. McAllister TW: Genetic factors modulating outcome after neurotrauma. PM R 2010, 2:S241 –S252. Ann C. McKee et al, Brain 2013: 136; 43–64, The spectrum of disease in chronic traumatic encephalopathy A. C. McKee, R. C. Cantu, C. J. Nowinski et al., “Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury,” Journal of Neuropathology and Experimental Neurology,
vol. 68, no. 7, pp. 709–735, 2009 B. Omalu, J. Bailes, R. L. Hamilton et al., “Emerging histomorphologic phenotypes of chronic traumatic encephalopathy in american athletes,” Neurosurgery, vol. 69, no. 1, pp. 173–183, 2011 B. I. Omalu, J. Bailes, J. L. Hammers, and R. P. Fitzsimmons, “Chronic traumatic encephalopathy, suicides and parasuicides in professional American athletes: the role of the forensic pathologist,”
American Journal of Forensic Medicine and Pathology, vol. 31, no. 2, pp. 130–132, 2010. Schmidt ML, Zhukareva V, Newell KL, et al. Tau isoform profile and phosphorylation state in dementia pugilistica recapitulate Alzheimer’s disease. Acta Neuropathol 2001; 101: 518–24 D. J. Thurman, C. M. Branche, and J. E. Sniezek, “The epidemiology of sports-related traumatic brain injuries in the United States: recent developments,” Journal of Head Trauma Rehabilitation, vol. 13,
no. 2, pp. 1–8, 1998. Rosenfeld, J. V., and Ford, N. L. (2010). Bomb blast, mild traumatic brain injury and psychiatric morbidity: a review. Injury 41, 437–443. doi: 10.1016/j.injury. 2009.11.018 Verghese PB, Castellano JM, Holtzman DM: Apolipoprotein E in Alzheimer's disease and other neurological disorders. Lancet Neurol 2011, 10:241 –252.
Faden AI and Loane DJ. Chronic Neurodegeneration After Traumatic Brain Injury: Alzheimer Disease, Chronic Traumatic Encephalopathy, or Persistent Neuroinflammation?. Neurotherapeutics (2015) 12:143–150
Orsini F et al. Versatility of the complement system in neuroinflammation, neurodegeneration and brain homeostasis, Frontiers in Cellular Neuroscience, November 2014, 8 (380) 1
Logsdon AF et al. Altering endoplasmic reticulum stress in a model of blast-induced traumatic brain injury controls cellular fate and ameliorates neuropsychiatric symptoms, Frontiers in Cellular Neuroscience, December 2014 | Volume 8 | Article 421 | 1
Lozano D et al. Neuroinflmmatory responses to traumatic brain injury: etiology, clinical consequences, and therapeutic opportunities. Neuropsychiatric Disease and Treatment 2015:11 97–106
McKee AC and Robinson ME. Military-related traumatic brain injury and neurodegeneration. Alzheimers Dement. 2014 June ; 10(3 0): S242–S253 Montenigro PH et al. Clinical subtypes of chronic traumatic encephalopathy: literature review and proposed research diagnostic criteria for traumatic
encephalopathy syndrome, Alzheimer's Research & Therapy 2014, 6:68 Saulle M and Greenwald BD. Chronic Traumatic Encephalopathy: A Review. Rehabilitation Research and Practice Volume 2012, 9 pages





























