Embed Size (px)
Citation preview
Chronic Traumatic Encephalopathy in Sports
Tennessee Psychological AssociationNovember 5, 2011Nashville, TNNashville, TN
Gary Solomon, Ph.D., ABN
Associate Professor, Departmentsof Psychiatry and Neurological Surgery, Vanderbilt University School of Medicine
Team Neuropsychologist, Nashville PredatorsConsulting Neuropsychologist, Tennessee TitansConsulting Neuropsychologist, TN Secondary
School Athletic Association
Disclosures/Competing Interests
• I receive royalties from book sales
• I receive consulting fees from the Nashville Predators • I receive consulting fees from the Nashville Predators and the Tennessee Titans
• I am involved in beta testing of a new module for ImPACT, and receive free use of the test for 1 year
• This presentation is not endorsed by any organization with which I am affiliated
Overview: Chronic Traumatic Encephalopathy
History of CTE: BoxingCTE in American professional footballNFL autopsy studiesSports CTE groupsThe media and CTEThe media and CTEPublished studies of CTETau and FTDTau and Alzheimer’s diseaseQuestions about CTEScientific summary of CTE

“Anatomic and clinical investigations seem to show definitely that our conception of concussion of the brain must be modified. It is no longer possible to say that “concussion is an essentially transient state which does not comprise any evidence of structural cerebral injury”. Not comprise any evidence of structural cerebral injury”. Not only is there actual cerbral injury in cases of concussion but in a few instances complete resolution does not occur, and there is a strong likelihood that secondary degenerative changes develop”.
Archives of Neurology and Psychiatry, 1927, 18, 181-211
*Read before the Fifty-Second Annual Meeting of the American Neurological Association, Atlantic City, N. J., June 1, 2 and 3, 1926.
Evolution of CTE concept
• Punch-Drunk Syndrome (Martland, 1928, JAMA)
• Dementia Pugilistica (Millspaugh, 1937, US Navy Medical Bulletin)
• Psychopathic deterioration of pugilists (Courville, 1962, Bulletin Los
• Angeles Neuro Society)• Angeles Neuro Society)
• Chronic traumatic encephalopathy (Miller, 1966, Proceedings of The Royal Society of Medicine)
• Chronic traumatic brain injury
(Jordan et al., 1997, JAMA)
Motor: tremor, incoordination,
Harrison Martland, 1928
“Cuckoo”“Goofy”“Slug nutty”
Motor: tremor, incoordination, extrapyramidal and other parkinsonian symptoms
Cognitive: “slight mental confusion”……”marked mental deterioration may set in requiring commitment to an asylum”

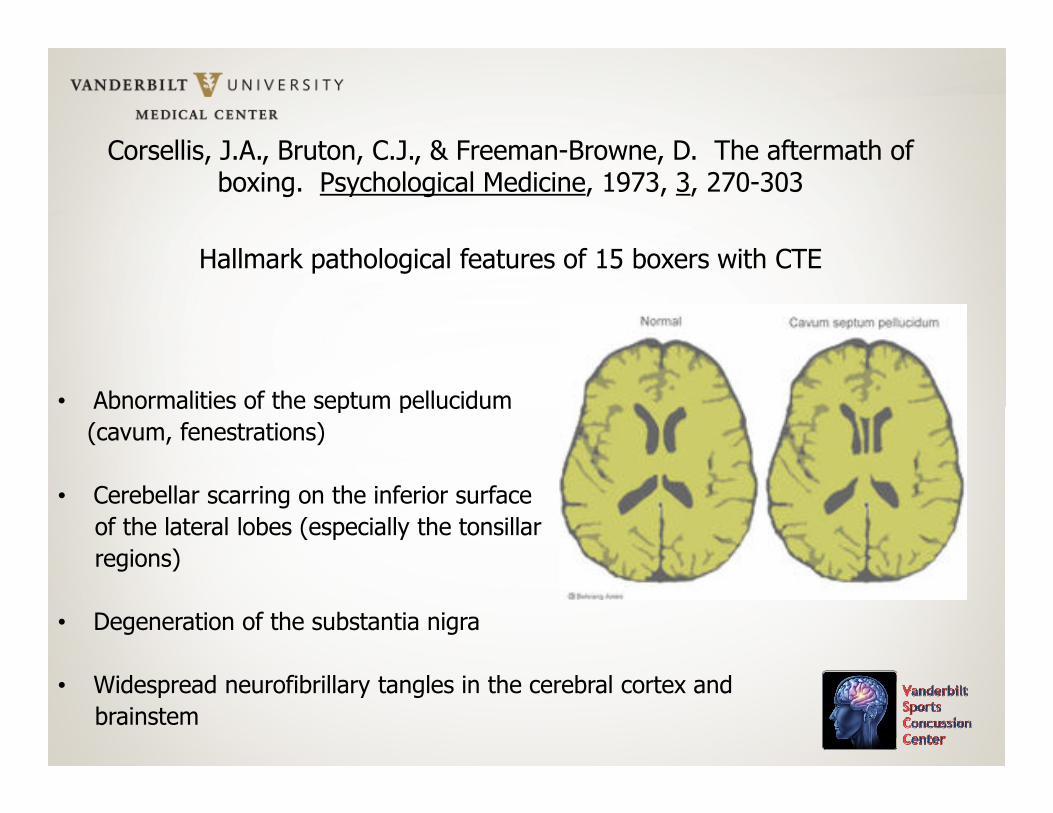
Corsellis, J.A., Bruton, C.J., & Freeman-Browne, D. The aftermath of boxing. Psychological Medicine, 1973, 3, 270-303
Hallmark pathological features of 15 boxers with CTE
• Abnormalities of the septum pellucidum • Abnormalities of the septum pellucidum
(cavum, fenestrations)
• Cerebellar scarring on the inferior surface
of the lateral lobes (especially the tonsillar
regions)
• Degeneration of the substantia nigra
• Widespread neurofibrillary tangles in the cerebral cortex and
brainstem
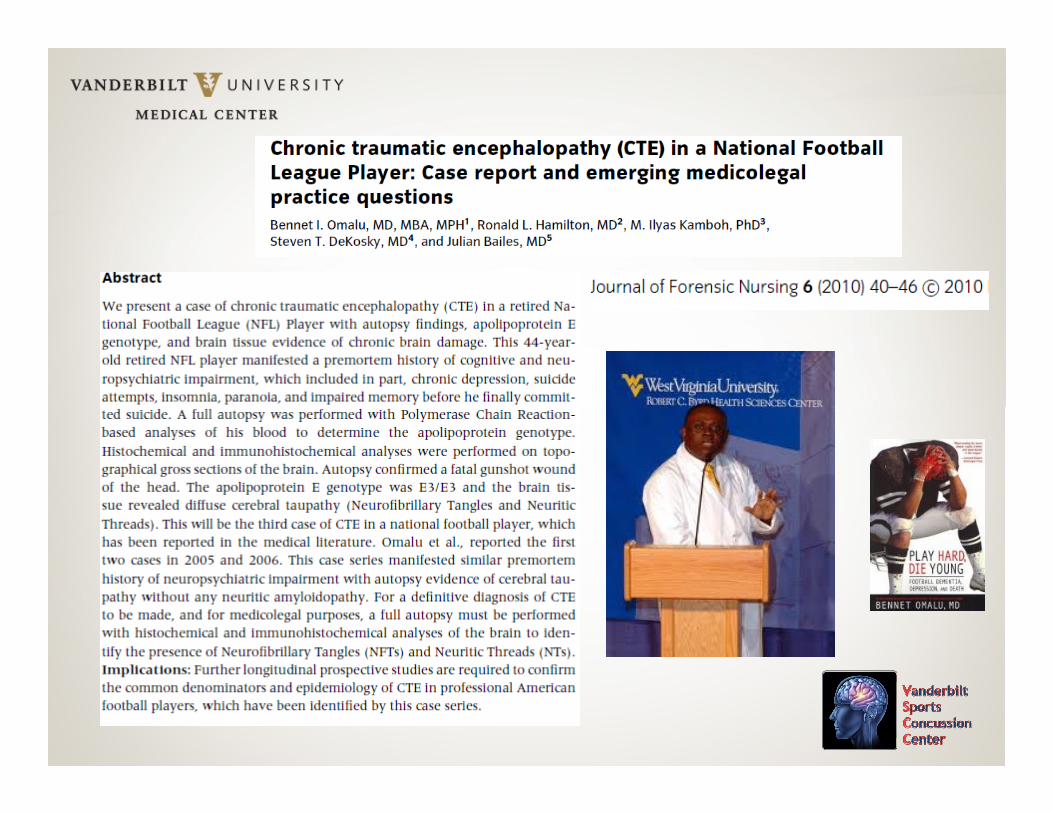
Autopsy Studies of NFL Players
Dr. Bennet OmaluDr. Bennet OmaluPreviously with the Allegheny County Coroner’s Office and the University of Pittsburgh; now a M.E. in in California

Autopsy Report: NFL Player #1Neurosurgery, 2005, 2005, 57, 128, 128--134134
“Iron” Mike Webster
Webster's estate entitled to disability benefits
Pittsburgh Tribune-Review
Friday, December 15, 2006
Rob Biertempfel
Webster, who sustained brain damage from repeated collisions during his 17-year football career, died in 2002 of a heart
attack. After his retirement, Webster was unable to find work and, at times, was
homeless.

Chris Nowinski: Head Games (2006)
Harvard football player and graduate whose career as a professional wrestler was cut short by concussions
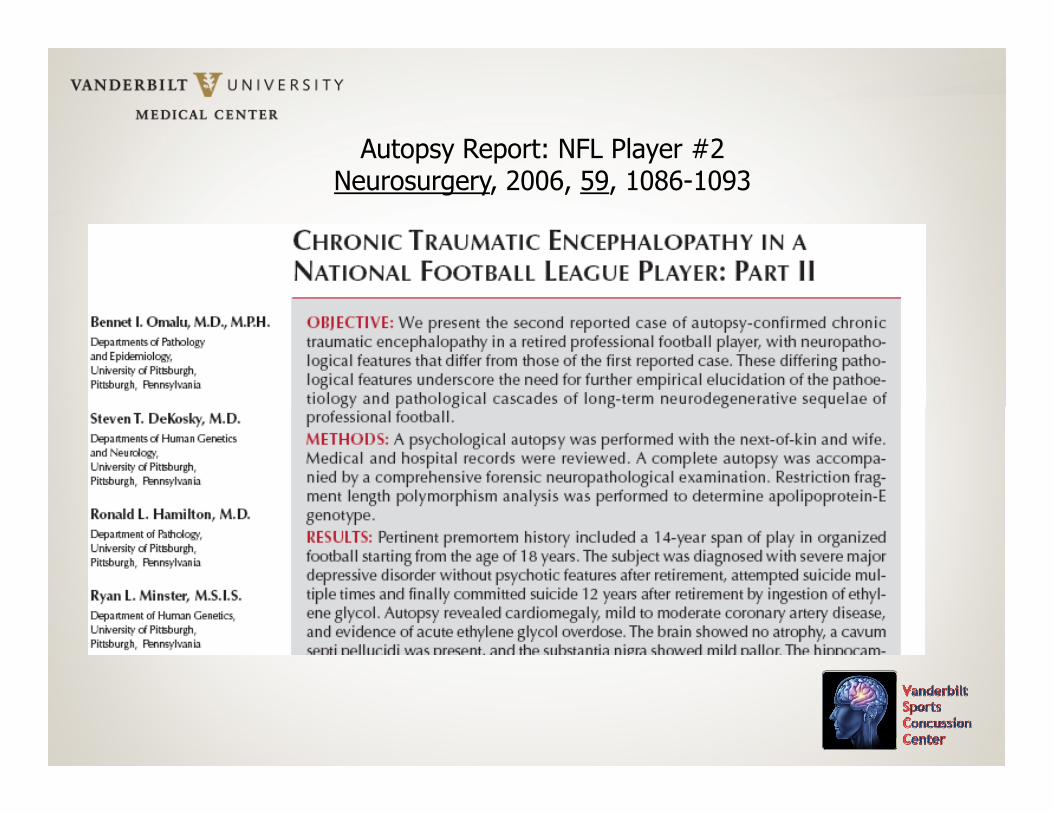
Autopsy Report: NFL Player #2Neurosurgery, 2006, 59, 1086-1093
Thursday, January 26, 2006By Jonathan D. Silver,Pittsburgh Post-Gazette
Suicide ruling in Long's death hasn't ended controversyThursday, January 26, 2006
By Jonathan D. Silver, Pittsburgh Post-Gazette
Toxicology tests and other evidence have revealed that former Steelers lineman Terry Long committed suicide by drinking antifreeze, but the Allegheny County
medical examiner's office also found that head trauma suffered during Mr. Long's eight-year career in the National Football League contributed to his death.
Mr. Long's death June 7 had been ruled accidental. But after further tests revealed the presence of antifreeze in Mr. Long's system,
the manner of death was changed to suicide.
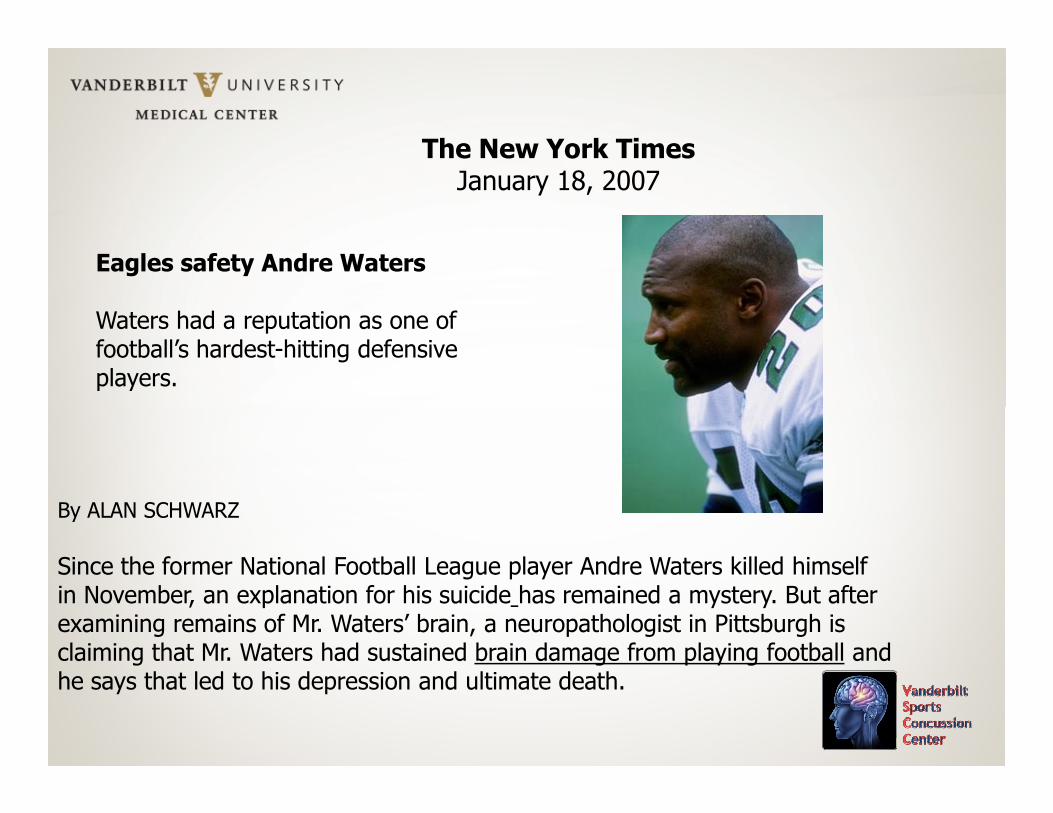
Eagles safety Andre Waters
Waters had a reputation as one of football’s hardest-hitting defensive players.
The New York TimesJanuary 18, 2007
By ALAN SCHWARZ
Since the former National Football League player Andre Waters killed himselfin November, an explanation for his suicide has remained a mystery. But afterexamining remains of Mr. Waters’ brain, a neuropathologist in Pittsburgh is claiming that Mr. Waters had sustained brain damage from playing football andhe says that led to his depression and ultimate death.

Sports Legacy Institute
• Chris Nowinski, Dr. Robert Cantu, Dr. Robert Stern, Dr. Ann McKee, Boston
• Partnered with Boston University School of Medicine to create The Center for the Study of Traumatic Encephalopathy
• www.sportslegacy.org
• www.bu.edu/cste
Brain Injury Research InstituteWest Virginia University School of Medicine
Drs. Julian Bailes and Bennet Omalu,Garrett Webster, Robert Fitzsimmons
Neurosurgery, , 2003-2009
Results published from the NFL mTBI Committee’sresearch: 16 articles based on data collected
from 1996-2001
Pellman steps down as NFL's top concussion expert
February 28, 2007
ESPN.com news services
Pellman, the head of the committee since it was formed in 1994, Pellman, the head of the committee since it was formed in 1994,
asked to be relieved of his duties as chairman, NFL spokesman
Greg Aiello told The Baltimore Sun, who first reported the story.
Dr. Ira Casson, a neurologist from Nassau, N.Y., and Dr. David
Viano, a biomechanical engineer from Wayne State University,
will head the committee, Aiello said.

N.F.L. Scolded Over Injuries to Its Players
By ALAN SCHWARZ
Published: October 28, 2009
New York TimesNew York Times
WASHINGTON — The commissioner of the N.F.L. faced heated
criticism Wednesday before the House Judiciary Committee,
with lawmakers, former players and even a former team
executive accusing the league of neglect in its handling of active
and retired players with brain injuries.
espn.go.com
November 24, 2009, 10:34 PM ET
Goodell announces two resignations
Goodell wrote that Dr. Ira Casson and Dr. David Viano, who have led the league committee on concussions since 2007, "have graciously offered to resign from those positions and to continue to assist the committee in its
important work”.
Casson has come under attack recently from the NFL Players Association and members of Congress for criticizing independent and league-sponsored studies linking NFL careers with heightened risk for dementia and cognitive decline.
Casson did not appear on Capitol Hill that day, and some House members complained when he did not testify. During the hearing, Rep. Linda Sanchez, a California Democrat, played a clip of a TV interview in which Casson denied
evidence of a link between multiple head injuries in NFL players with brain disorders.
Author on 11 of the 16NFL studies in Neurosurgery


Do the ‘Facts’ Really Support anAssociation Between NFL Players’
Concussions, Dementiaand Depression?
By Ira R. Casson, MDNEUROLOGY TODAY, JUNE 3, 2010
“The public has been led to believe that dementia and depression are frequentand an inevitable consequence of a career in professional football. This “falseand an inevitable consequence of a career in professional football. This “false
fact” is belied by the presence of a large number of retired players who, despite experiencing multiple concussions, have gone on to have brilliant
careers in broadcasting and other endeavors as well as the numerous retired playerswho testified so eloquently and articulately before Congress. Many also believe that all retired players who have dementia and depression are suffering as a result of multiple head injuries sustained during their NFL careers. This“false fact” implies that retired NFL players are somehow immune to themultiple risk factors and diseases that are associated with dementia and
depression in the general population”.
In the interim, it is our conclusion based on the literature reviewedthat adverse long-term neurocognitive effects of concussive injuryhave been demonstarted empirically in professional boxers only.
Center for the Study of Retired Athletes at the University of North Carolina at Chapel Hill.
Sent a general health questionnaire to 3,683 living members of the National Football League’s Retired Player’s Association.
A total of 2,552 players responded, yielding a response rate of 69.3%.
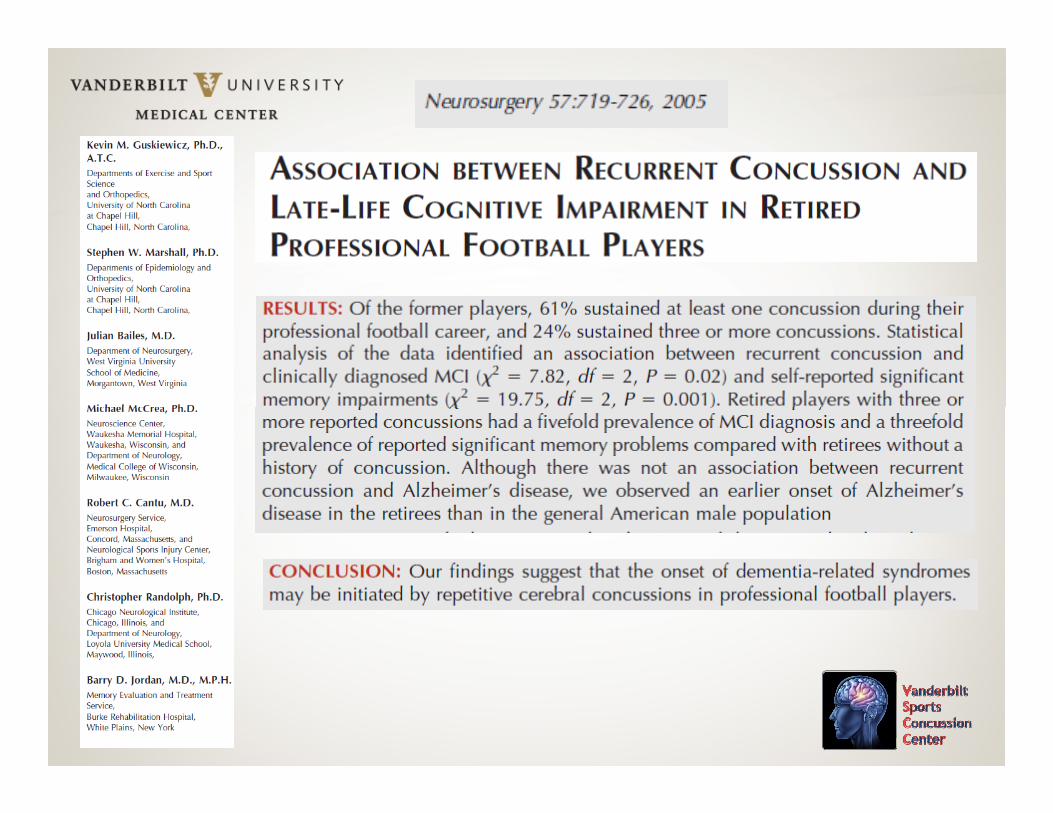
1,513 retirees (60.8%) reported having sustained at least 1 concussion during their professional playing career, and 597 (24%) reported sustaining 3 or more concussions.
17.6% of those athletes sustaining a concussion believed that the concussion had a permanent effect on their thinking and memory skills.
Retirees completed the SF-36 Measurement Model for Functional Assessment of Health and Well-Being, an index of health, well-being, and activities of daily living. The investigators derived a “mental health component score, which includes scores of vitality, social functioning, role emotional, and mental health” (p. 720), and compared the scores of the retired athletes with age-and gender-matched norms.
The Mental Component Scale (MCS) scores on the SF-36 for the NFL retirees aged 50 years and older were similar to those of the general population for all age groups.
However, when players were grouped according to the number of reported concussions sustained while playing professional football, the MCS scores of the retired players with 3 or more concussions were worse than those retirees with 0, 1, or 2 concussions at a statistical probability level < .001.
Inspection of the group means, however, reveals that the average score of the normative group was 52.42 (SD not reported), and the average score of the NFL retirees with 3 or more concussions was 50.31 (SD = 11.26), a mean difference of roughly 2 points.
The standard deviations of the MCS scores of the concussion groups ranged from 8.50 to 11.26. Although mean difference between the groups was statistically significant (with subject between the groups was statistically significant (with subject numbers ranging from 374 to 814 per group), the question arises as to whether this 2-point mean difference between groups is of any clinical, functional, or practical significance.
Guskiewicz and colleagues interpreted this finding as evidence of a “progressive decline in mental health functioning .” (p. 722).
This conclusion may be debatable.
Approximately 4 months later a second survey focusing on memory and issues related to mild cognitive impairment (MCI) was sent to a subset of 1,754 NFL retirees aged 50 years or older, with a copy sent to the player’s informant, defined as a spouse or close relative.
MCI and memory questionnaire data were available for 758 players and from 641 retired players’ spouses/informants.and from 641 retired players’ spouses/informants.
There were 22 cases of physician-diagnosed MCI among the retirees (3 cases involving cerebrovascular accident) and 77 cases of retirees who had significant memory impairment based on informant data.
Although percentages are not reported by the investigators, we calculate a rate of physician diagnosed MCI at 2.9% among retiree-reported data (22/758), and a rate of 12.01% (77/641) based on the informant data.
Plassman et al. (2008) assessed the prevalence of cognitive impairment without dementia (a functional diagnostic equivalent of MCI) in the US population in a longitudinal study conducted from 2001 to 2005.
They found a 16% prevalence rate in the 71- to 79-year-old cohort (the youngest cohort reported), which is closest to the cohort (the youngest cohort reported), which is closest to the older NFL retirees in age (mean age of 62.4 years).
For the NFL retirees, the physician-based diagnosis rate of MCI (2.9%) and the informant-base rate (12.01%) are less than those reported by Plassman and colleagues for the general population (16%).
Age is a critical variable in the prevalence of MCI, as it is the greatest single risk factor for this diagnosis
Plassman et al. did not report prevalence rates of MCI in the Unites States among the 60- to 69-year age range, as most studies use age 70 years as the lower limit for inclusion
Thus, the rates reported earlier based on the Plassman data may not be ideally comparable with the NFL retirees, because may not be ideally comparable with the NFL retirees, because the Plassman cohort is, on average, a decade older than the NFL cohort
However, if the rates reported by the NFL retirees were increased by 50% in an inelegant attempt to make age-appropriate prevalence estimates, the NFL retirees’ prevalence data remain consistent with (and certainly do not exceed)the general US population data reported by Plassman and colleagues

Guskiewicz et al. reported that there was no association between the number of concussions sustained as a professional football player and a diagnosis of AD. Thirty-three retirees (1.3%) reported a physician’s diagnosis of AD.
However, the investigators reported that there was a higher prevalence of AD in the retiree cohort than in the corresponding general population, leading the investigators to conclude that “this group may have an earlier onset of AD than the general American group may have an earlier onset of AD than the general American male population” (p. 721). Plassman and colleagues reported a 5.5% prevalence rate for prodromal AD in the general population.
The 1.3% prevalence rate of AD among NFL retirees reported by Guskiewicz and colleagues is less than the age-matched population rate of 5.5% reported by Plassman and colleagues. Again, however, the age variable must be kept in mind, as theretirees were on average, younger than those in Plassman.
CTE in football: A media phenomenon?
Is this the 21st century equivalentof Freudian “Mass Hysteria”?of Freudian “Mass Hysteria”?
CTE has been discussed primarily in the popular press and only recently has been addressed in the scientific literature
• “…is a progressive neurodegeneration clinically associated with memory disturbances, behavioral and personality changes, parkinsonism, and speech and gait abnormalities” (p. 732).
• “There is overwhelming evidence that the condition is the result of repeated sublethal brain trauma that often occurs well before the development of clinical manifestations” (p. 732).
• “…at least 17% of individuals develop CTE” (p. 709).
• However, in arriving at this prevalence rate, the authors referenced the study by Roberts et al., “The occult aftermath of boxing”, JNNP, 1990, 53, 373-378. The Roberts study was confined to boxers.

CTE cases: McKee et al., 2009
• 51 neuropathologically confirmed cases of CTE; 46 (90%) were athletes
• The 5 non-athletes included 1 patient with epilepsy, 2 with autistic head banging, 1 with physical abuse, and 1 dwarf alcoholic circus clown who was repeatedly shot out of a canon, ages 24-76
• 39 of the 46 athletes (85%) were boxers, both amateurs and professionals, ages 28-91
• 5 (11%) were football players ( 3 OL, 1 DL, 1 LB), ages 36-50. Cause of death among the football players: 2 were suicides (one GSW, one drank antifreeze), 1 was an accidental GSW, 1 died in a high speed MVA, 1 died from a myocardial infarction
• 1 (2%) professional wrestler (age 40)
• 1 (2%) soccer player (age 23)
“To date, there have been no randomized neuropathologic studies of CTE in deceased athletes, and as such, there is a selection bias in the cases that have come to autopsy”.
“Whereas concussion and postconcussion syndrome represent temporary states of neuronal and axonal derangement, CTE is a neurodegenerative disease that occurs years or decades after recovery from the acute or postacute effects of head trauma”.
“The onset of CTE is often in midlife, usually after athleteshave retired from their sport”.
cases that have come to autopsy”.
“…estimated lifetime prevalence of at least 3.7%” in NFL players
Emerging Histomorphologic Phenotypes ofChronic Traumatic Encephalopathy in
American Athletes
Bennet Omalu, Julian Bailes, Ronald L. Hamilton, M. Ilyas Kamboh, Jennifer Hammers, Mary Case,
Robert Fitzsimmons
Neurosurgery, 2011, 69 ,173–183
“We define CTE as a progressive neurodegenerative syndromecaused by single, episodic, or repetitive blunt force impacts to thehead and transfer of acceleration-deceleration forces to the brain.
CTE presents clinically after a prolonged latent period asa composite syndrome of mood disorders and neuropsychiatric
and cognitive impairment…CTE usually presents with a prolonged latency period; however, some patients with
CTE may not exhibit the classic prolonged latencyperiod before clinical symptoms begin”.
(p. 174)

RESULTS:
Ten of 14 professional athletes (71%) were positive for CTE: 7 of 8 football players, 2 of 4 wrestlers, and 1 boxer. One of 3 high school players manifested incipient CTE.
The age range of those with CTE was 18 to 52 years; they were all male athletes.
In all cases of CTE, Alzheimer-type cerebral cortical atrophy was absent; negligible to mild neocortical neuronal dropout was present.
The fundamental neuropathologic feature of CTE was the topographic distribution of sparse, moderate, and frequent band-shaped, flame-shaped, small and large globose neurofibrillary tangles and neuritic threads in the cerebral cortex, subcortical nuclei/basal ganglia, hippocampus, and brainstem nuclei.
Does tau protein accumulation from brain trauma cause these cognitive and neurobehavioral abnormalities in mid-life reported in
professional athletes with CTE?
Let’s look at Alzheimer’s and Frontotemporal Diseasesas parallel Tau-related processes
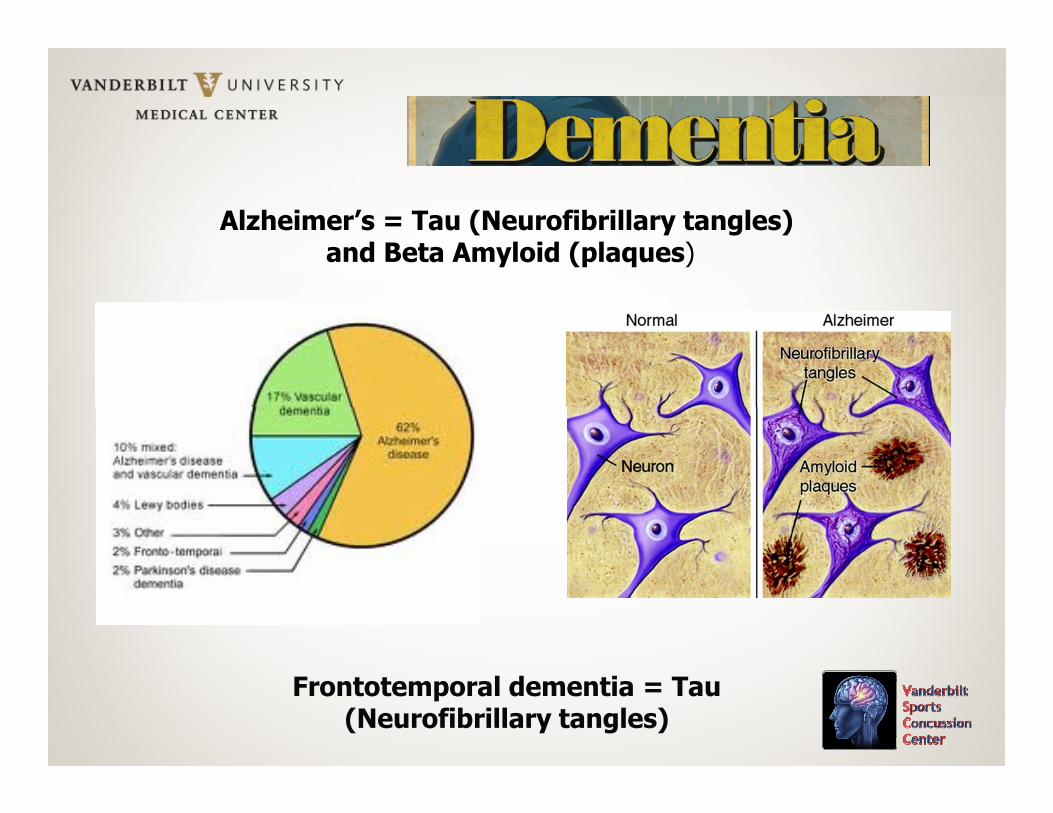
Alzheimer’s = Tau (Neurofibrillary tangles)and Beta Amyloid (plaques)
Frontotemporal dementia = Tau (Neurofibrillary tangles)
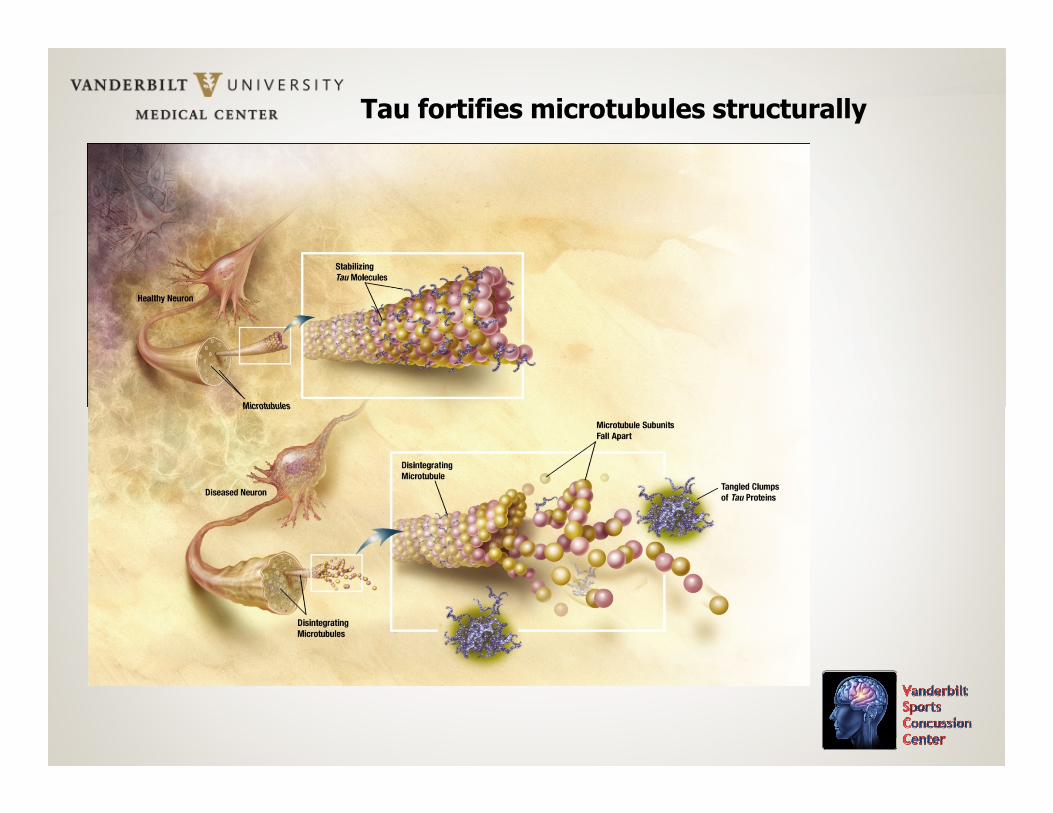
Tau fortifies microtubules structurally
Tau Protein (Tangles)
Chromosome 17
17 polymorphisms17 polymorphisms
Mutations lead to FTD and associated neurodegenerative diseases
Tau gene has 2 exon 6 polymorphisms (unrelated to AD): His 47 Tyr and Ser 53 Pro
Frontotemporal Dementia (FTD): Tau Protein
Several types and various names; taxonometric disagreement exists
Onset in late 50s and 60s; disturbances of speech, personality, mood, motivation, cognition (executive functions), social behavior
3 behavioral types: Disinhibition,3 behavioral types: Disinhibition,Executive Dysfunction, Apathy
PicksSemantic DementiaPrimary Progressive AphasiaCorticobasal DegenerationProgressive Supranuclear Palsy
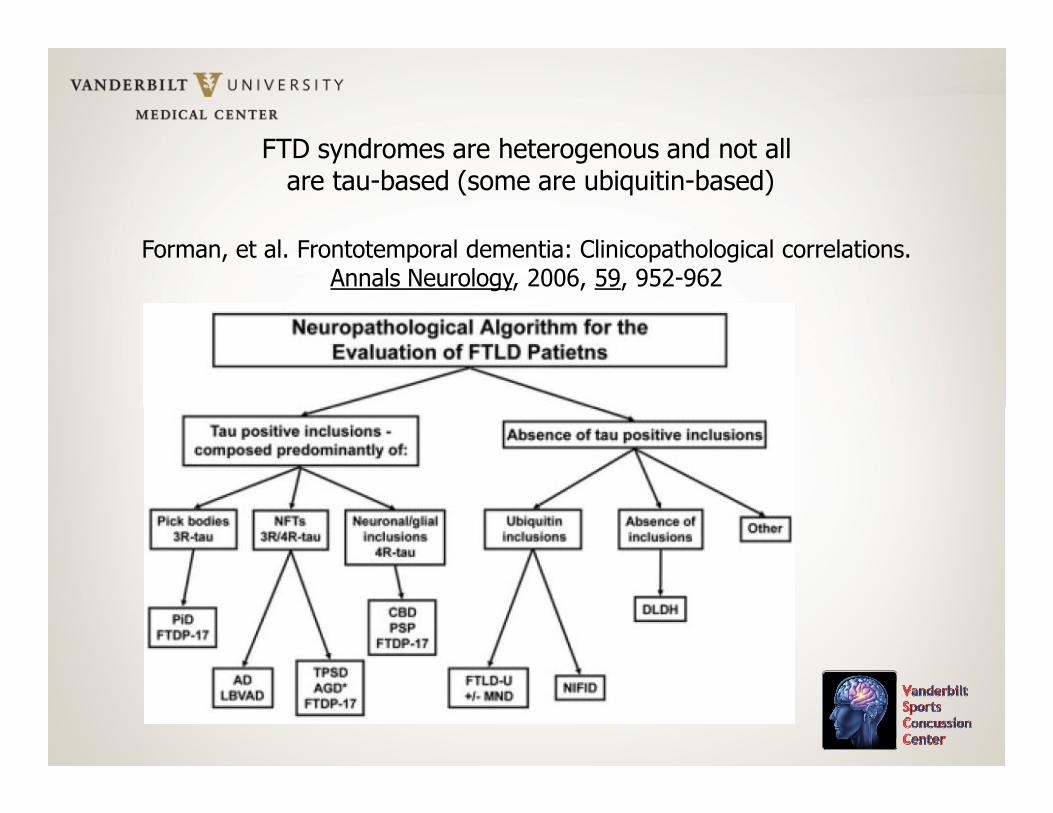
FTD syndromes are heterogenous and not allare tau-based (some are ubiquitin-based)
Forman, et al. Frontotemporal dementia: Clinicopathological correlations. Annals Neurology, 2006, 59, 952-962

5 Types FTD---Ubiquitin based
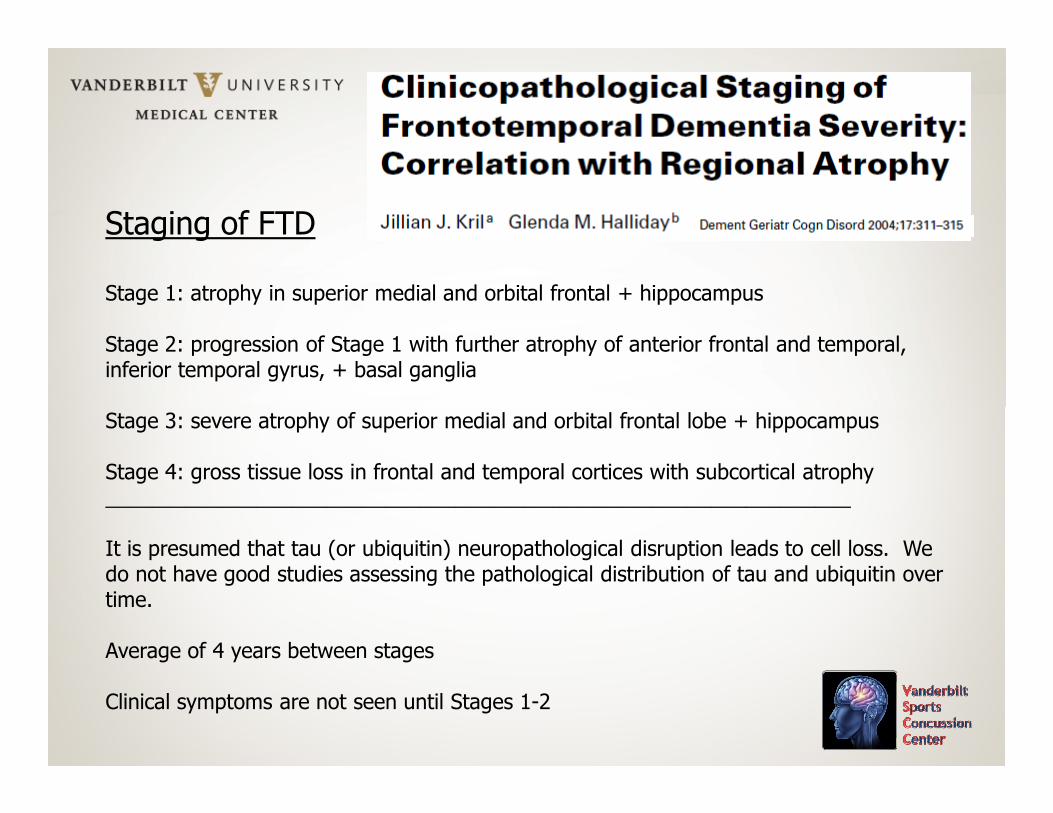
Staging of FTD
Stage 1: atrophy in superior medial and orbital frontal + hippocampus
Stage 2: progression of Stage 1 with further atrophy of anterior frontal and temporal, inferior temporal gyrus, + basal ganglia
Stage 3: severe atrophy of superior medial and orbital frontal lobe + hippocampus
Stage 4: gross tissue loss in frontal and temporal cortices with subcortical atrophy________________________________________________________________
It is presumed that tau (or ubiquitin) neuropathological disruption leads to cell loss. We do not have good studies assessing the pathological distribution of tau and ubiquitin over time.
Average of 4 years between stages
Clinical symptoms are not seen until Stages 1-2
Stages of Neuropathology in ADStages of Neuropathology in AD
Braak et al., European Archives of Psychiatry and Clinical Neurosciences,1999, 249, Supplement 3
Braak Stages I-X
With a focus on Neurofibrillary tangles (Tau)
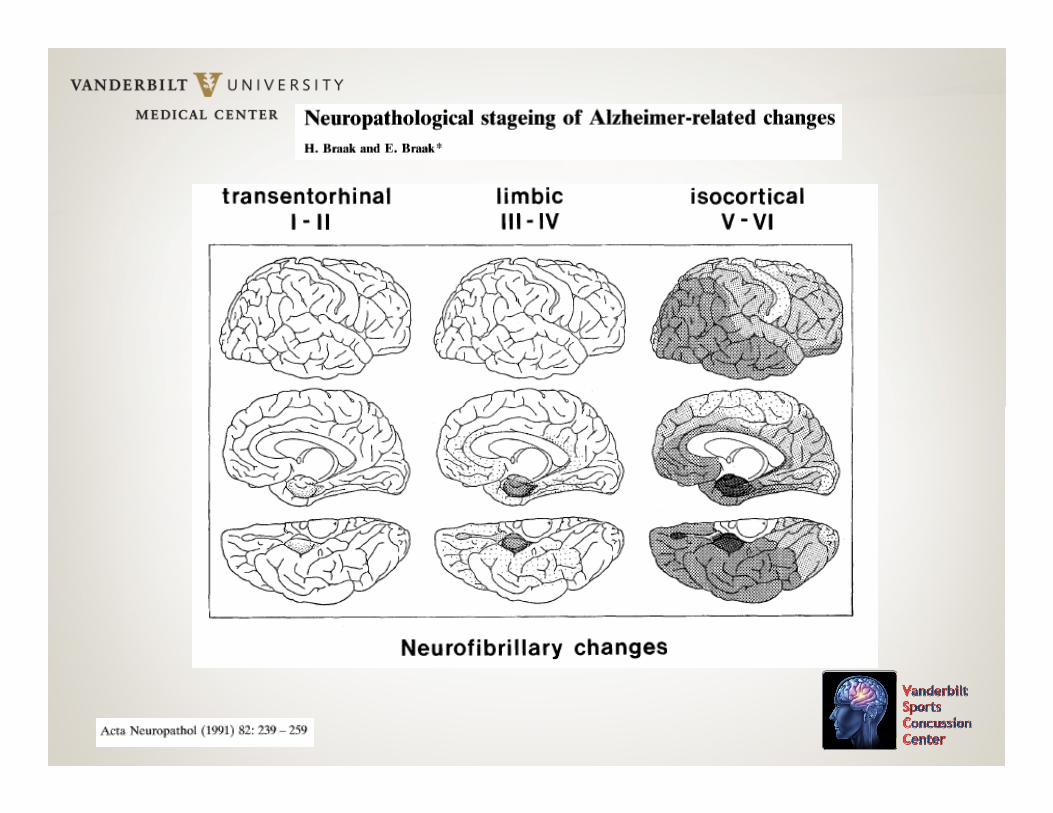
Transentorhinal I-IILimbic III-IV
Isocortical (Neocortical) V-VIAD is diagnosed clinically at Stages V-VIStages VII-X: Dementia is clearly evident
“The changes evolve according to a predictable sequence with little variation among individuals (Kemper 1978, 1984, Hyman et al. 1984, 1986, 1990, van Hoesen and Hyman 1990, van Hoesen et al. 1991). This sequence is highly reminiscent of the inverse pattern of cortical maturation and refinement during both phylogenesis and ontogenesis”. (p. 16).
“The lesions extend outward from the transentorhinal region, and gradually appear in the entorhinal region proper, the hippocampal formation, the amygdala, in higher order multimodal association areas of the neocortex, and eventually in the primary motor area and primary sensory fields. This sequence of encroachment is remarkably consistent across cases and exhibits little variation among patients. Through post mortem identification of the location of the damaged neurons and the severity of the pathology, six stages in the evolution of the neurofibrillary changes can be differentiated (Braak and Braak 1991, 1994, 1997, Samuel et al. 1996, Hansen and Samuel 1997, Hyman and Trojanowski 1997, Nagy et al. 1997,Hyman 1998). The initial NFT/NT stages develop preferentially in the absence of ß-amyloid deposits.” (p. 18).
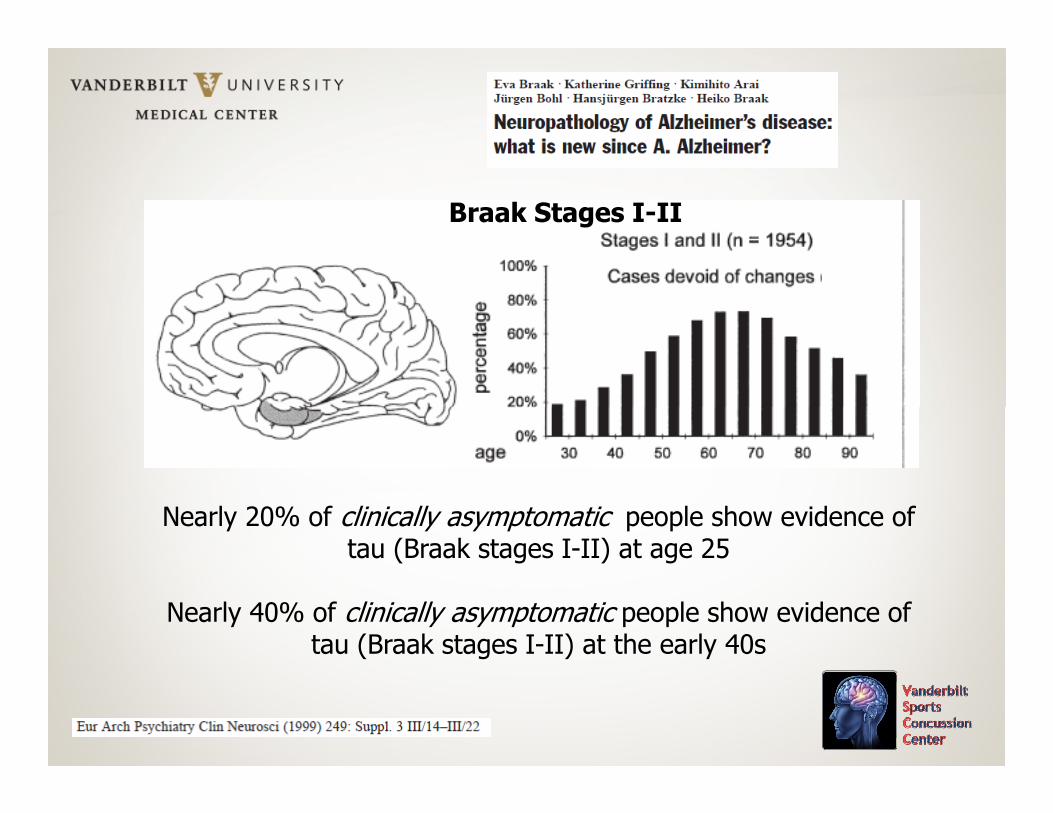
Braak Stages I-II
Nearly 20% of clinically asymptomatic people show evidence of tau (Braak stages I-II) at age 25
Nearly 40% of clinically asymptomatic people show evidence of tau (Braak stages I-II) at the early 40s
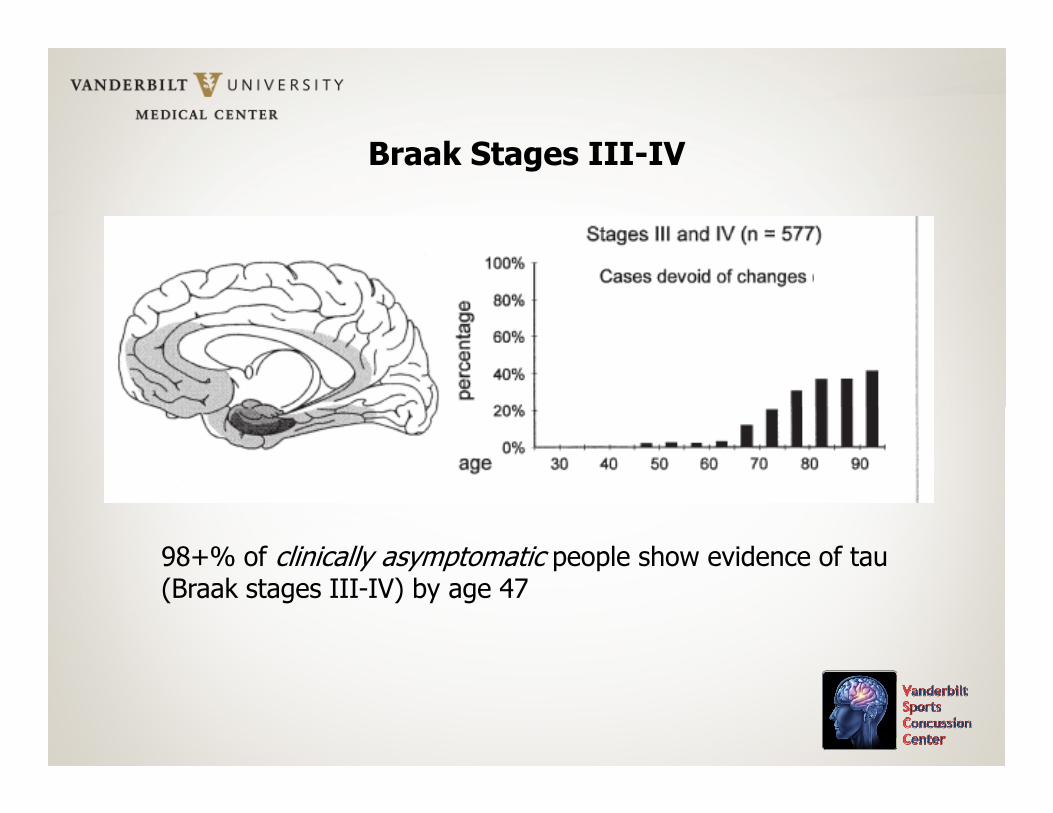
Braak Stages III-IV
98+% of clinically asymptomatic people show evidence of tau (Braak stages III-IV) by age 47
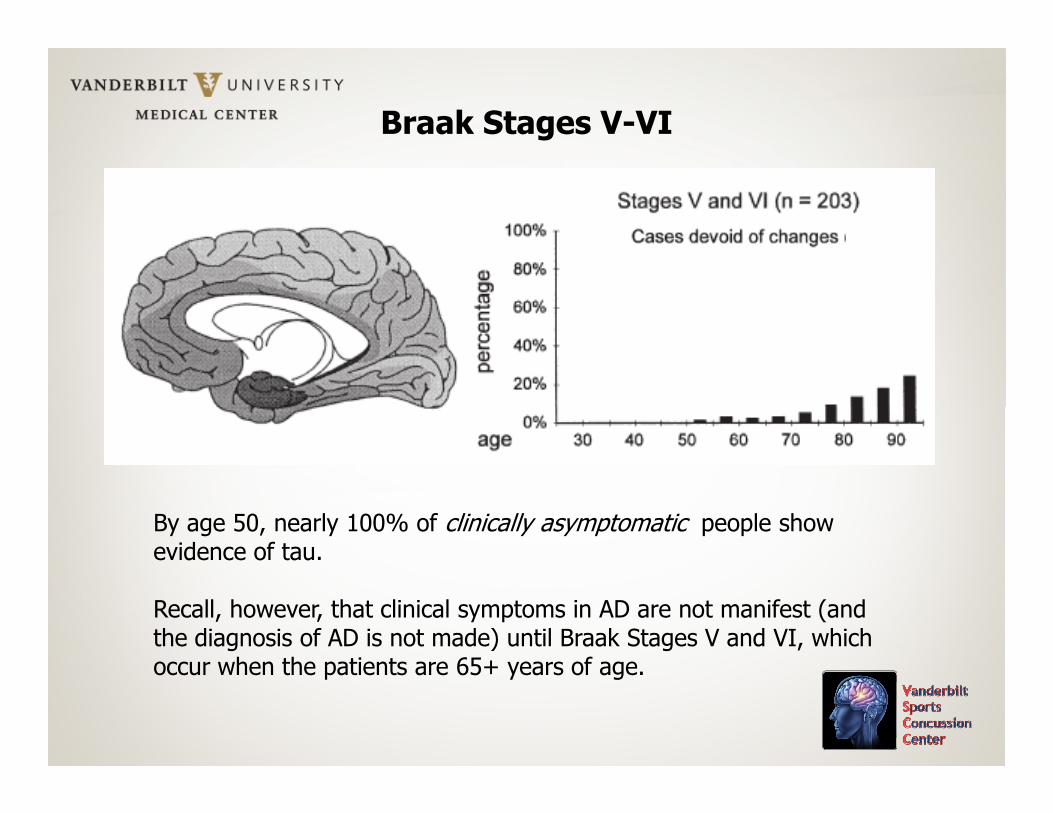
Braak Stages V-VI
By age 50, nearly 100% of clinically asymptomatic people show evidence of tau.
Recall, however, that clinical symptoms in AD are not manifest (and the diagnosis of AD is not made) until Braak Stages V and VI, which occur when the patients are 65+ years of age.
“Rather, a typical feature of this neurodegenerative disorder is that “Rather, a typical feature of this neurodegenerative disorder is that several decades elapse between the onset of histologically-verifiable
lesions and those phases of the illness in which the damage is extensive enough for clinical symptoms to become apparent.” (p. 19)
Amyloid-beta plaque growth in cognitively normal adults: Longitudinal PIB data
Vlassenko, Mintun, Xiong, et al. Annals of Neurology, 2011, in press
Amyloid-beta accumulation was evaluated with 2 PET scans approximately 2.5 years apart in 146 cognitively normal subjects (based on CDR scores) ages 45-86(based on CDR scores) ages 45-86
Marking PIB (C-Pittsburgh compound, an index of beta-amyloid burden)
17/21 with initially elevated amyloid-beta levels showed increased burden (estimated increase 8% per year)
10 converted from negative to positive amyloid-beta status
No subject reverted to a state of no amyloid-beta deposits

What are the implications of the Braak
and FTD staging data for CTE?
The findings of tau pathology in athletes ages 20+ years with reported CTE is not surprising. There is no doubt that significant head trauma can lead to tau (and beta amyloid) accumulation.can lead to tau (and beta amyloid) accumulation.
Here is what is puzzling in recent cases of reported CTE in professional athletes (non-boxers): Why do the cognitive and neurobehavioral changes occur so early (in the 20s-50s), whereas these changes and symptoms are not manifest in cases of tau-based FTD in non-athletes until the late 50-60s and in tau- (and amyloid-) based AD patients until after age 65+ years?
In other words, if tau is the sole culprit, why are the symptoms manifest so early in athletes and not until later in non-athlete patients? Are professional athletes’ brains that different biologically? Are they somehow particularly vulnerable to the biologically? Are they somehow particularly vulnerable to the effects of tau? Are we not accounting for the base rates of tau incidence in aging?
Whether the neurocognitive, mood, and behavioral changes are attributable solely to tau pathology is debatable, as such is clearly not the case early on in AD (prior to age 65+ years) or in FTD, despite the presence of abundant tau. In AD and FTD the tau is there for decades prior to the onset of symptoms.
The current thinking among someCTE clinicians and researchers seemsto be that the presence of postmortemtau is causal proof of the ante mortemcognitive, mood, and neurobehavioral changes seen in professional athletes.
It is not clear that the presence of tau causes these It is not clear that the presence of tau causes these aberrations. We have genetic and psychosocial data on <5 published cases. We know virtually nothing of these other athletes’ family (genetic) history and do not have all the facts related to premorbid psychiatric, substance abuse, and psychosocial data which could well be relevant in the final neurobehavioral (and etiologic) outcome. The base rates of tau occurrence must be taken into consideration.

Scientific Summary
• There has yet to be a conclusive scientific study showing that multiple mildconcussions leads to dementia of any type.
• Plassman et al. (“Documented head injury in early adulthood and risk of Alzheimer’s disease and other dementias”, Neurology, 2000, 55, 1158-1166) have shown that WWII veterans with a concussion involving loss of consciousness or PTA >30 minutes had a greater risk of developing Alzheimer’s or other dementia later in life (Odds Ratios = 2.16 - 2.46). The Alzheimer’s or other dementia later in life (Odds Ratios = 2.16 - 2.46). The presence of ApoE e4 suggested a trend for increased risk.
• The patients in the Plassman study with a mild concussion (more similar to what is seen in sport-related concussion) did not have a greater risk for developing dementia later in life.
• Keep in mind that the current data on non-boxing professional athletes is anecdotal, and that the professional athlete autopsy data are from a small sample.
• Working hypothesis: There may be a relationship between multiple concussions and late life dementia (CTE, AD, FTD, etc.)

Professor Henry MillerDepartment of NeurologyRoyal Victoria Infirmary, Newcastle upon Tyne
Meeting November 9, 1965Mental Sequele of Head Injury
Post-traumatic Dementia
It will be observed that these cases included none in which cerebral It will be observed that these cases included none in which cerebral trauma had been followed by progressive intellectual deterioration. This picture has been discussed by Corsellis & Brierley (1959) and is of considerable interest both intrinsically and medico-legally. The usual story is of a typical and insidiously progressive presenile dementiawith gross cerebral atrophy and histopathological changes analogous to those of Alzheimer's disease, beginning immediately after a headinjury. The interpretation of such a sequence of events is clearly problematical.
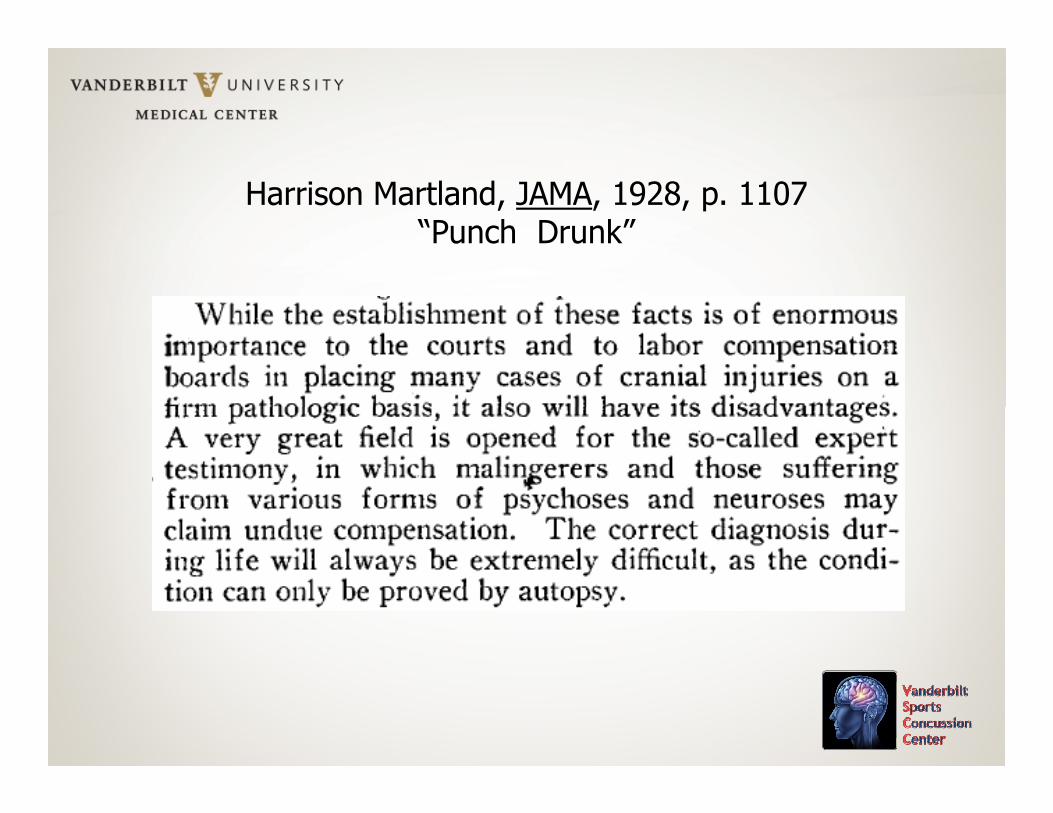
Harrison Martland, JAMA, 1928, p. 1107“Punch Drunk”
I have no doubt that CTE exists in some athletes
It has been proven empirically in professional boxers
My doubt at present is whether a tau protein-positive autopsied brain (of less than 10 professional football players) is causal proof of concussions leading to a CTE syndrome in American professional footballsyndrome in American professional football
There are alternative explanations for the clinical outcome in many of these tau-positive athletes
Let us address this scientifically and not in the popular press. Let us focus on the data, and not on the hype.

Thank you for your attention.
Questions?