Embed Size (px)
DESCRIPTION
Detail explanation of mechanism of action of Lithium as a mood stabiliser
Citation preview

Dr.Rachana Menon
PHARMACOTHERAPY OF MANIAPHARMACOTHERAPY OF MANIA

As we go along….
History Introduction to mood disordersDSM 4 criteria & subtypesPathogenesisPharmacology of antimanic drugsNewer approachesNon pharmacological treatmentsTreatment in special populationsTreatment of resistant mania

400 B.C- Hippocrates
30 A.D- Roman physician described melancholia-
Aretaeus of Cappadocia
1899-Emil Kraepelin
1949, John Cade
Works of Sigmund Freud



Mania & Hypomania– Distinct period of an abnormally and persistently elevated
expansive, or irritable mood lasting for at least 1 week, or less if a
patient must be hospitalized
Hypomanic episode
– At least 4 days
– Not sufficiently severe to cause impairment in social or
occupational functioning, and
– No psychotic features are present
Cyclothymia - one or more Hypomanic episodes Dysthymic (chronic depression) episodes


Euthymia
Mania
Depression
Euthymia
Mania
Depression


DSM-IV DIAGNOSIS OF MANIA
DSM-IV


Dopamine Hypothesis
Striatum, the nucleus accumbens,
olfactorytubercle.
Substantia nigra,
VTA , hypothalamus,
cortical areas
Hippocampus

Mesolimbic- mesocortical:
Control behavior, cognitive
funtion - D₂
Receptor.
Nigrostriatal: Control
Voluntary Movement
D₁ and D₂
receptor.
Tuberoinfundibular:
Control prolactin secretion
D₂ receptor.
Vesicular monoamine transporter protein (VMAT2)

CHOLINERGIC SYSTEM
Cholinergic monoaminergic interaction hypothesis
Complex interrelations of cholinergic and monoaminergic neurotransmitter
Play a role in the pathophysiology and treatment of affective disorders.
Hypocholinergic or hyperadrenergic drive would cause mania.
• By stimulation of muscarinic M4 receptors
• M4 receptors are found in high density in limbic and cortical, decrease
cAMP
Acetylcholineprecursors, such as lecithin (phosphotidylcholine) or choline in combination with lithium, have
been used to successfully treat manic patients.

Noradrenergic system
MHPGNE

GLUTAMATE HYPOTHESIS
• Major excitatory neurotransmitters in the CNS.
• Intergral for synaptic transmission in brain circuitry.
• Key regulator of synaptic strength and plasticity
• Bind to (NMDA) receptor, and an excess of
glutamatergic stimulation
• High concentration of NMDA receptors exists in the
hippocampus

Deleterious glutamate signaling

Second Messengers and Intracellular Cascades
Increase in Gs levels in frontal, temporal and occipital cortices of BD subjects.
Mononuclear leucocytes of manic patients Platelets
G PROTIENS Mood states

A significantincrease in the activity of basal and activated AC among maniacsubjects
Significant increase in PIP2 levels

The PKC signaling pathway
• Regulation of neuronal excitability
• neurotransmitter release
• long-term synaptic events
attenuation of PKC activity may play arole in the antimanic effects of mood stabilisers
Alter the conformation of the cytoskeleton throughactin filaments.

`Modulation of proteins associatedwith cytoskeleton microtubules- tau, MAP-1BMAP-2, Apoptosis
destabilization of microtubules conformation
NEURONAL SURVIVAL

CALCIUM-SIGNALING ABNORMALITIES
Abnormal Ca2+ homeostasis in bipolar disorder
• Elevated intracellular Ca2+ levels in platelets, lymphocytes and
neutrophils of patients with BD
Marked blunting of Gprotein-
activated PI hydrolysis
Altered mRNA expression of
proteins important roles in Ca2+
homeostasis
IMPase type2a,
TRPM2

ALTERATIONS OF HORMONAL REGULATIONS

Genetics…
• MZ concordance – 40 -45%• Heritability – 80 – 85%• Leading linked regions – 6q, 8q, 13q, 22q• Leading candidate genes
– BDNF– DAOA– DISC– TPH2– SLC6A$
• Genes implicated by GWAS – DGKH– CACNA1C– ANK3
Concordance in MZ
twins of 50-70%
Early-onset bipolar
disorder may be
even more genetic
Strongly
genetic

DRUG INDUCED MANIA• Levodopa• Corticosteroids • Tricyclic and monoamine oxidase inhibitor• Thyroxine • Isoniazid • Sympathomimetic drugs• Chloroquine, baclofen• Alprazolam• Captopril • Amphetamine • Phencyclidine.

CLASSIFICATION
Mood Stabiliser Anti epileptics Anti PsychoticsAnti Adrenergic
Drugs
Lithium Sodium valporate Olanzapine Clonidine
Carbamezapine Quatepine Propranalol
Lamotrigine Apriprazole
Gabapentin Zisaperidone
Toperamate Risperidone
Benzodiazepines Cholinomimetics Calcium Channel Blockers
Clonazepam Physostigmine Verapramil
Lorazepam Nifedipine
Nimodipine

LITHIUM
Introduction of Li+ in 1949
(Li+) is the lightest of the alkali metals
Monoamines implicated in the pathophysiology of
mood disorders
Second-messenger and other intracellular
molecular mechanisms involved in signal
transduction
Gene regulation and cell survival.

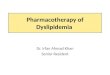
Lithium increase the SE inhibitory input to VTA and SNc nuclei

Lithium at conc of 1-10 mEq/L inhibits the Ca++-dependent release of NE and DA
BEFORE
AFTER

Influence G-protein function is by modulating the posttranslationalmodification of ADP-ribosylation of Gproteins

INOSITOL MONOPHOSPHATE
Interference with PIP2 PATHWAY
Activated PLC

phosphorylation
HIPPOCAMPUSAXONAL GROWTH

Enhances the bindingof tau to microtubules which promotes microtubuleassembly
DEPHOSPHORYLATION

Decrease gene expression of PLA2

AP-1, AMI-1, PEBP-2
Bcl-2

PHARMACOKINETICS
Completely absorbed in GIT within 6–8 hours; peak plasma levels in
30 minutes to 2 hours
• Distribution: Initial volume of distribution is 0.5 L/kg, rising to 0.7–
0.9 L/kg; some sequestration in bone. No protein binding.
• Excretion: virtually entirely in urine. Lithium clearance about 20% of
creatinine. Plasma half-life about 20 hours
• Target plasma concentration: 0.6–1.4 mEq/L
• Dosage: 0.5 mEq/kg/d in divided doses
Carbonate capsules slow release tablets citrate syrup (8 mmol/
5 mL)

ThaizidesSpironolactone Amiloride FurosemideIndomethacinIbuprofen NaproxenCOX-2 inhibitorsFosinopril Lisinopril

SERUM LEVEL MONITORING
• Acceptably safe are between 0.6 and 1.5 mEq/L.
• 1.0-1.5 mEq/L- acutely manic or hypomanic patients.
• 0.6-1.0 mEq/L long-term prophylaxis.
• 0.8-1.0 mEq/L experience decreased relapse risk
• Trough from samples obtained 10-12 hours after the last
oral dose of the day.
• Trough concentration:0.8-1mEq/l Individualization of serum levels is often necessary to obtain a favorable risk-benefit relationship

•Acute poisoning - Voluntary or accidental ingestion in a previously untreated patient
•Acute-on-chronic - Voluntary or accidental ingestion in a patient currently using lithium
•Chronic or therapeutic poisoning - Progressive lithium toxicity, generally in a patient on lithium therapy

Acute Toxicity and Overdose
• Nausea, vomiting, abdominal pain, profuse diarrhea
• Polyuria,Coarse tremor
• Ataxia, coma, and convulsions
• Mental confusion, hyperreflexia, gross tremor, dysarthria, seizures,
and cranial nerve and focal neurological signs
• Coma and death.
• Cognitive and motor neurological damage irreversible, with
persistent cerebellar tremor being the most common

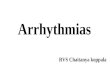
SERUM PLASMA LEVELS
Mmol/L Effects
0.5 None
1 Mild tremor
1.5 Coarse tremor
2 Hyperreflexia, dysarthria
2.5 Myoclonia, ataxia, confusion
> 3.0 Delirium, coma, seizures

LITHIUM TOXICITY

Role of sodium polystyrene sulfonate (Kayexalate)
•Admit patients with serum lithium levels higher than 2 mEq/L.•Admit to an ICU patients with chronically elevated lithium levels higher than 4 mEq/L
NO ANTIDOTE
HEMODIALYSIS

Adverse effects Polyuria and compensatory polydipsia
Benign, diffuse, non tender thyroditis
Benign and reversible T-wave flattening in ~20% of
patients , U wave enlargement
Sinus bradycardia, AV blocks
Dermatitis, folliculitis, and vasculitis can occur with Li+
administration
Ebstein's malformation
Floppy baby syndrome
Polymorphonuclear leukocytes

Therapeutic uses
Acute mania- 600-mg loading dose (150,300,600mg)
Prophylactic treatment of bipolar disease
Treatment-resistant major depression
Monotherapy for unipolar depression
Suicide reduction extends to unipolar mood disorder
Alzheimer type, stroke, Parkinson's disease,
Huntington's disease, amyotrophic lateral
sclerosis, progressive supranuclear palsy,
spinocerebellar ataxia

ANTIEPILEPTICS
CARBAMEZAPINE SODIUM VALPROATE LAMOTRIGINE TOPIRAMATE GABAPENTIN

CARBAMAZEPINE• Iminostilbene derivative with a tricyclic structure
• Mechanism of action
Inositol depletion as a mechanism underlying carbamazepine's mood
stabilizing properties (Williams et al., 2002).

Pharmacokinetics
• Absorbed slowly and erratically after oral administration
• 75% to 90% is protein bound
• Undergoes extensive hepatic metabolism predominantly by conversion to a
10,11-epoxide
• Substrate and inducer of CYP3A4
• Induces CYP2C, CYP3A, and UGT, thus enhancing the metabolism of drugs
degraded by these enzymes
• Half life – 20 to 40hrs
• Therapeutic plasma concentrations 6 to 12 µg/mL
Anticonvulsants ,Hormonal contraceptives NeurolepticsErythromycin,Cimetidine,Isoniazid,Fluoxetine

Therapeutic uses
• Acute bipolar mania- 400-1400mg/day
• Maintenance therapy- 4-12 ug/ml drawn at 12 hrs
after last dose, minimum of 5 days after last dose
change
• Partial seizures
• Generalized tonic-clonic seizures
• Absence seizures
• Trigeminal neuralgia.

Acute mania
400 mg/day- larger dose given at bedtime due to the
sedating properties
Titration proceeds by 200-mg increments every 24-48
hours based on clinical response and serum trough
levels
Extended-release form – FDA 2005
Better tolerated compared to older preparations
Effective as monotherapy with once-daily dosing
Immediate release forms of carbamazepine cannot be loaded

Adverse effects Nausea, vomiting, diarrhoea and visual
disturbances Hypersensitivity – rash, photosensitivity,
hepatitis, granulocyte suppression and aplastic anemia
Lyell’s syndrome,Stevens-Johnson
ADH action enhancement – hyponatremia and water retention
Teratogenicity Transient elevation of hepatic
transaminases Aplastic anemia,Agranulocytosis
CBZ level, CBC + differential,reticulocyte countSGPT every 3 months till stable.

Oxcarbazepine 10-keto analogue of carbamazepine.
Metabolite: MHD- 10-monohydroxy derivative Half-life 8-10 h
Therapeutic use: 600 -1200 mg/day.Augmented to 1400 to 2400 mg/day in order to obtain the desired effect
DRUG INTERACTION: reduces the plasmatic levels of felodipine, verapamil,OCPS
Substitution of oxcarbazepine for carbamazepine is associated with increased levels of phenytoin and
valproic acid

Sodium valproate
• Simple branched-chain carboxylic acid

Mechanism of action
Inhibit the activity of glycogen synthase kinase-3 –ALTER
MARCK protiens
INHIBIT MYO-INOSITOL PHOSPHATASE
Reduction in arachidonic acid turnover in brain membrane
phospholipids
Interact with nuclear regulatory factors that affect gene
expression AP-1, AMI-1, PEBP-2
Increase expression of Bcl-2, which is associated with
protection against neuronal degeneration/apoptosis
Reduce isofoms of PKC
6 MECHANISMS IN COMMON!

PHARMACOKINETICS
Completely absorbed after oral administration t ½ : 14 hoursplasma proteins bound ~90%
Metabolism: beta-oxidation and UGT enzymes
Metabolites: VA Glucuronide (40% of VA) Urinary excretion3 oxo VA (33% of VA) Urinary excretion2 ene VA
Delayed but significant accumulation in brain
< 5% excreted unchanged in urine
CYP2C9 CYP2C19

Increases the serum levels of SVP
Phenytoin Phenobarbitone : 70%Lamotrigine : > 2.5 times of T ½ CBZ Metabolite increasedDPH Others:
Rufinamide, Lorazepam, Felbamate, TCAs, Zidovudine, Nimodipine

DRUGS ↓ Serum SVP
CBZ + DPH (Combined) ↓ SVP by 50% (Reduction is more in children)
Lamotrigine ↓ SVP by 25%
Estrogen (OCP) ↓ SVPOthers ↓ SVP
Meropenem, Imepenam, Rifampicin, Ritonavir

Therapeutic uses
• Acute mania
• Oral loading of VPA can achieve rapid control of symptoms- 3 days
• Day 1: single dose of 20 mg/kg
• Days 2-4 :same dose but split bid
• Day 4 : labs (VPA level, platelets, LFTs) then titrate dose to get level > 80
ug/ml or best clinical response.
• Some patients need > 100ug/ml.
Cyclothymia:DOC
Effective at surprisingly low doses,125-500 mg/day.
Maintenanace: Superior to lithium in preventing recurrence of episode.
Immediate Release-12-hour troughs are used to guide treatment
Extended Release- 24-hour trough levels
Divalproex sodium
90-120 g/mL

• Weight gain,GI distress
• Tremor, Ataxia
• Dizziness, sedation, headache, nausea, dyspepsia
• Hair loss- curly scalp hair .
• Severe hepatic damage can occur within the first six months of
treatment
• LFT TO BE MONITERED- fulminanat hepatits!!!!
• Acute pancreatitis,PCOD –RARE
SIDE EFFECTS

LAMOTROGINE
• A phenyltriazine derivative

PHARMACOKINETICS Half-life -25-35 hrs
Metabolized primarily by glucuro nidation to an inactive
2-N-glucuronide conjugate.
Renal excretion
Protein binding ~55%
The kinetics linear at steady-state within a dose range of
100 to 700 mg/day
chewable dispersable formulations
Phenytoin, CBZ, phenobarbital reduces
the t1/2 and plasma concentrations of
lamotrigine

THERPEUTIC USES• Maintenance therapeutic range: not established
75-250 mg/day (with CBZ 300-500mg/day; with VPA 50-150 mg/day
LTG monotherapy: 25 mg/day week 1
50 mg/day week 2
up to target dose of 150-200 mg/day
12.5 mg/day week 1
25 mg/day week 2
target dose of 75-100mg/day
50 mg/day wks 1-2
100 mg/day weeks 3-4wks
target dose of 300 mg/day
In combination with VPA
In combination with CBZ

50-100 mg/day
Treatment-resistant depression- 100 mg/day to 20 mg/day of
fluoxetine
• Bipolar I depression- 200mg/day (Maintenanace)
• Rapid cycling- 100 to 500 mg per day.
Fixed lithium dose (800 mg/day)
Adverse effectsDizziness, ataxia, blurred or double vision, nausea, vomiting
Stevens-Johnson syndrome and DIC

GABAPENTINE
• Consist of a GABA molecule covalently bound to a lipophilic
cyclohexane ring or isobutane.
• Centrally active GABA agonist,
• High lipid solubility
• Transfer across the blood-brain barrier.• Blocking of voltage-dependent calcium channels
Its use in bipolar disorder is based on clinical impressions of efficacy, usually as an adjunctive agent; it has not at this point been adequately
established as a primary mood stabilizer!!!!

Pharmacokinetics• Orally absorbed.Half-life: 5-7 hrs.
• Metabolism: none
• Excreted unchanged in urine
• Maintenance therapeutic range: N/A
• Dosage: 300-3600 mg/day. Dosage range is variable; when
given as an adjunct mood stabilizer
• “You must split the dose when getting into higher dosage
ranges.”
• Drug interactions: none
split dosing may be necessary for good response

Adverse Effects• Sedation • Fatigue, ataxia• Ejaculatory problems
• Caution!!!!: sudden discontinuation in patients with OCD

TopiramateSulfamate-substituted monosaccharide
Rapidly absorbed after oral administration
(10-20%) binding to plasma proteins
Mainly excreted unchanged in the urine.
Metabolism by hydroxylation, hydrolysis, and
glucuronidation with no single metabolite
t1/2 is ~24 hrs
Further double-blind studies to elucidate the antimanic and
mood stabilizing effects of topiramate are warranted.

Adverse Effects• Sedation, dizziness, anxiety, tremor, confusion• tingling in fingers, toes• GI distress,• Cognitive impairment, • Weight loss!!!• Teratogenicity,• Renal calculi!!!!
• Therapeutic use• Acute mania 100-200 mg/day, perhaps higher (for
seizure disorder 400mg/day is recommended)
400mg/day
Decrease serum levels of CBZ, VPA, digoxin, OCPs

ANTIPSYCHOTICS

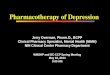
Dopamine Synapse
DA
L-DOPA
Tyrosine
Tyrosine
D2
Dopaminereceptorantagonist



HIT AND RUN!!!!
Fills D2 receptors,preventing blockade by the antipsychoticagent.


10-15mg
25mg bd
5mg
20mg bd
Prophylaxis
Prophylaxis

2009
5-HT1A,5-HT1B, 5-HT2A, 5-HT2B, 5-HT2C, and 5-HT5–7 ,

Adverse effects

Benzodiazepines Lorazepam and Clonazepam
Useful adjuncts with mood stabilizers in the treatment of acute mania
• Lorazepam- 2 to 4 mg per day, three to four divided doses. Titrated up to a target dose ranging from 3 to 8 mg per day
• Clonazepam 1 - 3 mg per day, two divided doses.
• 2 to 6 mg per day, depending upon efficacy and tolerabity
• high as 24 mg per day
• Promote sleep improvement
Sedation, and respiratory depression
Hypomanic Mild to moderate manic or mixed episodes Cannot tolerate lithium

Calcium channel blockers
Nimodipine may be more effective than Verapramil
• Special promise for rapid and ultrarapid cycling patients
Verapamil and nimodipine • Controlled symptoms of mania in PREGNANCY • VERAPRAMIL- 160-320mg/day• Low teratogenecity

Treatment resistant mania• Clozapine + ECT
• Donepezil
• Gabapentin, topiramate, mexiletine,
• IV magnesium sulphate

Pediatric Use• ONLY Li+ has FDA approval for child/adolescent bipolar
disorder for ages 12 years.
Aripiprazole and risperidone 10-17yrs
Geriatric Use
• Targeting lower maintenance serum levels (0.6-0.8 mEq/L) may
reduce the risk of toxicity.
• As GFR> 60 mL/min - alternative agents, despite lithium's
therapeutic advantages
• Use of loop diuretics and angiotensin-converting enzyme inhibitors
.
30 mg/kg/day given in three divided doses will produce a Li+
concentration of 0.6-1.2 mEq/L in 5 days

PREGNANCY
Lithium- Category D
• First trimester - Ebstein’s Anomaly
• 1: 10-20,000 to 1: 1000. foetal echo is warranted, Floppy baby
syndrome
• Maternal polyuria
Valproate: Category D
Neural tube defects, limb defects, cardiac defects and facial
dysmorphism
.

Lamotrigine & Carbamazepine: Category D
Absolute risk of birth defects (~ 5-6%). n oral cleft
defect
Atypical Antipsychotic Medications
Weight gain throughout the pregnancy
• Risk of gestational diabetes. RISK-BENEFIT RATIO!!!

Novel stratergies and novel therapies
• Prophylaxis• Decreasing the episode severity• Increasing the inter-episode interva
Non-competitive, high-affinity NMDA receptor antagonist Memantine
• Demonstrated potential to relieve “manic-like” symptoms in animal models; appeared beneficial in two open-label studies
• Allopurinol • Hypothesized to be involved in the pathophysiology of mania. • An adjunct to mood stabilizer or antipsychotic
GOAL
Glutamatergic modulators

TAMOXIFEN
• Protein kinase C (PKC) inhibitor
• Antiestrogenic drug
• Crosses the blood-brain barrier and is relatively well
tolerated (up to 200 mg/d)
• starting dosage 20 mg twice daily (40 mg/d).
• Subsequently increased by 10 mg to achieve 80 mg/d in
twice-daily divided doses.
• long-term safety data are limited
• increased risk of endometrial carcinoma and uterine
sarcoma
. The Canada Network for Mood and Anxiety Treatment (CANMAT) lists it as
a third-line option
Young Mania Rating Scale (YMRS).

The GlyT1 inhibitor SSR504734
Effective as haloperidol in blocking PCP-induced CNS metabolic changes in rats.
Lurasidone - 5-HT/DA antagonist- FDA approval 2009
Possesses potent activity at 5-HT7 receptor sites, actions that, based on preclinical and early clinical studies, may be associated with cognitive benefits
Xanomeline, M1/M4 agonist, has shown antipsychotic and procognitive affects .schezo trial

Brain StimulationNon-invasive method• transcranial magnetic stimulation • transcranial direct current stimulation
Invasive method• Deep brain stimulation (DBS) that targets brain areas via
implanted electrodes• Stimulation could elicit circuit-level modifications that can
improve symptoms

ECT
• A prolonged or severe episode of mania • Severe depressive illness or refractory depression.• Catatonia.
• Should stop once a response is achieved or if the patient
develops side-effects.

THANK YOU