PHARMACOTHERAPY DIABETES MELLITUS
PHARMACOTHERAPYofDIABETES MELLITUSdr. Ave Olivia Rahman,
MSc.Bagian Farmakologi FKIK UNJADIABETES MELLITUS (DM)TYPE 1 TYPE 2
Insulin-dependent Diabetes Mellitus Destruction of
insulin-producing B cells in the pancreas. Non-insulin-dependent
diabetesRelative insulin deficiency, Insulin resistance.
GOAL OF THERAPYBLOOD SUGAR CONTROL AT NORMAL OR NEAR-NORMAL
VALUE DIET, EXERCISE, DRUGTREAT ASSOCIAETED CONDITIONS &
COMPLICATION RISK CONTROLPHARMACOTHERAPY OF DM TYPE 1 INSULIN
REPLACEMENT4 INSULIN ACTION
In healthy subjects, the amount of insulin is automatically
matched to blood glucose concentration.1. Under fasting conditions,
the pancreas SECRETES about 40 g (1 unit) of insulin per hour into
the portal vein toachieve a concentration of insulin in portal
blood of 2 to 4 ng/ml (50 to 100 units/ml) and in the peripheral
circulation of 0.5 ng/ml (12 units/ml) or about 0.1 nM. After
ingestion of a meal, there is a rapid rise in the concentration of
insulin in portal blood, followed by a parallel but smaller rise in
the peripheral circulation.2. The HALF-LIFE of insulin in plasma is
about 5 to 6 minutes in normal subjects and patients with
uncomplicateddiabetes. This value may be increased in diabetics who
develop anti-insulin antibodies. The half-life of proinsulinis
longer than that of insulin (about 17 minutes).3. DEGRADATION of
insulin occurs primarily in liver, kidney, and muscle (Duckworth,
1988). About 50% of the insulin that reaches the liver via the
portal vein is destroyed and never reaches the general circulation.
Insulin is filtered by the renal glomeruli and is reabsorbed by the
tubules, which also degrade it. Peripheral tissues such as fat also
inactivate insulin, but this is of less significance
quantitatively.4. Glucose enters cells by facilitated diffusion
through one of a family of glucose transporters (GLUT1 through
GLUT5) are thought to be involved in Na+-independent facilitated
diffusion of glucose into cells. This effect is reversible; the
transporters return to the intracellular pool on removal of
insulin.5. insulin inhibits the transcription of
phosphoenolpyruvate carboxykinase, contributing to insulins
inhibition of gluconeogenesis; this effect of insulin may explain
why the liver overproduces glucose in the insulin resistantstate
that is characteristic of type 2 DM.5Continue...Insulin
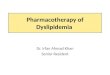
ActionStimulates glikogenesisInhibits gluconeogenesis.Inhibits
lipolysisStimulates fatty acid synthesis
1. Insulin STIMULATES glucose storage in the liver as glycogen
and in adipose tissue as triglycerides and amino acid storage in
muscle as protein; it also promotes utilization of glucose in
muscle for energy. These pathways, which also are enhanced by
feeding, are indicated by the solid blue arrows. 2. Insulin
INHIBITS the breakdown of triglycerides, glycogen, and protein and
the conversion of amino acids to glucose (gluconeogenesis), as
indicated by the white arrows. These pathways are increased during
fasting and in diabetic states.3. insulin inhibits lipolysis,
stimulates fatty acid synthesis (thereby increasing the
concentration of malonyl CoA, Inhibiting enzyme acylcarnitine
transferase, an enzyme involve in oxidation of free fatty acids),
and decreases the hepatic concentration of carnitine; these factors
all decrease the production of ketone bodies. 4. Conversely,
glucagon stimulates ketone body production by increasing fatty acid
oxidation and decreasing concentrations of malonyl CoA.5. Insulin
enhances the transcription of lipoprotein lipase in the capillary
endothelium. This enzyme hydrolyzes triglycerides present in VLDL
and chylomicrons, resulting in release of IDL. The IDL particles
are convertedby the liver to the more cholesterol-rich low-density
lipoproteins (LDL). Thus, in the untreated or undertreateddiabetic
patient, hypertriglyceridemia and hypercholesterolemia often occur,
also increased production ofVLDL.6. The important role of insulin
in protein metabolism usually is evident clinically only in
diabetic patients with persistently poor control of their disease.
In poorly controlled diabetics, there is increased conversion of
alanine (precussor of gluconeogenesis) to glucose, contributing to
the enhanced rate of gluconeogenesis. The increased conversion of
amino acids to glucose also results in increased production and
excretion of urea and ammonia. Increased proteolysis, decreased
protein synthesis.7.Covalent reaction of glucose with hemoglobin
Hemoglobin undergoes glycosylation on its aminoterminal valine
residue to form the glucosyl valine adduct of hemoglobin, termed
hemoglobin A1c. The amount of glycosylated protein formed is
proportional to the glucose concentration and the time of exposure
of the protein to glucose.
6Insulin Replacement
Subcutaneous administration Absorption is usually most rapid
from the abdominal wall, followed by the arm, buttock, and
thighDifferent type of insulin according to their duration of
action7Type of Insulin...based on its actingType Onset Peak
Duration Ultra rapid- acting15-30 minutes30 minute-2
hoursShort-acting/Regular30 minutes-1 hours2-4 hours6-8
hoursIntermediate-acting2-4 hours1-8 hours14-15 hoursLong-acting1-3
hoursWitout peak24 hours insulin replacement consists of prandial
(bolus) insulin, basal insulin, and a correction-dose insulin
supplement. 2. Prandial insulin is given in an attempt to mimic the
response of endogenous insulin to food intake. Normally, this
response occurs in a robust first-phase secretion and then a more
prolonged second-phase release into the portal circulation. A
subcutaneous injection of insulin will never precisely replicate
the second-phase release. (reguler/short acting, rapid acting)The
basal-insulin component mimics the relatively small but constant
release of insulin that regulates lipolysis and the output of
hepatic glucose. (intermediate and long acting)correction-dose
insulin addresses premeal or between-meal hyperglycemia,
independently of the prandial insulin.
8Continue...NPH: neutral protamine Hagedorn.Long acting insulin
is often given at bidetime to help normalize fasting blood glucose.
The use of long acting basal insulin alone will not control
postprandial glucose elevation.9
Insulin BasalInsulin PostprandialFactors Affecting Insulin
AbsorptionSite of injectionType of insulinSubcutaneous blood
flowSmokingRegional muscular activity at the side of
injectionVolume& concentration of injected insulinDepth of
injection.Indication of Insulin TherapyDM type 1DM type 2
uncontrolled with diet, excersice, oral antidiabetic
drugsGestational DMDM with severe kidney and liver diseaseDM with
infection, major operation, malnutrition, tumor, corticosteroid
therapy, graves diseaseDM Ketoacidosis
Insulin DosingInsulin replacement therapy includes long acting
insulin (basal) and short acting insulin to provide postprandial
needs. IHT (Insulin Harian Total) = 0,5 U x BB (kg) IPT (Insulin
Prandial Total) = 60% dari IHT dibagi 3 dosis (sarapan, makan
siang, makan malam)IBT (Insulin Basal Total) = 40% dari IHTORAL
HYPOGLICEMIC AGENTSBIGUANIDE INSULIN SECRETAGOGUES:SULFONYLUREASNON
SULFONYLUREAS (MEGLITINIDE): REPAGLINIDE,
NATEGLINIDETHIAZOLIDINEDIONESGLP-1 AGONIST : EXENATIDEDIPEPTIDYL
PEPTIDASE 4 INHIBITORS : SAXAGLIPTIN, SITAGLIPTIN, VIDAGLIPTINALPHA
GLUCOSIDASE INHIBITORSPRAMLINTIDE
BIGUANIDESMetformin. 1st line therapy in DM type 2.Metformin is
antihyperglycemic by decreasing hepatic glucose production
(gluconeogenesis) and by increasing insulin action in muscle and
fat. Only Metformin has been demonstrated to reduce macrovascular
events in type 2 DM (U.K. Prospective Diabetes Study Group,
1998b).Limited use of buformin, phenformin (withdrawn in 1970s).2.
Metformin has no significant effects on the secretion of glucagon,
cortisol, growth hormone, or somatostatin.3. AMPK activators fatty
acidoxidation, glucose uptake, nonoxidative metabolism, reduce
lipogenesis and
gluconeogenesis.15Continue...MetforminCONTRAINDICATION : renal
impairement, hepatic disease, history of lactic acidosis, cardiac
failure, cronic hypoxic lung disease.SIDE EFFECTS: lactic acidosis,
diarrhea, abdominal discomfort, nausea, metallic taste,
anorexia.Metformin can be administered in combination with
sulfonylureas, thiazolizinediones, and/or insulin.Available
Fixed-dose combinations.
1. Metformin should be discontinued temporarily prior to the
administration of intravenous contrast media and prior to any
surgical procedure (should not be readministered any sooner than 48
hours after such procedures, until renal function is determinedto
be normal). 2. Intestinal absorption of vitamin B12 and folate
often is decreased during chronic metformin therapy, and calcium
supplements reverse the effect of metformin on vitamin B12
absorption.3. Metformin does not promote weight gain and can reduce
plasma triglycerides by 15% to 20%.16Dosing of Metformin Available
generic Tablet 500 mg, forte 850 mg. Dose : 2-3 x 500 mg daily with
meals, max 2,5 g/daily. 1. Some merk : also available in forte
tablet 850 mg(2x daily)17SULFONYLUREASGroup 2 more potent.K ATP
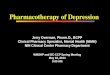
channel modulator18SULFONYLUREAS : Stimulating insulin release from
pancreatic cellsSULFONYLUREAS
1. Sulfonylureas also may further increase insulin levels by
reducing hepatic clearance of the hormone. 2. stimulate release of
somatostatin, and they may suppress the secretion of glucagon
slightly.3. During chronic treatment is attributed to
down-regulation of cell surface receptors for sulfonylureas on the
pancreatic cell. If chronic sulfonylurea therapy is discontinued,
pancreatic -cell response to acute administration of the drug is
restored.4. Sulfonylureas bind to the SUR1 subunits and block the
ATP-sensitive K+ channel Reduced K+ conductance membrane
depolarization and influx of Ca2+ through voltage-sensitive
Ca2+channels.19INCREASED INSULIN SECRETION
20SIDE EFFECT : mild- severa hipoglycemia, (glibenclamide cause
up to 20-30%), nausea, vomiting, cholestatic jaundice,
agranulocytosis, aplastic and hemolytic anemias, hypersensitivity
reactions, hyponatremia. DRUG INTERACTION : other sulfonamides,
clofibrate, and salicylates, ethanol.CONTRAINDICATIONS : type 1 DM,
pregnancy,lactation, significant hepatic or renal insufficiency for
the older preparationsThis glucosedependent inhibition of insulin
secretion during hypoglycemia occurs with glimepiride but not with
glyburide. Additionally, the major anti-insulin counter-regulatory
hormone glucagon appears to be reduced by glyburide during
hypoglycemia but is preserved during glimepiride therapy.2. Also
may induce hyponatremia (especially chlorpropamide) by potentiating
the effects of antidiuretic hormone on the renal collecting
duct.
21Repaglinide Stimulates insulin release by closing
ATP-dependent potassium channels in pancreatic cells. Side effects
: hypoglicemicemia.Initial dose 0,5 mg every timt before meals. Max
dose 16 mg/day
1. allow for multiple preprandial. 22NateglinideStimulates
insulin secretion by blocking ATP-sensitive potassium channels in
pancreatic cells.Dose of 3x 120 mg, 1 to 10 minutes before a meal.
Side effects : hypoglicemia (more rare)1. Nateglinide promotes a
more rapidbut less sustained secretion of insulin than do
otheravailable oral antidiabetic
agents23ThiazolidinedionesTroglitazone (withdrawn because causing
severe hepatic toxicity), Rosiglitazone, and Pioglitazone. Can be
combined with insulin or other classes. Side effects :
hepatotoxicity, anemia, weight gain, edema, and plasma volume
expansionPioglitazone Dose : 1x 15-30 mg/day.
24Mechanism of action Thiazolidinediones are selective agonists
for nuclear peroxisome proliferatoractivated receptor- (PPAR)
activates insulin-responsive genes that regulate carbohydrate and
lipid metabolism.Increasing insulin sensitivity in peripheral
tissue, lowering glucose production by the liver, increasing
glucose transport into muscle and adipose tissue
Increase glucose transport into muscle and adipose tissue by
enhancing the synthesis and translocation of specific forms of the
glucose transporters. 2. The thiazolidinediones tend to increase
high-density lipoprotein (HDL) cholesterol but have variable
effects on triglycerides and low-density lipoprotein (LDL)
cholesterol.3. Thiazolidinediones require insulin to be present for
their action.4. Although muscle is a major insulin sensitive
tissue, PPAR is virtually absent in skeletal muscle.5. Suggestion :
a) Activation of PPAR in adipose tissue reduces the flux of fatty
acids into muscle, thereby lowering insulin resistance. b)
Activation of adiponectin. Adiponectin is associated with increased
insulin sensitivity and reportedly increases insulin sensitivity by
elevating AMP kinase, which stimulates glucose transport into
muscleand increases fatty acid oxidation.
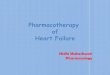
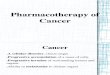
25-Glucosidase InhibitorsAcarbose, Miglitol.Inhibition of
-glucosidase enzyme in the intestinal brush border slows the
absorption of carbohydrates. Used in combination with other oral
antidiabetic agents and/or insulin.SIDE EFFECTS : malabsorption,
flatulence, diarrhea, and abdominal bloating.Reduce postprandial
plasma glucose levels in type 1 and type 2 DM subjects. 2. Acarbose
is most effective when given with a starchy, high-fiber diet with
restricted amounts of glucose and sucrose. 26Mechanism of
Actions
Acarbose Dosing of AcarboseGLUCOBAY : acarbose 50, 100
mg.Initial dose 3x 50 mg, can be increase after 4-8 weeks 3x
100-200 mg