-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
1/16
Official reprint from UpToDatewww.uptodate.com 2013 UpToDate
Author Jeffrey Stovall, MD
Section Editor Paul Keck, MD
Deputy Editor David Solomon, MD
Bipolar disorder in adults: Pharmacotherapy for acute mania,
mixed episodes, and hypomania
Disclosures
All topics are updated as new evidence becomes available and our
peer review process is complete.Literature review current through:
Oct 2013. | This topic last updated: Ago 5, 2013.
INTRODUCTION Bipolar disorder is marked by episodes of mania (
table 1 ) and hypomania ( table 2 ), as well asmixed episodes of
concurrent major depression ( table 3 ) and mania or hypomania [
1]. Despite clinical differencesamong manic, hypomanic, and mixed
episodes, for the purpose of treatment they are considered to be
similar andthus treated with the same medications [ 2-4 ].
This topic reviews treatment of acute mania, mixed episodes, and
hypomania. Treatment of acute bipolar depression and maintenance
treatment are discussed separately. (See "Bipolar disorder in
adults:Pharmacotherapy for acute depression" and "Bipolar disorder
in adults: Maintenance treatment" .)
DEFINITIONS Bipolar disorder is a mood disorder that is
characterized by periods of pathologic mood elevation(mania or
hypomania) [ 1]. Patients with bipolar I disorder experience manic
episodes ( table 1 ) or mixed episodes(major depression concurrent
with mania), and nearly always experience major depressive episodes
( table 3 ). Theclinical course of bipolar II disorder is
characterized by at least one episode of hypomania ( table 2 ), and
one or more major depressive episodes. Despite clinical differences
among manic, hypomanic, and mixed episodes (eg,hypomania is less
severe than mania), for the purpose of treatment they are
considered to be similar and thustreated with the same medications
[ 2-4 ]. The clinical features and diagnosis of bipolar disorder
are discussedseparately. (See "Bipolar disorder in adults: Clinical
features" and "Bipolar disorder in adults: Assessment anddiagnosis"
.)
Pharmacotherapy for mania or mixed episodes depends upon their
severity. Although there are no establishedcriteria that demarcate
severe episodes from mild to moderate illness, we classify episodes
as severe if theyinclude any of the following:
Suicidal ideation or behavior Homicidal ideation or behavior
Aggressive behavior Psychotic features (ie, delusions or
hallucinations)
Poor judgement that places the patient or others at imminent
risk of being harmed
TREATMENT Despite clinical differences among manic, hypomanic,
and mixed episodes (eg, hypomania is lesssevere than mania), for
the purpose of treatment they are considered to be similar and thus
treated with the samemedications [ 2-6 ].
Goal The goal of treating acute manic, hypomanic, and mixed
episodes is remission, which is defined asresolution of the mood
symptoms or improvement to the point that only one or two symptoms
of mild intensitypersist. If psychotic features (delusions or
hallucinations) are also present, resolution of the psychosis is
requiredfor remission. For patients who do not achieve remission, a
reasonable goal is response, which is defined asstabilization of
the patients safety and substantial improvement in the number,
intensity, and frequency of mood
(and psychotic) symptoms. A standardized rating scale, such as
the Young Mania Rating Scale, can be used toquantify response [ 7],
although this is not standard clinical practice.
General principles Treatment of mood elevated syndromes (ie,
manic, hypomanic, and mixed episodes) beginswith an initial
psychiatric history and mental status examination that emphasizes
symptoms of the mood episode,
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
2/16
particularly risk of suicide, aggressiveness, and violence to
others [ 2,3,8 ]. The assessment should also pursuecomorbid
disorders (eg, substance use disorders) that require treatment. The
evaluation includes a generalmedical history, physical examination,
and focused laboratory studies to establish whether the mood
syndrome isdue to the direct physiologic effects of a general
medical condition, and to rule out any contraindications
totreatment (eg, renal impairment and use of lithium , or hepatic
disease and use of valproate ). Additional informationabout the
assessment for bipolar disorder is discussed separately. (See
"Bipolar disorder in adults: Assessmentand diagnosis", section on
'Assessment' .)
Patients who suffer mania, hypomania, or a mixed episode during
maintenance pharmacotherapy should beassessed for adherence to
treatment and are initially treated by optimizing medication doses
[ 2,9,10 ]. This includesensuring serum concentrations are in the
therapeutic range for medications such as lithium or valproate , as
well asincreasing the dose to achieve a higher serum level within
the therapeutic range, provided that side effects do notintervene.
For medications that do not have an established therapeutic serum
concentration, such asantipsychotics, the dose can be increased
within the target dose range.
Substances may cause or exacerbate a mood elevated syndrome.
Thus, antidepressants should be abruptlydiscontinued, and patients
should discontinue drugs of abuse and reduce or eliminate their use
of alcohol, caffeine,and nicotine.
Evidence for the efficacy of treating mood elevated syndromes is
primarily based upon randomized trials withbipolar I manic
patients, although the majority of trials included some patients
with mixed episodes [ 11,12 ]. Eventhough bipolar II disorder is
more prevalent than bipolar I disorder, relatively little research
has focused specificallyon treating hypomania [ 13,14 ]. Many
randomized trials either exclude patients with bipolar II disorder
or lump themtogether with bipolar I patients in the analyses.
Setting and monitoring The treatment setting for manic,
hypomanic, or mixed episode patients dependsupon the severity of
symptoms, comorbid psychopathology (eg, substance use disorder),
level of psychosocialfunctioning, and available support:
Inpatient Hospitalization may be required for managing the
patients safety and symptoms such assuicidal ideation with a
specific plan and intent, delusions or hallucinations, and poor
judgment that poses animminent risk to the patient and others
Partial hospital Moderately ill patients can often be treated in
a partial hospital (day) program, includingpatients with
suicidality that does not pose an imminent risk (eg, fleeting
thoughts of killing oneself, vague or nonexistent plans, and no
intent)
Outpatient Outpatient care may be suitable for less acutely ill
patients (eg, thoughts that family memberswould be better off if
the patient was dead, with no plan or intent to commit suicide)
For outpatient treatment of bipolar disorder, specialized mood
disorder clinics may be preferable to general(standard) psychiatric
clinics early in the course of illness. An open label, two year,
randomized trial compared a
mood disorder clinic (staffed by a cross-disciplinary team who
administered pharmacotherapy and grouppsychoeducation) with
standard care (pharmacotherapy provided at a local community health
center or at apsychiatrists office) in 158 bipolar patients who
were discharged from their first, second, or third
inpatientadmission [ 15 ]. Readmission to the hospital occurred in
more patients who received standard care than specializedcare (55
versus 36 percent). In addition, the median duration of the
readmission was nearly twice as long for patients who had received
standard care rather than specialized care (22 versus 12 days).
The frequency of assessment generally ranges from daily to
monthly, depending upon the severity of persistentsymptoms.
Hospitalized patients are monitored daily, and patients with active
suicidal ideation, a specific plan, andintent to kill themselves
may require constant observation. Outpatients who have responded
less than 50 percentare generally seen weekly; those who have
responded 50 percent or more may be seen every two to four
weeks
until they remit.
Drug classes Based upon randomized trials, drug classes commonly
used to treat acute mania, mixedepisodes, or hypomania include:
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
3/16
Lithium Anticonvulsants AntipsychoticsBenzodiazepines
The mainstays of t reatment are lithium , anticonvulsants, and
antipsychotics used in combination pharmacotherapy(eg, lithium plus
an antipsychotic) or as monotherapy, depending upon the severity of
symptoms. Benzodiazepinesare primarily used as adjunctive treatment
for insomnia, agitation, or anxiety. Treatment of insomnia,
agitation, and
anxiety are discussed separately. (See "Treatment of insomnia"
and "Assessment and management of the acutelyagitated or violent
adult" and "Pharmacotherapy for generalized anxiety disorder"
.)
Duration Although it is not established how long clinicians
should wait to assess the benefit of a medicationregimen, it is
reasonable to allow up to two weeks for a treatment trial [ 4].
Most randomized trials last threeweeks, and the superior efficacy
of active drugs compared with placebo generally begins to manifest
within oneweek.
In a post hoc analysis of a randomized trial that treated manic
or mixed episode patients with olanzapine or risperidone ,
improvement at week one was evaluated as a predictor of either
remission or response (improvementfrom baseline on the mania rating
scale 50 percent) at week three [ 16 ]. Among 234 patients with
improvement 25 percent at week one, 52 percent remitted and 71
percent responded at week three. Conversely, of the 40patients
with
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
4/16
Two other meta-analyses of 6 randomized trials (1396 manic or
mixed episode patients) compared secondgeneration antipsychotics
(including olanzapine , quetiapine , or risperidone ) with placebo
as adjunctivetreatment for patients who did not respond to lithium
, valproate , or carbamazepine monotherapy [ 12,25 ]. Inboth
studies, improvement was significantly greater with the
antipsychotic than placebo. In addition, dropoutdue to adverse
events was comparable for the two groups [ 12 ]. However,
adjunctive antipsychotics causedsignificantly greater weight gain,
somnolence, and extrapyramidal symptoms.
A subsequent randomized trial compared aripiprazole with placebo
as add-on treatment to lithium or valproate in 377 patients [ 26 ].
Remission occurred in significantly more patients who received
aripiprazolecompared with placebo (66 versus 51 percent). However,
aripiprazole caused significantly higher rates of akathisia (19
versus 5 percent).
Combination pharmacotherapy for severe manic or mixed episodes
is endorsed by several treatment guidelines[2,4,21 ].
However, adding ziprasidone to lithium or divalproex is not
efficacious, based upon two randomized trials [ 12,22 ]. As an
example, a three week trial assigned 656 patients with manic or
mixed episodes who had not responded toeither lithium or divalproex
to receive adjunctive treatment twice per day with ziprasidone 20
to 40 mg, ziprasidone60 to 80 mg, or placebo [ 22 ]. Neither high
dose nor low dose ziprasidone provided any benefit.
In addition, we generally avoid combining carbamazepine with an
antipsychotic, based upon randomized trials thatfound this
combination is no more efficacious than carbamazepine alone [ 27,28
]. Carbamazepine induces hepaticenzymes that metabolize
antipsychotics, and in one trial lowered the antipsychotic blood
level by 40 percent [ 28 ].
When prescribing a medication combination, both drugs are
started and titrated up simultaneously. The doses andside effects
of lithium , valproate , and antipsychotics are discussed elsewhere
in this topic. (See 'Medication dosesand side effects' below.)
Specific medication interactions that can occur may be
determined using the drug interactions tool (Lexi-InteractOnline)
included in UpToDate. This tool can be accessed from the UpToDate
online search page or through theindividual drug information topics
in the section on Drug interactions.
Patients who cannot tolerate combination pharmacotherapy are
treated with monotherapy. (See 'First linemonotherapy' below.)
Resistant patients A severe manic or mixed episode that does not
respond to one medication combinationshould be treated with a
second medication combination. Generally, lithium is switched to
valproate or vice versa.
As an example, for patients who do not respond to lithium plus
haloperidol within two weeks of reaching targetdoses, we suggest
tapering and discontinuing lithium at the same time that valproate
is started and titrated up.Lithium is generally tapered over one
week by the same amount for each dose decrease (eg, lithium 1800 mg
per day is decreased by 600 mg per day, every one to two days). The
dose and side effects of lithium and valproateare discussed
separately. (See 'Lithium' below and 'Anticonvulsants' below.)
Conversely, for patients who do not respond to valproate plus
haloperidol within two weeks of reaching targetdoses, we suggest
tapering and discontinuing valproate at the same time that lithium
is started and titrated up.Valproate is generally tapered over one
week by the same amount for each dose decrease (eg, valproate
2000mg per day is decreased by 500 mg per day, every one to two
days).
For patients who do not respond to lithium plus an antipsychotic
or to valproate plus the same antipsychotic, wesuggest starting a
third medication combination involving lithium or valproate plus an
antipsychotic. The choicebetween lithium and valproate is based
upon efficacy and tolerability in the two prior trials. In
addition, theantipsychotic used in the two prior trials is
discontinued and a new one chosen from amongst aripiprazole
,haloperidol (or another first-generation antipsychotic),
olanzapine , quetiapine , risperidone , or ziprasidone .
Nohead-to-head trials have compared antipsychotics in combination
with lithium or valproate; thus, the choice of anantipsychotic is
based upon other factors, including past response to medications,
side effect profiles, comorbidgeneral medical conditions, potential
for drug-drug interactions, patient preference, and cost.
The antipsychotic is generally tapered over one week by the same
amount for each dose decrease (eg,
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
5/16
haloperidol 10 mg per day is decreased by 5 mg per day, every
one to two days), and at the same time, the other antipsychotic is
started and titrated up. The dose and side effects of
antipsychotics are discussed separately. (See'Antipsychotics'
below.)
Refractory patients
Electroconvulsive therapy We suggest electroconvulsive therapy
(ECT) for refractory patients whosemanic or mixed episode does not
respond to four to six medication combinations [ 4,29,30 ]. In one
controlled trial of
30 manic patients, improvement occurred in significantly more
patients who received ECT plus chlorpromazinecompared with patients
who received simulated ECT plus chlorpromazine (80 versus 7
percent) [ 31 ].
ECT is generally safe and there are no absolute
contraindications, even in patients whose general medical status
iscompromised [ 32 ]. However, safety concerns regarding ECT
necessitate preprocedure medical consultation.
Adverse effects include cardiopulmonary events, aspiration
pneumonia, fractures, dental and tongue injuries,headache, nausea,
and cognitive impairment. Medical consultation prior to ECT is
discussed separately. (See"Medical consultation for
electroconvulsive therapy" .)
Electrode placement and other aspects of ECT technique for
treating geriatric bipolar disorder have not beenstandardized.
Thus, ECT is typically administered with the same technique used
for other indications and isgenerally given three times per week on
alternating days. Most patients, regardless of indication, remit
with 6 to 12
treatments, but some patients may require 20 or more. Additional
information about ECT is discussed separately.(See "Overview of
electroconvulsive therapy (ECT) for adults" and "Technique for
performing electroconvulsivetherapy (ECT) in adults" .)
Other medications For patients with refractory manic or mixed
episodes who decline ECT, do not remitwith it, or have no access to
it, and who do not respond to medication combinations involving
lithium or valproateplus aripiprazole , haloperidol (or another
first-generation antipsychotic), olanzapine , quetiapine ,
risperidone , or ziprasidone , we suggest pharmacotherapy with
lithium or valproate plus asenapine , clozapine , or
paliperidone[33-38 ]. Patients unresponsive to lithium or valproate
plus asenapine, clozapine, or paliperidone may possiblybenefit from
allopurinol plus lithium, tamoxifen monotherapy, and tamoxifen plus
lithium [ 39-43 ]. No head-to-headtrials have compared these other
medication options. Thus, the choice is based upon other factors,
including past
response to medications, side effect profiles, comorbid general
medical conditions, potential for drug-druginteractions, patient
preference, and cost.
In randomized trials with 977 manic or mixed episode patients,
asenapine 5 to 10 mg two times per day was moreefficacious than
placebo, but much less efficacious than olanzapine 5 to 20 mg once
per day [ 34,35 ]. Common sideeffects of asenapine include
sedation, fatigue, dizziness, extrapyramidal symptoms, vomiting,
dry mouth, andweight gain [ 34,35 ]. Additional information about
asenapine is discussed separately. (See
"Second-generationantipsychotic medications: Pharmacology,
administration, and comparative side effects" .)
Limited evidence suggests that clozapine may ameliorate
refractory manic or mixed episodes [ 33,36,37 ]. Clozapineis
started at a dose of 12.5 or 25 mg at bedtime, and then increased
by 25 mg per day every two days as
tolerated, to a target dose of 150 to 450 mg two t imes per day.
However, clozapine can cause agranulocytosisand other blood
dyscrasias, and clinicians must monitor complete blood counts every
one or two weeks. Clozapineis also associated with the metabolic
syndrome. Thus, patients taking clozapine should be regularly
monitored for weight, waist circumference, blood pressure, and
serum glucose and lipids. Additional information about clozapineis
discussed separately. (See "Second-generation antipsychotic
medications: Pharmacology, administration, andcomparative side
effects", section on 'Clozapine' .)
Paliperidone has demonstrated inconsistent benefits in patients
with acute manic and mixed episodes. Arandomized trial compared
paliperidone (flexibly dosed 3 to 12 mg per day) with placebo in
268 patients with amanic or mixed episode, and found that remission
occurred in significantly more patients who received
paliperidonethan placebo (52 versus 29 percent) [ 38 ]. However, a
second randomized trial found remission did not differ
significantly between the groups who received fixed doses of
paliperidone 3 mg, 6 mg, or 12 mg, and the groupthat received
placebo (37 or 42 or 45 versus 37 percent) [ 44 ]. A third
randomized trial found that among patientswith an inadequate
response to lithium or valproate monotherapy, there was no
significant difference betweenadjunctive paliperidone and
adjunctive placebo [ 45 ]. The most common adverse events with
paliperidone areheadache, somnolence, dizziness, akathisia,
hypertonia, and dyspepsia. Additional information about
paliperidone
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
6/16
is discussed separately. (See "Second-generation antipsychotic
medications: Pharmacology, administration, andcomparative side
effects", section on 'Paliperidone' .)
Allopurinol , which is typically used to prevent attacks of
gouty arthritis and nephropathy, has been studied as anoption for
treating mania [ 46 ], based upon observations that adenosine, a
purine compound and neuromodulator, ismetabolized to uric acid, and
that increased uric acid turnover is related to remission of mania
[ 39,47 ]. Ameta-analysis of three randomized trials compared
allopurinol with placebo as adjunctive treatment in 186
manicpatients, and found a significant, clinically moderate
advantage favoring active drug; there was little to no
heterogeneity across studies [ 48 ]. In addition,
discontinuation due to side effects was comparable.
Tamoxifen is a centrally active protein kinase C inhibitor that
has demonstrated efficacy for treating manic andmixed episodes in
several small randomized trials [ 40-43 ]. The largest compared
tamoxifen (20 to 40 mg two timesper day) with placebo in 66
patients [ 40 ]. Response (improvement from baseline on the mania
rating scale 50percent) occurred in significantly more patients who
received tamoxifen than placebo (48 versus 5 percent), as
didremission (28 versus 0 percent). Tamoxifen is widely used to
prevent breast cancer because it is a selectiveestrogen receptor
antagonist, and these antiestrogen effects preclude its use beyond
patients unresponsive tomost or all other t reatments.
There is little or no evidence to support treating acute mania
or mixed episodes with anticonvulsants other thanvalproate and
carbamazepine . Lamotrigine , gabapentin , and topiramate are not
effective for treating mania[49-54 ]. In addition, a systematic
review found that there was insufficient evidence to evaluate the
anticonvulsanttiagabine , and results from available case series
are conflicting [ 55 ].
Nor do we suggest oxcarbazepine , which has been substituted for
carbamazepine to treat mania because their molecular structures are
similar and oxcarbazepine has fewer side effects. There is no high
quality evidence thatoxcarbazepine has any benefit in adults [ 56
]. In addition, a randomized trial found that oxcarbazepine
wascomparable with placebo in 116 manic or mixed episode children
and adolescents [ 57 ].
Mild to moderate illness Mild to moderate illness is marked by
the absence of suicidal or homicidal ideation or behavior,
aggressiveness, psychotic features (ie, delusions or
hallucinations), and poor judgement that places thepatient or
others at imminent risk of being harmed. Monotherapy is commonly
used for initial treatment of
hypomania and mild to moderate manic and mixed episodes.
First line monotherapy For patients with hypomania and mild to
moderate manic and mixed episodes, wesuggest monotherapy with
risperidone or olanzapine , based upon efficacy and tolerability [
54 ]. However,reasonable alternatives include aripiprazole ,
carbamazepine , haloperidol , lithium , quetiapine , valproate , or
ziprasidone . Doses and side effects are discussed elsewhere in the
topic. (See 'Medication doses and side effects'below.)
A multiple-treatments meta-analysis of 68 randomized trials
(16,073 patients with an acute manic or mixedepisode, treated for
three weeks) found that aripiprazole , carbamazepine , haloperidol
, lithium , olanzapine ,quetiapine , risperidone , valproate , and
ziprasidone were each significantly more efficacious than placebo [
54 ]. In
addition, the meta-analysis ranked these drugs by efficacy,
using indirect comparisons of the drugs (through their relative
effect with a common comparator, typically placebo), as well as
analyzing direct comparisons betweendrugs. Beginning with the most
efficacious drug, the rank order for efficacy was:
HaloperidolRisperidoneOlanzapine
AripiprazoleCarbamazepineLithiumQuetiapine
Valproate (or divalproex)Ziprasidone
Further, the meta-analysis ranked the drugs by frequency of
treatment discontinuation for any reason, includingadverse effects
and lack of efficacy. Beginning with the drug with the lowest rate
of dropout, the rank order was:
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
7/16
OlanzapineRisperidoneQuetiapineValproateCarbamazepine
AripiprazoleHaloperidolZiprasidoneLithium
The indirect comparisons distinguish this multiple-treatments
meta-analysis from smaller, conventionalmeta-analyses, which
concluded that efficacy was comparable for aripiprazole ,
carbamazepine , haloperidol ,lithium , olanzapine , quetiapine ,
risperidone , valproate , and ziprasidone [11,12,25,58 ]. Although
substantialuncertainties are introduced when these sorts of rank
orders are created through a multiple-treatmentsmeta-analysis, this
is probably the best evidence for comparing drugs for acute
hypomania and mild to moderatemanic and mixed episodes. While it is
not clear that there are meaningful differences between adjacently
rankedmedications, drugs near the top of the rank order are
probably superior to those near the bottom of the rank
order.Multiple-treatments meta-analysis is discussed separately.
(See "Systematic review and meta-analysis", section on'Network
meta-analysis' .)
Clinicians should consider factors other than the rank order of
efficacy and treatment discontinuation whenchoosing a drug,
including the patients past response to medications, the past
response of family members withbipolar disorder to medications,
specific symptoms, adverse drug effects, comorbid medical
illnesses, concurrentmedications, and cost. As an example, lithium
is generally avoided in patients with significant renal
disease,valproate in patients with liver disease, and olanzapine in
obese patients. In addition, carbamazepine may bedifficult to use
because of its tendency to increase metabolism of concomitant
medications. Medication side effectsare discussed separately. (See
'Medication doses and side effects' below and "Bipolar disorder in
adults andlithium: Pharmacology, administration, and side effects",
section on 'Lithium side effects' and "Pharmacology of
antiepileptic drugs" and "First-generation antipsychotic
medications: Pharmacology, administration, andcomparative side
effects" and "Second-generation antipsychotic medications:
Pharmacology, administration, andcomparative side effects" .)
The long-term implications of choosing a drug also need to be
considered; all patients with bipolar disorder shouldreceive
maintenance treatment, which commonly consists of the drug used to
induce remission. As an example,maintenance lithium is common
because it has been widely studied and is efficacious [ 59,60 ],
and long-termtreatment with lithium may reduce the risk of suicide
attempts and deaths [ 61-64 ]. By contrast, haloperidol isgenerally
not used in maintenance treatment because it can cause movement
disorders and may increase the riskof bipolar major depression [
65,66 ]. Maintenance treatment is discussed separately. (See
"Bipolar disorder inadults: Maintenance treatment", section on
'Reduced risk of suicide' .)
For mildly to moderately ill patients who do not respond to
treatment with one monotherapy trial within two weeks
of reaching the target dose, or do not tolerate the drug, we
suggest tapering and discontinuing the failedmedication over one
week at the same time that another monotherapy is started and
titrated up. The failedmedication is generally tapered by the same
amount for each dose decrease. As an example, quetiapine 600 mgper
day is decreased by 100 to 200 mg per day, every one to two
days.
Treatment resistance For hypomanic and mild to moderate manic
and mixed episodes that do not respondto three to five monotherapy
trials involving aripiprazole , carbamazepine , haloperidol ,
lithium , olanzapine ,quetiapine , risperidone , valproate , and
ziprasidone , we suggest combining lithium or valproate with
anantipsychotic. However, lithium plus valproate is a reasonable
alternative [ 67,68 ]. Medication combinations involvinglithium or
valproate plus an antipsychotic are discussed elsewhere in the
topic. (See 'First line medicationcombinations' above.)
Benzodiazepines We suggest clonazepam for patients who have
hypomanic or mild to moderate manicor mixed episodes and cannot
tolerate lithium , anticonvulsants, or antipsychotics. However,
lorazepam is areasonable alternative. Monotherapy with a
benzodiazepine is unusual due to the large number of
availablemedication options for manic, hypomanic, or mixed
episodes; benzodiazepines are generally used as adjunctive
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
8/16
therapy to treat insomnia, agitation, or anxiety in patients
with pathologic mood elevated syndromes. Given the highrate of
substance use disorders among bipolar patients and the potential
for abusing benzodiazepines, these drugsare generally limited to
acute treatment [ 69 ].
Clonazepam is usually started at a dose of 1 to 3 mg per day,
taken in two divided doses. The drug is generallytitrated up to a
target dose ranging from 2 to 6 mg per day, depending upon efficacy
and tolerability, althoughdoses as high as 24 mg per day have been
used [ 70 ]. Side effects include disinhibition, sedation, and
respiratorydepression.
Lorazepam is usually started at a dose of 2 to 4 mg per day,
taken in three to four divided doses. The drug isgenerally titrated
up to a target dose ranging from 3 to 8 mg per day, depending upon
efficacy and tolerability,although doses as high as 24 mg per day
have been used [ 70 ]. Side effects include disinhibition,
sedation, andrespiratory depression.
Evidence of efficacy includes a meta-analysis of five
heterogeneous randomized trials (122 manic patients), whichfound
that clonazepam monotherapy (2 to 24 mg per day) was efficacious [
70 ]. The same study analyzed four heterogeneous randomized trials
(108 manic patients) involving lorazepam (4 to 24 mg per day) and
found that itwas not effective. However, one randomized trial
directly compared lorazepam (mean daily dose 13 mg) withclonazepam
(mean daily dose 14 mg) in 24 manic patients, and found that
moderate to marked improvementoccurred in significantly more
patients who received lorazepam than clonazepam (63 versus 18
percent), as didremission (38 versus 0 percent) [ 71 ]. The
frequency of side effects does not differ between the two drugs [
70 ].
The pharmacology and abuse of benzodiazepines are discussed
elsewhere.
Medication doses and side effects
Lithium The starting dose of lithium is usually 300 mg two or
three times daily; smaller doses (eg, 150 mgtwice daily) are used
in the elderly [ 69,72-74 ]. The dose should be increased by 300 to
600 mg every one to fivedays based upon response, tolerability, and
body mass index. The goal is to reach a therapeutic serum level,
whichgenerally occurs with a dose of 900 mg to 1800 mg per day.
Dose increases generally occur more frequently atthe beginning of
treatment, and less often as clinicians approach the target dose.
Additional information about the
dose of lithium is discussed elsewhere. (See "Bipolar disorder
in adults and lithium: Pharmacology, administration,and side
effects", section on 'Lithium dose and serum concentrations' and
"Geriatric bipolar disorder: Acutetreatment", section on 'First
line medications' .)
The target serum level for acute treatment is between 0.8 and
1.2 meq/L; levels should not exceed 1.2 meq/L toreduce the risk of
toxicity [ 73 ]. Patients who cannot tolerate a level of 0.8 meq/L
may respond to a level of 0.6meq/L. Lithium levels should be
measured five to seven days after each dose increase. Levels are
drawn 12 hoursafter the last dose (12-hour serum trough level) and
generally collected in the morning, before the first dose of
theday. Additional information about lithium serum levels is
discussed elsewhere. (See "Bipolar disorder in adults andlithium:
Pharmacology, administration, and side effects", section on
'Lithium dose and serum concentrations' .)
Lithium can cause many acute and long-term adverse effects. The
most common acute side effects are nausea,
tremor, polyuria and thirst, weight gain, loose stools, and
cognitive impairment [ 74-76 ]. Severe or suddenworsening of acute
side effects may be a sign of lithium toxicity. Over the long term,
lithium can adversely affectthe kidneys and thyroid gland. In
addition, cardiac rhythm disturbances have been described; these
almost alwaysoccur in patients with preexisting cardiac disease.
Additional information about side effects and how to managethem is
discussed elsewhere:
(See "Bipolar disorder in adults and lithium: Pharmacology,
administration, and side effects", section on'Lithium side effects'
.)(See "Lithium poisoning" .)(See "Renal toxicity of lithium"
.)(See "Lithium and the thyroid" .)
Contraindications to lithium , lithium toxicity, drug
interactions with lithium, the different available preparations of
lithium, and laboratory tests and monitoring are discussed
elsewhere. (See "Bipolar disorder in adults and
lithium:Pharmacology, administration, and side effects" .)
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
9/16
Anticonvulsants Anticonvulsants that are efficacious for acute
mania, mixed episodes, and hypomaniainclude valproate and
carbamazepine .
Suicidality Bipolar disorder is associated with an increased
risk of suicide deaths [ 77 ], and all patientsshould be monitored
for emergence or worsening of suicidal thoughts and behavior.
Although some observationalstudies suggest that anticonvulsants may
increase the risk of suicidal ideation or behavior, these drugs
aregenerally safe to use when patients are regularly monitored.
The US Food and Drug Administration warned clinicians that
anticonvulsants are associated with an increased riskof suicidal
thoughts and behavior, based upon a pooled analysis of 199
controlled trials that included 43,892patients with a variety of
illnesses [ 78 ]. In addition, a separate exploratory analysis of a
medical and pharmacyclaims database that included 297,620 new
episodes of treatment with an anticonvulsant suggested
thatgabapentin , lamotrigine , oxcarbazepine , and tiagabine may be
associated with an increased risk of suicidal acts or violent
deaths, compared with topiramate [79 ].
However, an analysis of a different national claims database
that involved 47,918 patients diagnosed specificallywith bipolar
disorder found [ 80 ]:
The frequency of suicide attempts in patients treated with
antiepileptic drugs and patients not receivingantiepileptic drugs
was comparable
For patients treated with antiepileptic drugs, the rate of
suicide attempts was greater before treatment thanafter
treatment
Patients receiving antiepileptic drug monotherapy (and no
concomitant antidepressant or antipsychotic) hadfewer suicide
attempts compared to patients receiving no pharmacotherapy
Other observational studies have found that antiepileptics were
not associated with an increased risk of suicidalbehavior in
bipolar patients [ 81 ]. As an example, analyses using a national
database with over 5,000,000 patientsfound that among patients with
bipolar disorder, treatment with antiepileptic drugs was not
associated with anincreased risk of suicide attempts [ 82 ].
Valproate or divalproex Valproate is usually started at a dose
of 250 mg two or three times per day.The dose is increased by 250
mg to 500 mg every one to three days as tolerated to reach a
therapeutic serumlevel, which generally occurs with 1500 mg to 2500
mg per day [ 74,83 ]. Valproate is usually administered twicedaily
(although a once-a-day formulation is available in the United
States). Oral loading and rapid titration to a fulldose within one
to two days by prescr ibing 20 mg/kg/day may result in earlier
improvement in symptoms and areduced need for adjunctive
antipsychotics or benzodiazepines [ 84 ].
We suggest drawing valproate serum levels two to five days after
each dose increase and prescribing the drug toachieve a target
serum level between 50 and 125 mcg/mL. Levels should be drawn 12
hours after the last doseand generally collected in the morning,
before the first dose of the day. A post hoc analysis of pooled
data fromthree controlled trials (374 acutely manic inpatients)
found that efficacy increased as serum levels increased [ 85 ].In
addition, the efficacy of valproate was significantly greater than
placebo for levels 71 mcg/mL, and the largestclinical effect for
valproate occurred in patients with a mean serum level of 88
mcg/mL. Levels should be checkedat 6 to 12 month intervals, and are
particularly useful in patients receiving medications that affect
valproateconcentrations and to confirm problems with adherence.
Some patients may not require regular valproate levels,and one
review concluded that clinical observation of efficacy and toxicity
can be used to guide some doseadjustments [ 86 ].
Common side effects of valproate include weight gain, nausea,
vomiting, hair loss, easy bruising, and tremor.Divalproex is a
formulation of valproate that can minimize gastrointestinal
distress. Valproate is rarely associatedwith hepatic failure and
thrombocytopenia; liver function tests and platelets should thus be
monitored at 6 to 12month intervals in all patients taking the drug
[ 33,69,87 ]. (The US Food and Drug Administration
recommendschecking liver function tests prior to initiating
treatment and at frequent intervals thereafter, especially during
thefirst six months.) In addition, valproate rarely causes
pancreatitis; symptoms of abdominal pain and vomiting shouldprompt
an assessment that includes a serum amylase and lipase.
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
10/16
Additional information about the pharmacology of valproate and
its adverse effects and available preparations arediscussed
separately. (See "Pharmacology of antiepileptic drugs", section on
'Valproate' .)
Carbamazepine Carbamazepine is usually started at a dose of 100
mg to 200 mg one or two times per day [ 74,88 ]. The dose should be
increased by 200 mg per day every one to four days, to a final dose
of about 800to 1000 mg per day, although the effective dose may
range between 200 and 1800 mg per day. Carbamazepine istypically
administered twice daily. Therapeutic serum levels have not been
established for treating acute manic or mixed episodes. However,
many clinicians aim for a level of 4 to 12 mcg/mL, which is the
target range established
for treating epilepsy. Extended release formulations are better
tolerated in patients with bipolar disorder [ 89 ].
The major systemic side effects of carbamazepine are nausea,
vomiting, diarrhea, hyponatremia, rash, pruritus,leukopenia, and
fluid retention. In addition, the drug is associated with
life-threatening rashes (Stevens-Johnsonsyndrome and toxic
epidermal necrolysis), particularly during the first eight weeks of
therapy [ 90 ]. This reaction issignificantly more common in
patients with the HLA-B*1502 allele (estimated incidence of 5
percent), which occursalmost exclusively in patients of Asian
ancestry, including South Asian Indians [ 91-93 ]. The US Food and
Drug
Administration recommends screening for this allele in patients
of these ethnic groups prior to startingcarbamazepine [ 94 ].
Neurotoxicity includes drowsiness, dizziness, blurred or double
vision, lethargy, and headache.Carbamazepine also induces liver
enzymes and frequently causes drug-drug interactions that result in
lower serumconcentrations of concomitant drugs [ 33,69,87 ]. This
induction of liver enzymes often decreases serum
concentrations of carbamazepine. Liver function tests and a
complete blood count, serum sodium, and serumcarbamazepine level
are recommended every 6 to 12 months.
The pharmacology of carbamazepine and its adverse effects and
available preparations are discussed in greater detail elsewhere.
(See "Pharmacology of antiepileptic drugs", section on
'Carbamazepine' .)
Antipsychotics First- and second-generation antipsychotics are
efficacious for treating both psychotic andnonpsychotic manic and
mixed episodes, as well as hypomania [ 2,3,11,12,21,24,25,95 ].
First-generation Among first-generation antipsychotics, we
prefer haloperidol for treating manic andmixed episodes because it
has been widely studied and generally causes less orthostatic
hypotension and sedationthan chlorpromazine , which is also
efficacious [ 58,96 ]. Other first-generation antipsychotics such
as fluphenazine ,
loxapine , perphenazine , thiothixene , and trifluoperazine are
effective as well [ 97 ].
We suggest patients initially receive haloperidol at a dose of 5
to 15 mg per day, depending upon the severity of symptoms, the
patients body mass index, and adverse effects that emerge. The drug
is taken either once per dayor in two divided doses, depending upon
tolerability and the patients ability to adhere to treatment with
divideddoses. One useful guide is to prescribe 0.2 mg per kg per
day [ 98 ]. In a meta-analysis of 15 randomized trials(2022
patients with acute manic or mixed episodes), which found that
haloperidol was comparable tocarbamazepine , olanzapine ,
risperidone , and valproate , the dose of haloperidol ranged from 2
to 85 mg per day[58 ].
Conventional antipsychotics are associated with extrapyramidal
symptoms, akathisia, and tardive dyskinesia.
Extrapyramidal symptoms are usually managed by lowering the dose
of the antipsychotic or by adding ananticholinergic drug, either
benztropine 1 to 2 mg two to four times daily or trihexyphenidyl 2
to 5 mg two to four times daily.
Although switching from mania to depression has been attributed
to first-generation antipsychotics, the evidence isnot clear. A
meta-analysis of six randomized trials (1774 manic patients;
heterogeneity across studies wasmoderate) compared haloperidol with
second-generation antipsychotics ( aripiprazole , olanzapine ,
quetiapine ,risperidone , or ziprasidone ), and found that
treatment emergent depression was comparable for patients
whoreceived haloperidol or second-generation antipsychotics (10 and
7 percent) [ 99 ]. However, a second analysis thatexcluded one
outlier trial (and eliminated the heterogeneity) found that
depressive switches occurred in morepatients treated with
haloperidol (12 versus 7 percent). In assessing patients treated
with an antipsychotic,
clinicians should distinguish between switching to a depressive
syndrome and the side effect of affective blunting or
flattening.
The pharmacology, administration, and side effects of
first-generation antipsychotics are discussed elsewhere.(See
"First-generation antipsychotic medications: Pharmacology,
administration, and comparative side effects" and
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
e 16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
11/16
"Neuroleptic malignant syndrome" and "Tardive dyskinesia:
Etiology and epidemiology" .)
Second-generation Aripiprazole , olanzapine , quetiapine ,
risperidone , and ziprasidone are eachefficacious for treating
manic, hypomanic, and mixed episodes [ 54 ], and the choice often
depends upon differencesin adverse side effects. Metabolic problems
such as weight gain, glucose intolerance, diabetes mellitus,
andhyperlipidemia are most likely to occur with olanzapine,
followed by quetiapine and risperidone. Thus, patientstaking
olanzapine, quetiapine, and risperidone should be regularly
monitored for weight, waist circumference, bloodpressure, and serum
glucose and lipids. Extrapyramidal side effects (EPS) are more
common with aripiprazole,
risperidone, or ziprasidone compared with olanzapine or
quetiapine. The metabolic syndrome and EPS arediscussed separately.
(See "The metabolic syndrome (insulin resistance syndrome or
syndrome X)" and"Pharmacotherapy for schizophrenia: Side effect
management" .)
The usual starting and target dose for second-generation
antipsychotics and common side effects that occurred inrandomized
monotherapy trials are described below [ 74,100 ]. Target doses can
generally be achieved within oneweek of starting the medication.
Some drugs are available as oral dissolvable formulations for
patients whopretend to swallow their pills (cheek) and spit them
out later when the clinician is not looking.
Aripiprazole Aripiprazole is started at a dose of 10 to 30 mg
once daily. The usual target dose is 15 to 45mg taken once per day.
Common side effects include headache, nausea, vomiting,
constipation, insomnia,
and akathisia. An oral dissolvable formulation is available.
Olanzapine Olanzapine is started at a dose of 10 to 15 mg once
daily or in two divided doses. The usualtarget dose is 10 to 30 mg
per day, taken at bedtime or in two divided doses. Some patients
may requireand tolerate 40 or 50 mg per day. Common side effects
include sedation, constipation, dry mouth, increasedappetite,
weight gain, and orthostatic hypotension. An oral dissolvable
formulation is available.
Quetiapine Quetiapine is started at a dose of 100 to 200 mg once
daily or in two divided doses. The usualtarget dose is 400 to 800
mg taken at bedtime or in two divided doses. Some patients may
require andtolerate 1000 or 1200 mg per day. Common side effects
include headache, dry mouth, constipation, weightgain, sedation,
dizziness, and orthostatic hypotension.
Risperidone Risperidone is started at a dose of 1 to 2 mg once
daily or in two divided doses. The usualtarget dose is 4 to 8 mg
per day. It is usually taken in two divided doses per day, but some
patients may dowell with a single dose at bedtime. Common side
effects include prolactin elevation, akathisia, sedation,dyspepsia,
nausea, and weight gain. An oral dissolvable formulation is
available.
Ziprasidone Ziprasidone is started at a dose of 40 mg two times
per day. The usual target dose is 40 to80 mg two times per day.
Some patients may require and tolerate 200 mg per day or more.
Common sideeffects include headache, sedation, extrapyramidal
symptoms, akathisia, and dizziness.
Additional information about second-generation antipsychotics is
discussed separately. (See "Second-generationantipsychotic
medications: Pharmacology, administration, and comparative side
effects" .)
SPECIAL CIRCUMSTANCES
Elderly Treatment of geriatric manic, hypomanic, and mixed
episodes is discussed separately. (See "Geriatricbipolar disorder:
Acute treatment", section on 'Manic, hypomanic, and mixed episodes'
.)
Pregnancy Treatment of mania, hypomania, and mixed episodes
during pregnancy; the teratogenic andpostnatal risks of
pharmacotherapy for bipolar disorder; the principles of teratology;
preconception and prenatalmaintenance pharmacotherapy for bipolar
patients; and preconception counseling for patients with bipolar
disorder are discussed separately. (See "Bipolar disorder in
pregnant women: Treatment of mania and hypomania" and"Bipolar
disorder in adults: Teratogenic and postnatal risks of
pharmacotherapy" and "Principles of teratology" and"Bipolar
disorder in women: Preconception and prenatal maintenance
pharmacotherapy" and "Bipolar disorder inwomen: Contraception and
preconception assessment and counseling" .)
INFORMATION FOR PATIENTS UpToDate offers two types of patient
education materials, The Basics andBeyond the Basics. The Basics
patient education pieces are written in plain language, at the 5 to
6 gradereading level, and they answer the four or five key
questions a patient might have about a given condition. These
th th
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
e 16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
12/16
articles are best for patients who want a general overview and
who prefer short, easy-to-read materials. Beyondthe Basics patient
education pieces are longer, more sophisticated, and more detailed.
These articles are writtenat the 10 to 12 grade reading level and
are best for patients who want in-depth information and are
comfortablewith some medical jargon.
Here are the patient education articles that are relevant to
this topic. We encourage you to print or e-mail thesetopics to your
patients. (You can also locate patient education articles on a
variety of subjects by searching onpatient info and the keyword(s)
of interest.)
Basics topics (see "Patient information: Bipolar disorder (The
Basics)" and "Patient information: Reducingthe costs of medicines
(The Basics)" )
Beyond the Basics topics (see "Patient information: Bipolar
disorder (manic depression) (Beyond theBasics)" and "Patient
information: Reducing the costs of medicines (Beyond the Basics)"
)
The National Institute of Mental Health also has educational
material explaining the symptoms, course of illness,and treatment
in a booklet entitled "Bipolar Disorder" that is available online
at the website
http://www.nimh.nih.gov/health/publications/bipolar-disorder/complete-index.shtml
or through a toll-free number, 866-615-6464. The website also
provides references, summaries of study results in language
intended for the lay public, and information
about clinical trials currently recruiting patients.
More comprehensive information is provided in books written for
patients and family members, including TheBipolar Disorder Survival
Guide: What You and Your Family Need to Know, written by David J.
Miklowitz, PhD(published by The Guilford Press, 2002) and An
Unquiet Mind: A Memoir of Moods and Madness, written by KayJamison
PhD (published by Random House, 1995).
The Depression and Bipolar Support Alliance (
http://www.dbsalliance.org or 800-826-3632) is a
nationalorganization whose mission is to educate patients and
family members about bipolar disorder and how to copewith it. Other
functions include increasing public awareness of the illness and
advocating for more research andservices. The organization is
administered and maintained by members and has local chapters.
The National Alliance on Mental Illness ( http://www.nami.org or
800-950-6264) is a similarly structured organizationdevoted to
providing education, support, and advocacy for patients with any
mental illness. Bipolar disorder is oneof their priorities.
SUMMARY AND RECOMMENDATIONS
Bipolar disorder is characterized by pathologic mood elevation.
Patients with bipolar I disorder experiencemanic episodes ( table 1
) or mixed episodes (major depression concurrent with mania or
hypomania), andnearly always experience major depressive episodes (
table 3 ). Bipolar II disorder is characterized by atleast one
episode of hypomania ( table 2 ) and one or more episodes of major
depression. (See 'Definitions'above and "Bipolar disorder in
adults: Assessment and diagnosis", section on 'Diagnosis' .)
Patients presenting with acute mania, mixed episodes, or
hypomania should be assessed for risk of suicideand homicide,
aggressiveness, psychotic features, and poor judgement.
Antidepressants should bediscontinued, and substance abuse treated.
(See 'General principles' above.)
Drug classes commonly used to treat acute mania, mixed episodes,
or hypomania include lithium ,anticonvulsants, antipsychotics, and
benzodiazepines. (See 'Drug classes' above.)
For patients with severe manic or mixed episodes, we suggest
initial treatment with lithium or valproate plusan antipsychotic,
rather than monotherapy ( Grade 2B ). (See 'First line medication
combinations' above and'Medication doses and side effects'
above.)
For resistant patients with severe manic or mixed episodes that
do not respond to one medicationcombination ( lithium or valproate
plus an antipsychotic), we suggest additional medication
combination trialsrather than electroconvulsive therapy (ECT) (
Grade 2B ). Lithium is switched to valproate (or vice versa),and
the antipsychotic is switched to another antipsychotic from among
aripiprazole , haloperidol , olanzapine ,
th th
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
e 16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
13/16
quetiapine , or risperidone . (See 'Resistant patients'
above.)
For treatment refractory patients with severe manic or mixed
episodes who do not respond to four to sixmedication combinations,
we suggest ECT rather than additional trials of pharmacotherapy
combinations(Grade 2C ). (See 'Refractory patients' above.)
For patients with acute hypomania or mild to moderate manic or
mixed episodes, we suggest initialtreatment with risperidone or
olanzapine monotherapy rather than other drugs ( Grade 2B ).
However,
reasonable alternatives include aripiprazole , carbamazepine ,
haloperidol , lithium , quetiapine , valproate , or ziprasidone .
In addition to eff icacy and tolerability, the choice depends upon
past response to medications,comorbid medical illness, concurrent
medications, specific symptoms, and cost. (See 'First
linemonotherapy' above.)
For patients with hypomania or mild to moderate manic or mixed
episodes that do not respond to three tofive monotherapy trials
involving aripiprazole , carbamazepine , haloperidol , lithium ,
olanzapine , quetiapine ,risperidone , valproate , and ziprasidone
, we suggest combining either lithium or valproate with
anantipsychotic (other than ziprasidone) rather than additional
monotherapy trials ( Grade 2C ). Another optionis using lithium
plus valproate. (See 'First line medication combinations'
above.)
Use of UpToDate is subject to the Subscription and License
Agreement .
Topic 679 Version 34.0
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
e 16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
14/16
GRAPHICS
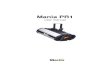
DSM-IV-TR diagnostic criteria for mania
A. A distinct period of abnormally and persistently elevated,
expansive, or irritable mood, lastingat least 1 week (or any
duration if hospitalization is necessary).
B. During the period of mood disturbance, three (or more) of the
following symptoms have
persisted (four if the mood is only irritable) and have been
present to a significant degree:1) Inflated self-esteem or
grandiosity
2) Decreased need for sleep (eg, feels rested after only 3 hours
of sleep)
3) More talkative than usual or pressure to keep talking
4) Flight of ideas or subjective experience that thoughts are
racing
5) Distractibility (ie, attention too easily drawn to
unimportant or irrelevant external stimuli)
6) Increase in goal-directed activity (either socially, at work
or school, or sexually) or psychomotoragitation
7) Excessive involvement in pleasurable activities that have a
high potential for painful consequences(eg, engaging in
unrestrained buying sprees, sexual indiscretions, or foolish
business investments)
C. The symptoms do not meet criteria for a mixed episode.
D. The mood disturbance 1) is sufficiently severe to cause
marked impairment in occupationalfunctioning, usual social
activities, or relationships with others, 2) necessitates
hospitalization toprevent harm to self or others, or 3) has
psychotic features.
E. The symptoms are not due to the direct physiological effects
of a substance (eg, a drug of abuse, a medication, or other
treatment) or a general medical condition (eg,
hyperthyroidism).
Reprinted with permission from the Diagnostic and Statistical
Manual of Mental Disorders, Text Revision,Fourth Edition (Copyright
2000). American Psychiatric Association.
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
e 16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
15/16
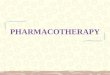
DSM-IV-TR diagnostic criteria for hypomania
A. A distinct period of persistently elevated, expansive, or irr
itable mood, lasting at least 4 days,that is clearly different from
the usual nondepressed mood.
B. During the period of mood disturbance, three (or more) of the
following symptoms havepersisted (four if the mood is only
irritable) and have been present to a significant degree:
1) Inflated self-esteem or grandiosity
2) Decreased need for sleep (eg, feels rested after only 3 hours
of sleep)
3) More talkative than usual or pressure to keep talking
4) Flight of ideas or subjective experience that thoughts are
racing
5) Distractibility (ie, attention too easily drawn to
unimportant or irrelevant external stimuli)
6) Increase in goal-directed activity (either socially, at work
or school, or sexually) or psychomotoragitation
7) Excessive involvement in pleasurable activities that have a
high potential for painful consequences(eg, engaging in
unrestrained buying sprees, sexual indiscretions, or foolish
business investments)
C. The episode is associated with an unequivocal change in
functioning that is uncharacteristic of
the person when not symptomatic.
D. The disturbance in mood and the change in functioning are
observable by others.
E. The episode 1) is not severe enough to cause marked
impairment in social or occupationalfunctioning, 2) does not
necessitate hospitalization, and 3) does not have psychotic
features.
F. The symptoms are not due to the direct physiological effects
of a substance (eg, a drug of abuse, a medication, or other
treatment) or a general medical condition (eg,
hyperthyroidism).
Note : Hypomanic-like episodes that are clearly caused by
somatic antidepressant treatment (eg,medication, ECT, light
therapy) should not count toward a diagnosis of bipolar II
disorder.
Reprinted with permission from the Diagnostic and Statistical
Manual of Mental Disorders, Text Revision,Fourth Edition (Copyright
2000). American Psychiatric Association.
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...
e 16 02/12/2013 04:38
-
8/13/2019 Bipolar disorder in adults - Pharmacotherapy for acute
mania, mixed episodes, and hypomania.pdf
16/16
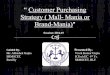
DSM-IV-TR diagnostic criteria for major depression
A. Five (or more) of the following symptoms have been present
during the same 2-weekperiod, and represent a change from previous
functioning. At least one of the symptoms is eitherdepressed mood
or loss of interest or pleasure.
(Note: Do not include symptoms that are clearly due to a general
medical condition, ormood-incongruent delusions or
hallucinations.)
Depressed mood most of the day, nearly every day (or
alternatively can be irritable mood in childrenand adolescents)
Markedly diminished interest or pleasure in all, or almost all,
activities, nearly every day
Significant weight loss while not dieting, weight gain, or
decrease or increase in appetite
Insomnia or hypersomnia nearly every day
Psychomotor agitat ion or retardation nearly every day
Fatigue or loss of energy nearly every day
Feelings of worthlessness or excessive or inappropriate guilt
nearly every day
Diminished ability to think or concentrate, or indecisiveness,
nearly every day
Recurrent thoughts of death (not just fear of dying), recurrent
suicidal ideation without a specificplan, or a suicide attempt or a
specific plan for committing suicide
B. The symptoms do not meet criteria for a Mixed Episode.
C. The symptoms cause clinically significant distress or
impairment in social, occupational, or otherimportant areas of
functioning.
D. The symptoms are not due to the direct physiological effects
of substance or a general medicalcondition.
E. The symptoms are not better accounted for by Bereavement, ie,
after the loss of a loved one,the symptoms persist for longer than
two months or are characterized by marked functional
impairment, morbid preoccupation with worthlessness, suicidal
ideation, psychotic symptoms, orpsychomotor retardation.
Adapted from American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders, 4thed, Text Revision.
American Psychiatric Association, Washington, DC 2000.
lar disorder in adults: Pharmacotherapy for acute mania, mixed
epi...
http://www.uptodate.com/contents/bipolar-disorder-in-adults-pharmaco...