Embed Size (px)
Citation preview

Arrhythmias
RVS Chaitanya koppala

Normal cardiac electrophysiology• Normal cardiac rhythm, sinus rhythm is characterized by contraction
of first atria and ventricles (Systole) followed by relaxation (diastole) during with the heart fill with blood before the next cardiac cycle begins• Above mention sequence is maintained by electrical activity of heart’s• Myocytes are electrically active and capable of generating action
potential.• Adjacent myocytes form the connections with the adjacent myocytes
through channels / protein channels called gap junctions

Cardiac action potential• Understanding of ionic basis of the cardiac action potential is
important (?)• Inherited abnormalities of ion channels functions (channelopathies)
are an important cause of sudden cardiac death (?)• Phospholipid membrane of the cardiac myocytes is spanned by
numerous proteins = ion channels• Permeablility to specific ions= diastolic depolarization + resting
membrane potential+ pacemaker activity + action potentials

• Resting membrane potential is -60 to -90 mV (more intracellular than extracellular (?) bcz of Na+/k+ - ATPase • Which pumps K+ ions into cell in exchange for Na+ ions,• Pumps K+ ions out of the cell with unaccompanied by anions resulting
in the net loss of charge and thus a negative resting/ diastolic/phase 4• Specialised myocytes form the cardiac conduction system and these
cell have pacemaker activity• Influenced by sympathetic nervous system ( Camp) and
parasympathetic nervous system by circulating catecholamines


RefractorinessAction potential of cardiac myocytes differs from that seen in nerve cells by the presence of a plateau phase (myocyte is inexictable and refractory)The time interval b/n the onset of the action potential and the regaining of the electrical excitability is known as the refractory period“Drugs that prolong the action potential duration (APD) prolong the refractory period”

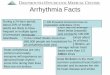
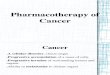
Normal cardiac conduction

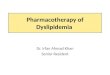
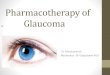
Normal electrocardiogram (ECG)

Arrhythmia mechanismsCauses
• Abnormal impulse formation
• Abnormal impulse propagation

Abnormal impulse formation Abnormal automaticity:Another term for pacemaker activityRate of firing of pacemaker is largely determined by the duration of
the phase 4 (?)PHASE 4: determined by
1. Max diastolic potential following repolarisation of preceeding AP2. Slope of the diastolic depolarization (pacemaker currents)3. Threshold potential for generation of a new action


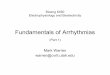
Trigger activity• Describes impulse formation dependent upon after depolarization • EADs (During phase 2/3)• DADs (During Phase 4)• In both cases after depolarization may reach the threshold potential
required for generation of a new action potentialEADs DADs
Congenital and acquired long QT syndromes Reperfusion following ischaemia, heart failure, digitalis toxicity and catecholamine
polymorphic VTProlonged APD promotes reactivation of the
inward calcium currents Spontaneous release of calcium in burst by
Sarcoplasmic reticulumActivation of Na+/Ca2+ EXCHANGER


Abnormal impulse propagation Re-entry: many clinically arrhythmias are due to re- entry in which an activation wave front rotates continuously around a circuitPrecise set of electrophysiological conditions must be met in order for re – entry to occur1. premature beat must encounter unidirectional condition2.Central non conducting obstacle around which re entry circuit develops3. Conduction proceed slowly enough down the other limb4. Circulating wave front activation must continue to encounter electrically excitable tissue


Clinical problems
Patients with cardiac arrhythmia may present with a number of symptomsPalpitations Sudden drop in cardiac outputSinus tachycardia Dizziness, syncope, sudden deathReduced cardiac output Atrial tachyarrhythmias/ flutterReduced exercise capacity Atrial fibrillation BreathlessnessFatigueAnginaMyocardial infarction

Arrhythmias may aggravate heart failure in two ways:
1. Haemodynamic effect of the arrhythmia (heart failure or aggravate existing heart failure)
2. Prolonged tachycardia or any type may lead to (tachycardia induced cardiomyopathy)

Diagnosis
1. DETAILED HISTORY SHOULD BE OBTAINED2. HISTORY OF CARDIAC DISEASE3. OTHER DIAGNOSED MEDICAL CONDITION 4. A FULL DRUG HISTORY (Both OTC/Rx)5. A FAMILY HISTORY OF HEART FAILURE 6. A FAMILY HISTORY OF SUDDEN DEATH

Mandatory investigation includes
1.12-LEAD ECG2. ECHOCARDIOGRAM3.AMBULATORY ECG (recording for up to 7days)4. Infrequent symptoms an event recorder, ECG strips, Insertable loop recorder

Management
• Pathological tachycardia is conventionally defined as resting heart rate over 100/min• Classified as two types
1. SVT (?)2. VT(?)

SVTINAPPROPRIATE SINUS TACHYCARDIA
12 LEAD ECG, AMBULATORY ECG, ECHO CARDIOGRAPHY
Beta blockers, verapamil, ivaradine
ATRIAL FLUTTER Right atrial tachycardia with re entry ( 300/min) 1:2 ratio av conduction
Beta blocker, verapamil, diltiazem and digoxin,1:1- sotalol, amiodarone
FOCAL ATRIAL TACHYCARDIA Uncommon arrhythmia discharge of focal source within the atria and surrounding venous structures
Adenosine, class ic, 1:1 av conduction,
JUNCTIONAL RE ENTRY TACHYCARDIA
SVT Used to explain JRTTWO TYPEAVNRTAVRT
Intravenous adenosine 12 mgIntravenous verapamil 5 mgProphylactic drugs: Beta blockers, verapamil, flecainide and sotalol


Atrial fibrillation :• Most common sustained arrhythmia• Classified as:
1. Paroxysmal – episodes of AF lasting no more than 7days2. Persistent- more than 7days3. Longstanding persistant – more than 7 year4. Permanent- no decision has been made not to attempt cure of persistant AF
Therapy5. ANTICOAGULANT THERAPY6. INTRAVENOUS Beta blockers, verapamil and digoxin7. Several class I (sotalol and amiodarone)8. Class Ic flecainide and class III amiodarone