Embed Size (px)
Citation preview

Pharmacotherapy of
Malaria
RVS Chaitanya Koppala

Introduction• Malaria is a tropic life threatening disease.• A disease caused by members of the protozoan
genus Plasmodium, a widespread group of sporozoans that pasitize the human liver and red blood cells.
• Humans are infected with Plasmodium protozoa when bitten by an infective female Anopheles mosquito vector.
• Symptoms may appear within weeks to months or even years.• There are 4 species:
– plasmodium falciparum– plasmodium vivax– plasmodium ovale– plasmodium malariae

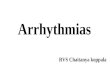
Malaria Transmission Cycle
Parasite undergoes sexual reproduction in the mosquito
Some merozoites differentiate into male or female gametocyctes
Erythrocytic Cycle: Merozoites infect red blood cells to form schizonts
Dormant liver stages (hypnozoites) of P. vivax and P. ovale
Exo-erythrocytic (hepatic) Cycle: Sporozoites infect liver cells and develop into schizonts, which release merozoites into the blood
MOSQUITO HUMAN
Sporozoites injected into human host during blood meal
Parasites mature in mosquito midgut and migrate to salivary glands


Who is at risk?• young children• pregnant women• people with HIV/AIDS• international travelers from non-endemic areas • immigrants from endemic areas and their children

uncomplicated malaria
in special groups (young children, pregnant women, HIV /AIDS)
in travellers (from non-malaria endemic regions)in epidemics and complex emergency situations
4 | Guidelines for the Treatment of Malaria
severe malaria
Clinical features and classification of malaria

UNCOMPLICATED MALARIA (all species) – Uncomplicated malaria definition:
Fever and any of the following: • Headache,• Body and joint pains• Feeling cold and sometimes shivering• Loss of appetite and sometimes abdominal pains• Diarrhoea, nausea and vomiting.• Hepatospleenomegaly

SEVERE COMPLICATED MALARIA
Alteration in the level of consciousness (ranging from drowsiness to deep coma)Cerebral malaria (unrousable coma not attributable to any other cause in a patient
with falciparum malaria)Respiratory distress (acidotic breathing)Multiple generalized convulsions (2 or more episodes within a 24 hour period)Shock (circulatory collapse, septicaemia)Pulmonary oedemaAbnormal bleeding JaundiceAcute renal failure - presenting as oliguria or anuriaSevere anaemia (Haemoglobin < 5 )High fever
Confusion, or drowsiness with extreme weakness.In addition, the following may develop:
defined as the detection of P. falciparum in the peripheral blood

Guidelines for the Treatment of Malaria
Malaria Diagnosis
• All clinically suspected malaria cases require laboratory examination and confirmation.
• Only in case where laboratory confirmation is not possible start treatment immediately.
• Parasitological confirmation is done by thin-thick blood smear microscopy examination or by dipstick (Rapid Diagnostic Test [RDT]).

Differential diagnosis for uncomplicated malaria
Consider other illnesses, such as:• Upper respiratory tract infection
(Pharyngitis, tonsillitis, ear infection), pneumonia , measles, dengue, influenza, typhoid fever.
Remember that the patient may be sufferingfrom more than one illness.

THE PHARMACOLOGY OF ANTIMALARIALS
Class Definition Examples
Class Definition Examples Class Definition Examples
Blood schizonticidal drugs
Act on (erythrocytic) stage of the parasite thereby terminating clinical illness
Quinine, artemisinins, amodiaquine, chloroquine, lumefantrine, tetracyclinea , atovaquone, sulphadoxine, clindamycina , proguanila
Tissue schizonticidal drugs
Act on primary tissue forms of plasmodia which initiate the erythrocytic stage. They block furtherdevelopment of theinfection
Primaquine, pyrimethamine,proguanil, tetracycline
Gametocytocidal drugs
Destroy sexual forms of theparasite thereby preventing transmission of infection tomosquitoes
Primaquine, artemisinins,quinineb
a Slow acting, cannot be used alone to avert clinical symptomsb Weakly gametocytocidal

THE PHARMACOLOGY OF ANTIMALARIALS (cont.)
Class Definition Examples
Class Definition Examples Class Definition Examples
Hypnozoitocidal drugs These act on persistentliver stages of P.ovaleand P.vivax which causerecurrent illness
Primaquine, tafenoquine
Sporozontocidal drugs These act by affectingfurther development ofgametocytes into oocyteswithin the mosquito thusabating transmission
Primaquine, proguanil,chlorguanil


1. Treatment of severe falciparum malaria
Preferred regime Alternative regime
IV Artesunate (60mg): 2.4mg/kg on admission, followed by 2.4mg/kg at 12h & 24h, then once daily for 7 days.
Once the patient can tolerate oral therapy, treatment should be switched to a complete dosage of Riamet (artemether/lumefantrine) for 3 day.
IV Quinine loading 7mg salt /kg over 1hr followed by infusion quinine 10mg salt/kg over 4 hrs, then 10mg salt/kg Q8H or IV Quinine 20mg/kg over 4 hrs, then 10mg/kg Q8H.PlusAdult & child >8yrs old: Doxycycline (3.5mg/kg once daily)or Pregnant women & child < 8yrs old: Clindamycin (10mg/kg twice daily). Both drug can be given for 7 days.

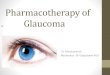
2. Treatment of uncomplicated p.falciparum

4. Treatment of of malaria caused by p.vivax, p. ovale or p. malariae.
CHLOROQUINE(150 mg base/tab) 25 mg base/kg
divided over 3 days
PRIMAQUINE(7.5 mg base/tab)
Day 1 Day 2 Day 3 Start concurrently with CHLOROQUINE 0.5 mg base/kg Q24H for 2 weeksTake with foodCheck G6PD status before start primaquineIn mild-to-moderate G6PD deficiency, primaquine 0.75 mg base/kg body weight given once a week for 8 weeks. In severe G6PD deficiency, primaquine is contraindicated and should not be used.
10mg base/kg
stat, then 5mg
base/kg
5mg base/kg
Q24H
5mg base/kg Q24H
1 tab of chloroquine phosphate 250mg equivalent to 150mg base. Calculation of dose for chloroquine is based on BASE, not SALT form. 1 tab of primaquine phosphate contains 7.5mg base.

Immediate clinical management of severe manifestations and complications of P. falciparum
malariaDefinitive clinical features Immediate management/treatmentCome (Cerebral malaria) Monitor & record coma scale, temperature, respiratory, and
depth, BP and vital signs.
Hyperpyrexia (rectal body temperature >40°C)
sponging, fanning &with an antipyretic drug.Rectal paracetamol is preferred
Convulsions A slow IV injection of diazepam(0.15mg/kg, maximum 20mg for adults).
Hypoglycaemia (glucose conc. <2.8mmol/L)
Correct with 50% dextrose (as infusion fluids). Check blood glucose Q4-6H in the first 48hrs.
Severe anaemia (hb < 7g/dl)
Transfuse with packed cells. Monitor carefully to avoid fluid overload. Give small IV dose of frusemide
Acute pulmonary oedema Prop patient upright (45°), give oxygen, give IV diuretic ,stop intravenous fluids. Early mechanical ventilation should be considered.

Monitoring & follow-up• Blood smear should be repeated daily
(twice daily in severe infection). Within 48-72 hr after start of treatment, patients usually improve clinically except in complicated cases.
• All patients should be investigated with repeated blood film of malarial parasite one month upon recovery of malarial infection, to ensure no recrudescence.

Prevention
•Avoid mosquito bites:Wearing long sleeves, trousers.Insecticide Treated BednetsRepellent creams or sprays.

Chemoprophylaxis• Indicated for travellers travel to
endemic areas• Mefloquinine 250mg weekly (up to 1
year) or doxycycline 100mg daily (up to 3 month), to start 1 week before and continue till 4 weeks after leaving the area.

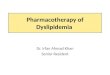
Dosing schedule for doxycycline
Weight in kg Age in years No of tablets< 25 < 8 Contraindicated25 - 35 8 - 10 ½36 - 50 11 - 13 ¾50+ 14+ 1