Embed Size (px)
Citation preview

What Do We Know about theGroup of Mental IMsorders
CaMed SChfZO@Wf$E?
Part 2: Dfagnods and Treatment
Number 27
In the first part of this essay, 1 I re-viewed several current theories on thecauses of schizophrenia. Schizophreniais one of the psychoses, or major mentalillnesses involving disordered thoughts,emotions, and behavior. About ten mil-lion people worldwide suffer fromschwphrenia, and between one and twopercent of the US population will be di-
agnosed as schizophrenic in their life-times. Despite its prevalence and morethan 50 years of intensive research,schizophrenia stilf is a poorly under-stood disease.
Part of the problem is that “schizo-
phrenia,” Iiie “cancer,” denotes a groupof diseases, each of which may have dif-ferent causes and outcomes. Research-
ers and clinicians have defined various
criteria for diagnosing schizophrenia,but they differ on exactly what symp-toms are more or less relevant to thedisease. An individual might be labeledschwphrenic according to one diagnos-tic system, but not according to another.
This confusion frustrates the efforts ofscientists studying schizophrenic pa-
tients. Experimental results reported on
one group of schizophrenics may be dif-ficult to confirm in another group diag-nosed according to a different system.Disagreements on diagnosis also compli-
cate the clinician’s decision on how totreat schizophrenics. For example, adrug therapy successful in treating somepatients may be ineffective in others.Many of the drugs used to treat this dis-
luiv4,1983,,
ease have serious side effects, and theyshould be prescribed only for those whowill benefit. In thk essay, I’lf discuss howschizophrenia is diagnosed and treated.
Current diagnostic views of schizo-phrenia are based on the work of twoEuropean psychiatrists in the early1900s, Emil Kraepelin, a German psy-chiatrist, considered the following to be
characteristic symptoms of schizophre-
nia: lack of insight, emotion, and will;confusion; loosening of associations; de-teriorated mental ability; hallucinations;delusions; and disturbed motor func-tioning, or catatonia. He also stressed aprogressive deterioration, or “demen-
tia,” as central to the disease process. z-4Eugen Bleuler, a Swiss psychiatrist,
agreed with Kraepelin that loosening of
associations and the “splitting” inthought processes and emotions fromreality were primary symptoms of
schizophrenia. But he regarded halluci;nations, delusions, negativism, and cat a-tonia as subordinate symptoms that werenot necessary for a diagnosis of schizo-phrenia. He also rejected any consider-
ation of the outcome of the disease-not
all schizophrenics were inevitably de-mented, in his experience. z-A
Current diagnostic criteria carry on
the Kraepelin-Bleuler debate as towhich symptoms are primary to schizo-phrenia, and whether or not to take intoaccount the course of the illness. Diag-noses based only on the present mentalstatus of the patient are called “cross-
204
sectional. ” Those that also take into ac-count the course of the illness and otherfactors, such as family history and thepatient’s condition before the onset ofschizophrenia, are called “longitudinal”diagnoses.s
In 1959, Kurt Schneider, a Germanpsychiatrist, provided the fmt set ofdetailed symptoms on which to make across-sectional diagnosis of schizophre-nia. He described 11 “first rank symp-toms” (FRS), any one of which was suffi-cient for diagnosing a patient as schizo-phrenic in the absence of neurologicaldkorders, such as retardation or braindisease.b The fmt three deal with audi-tory hallucinations: voices repeat or an-ticipate the patient’s private thoughts;they d~cuss or argue about the patient;or they keep up a running commentaryon the patient’s actions. Three moresymptoms involve bizarre thinking: thebelief that one’s thoughts are removedby some outside force; that one’s
thoughts are magically broadcast forothers to hear; and that thoughts areforcibly inserted into the patient’s mind.Another three symptoms relate to thepatient’s experience of his or her feel-ings, acts, and impulses being under thecontrol of some external agency, as if thepatient were a robot or hypnotized. The
patient also feels that he or she is a pas-sive recipient of various sensations—heat, touch, or movement—imposed byoutside forces. Finally, the patient’sperceptions are deluded—what wewould perceive as commonplace occur-rences, the schizophrenic interprets ashaving a very special or profound per-sonal significance .2)4
Schneider’s FRS are still regarded by
many clinicians as the definitive criteriafor making a diagnosis of schizophrenia.They are commonly used in Europe, andhad a significant impact on British re-searchers and c~lcians in particular.TBut studies show that FRS occur in
about 50 percent of clinically diagnosedschiiplu-enics. That is, half of the pa-tients labeled schizophrenic do not showany FRS. Also, FRS occur in other psy-chiatric disorders, especially mania, sothey are not exclusive to schizophrenias
Other cross-sectional diagnosticsystems are more or less based onSchneider’s FRS, but they include othersymptoms as well. For example, the NewHaven Schizophrenia Index (NHSI),Sdeveloped in 1972 by B .M. Astrachanand colleagues, Yale University, NewHaven, Connecticut, lists more than 20symptoms, including visual hallucina-
tions, confusion, catatonia, suspicious-ness, and other paranoid signs. The flex-ible system,g designed in 1973 by W .T.Carpenter and J.S. Strauss, National In-stitute of Mental Health (NIMH), Be-thesda, Maryland, itemizes 12 relevantsymptoms of schizophrenia, includingpoor rapport and insight, incoherentspeech, and absence of early waking,
elation, and depression. The presence ofeither five or six symptoms are necessaryfor a diagnosis of schizophrenia with theflexible system. The CATEGO system, 10a computer program used to processdata from the Present State Examina-tion, 11was developed by J.K. Wing andcolleagues, Medical Research Council,London, in 1974. It allows for sirseparate diagnoses: definite or uncertainschizophrenia; defiiite or uncertain
paranoia; and definite or uncertain“other” psychoses, such as simple and
catatonic schizophrenia.At the same time that these cross-
sectional diagnostic systems were evolv-ing, other researchers and cliniciansdeveloped a longitudinal approach. Jnaddkion to considering present symp-
toms, they examined the patient’s past
h~tory-whether or not other relativeswere schizophrenic, the patient’s workor school performance before the onsetof the disease, the age at onset and dura-
205
tion of the illness, and so on. Their goalwas to distinguish between “true” or
chronic schizophrenics and patientswith an acute form of the disease.Chronic schizophrenics, who developsymptoms earlier in life and over alonger pefiod of time, have a poor prog-nosis. That is, there is little chance that
they will recover. But acute schizo-
phrenics, who develop symptoms sud-denly, often recover spontaneously.
The Diagnostic and Statistical Manualof Mental Disorders (DSM-IID~2 is themost current example of a longitudinaldiagnostic system. DSM-IIIis a standardreference work in the US, and was pub-
lished in 1980 by the American PsychLatric Association. It evolved from twoearlier longitudinal diagnostic criteria:the Feighner criteria, IS defined in 1972by J.P. Feighner and colleagues, Wash-ington University, St. Louis, MKsoun;and the research diagnostic criteria(RDC), 14 developed in 1975 by R.L.Spitzer and colleagues, NIMH.
DSM-111 draws a distinction betweenthree classes of symptoms. “Prodromal”
symptoms may develop before the onsetof schizophrenia. They indicate that theindividual’s previous level of functioningis deteriorating-social withdrawal, per-sonalityy changes, eccentric behavior,neglected hygiene and grooming, and di-minished performance at work or schoolare listed as prodromal symptoms inDSM-IZI.59159lb
“Active” symptoms indicate the psy-
chotic phase of schizophrenia. Again,they are derived from Schneider’sFRS—delusions, hallucinations, andthought disorders. Any one of thesesymptoms is necessary for a diagnosis,but thought disorders alone are not suffi-cient. Thought disorders-incoherence,loose associations, and poverty ofspeech, for example—must occur with
delusions or hallucinations, catatonic
behavior, or flat or inappropriate emo-
tions for a DSM-111 diagnosis of schizo-phrenia.s,lslb
“Residual” symptoms may persist af-ter the active phase of schizophrenia.They are similar to the prodromal symp-toms, but emotional flattening and im-paired role functioning are more com-
mon in the residual phase.In addition to these symptoms, DSM-
111 requires several longitudinal factors:onset before age 45 and continuous ill-ness for at least six months, for example.Also, a diagnosis of schwophrenia is notatlowed if the patient has a history ofmanic or depressive disorders, or braindisease and retardation.
As you can see, there is considerable
room for disagreement on exactly whatschwphrenia is and how it can be diag-nosed. I should point out that I haven’tdiscussed several other diagnosticsystems for reasons of space-those ofG. LangfeldtlT and M.A. Taylor and R.Abrams, @ for example. But there is noreason to believe that any one system is“better” than another.s The situation
would be considerably improved if diag-
noses were based on biological “mark-ers” of schizophrenia. 15In Part 1 of thisessay, I reviewed current research onseveral biological causes of the dis-ease-hypersensitive dopamine recep-tors, structural and physiological abnor-malities in the brain, and so on. Re-searchers and clinicians may eventuallybe able to diagnose subtypes of schizo-phrenia according to these biological
factors.The vast majority of patients diag-
nosed as schmphrenic are treated witha group of drugs called “neuroleptics.” Itis important to understand that neuro-Ieptics do not cure schizophrenia. Theysimply reduce the more obvious symp-toms—hallucinations, paranoid behav-ior, agitation, combativeness, sleep
disturbance, and soon, But neuroleptics
have little or no effect on other symp-
toms—impaired judgment, withdrawal,lack of insight, and poor motivation, forexample. In addition, neuroleptic drugsreduce the risk of relapse. Two out ofthree patients who discontinue drug usereexperience schmphrenic episodeswithin one year. Drug maintenance re-duces the relapse rate to between 20 and30 percent. 19
There are five categories of neurolep-tics, classed by chemical structure. Thephenothiazines include chlorpromazine,marketed under the trade name Thora-zine; triflupromazine or Vesprin; meso-ridazine or Serentil; thioridazine or Mel-laril; fluphenazine or Prolixii and Per-mitil; perphenazine or Trilafon; and tri-fluoperazine or St elazine. Anothergroup, the thloxanthenes, includeschlorprothixene or Taractan, and thlo-thixene or Navane. Loxapine, marketedas Loxitane and Daxolin, is a dlbenzox-azepine. Haloperidol, or HaIdol, is a
butyrophenone. Finally, moliidone, orMoban, is an indole.m
The neuroleptics differ in their poten-cy, or the dose required to have an effecton schizophrenic symptoms. High po-tency drugs, such as Haldol, Prolixin,Stelazine, and Moban, are prescribed inlow doses. Thorazine, Mellaril, Tarac-tan, and other low potency drugs aregiven in higher doses. The high potencydrugs are not more effective or fasteracting than low potency agents—theygive comparable clinical results, but
with fewer milligrams per dose. Typical-ly, it takes between ten days and twoweeks for the neuroleptics to show ther-
apeutic results, but some schizophrenicsrespond within two or three days. 19
AS with any oral medication in tabletor liquid form, there is the risk that pa-tients will not comply with the doctor’sprescription. I’ve discussed patient non-compliance in a separate essay.zl
Among schizophrenics in hospitals, non-compliance has been estimated at about
20 percent. For schizophrenic outpa-
tients, it increases to between 40 and 70percent. Injectable long-acting neuro-leptics have been developed to treatnoncompliant schizophrenics. For ex-ample, fluphenazine decanoate injec-tions have a duration of action betweenthree and four weeks. 19
While neuroleptics are very effectivein treating schizophrenic symptoms,
they have unpleasant side effects forsome patients which contribute to non-compliance. Before I discuss these sideeffects, let me point out that most re-searchers and clinicians consider theneuroleptics to be no more “dangerous”than other drugs used to treat physicaldisorders in general medical practice.Afso, not alf schizophrenics on neuro-Ieptic therapies suffer side effects. Thebenefits of neuroleptics in treatingsymptoms of schizophrenia usually out-weigh their side effects.
The short-term side effects of neuro-leptic drugs include urinary hesitation,constipation, blurred vision, dry mouth,decreased blood pressure, and exacer-bation of glaucoma. Thus, elderly pa-tients and those with heart dkease aremore vulnerable to these side ef-fectso19.22
Neuroleptic drugs also have long-termside effects for some patients that aredisabling, sometimes irreversible, andeven fatal. Soon after the neurolepticswere introduced in 1952, clirdcians ob-served odd jaw movements, grimacing,and other “dyskinetic” movements in theoral region of some schizophrenic pa-tients.~ In 1%0, this syndrome wasnamed “tardive dyskinesia,”zg and it hasproved to be the most frequent andfeared of long-term risks of neurolepticdrug therapy.zz
The cliiical signs of tardhe dyskinesiainclude sucking or smacking of the lips,moving the jaw from side to side, puffingout the cheeks, and occasionally thrust-
ing the tongue out of the mouth, In addi-
tion, jerking movements of the arms and
207
extremities, contractions of the neckand back, and writhhg movements ofthe fingers, toes, or ankles are ob-
served.19,22,25 These involuntary andgrotesque movements obviously are asource of distress and embarrassmentfor schizophrenics, and they may decide
to stop taking the medications that causethem.zs
Tardive dyskinesia usualy appearsabout two years after drug treatment isstarted, but the syndrome can occurwitiin three months. Only about 20 per-
cent of older, chronic patients with along’ hktory of neuroleptic medicationare afflicted. The incidence is muchlower in younger, acute schizophren-ics. 1g It is most frequentf y observed inefderly females, in particular those witha history of brain disease.zs When drugsare discontinued, tardive dyskinesia isreversed in about 30 percent of pa-
tients.lgPseudoparkinsonism is another long-
term side effect that appears weeks ormonths after the start of drug therapy,most frequently in elderly females, Thesymptoms are muscle fatigue and weak-ness, tremor in the hands and fingers,rigidity, drooling, and heat intolerance.Ahnost alf cases of pseudoparkinsonismremit within a month or two after medi-
cation is discontinued.zsAkathfiia often occurs in combination
with pseudoparkinsonism, but this long-term side effect can occur alone. It ismarked by the inability to sit still-rest-less movements, rocking back and forthwhile standing, and tapping the feetwhiie sitting are observable severalweeks or months after drug therapy be-
gins. Again, akathisic symptoms disap-pear after drug therapy is stopped.zs
Acute dystonic reactions most fre-quently afflict children and youngadults, especially males, within three
days after drug therapy is started.Dystonic means abnormal muscle ten-sion—the patient suffers spasms of the
face and throat muscles, curling andsticking out the tongue, grimacing andother facial distortions, and unusual pos-turing of the head, neck, and jaw. In ad-dition, the patient’s eyes may be fixed inan upward gaze. These symptoms comeand go while drug therapy continues,but they remit about a week after drugsare stopped.zs
The neuroleptic malignant syndrome(NMS), a potentially lethal and rarecomplication, was first noticed in 1960.The symptoms are apparent anywherefrom a few hours to several months afterneuroleptic therapy begins. Once itstarts, NMS develops very rapidly overthe next 24 to 72 hours. The symptomsare rigidity and akinesia, elevatedtemperatures as high as 110-20 degreesFahrenheit, stupor and coma, rapidheartbeat, unstable blood pressure, andperspiration. Young adult males are pre-
dominantly affected, but NMS can strike
patients of alf ages and either sex.zbOnly 60 cases of NMS have been doc-
umented in the literature. Of these, 12patients died. The fatalities resultedfrom respiratory or kidney failure andcardiovascular collapse, and they oc-curred from three to 30 days after the
onset of symptoms. The patient recoversabout a week after drugs are discontin-
ued, or two to three weeks later if long-acting injectable neuroleptics were pre-scribed. Interestingly, some patientswere treated with drugs on several dif-ferent occasions before NMS devel-oped. Also, NMS sometimes does notrecur after drug therapy is restarted.Thus, neuroleptics alone are not suffi-cient to trigger NMS. The patient’s state
of health at the time of medication mayhave considerable impact on the onset ofNMS.26
The long-term side effects of neuro-leptic drugs make it desirable to developalternative treatment strategies. Also,you should remember that 25 percent ofschizophrenics do not respond to neuro-
208
leptics.zT Propranolol, a drug used totreat high blood pressure and migraineheadaches, has been used in combina-tion with the neuroleptic chlorprorna-
zinc.n But more controlled studies onlarger populations of schizophrenics areneeded to test the efficacy of pro-pranolol, and to see what its long-termside effects are.
Lithium is another drug used in com-bination with neuroleptics to treatschizophrenics who do not respond toneuroleptics alone. E. Fulfer Torrey, St.Elizabeth Hospital, Washington, DC,
says, “Lhhium is being used quite widelyas an ancillary drug in schizophrenia.Lithium is well established in the bipolar[depressions], but many are starting touse it on treatment resistant schizo-phrenics in conjunction with antipsy-chotics. Its use is spreading quite quick-ly.”zg I previously reviewed the liter-ature on lithium as a treatment for de-pression.~
1 should point out that large doses ofvitamins have been suggested as a treat-ment for schizophrenia for more than 20years now.gl.az But recent controlledstudies have not supported the claimsthat megavitamin therapy is useful intreating this dwease. Torrey concluded,“Unfortunately, this therapeutic regi-men has not been shown to be effectivein controlled studies of schizophrenics.It is possible that it maybe effective forsome subgroups, but no evidence hasbeen offered to date.”Jg
The endorphins also have been testedas a treatment for schizophrenia. Whenbeta-type endorphins were used onchronic schizophrenics, no clinically sig-ntilcant improvement in symptoms wasobserved.~ In fact, symptoms worsenedwhen beta-endorphin was tested on
acute schizophrenics.ss This finding sug-gests that too much of these opiates inthe brain might actually be a cause ofschizophrenia. Thus, reducing or block-ing the effects of endorphins might im-
prove symptoms. Several studies testedthe effects of naloxone, an opiate antag-onist, on schizophrenics. But the bal-ance of research results indicates thatnaloxone has little or no effect on thisdisease.Jb.BT I recently discussed nalox-
one in a separate essay on Jack Fishmanand Harold Blumberg, who won the1982 John Scott Award for their synthe-sis and investigation of this drug.~
More recently, gamma-type endor-phins were studied for their effects onschizophrenics who did not respond toneuroleptics. Half of the patients testedshowed clinical signs of improvement.
More intensive research on gamma-en-dorphins is needed. If it proves success-ful in treating some schizophrenics, thelack of side effects would give it a dis-tinct advantage over neuroleptic medi-cation.B9
Interestingly, research on endorphinsand schizophrenia has revived the con-troversial practice of treating psychiatricpatients with hemodialysis. Hemodialy-sis is used on patients whose kidneyshave failed in order to clear the blood oftoxic substances. In 1977, an endorphinwas reportedly found in excess amountsin the blood of schizophrenics.@ Thisfiiding, combined with anecdotal evi-dence that schizophrenic symptoms im-proved after hemodialysis, suggestedthat dialysis might be a useful treatmentstrategy .41 But recent controlled studieshave shown dialysis to be ineffective intreating schizophrenia .4z-44
One of the earlier treatments forschizophrenia was electroconvuktvetherapy (ECT). In fact, the first patienttreated with ECT, in 1938, was a schizo-phrenic.4s Chronic schizophrenics orpatients who have been ill for more thantwo years do not respond well to ECT.
However, acute schwphrenics, espe-cially those with catatonic symptoms,benefit from ECT—they are dischargedfrom the hospitrd earlier, and their self-care behavior improves. The number of
209
schizophrenics treated with ECT whoimprove has been reported at between40 and 80 percent. But relapse rates arehigh.ls.lb I’ve previously discussed theuse of ECT for schizophrenia and othermental dk.orders.qT
Like many patients with major psychi-atric disorders, schizophrenics are alsotreated with psychotherapy. Studiescomparing the effectiveness of psycho-therapy to other treatment strategiesshow that it is most useful in combina-tion with drugs and/or ECT. Schizo-phrenics treated with ECT, drugs alone,or drugs and psychotherapy spent lesstime in the hospital than those undergo-ing psychotherapy alone. Psychotherapydesigned to support and rehabilitate the
patient’s social skills was more effectivethan psychotherapy aimed at improvingthe patient’s insight and understandingof the psychodynamics of schizophre-nia.~
Other forms of “talk therapy” includethe schizophrenic’s family in the treat-ment plan. Family treatment programsevolved in response to research showingthat stress in the home environment in-creases the rate of relapse in patients.Family members who have to cope with
the emotional demands of dealing with asch~ophrenic relative can be critical of,and hostile toward, the patient. Or theyfeel somehow guilty for the patient’scondition and are overanxious and pro-tective of the schizophrenic. About 50percent of patients who return to “high-stress” home environments relapse with-
in the year. The relapse rates improve
significantly when patients continue tak-ing medication and spend less time withhigh-stress family members.qg
However, spending less time with crit-ical or emotionally overinvolved familymembers often is not a practical alterna-tive for the schizophrenic. Thus, re-searchers have tried to reduce the stresslevels in the home environment through
family counseling. The program involves
educating the patient and Iamdy aboutschizophrenia and the use of medica-tions. They are also trained in variousmethods of problem solving. For exam-ple, the family learns to be more positiveand less critical of the patient. They arealso taught various strategies to copewith difficult situations as they arise. In
addition, the patient is encouraged tobecome more independent of the family,and to develop and maintain social skillsand outside interests. ~
Studies show that family treatmentplans are a successful therapeutic ap-proach to schizophrenia. Relapse ratesare significantly reduced, as are thenumber of days spent in the hospital.Also, better compliance with drug treat-ments is associated with family manage-ment.sl,sz
Unfortunately, not all families ofschizophrenics are willing to accept thepatient after he or she is discharged fromthe hospital. Some schizophrenics sim-ply may not have a family to return to.The problem of where to place schizo-phrenic patients has become a majorconcern over the last two decades. Shcethe early 1960s, state mental hospitals inthe US have discharged hundreds ofthousands of psychiatric patients. Partof the reason is due to the introductionof the neuroleptic drugs. Since theytreated the symptoms so dramatically, itwas felt that the patient’s life would beimproved if he or she returned to thecommunity instead of being confined tothe hospital ward.ss,sq
Also, there was growing pressure todevelop more humane community-based treatment programs. The spirit ofreform resulted in passage of the Com-munity Mental Health Centers Act in1963.55 Although the act made provi-sions for a network of counselig andoutpatient services, they were not fullyimplemented. Many mental patientswere simply “reinstitutionalized innursing homes, homes for the aged, or
210
“welfare hotels” in the poorest sectionsof the city. Medical and psychiatric carewas inadequate or nonexistent, and thedischarged mental patients often woundup on the streets.ss,~ I’ve d~cussed theincreasing phenomenon of street peopleand “bagladles” previously.%
In contrast, the Veterans Administra-tion (VA) hospitals began to place theirdischarged mental patients in “fosterhomes” in 1951. Foster homes are small,private family houses in which the pa-tient lives with at least one adult “spon-ser. ” The patients pay for their care andare treated as members of the family. So-cial workers periodically look in on pa-tients to make sure they are taking medi-cation and to monitor their progress.The VA has placed more than 60,000 pa-tients in foster homes since the programwas started, and about 12,000 patients
are currently in foster care .s7-59The relapse rate for schizophrenics in
foster care after one year is about 36 per-cent. Keep in mind that chronic schizo-phrenics treated with drugs have a re-lapse rate of about 45 percent one yearafter discharge. Researchers comparedrelapsed and nonrelapsed patients infoster care to see if they ddfered signifi-cantly on the kinds of activities they pur-sued. Nonrelapsed schizophrenics spent
more of theu time reading, working inthe garden or doing other outside activi-ties, and caring for chfldren. Relapsedpatients tended to watch more televisionand movies.5Q
Several characteristics of the fosterhome itself were found to have an im-
pact on relapse rates. Relapsed patientstended to come from larger foster homeswith more than ten people. These homes
also had more than two patients in fostercare. Relapse rates also were higher ifthe home had no children in the family.That is, the more the foster home resem-bled an institution rather than a familyenvironment, the higher the relapse
rates.ss,sg In addition, relapse rates werehigher when the sponsor initiated many
social activities, or when the patient wasclosely supervised by the sponsor or social worker. Thus, when the schizo-phrenic was treated more as a patientthan a family member, there was a great-er chance of deterioration and relapse.%
The VA foster care program is pat-terned after a form of treatment for thementally ill that dates back to the thir-teenth century in Gheel, Belgium. Ac-cording to tradition, the patron saint ofthe mentally disturbed, St. Dymphna,was murdered in Gheel by her father. In
response to this tragedy, the churchfounded an infiiary to treat the in-creasing number of mentally ill peoplewho made pilgrimages to her tomb insearch of a miraculous cure. When thenumber of patients overflowed thewards, the townspeople began to accept
them into their homes as members of thefamily.~
Today, patients are placed with fami-lies from similar social and economicbackgrounds. They are given their ownroom and have their meals at the familytable. No more than two patients areplaced in one home. They are free tocome and go as they liie, and can evenget a job. Many of the patients havebeen with their families for 20 or moreyears. The townspeople treat the men-tally ill as friends and neighbors. This isin contrast to most people in the US,who are suspicious or fearful of the men-tally ill and avoid contact with them.m
The most difficult task in successfullytreating schizophrenia may be to changeour attitudes toward the mentally ill.Several groups in the US have been or-ganized to improve the public image of
the mentally disturbed. In addition, theyhelp families cope with the pressures ofcaring for affficted relatives, advocatethe patients’ rights to treatment andsocial services, and lobby for more
211
research funds. Many of them are localor statewide organizations, while othershave joined to form national coalitions.
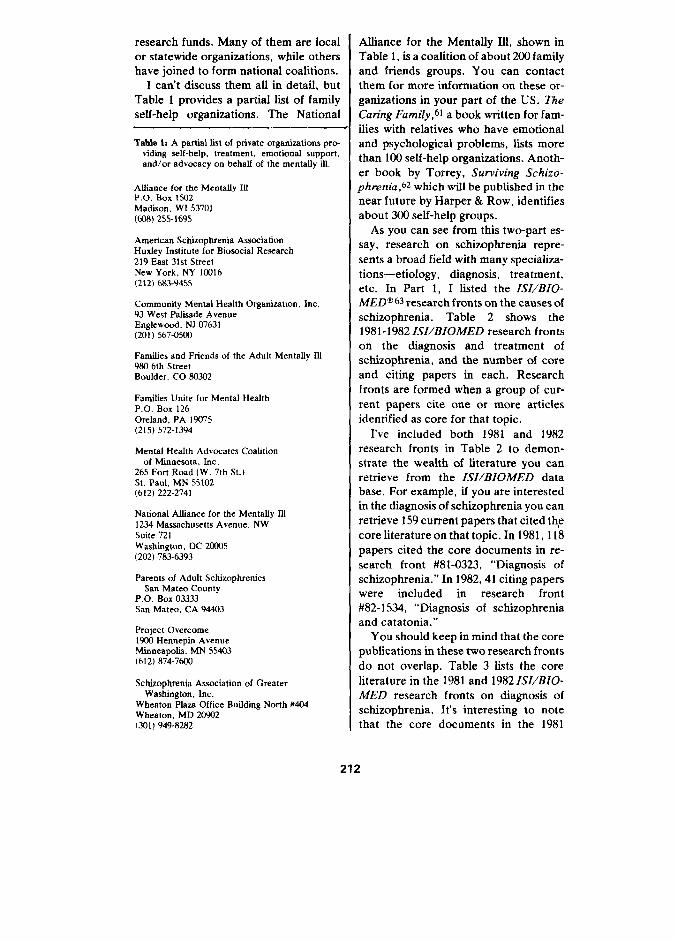
I can’t discuss them aU in detail, butTable 1 provides a partial list of familyself-help organizations. The National
Table I: A partial Sist of private organizations pro-viding self-help, treatment, emotional support,and/or advocacy on behalf of the mentalSy ill,
Affiance for the Mentaffy IllP.o. Box 1502Madison, WI 53701(tQ8) 255-1695
American Schizophrenia AssociationHuxfey fnstitute for Biosncial Research219 East 31st StreetNew York, NY 10316(212) 683-9455
Commurdty Mental Health Organization, Inc.93 West Pafiaade AvenueEnglewood, NJ 07631(20 1) 567-0503
Famifies and Friends of the Adult Mentalfy Uf983 6th StreetBoulder, CO 603432
Families Unite for Mental HealthP.0, Box 126Oreland, PA IW75(215) 572-1394
Mental Health Advucates Coalitionof Mmnesnta, Inc.
265 Fort Road (W. 7th St.)St. Paul, MN 55102(612) 222-2741
National Affiance for the Mentaffy 1111234 Massachusetts Avenue, NWSuite 721WashiigtOn, OC 24M05(202) 783-6393
Parents of Adult SchizophrenicsSan Mateo County
P,O. Box 03333San Mateo, CA 94403
Project Overcome1900 Hennepin AvenueMmneapcdis, MN 55403(612) 874-76CS3
Schizophrenia Association of GreaterWashington, fnc.
Wheaton Pfaza Office Buifding North M04Wheaton, MD 2t3932(301 1949-82E2
AUiance for the MentaUy Ill, shown inTable 1, is a coalition of about 200 familyand friends groups. You can contactthem for more information on these or-ganizations in your part of the US. The
Caring Family,bl a book written for fam-ilies with relatives who have emotionaland psychological problems, lists morethan 100 self-help organizations. Anoth-er book by Torrey, Surviving Schizo-phrenia ,62 which will be published in thenear future by Harper & Row, identifiesabout 300 self-help groups.
As you can see from this two-part es-say, research on schizophrenia repre-
sents a broad field with many specializa-tions—etiology, diagnosis, treatment,etc. In Part 1, I listed the LSI/BIO-MELN 63 research fronts on the causes of
schizophrenia. Table 2 shows the1981-1982 ISI/BIOMED research frontson the diagnosis and treatment ofschizophrenia, and the number of coreand citing papers in each. Researchfronts are formed when a group of cur-rent papers cite one or more articlesidentified as core for that topic.
I’ve included both 1981 and 1982research fronts in Table 2 to demon-strate the wealth of literature you canretrieve from the ISI/BIOMED database. For example, if you are interestedin the diagnosis of schuophrenia you canretrieve 159 current papers that cited thpcore literature on that topic. In 1981, 118papers cited the core documents in re-search front #81-0323, “Diagnosis ofschizophrenia. ” In 1982,41 citing paperswere included in research front#82- 1534, “Diagnosis of schizophreniaand catatonic. ”
You should keep in mind that the corepublications in these two research fronts
do not overlap. Table 3 lists the coreliterature in the 1981 and 1982 LSZ/BIO-MED research fronts on diagnosis ofschizophrenia. It’s interesting to notethat the core documents in the 1981
212
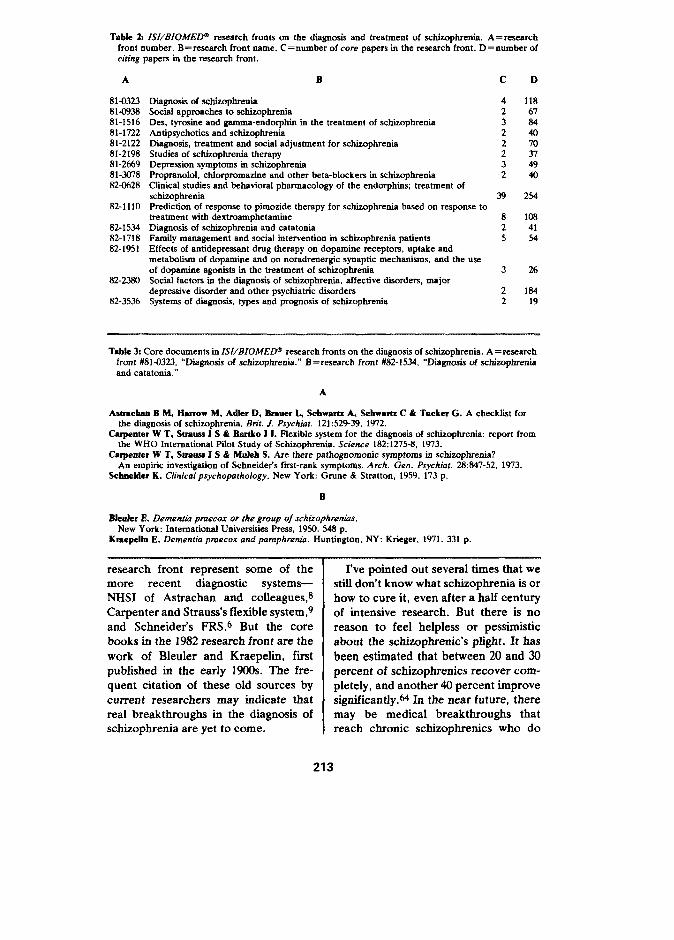
Tabfe 2: ZS[/BIOIUEDa research fronts un the disgnosis and treatment of scfdmphrerda, A= researchfront number. B=research front nsme. C=number of core papers in the resesrch front. D=number ofciting papers in the research front.
A
81-032381-093881-151681-172281-212281-219881-266981-24)7882-0628
82-1110
82-153482-171882-195 I
82-2330
82-3536
B
Diagrmsiz of achizopbrerdaSUCial approachesto acfdzophrerdaDes, tyrnsine and gmnma-endorpbin in the treatment of scbiznphreniaAntipsychotics and schizophreniaDiagnosis, treatment and socisl adjustment for schizophreniaStudies of scfdzc.pfrrerda therapyDepression symptoms in schizophreniaProprenolol, cfrforpromazine and other beta-blockerz in zchiznpbreniaClinkal studies and behavioral pharmacology of the endorphirrs; treatment ofschizophreniaPrediction of respnnse to pimozide therapy for schizophrenia based on respnse totreatment with dextruarnphetarrrineDisgnoaiz of schizophrenia and catatoniaFsrrrily management and -id intervention in scfriznphrenia petientsEffects of antidepressant dmg therspy on dopamine receptors, uptake andrnetabcdizm of dopamine end on noradrenergic synaptic mechanisms, and the uscof doparrrirreagonists in the treatment of schizophreniaSocisl factors in the diagnosis of schizophrenia, sffective dmrdem, majordeprezaive dkrrder snd other psychiatric dianrdersSystenrz of diagnrrsiz, typez and prognosis of schizophrenia
c
42322232
39
825
3
22
D
11867844070314940
2s4
1084154
26
18419
Tabfc 3: Core documents in ISI/BIOMED@ research fronts on the diagnosis of zchizophrerda. A =resesrchfront #81 -0323, “fliagncrsis of schizophrenia. ” B= research front #82-1534, “DIagnoai.s of schizophreniaend catatonic. ”
A
Asrracfran B M, Hurow M, Adfer D, Brarrer L, Schwartz A, Schwartz C & Trrcker G. A checklist furthe diagrrosiz of schizophrenia. M-it. J. Psychiat. 121:52939, 1972.
Cerpanter W T, Strauss J S & Bartko J L Flexible system for the dlagnnaia of schizophrenia: report fromthe WHO International Pdot Study of Schiiphrenia. Science 182:1275-8, 1973.
Cerpenter W T, StTSrJasJ S & Mrefeh S. Are there pstfrognonronic symptoms in schizophrenia?An empiric investigation of Schneider’s fwst-rank symptoms. Arch. Gen. Psychiar. 28:847-52, 1973.
Scbnekfer K. Clinical psychopathology. New York: Gmne & Stratton, 1959.173 p.
B
Bfeerfm 1?. Demeatia ptuecar or the group of schizophnrrrias,New York: Intemationsf Universities Press, 1950.548 p.
Kmepaffn E. Dementia prueco.x and pamphrerria. Huntington, NY: Krieger, 1971.331 p.
research front represent some of themore recent diagnostic systems—NHSI of Astrachan and colleagues,ECarpenter and Strauss’s flexible system,gand Schneider’s FRS.6 But the corebooks in the 1982 research front are the
work of Bleuler and Kraepelin, firstpubfished in the early 1900s. The fre-quent citation of these old sources bycurrent researchers may indicate thatreal breakthroughs in the diagnosis ofschimphrenia are yet to come.
I’ve pointed out several times that westill don’t know what schizophrenia is orhow to cure it, even after a half centuryof intensive research. But there is noreason to feel helpless or pessimisticabout the schizophrenic’s plight. It has
been estimated that between 20 and 30percent of schizophrenics recover com-pletely, and another 40 percent improvesign~~cantly. ~ In the near future, theremay be medical breakthroughs thatreach chronic schizophrenics who do
213

not respond to drug therapy. Even gress for basic research to help unlock
though they may have little chance of the puzzle of schizophrenia.
being cured, we can at least improve the *****quality of their lives by being acceptingand compassionate. More tolerance and My thanks to Linda Cooper and
undt?rstanding might create the atmo- Alfred Welljams-Dorof for their heip in
sphere needed to gain support in Con- the prepamtion of this essay.Olm 1s1
REFERENCES
1. Garffefd E. What do we know about the group of mental disordem caffed schizophrenia?Par-t 1: etiolcgy. Currant Contents (25):5-13, 20 June 1983.
2. Gu~rsb W R. Schizophrenia: the problem of definkion. f3n”t.J. Hosp. Med. 25:23&47, 1981.3. Pope H G & Llpfmkf 1 F. Diagnosis in schisnphrenia snd manic-depressive illness.
Arch. Gen, Psychiat, 35:811-28, 1978.4. van Prnag H M. About the impossible concept of schwphrenia, Compr. Psychiat, 17:481-97, 1976.5. Fenton W S, Mrssber L R & Matthews S M. Diagnosk of schizophrenia: a critical retiew of current
diagnostic systems. Schizophrenia Bull. 7:452-76, 1981.6. Sdmefder K. Clinical psychopathology. New York: Grrme & Stratton, 1959. 173p.7. Sflverwefn M L & Hmsnw M. Schneidcrian fiist-rank symptoms in schirmphrenia.
Arch, Gem P.ychiat. 38:288-93, 1981.8. Astrnchan B M, Harrow M, Ark D, Bsmmr L, SehwnmE A, ScJrwasts C & Tdtcr G. A checklist
for the dngnosir of schizophrenia. Bn’t. J, Psychiat. 121:529-39, 1972.9. Carpmmsr W T, Straws J S il BsxtkoJ J. Flexible system for the dkgnosis of schkmphrenia:
report from the WHO Intemationrd Pifot Study of Schizophrenia. Scierme 182:1275-8, 1973,10. WJmgI K, Cnqer J E & %rtorfrrs N. Measurement and classification ofpsychiatnk symptoms.
London: Cambridge University Press. 1974.233 p.11. LHrfs R E & Gozlec R J. Comparative description of the SADS sod PSE.
Schizophmria Bull. 7:248-57, 1981.12. AmaJcsm Paycfdatrfc .hsdiatfmi.DSM-111: diagnostic and statistical manual of mental disorders.
Washington, DC:APA, 1980. 494p.13. Fetsfmer J P, Robin.s E, Guza S B, Woodmtf R A, Wfnokur G & MrrrtsmR. Diagnostic criteria for
usc io psycfdatnc research. Arch. Gerr. Psychiat. 26:57-63, 1972.14. Sphzer R L, Eadfcott 1 & RoMna E. Research diagnostic criteria.
Psychophamnacol. Brdi. 11(3):22-5, 1975,15. Hake R 1. The diagnosis of schwphrenia: a review of recent developments.
Schizophrenk Bull. 6517-28, 1980.16. Fox H A. The DSM-111 concept of schizophrenia. Bn’t. J. P~ychiat. 138:03, 1981.17. Lm@eMt G. Diagnosis and prognosir of schizophrenia. Proc. Roy. Sot. Med. 531047-52, 1’XQ.18, Taylor M A & AfmarrrsR. The prevsfence of schizophrenia: a reassersmmrt using modem diagnostic
criteria. Amer. J. Psychiat. 135:945-8, 1978.19. Kcwder K A & Waletzky J P. C~micsl use of the antipsychotics. Amer. J. Psychiat 138:202-9, 1981.20. Caamm NH. Managing the person with major psychiatric iffrsers. (Rubenstein E & Federrrran D D,
eds.) Scientific Amenkan medicine. New York: Scientific American, 1982,Vol. 2, Sect. 1~11). p. 1-18.
21, GasfJeM E. Patient compfisnce: a multifaceted prnblem with no easy snlution.Current Content~ (37):5-14, 13 September 1982.
22. 13irvk J M, Sdwdfer C B, Kfllfari G A, Kirrard C & CJrm C. Important issues in the drug treatment ofscbisophrenia. Schizophrenia Bult. 6:7W7, 1980.
23. Perrfa C, LJfmftrfjevic P, Jacobmora L, PmrLwon P, Rapp W & Froberg H. Tardive dyskinesia inpsychiatric patients treated with neurolcptics. Brit. f. Psychid. 135:509-14, 1979.
24, UbrhramrJ L & Frmrbye A. Reversible and irreversible dyskinesia after treatment with prx-phenazine,chlorpromazine, reserpirre and electrcconvufsNe therapy. Psychophannacologia 1:408-18, 1960.
25. Dordorr P T & Stensmr R L. Neurrdeptic induced extrapymmidal symptoms.D&. Nerv. Syst. 37:6%35, 1976.
26. Grwff S N. The rreuroleptic maligrmrrt syndrome. J. C/in. Psychiat. 41:79-83, 19S0.27. Freedman R, KJrclI D, BelI J, Adler L E, PacevJch M, PacJrtmrm E & Denver P. Clonidlne treatment
of schizophrenia. Acts Psychiirt. Scond. 65:35-45, 1982.2E. Yorkston N 1, Gmze!!er 1 H, Zakf S A, Holhwrder D, Phcher D R & Smgmwrt H G S. Propmnolol as
an adjunct to the treatment of schizophrenia. f.uncet 2:575-8, 1977.29. Tmrwy E F. Telephone communication. 23 May 1983.30. Garffe!d E. what do Weknowabout depression? Part 2: diagnosis and treatment.
Currant Contents (20):5-12, 18 May 1981.
214

31. Osmond H & Hoffer A. Massive niacin treatment in achimphrenia. Lmcef 2:316-20, 1%2.32. Demon R. Nicotincmide in the treatment of schizophrenia. Dis. Nerv. .$y$f, 23: [67-72, 1%2.33. Torrey E F. Schizophrenia and civilization. New York: Jason Armrson, 1980. p. 185,34. Berger P A, Watson S J, AM H, Eflfott G R, Rubb R T, Pfefferbarrm A Dmfs K L, Barcbas J D &
Li C H. &Endorphm and schizophrenia. Arch. Gen. Psychiat. 37:635-40, 1980.35. Center R H, Catffn D H, Goreffck DA, Hnf K K & D C H. &Endorphin: intravenous infusion
causes behatiorsl change in psychiatric inpatients. Arch. Gen, Psychiat. 37:642-7, 1980.36. Verboev@n W MA, van Pmag H M, & JorrgJ T V M. Use of naloxone in schizophrenic psychows
and manic syndromes. Neurvpsychobiology 7:159-68, 1981.37. Maekay A V P. Endorphins and the psycbiatrixt, Trends Ne.rosci, 4(5): ix-xi, 1981.38. Garffeld E. The 1982 John Scott Award goes to Jack Ftian and Harold Blumberg for synthesis and
investigation of nrdoxone. Curmvrt Contenfi (16):5-14, 18 April 1983.39. van Pmag H M, Verfmeverr W MA, varrRae J M & de Wfad D. The treatment of schimpfrrenic
psycbcmes with 7-type endorpbins. BioL Psychiat. 17:83-98, 1982.40. PeJmour R M, Ervfa F R, Wageruaker H & Cade R. Characterization of a peptide derived from the
serum of psychiatric patients. Sot. Neurasci. A bstr. 3320, 1977.41. Wagemaker H & Cade R. The use of hemcxhlyxis in chronic scbiiphrenia.
Amer. J. Psychiot. 134:684-5, 1977.42, Dfaz-Brrxo J A, Candfe J A. ChamlJer J T, Farmer C D & Hofbrook W D. DieJyais of schizophrenic
patients: a double-bfind study. Amer. J. Psychiat. 137:12202, 1980.43. ScbuJz S C, vim K-en D P, Bafow J E, FJye M W & B-y W E. DAysis in scbk.ophrenia: a
double-bfind evaluation. Science 211: lW&8, 1981,44. Vanherwegbem J L, LJnkowakf P & Mendfewfcz J. Hemudialysis in schizophrenics.
Arch. Gen. Psychiat. 40(2):21 1-4, 1983.45. Safzosan C. The use of ECT in the treatment of schizophrenia. Amer. J. Psychiaf. 137:1032-41, 19&3.46. Webrer R D. The paycbiatric use of electricaJJy induced seizures.
Amer. J. Psychiat. IM:1W7-17, 1979.47. GarffeJd E. Electroconwdake therapy: mafignant or maligned? Jkays of an information scienti$(.
Philadelphia: ISI Press, 1981. Vol. 4. p. 294-8.(Reprinted from: Current Contents (42):5-9, 15 October 1979.)
48. Epstebr N B & Vlok L A. Research on the results of psychotherapy: a summary of evidence.Amer. J. Psychiat. 138:1027-35, 1981.
49. Vaughn C E & Leff J P. The influence of famiJy and social factors on the course of psychiatriciltnexs. Btif. J. Psychiat. 129:12$37, 1976.
50. Faffumi J R H, LSse- R P, LflJJeF J & Vaughn C E. FamiJy therapy of schizophrenics with highrisk of rcfapae. Fare. process 20:21 l-2f, 1981.
51. Faffomr I R H, Boyd J L. McGffl C W, Jtarad J, MossH B & Gffderrmm A M. Family managementio the prevention of exacerbations of acbiznpbrenia. N. EngL J. Med. 306:1437-40, 1982.
52. Wang 1 S, FaJJuun J R H, Mom H B, J?azaaf J & Boyd J L. The effects of famiJy therapy ontreatment compliance in schizophrenia. Psychopharmacol. Bull. 17:87-8, 1981.
53. Greenbfatt M & GfarJer E. The phasing out of mentaf hospitaJa in the United States.Amer. 3. Psychiat. 1321135-40, 1975.
54. Bassuk E L & Gersum S. Reinstitutionalization and mentaf herdth services.Sri, Amer. 238(2):46-53, 1978.
55. Community Mentaf Heafth Centers Act, Publ. L. No. 88-164, $~2681-2687, 77 Stat. 290(1963).56. Garffefd E. Of beggars, bagkwfies, and bums. Crmsvrt Contenti (6):5-15, 8 February 1982.57. LfssssM W, CaJfay E ~ KJatt C J & Hogarty G. Hospital vs. commrmity (foster) care for psychiatric
patienta. Arch. Gen. Psychiat. ?4:78-83, 1977.58. Lhm M W, KJett C J & fXfey E M. Foster home characteristics and psychiatric patient outcome.
Arch. Gem Psychiat. 37:129-32, 1980.59. ----------------------------------------------- Relapse of psychiatric patients in foster care.
Amer. J. Psychkrt. 13%778-83, 1982.60. Arfng C D. The Gheel experience. J, Amer. Med. Awn. 230W48-l(KU, 1974.61. Benrbefm K F, Lewfrre R R J & Benfe C T. The caring family.
New York: Random House, 1982. p. 207-15.62. Torrey E F. Surviving $chizophmnih. New York: Harper& Row, 1983. (In press. )63. Ir@ftute for ScJerrtfffcJssforrrratfurr.Index to mse.rch fmrrts in LWB1OMED 1983.
PbJfadeJpJda: 1S1, 1983. 544p.64. Scbis@renia can ‘burn itseJf out.’ Med. Worfd News 23(19):25-6, 1982.
215