Embed Size (px)
Citation preview

Glycogen Storage Disease type VI and IX; additional recommendations for follow-up and
treatment beyond childhoodUniversity Medical Centre Groningen

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Author: Anoek MullerStudent number: S1569147Department: Beatrix Children’s Hospital,
Section of Metabolic DiseasesUMCG
Supervisors: Dr. T.G.J. DerksProf. dr. G.P.A. Smit
Period: May – October 2011
2

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
ABSTRACT
Background Glycogen storage diseases (GSD) are inherited disorders primarily affecting the liver or muscle. There are different types of hepatic GSDs, of which type VI and IX are assumed to be the mildest forms. GSD VI and IX are caused by deficiency of the enzymes phosphorylase and phosphorylase b-kinase, respectively. The reduced ability to mobilize glucose from glycogen in the liver results in fasting hypoglycemia, hepatomegaly, growth retardation and biochemical abnormalities. There is a high variability in clinical phenotype and little is known about the long term complications. The goal of this study is to identify the frequency of long-term clinical problems and to provide guidelines for the long-term follow-up during the disease course. Moreover, in the absence of an X-linked inheritance pattern, differentiation between both types of GSD is complicated by indistinguishable clinical symptoms. DNA-analysis is necessary to establish accurate diagnosis. To provide optimal care in older patients and enable genetic counseling for patients and their families, this study describes the natural course of patients with GSD VI and IX.Methods At first a retrospective analysis of clinical features during follow-up was performed. This was followed by a cross sectional study including full medical history, physical examination, biochemical analysis, abdominal ultrasound and bone density measurement of 20 patients from 14 families with GSD VI and IX. In 16 patients DNA-analysis was initiated.Results Clinical features including hepatomegaly, hypoglycemic events, growth retardation and motor developmental delay, were most pronounced during childhood. There is a strong correlation between hepatomegaly and age. Biochemical findings displayed elevated concentrations of TSH (25%), liver transaminases (25%), triglycerides (30%) and uric acid (35%) and decreased concentrations of vitamin D (45%). The use of XO-inhibitors appeared to be beneficial in patients with hyperuricemia. In two patients focal lesions in the liver were detected during abdominal ultrasound and seven out of 20 (41%) patients were diagnosed with osteopenia or osteoporosis based on results of DEXA-scanning. Nine out of 20 patients carry one founder mutation in the PHKA2 gene (c.3614 C>T) causing X-linked hepatic GSD IX. Conclusion Our study confirmed that the majority of clinical signs seem to improve with age. However, based on several findings, we advocate the annual follow-up of biochemical parameters, including 25(OH)D, in adult patients. Additional evaluation of thyroid function depends on clinical symptoms and serum concentrations of TSH and FT4. Hyperuricemia should be treated with XO-inhibitors. Furthermore, as we found that focal lesions in the liver are a long term complication in these patients as well, we advise the use of abdominal ultrasound to detect patients at risk of hepatic tumor. Moreover, this data presents a surprisingly high incidence of osteopenia and osteoporosis, its cause and treatment require further investigation. We advise to optimize calcium intake and, if indicated, start supplementation of vitamin D at an early age. DEXA scan should be performed every two years to assess BMD status. In addition, DNA analysis is recommended for accurate diagnosis and identifies the pattern of inheritance allowing adequate genetic counseling.
3

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
CONTENTS
1. Introduction 41.1 Background 41.2 Hepatic GSDs 51.3 GSD type VI and IX 7 1.4 Genetics 71.5 Management 71.6 Long term complications 8
2. Aim of the study 9
3. Materials and methods 103.1 Patients 103.2 Follow-up investigations 10
3.2.1 Medical history and physical examination 103.2.2 Biochemical analysis 113.2.3 Abdominal ultrasound 113.2.4 Bone density measurement 11
3.3 DNA analysis 113.4 Construction of pedigree 113.5 Feedback of results 123.6 Statistical analysis 12
4. Results4.1 Retrospective clinical data 13
4.1.1 Presenting symptoms 134.1.2 Medical history during follow-up 13
4.2 Outpatient follow-up 144.2.1 History 144.2.2 Physical examination 144.2.3 Biochemical analysis and associated complications 144.2.4 Abdominal ultrasonography 154.2.5 Bone mineralization 16
4.3 DNA analysis 174.4 Pedigree 17
5. Discussion 18
6. Conclusion 21
References 22
Appendices 25I. Invitation letter 26II. Pedigree 28III. Abstract (Dutch) 30
4

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
1. Introduction
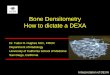
1.1 Background Glycogen, an important energy source, is a macromolecule composed of glucose units. It is found in all tissues, but is most abundant in muscle and liver where it serves as an energy store.(1) Glycogen in muscle serves only to fuel muscular activity. The utilization of glycogen is controlled by muscle contraction and by catecholamines. In the liver, glycogen serves for the maintenance of blood glucose concentration upon short term fasting.(2) Synthesis and degradation of glycogen in the liver follow distinct pathways that begin and end with glucose-1-phosphate (Fig.1). In the liver, glucose is converted to glucose-6-phosphate (G6P) before it can enter one of several metabolic pathways. It can be reversibly converted to glucose-1-phosphate (G1P), the starting point for glycogen synthesis. Alternatively, G6P can be hydrolyzed to glucose or it can be metabolized via the glycolytic pathway to pyruvate and lactate or via the pentose phosphate pathway to ribose-5-phosphate, a precursor of nucleotide synthesis. The rate-limiting enzyme of glycogenolysis, hepatic glycogen phosphorylase, is activated by a cascade of enzymatic reactions. It removes glucose from the outer branches of glycogen, yielding G1P.(3) Different hormones, including insulin, glucagon and cortisol regulate glycogenolysis (GLY), gluconeogenesis (GNG) and glycogen synthesis.(4)
Fig.1. Simplified scheme of glycogen synthesis and breakdown.(3) UDP-glucose is uridine diphosphoglucose; 1. hexokinase/glucokinase, 2. glucose-6-phosphatase, 3. phosphoglucomutase, 4. glycogen synthase, 5. branching enzyme, 6. glycogen phosphorylase, 7. debranching enzyme.
5

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Glycogen storage diseases (GSDs) are the result of inherited defects within glycogen metabolism, which results in abnormal amounts and/or forms of glycogen in various tissues. The overall incidence of GSD is approximately 2.3 per 100,000 births.(5) Biochemical classification became possible when the details of the metabolic pathways were elucidated.(6) Today, virtually all proteins involved in the degradation and synthesis of glycogen are discovered. Different types of GSDs are classified based on the enzyme deficiency and the affected tissue.(7)
1.2 Hepatic GSDsGlycogen storage diseases may affect primarily the liver, the muscle or both. Hepatic GSDs comprise defects in glycogen synthase (GSD 0), the microsomal glucose-6 phosphate complex (GSD I), the debranching enzyme (GSD III), the branching enzyme (GSD IV) and two types that are due to deficient hepatic phosphorylase activity (GSD VI and IX).(7) (Fig.2) Because GLY is defect, patients with hepatic GSDs depend on either GNG or exogenous glucose from intestinal absorption for the maintenance of normal blood glucose concentrations. In general, hepatic GSD should be suspected when a patient presents with (fasting) hypoglycemia, marked hepatomegaly and retarded growth during infancy or childhood. There are two exceptions to this general rule. In GSD I, both GNG and GLY are impaired leading to a severe phenotype and in GSD IV patients present with hepatic cirrhosis in early life leading to end-stage liver disease.(8) GSD 0 results, in contrast to the other types of GSD, in reduced glycogen storage in the liver. Patients present with fasting hypoglycemia and ketosis as well as postprandial hyperglycemia and hyperlactatemia. Patients with GSD III often present with a syndrome that includes hepatopathy, myopathy and cardiomyopathy. Compared to other hepatic GSDs, GSD VI and the hepatic form of GSD IX, are considered the mildest conditions. Medical history, physical examination, basic laboratory and radiology investigations help to differentiate them from other types of hepatic GSD.(1,9,10) (Table 1). In patients with GSD VI and IX, there is a mild tendency to fasting hypoglycemia, hepatomegaly usually disappears around puberty and a late growth spurt results in complete catch-up in final height in the majority of the cases.(1,11-13) GSD VI and IX together account for 25-30% of all glycogen storage diseases with an estimated prevalence of one in 100,000.(14) Most of these are GSD IX. However, these disorders might be under diagnosed as a result of the variable presentation and challenges with diagnostic confirmation.(15)
Fig.2. Targets of hepatic glycogen storage diseases.(16)
6

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Table 1. Differentiation of hepatic glycogen storage diseases.
N = NormalAR = Autosomal RecessiveXL = X-linked
The mode of inheritance, based on family history, can be helpful in distinguishing X-linked GSD IX from the other types as they are all inherited in an autosomal recessive manner. Nevertheless, rare forms of GSD IX are due to mutations on autosomal genes as well.(17) Previously, the diagnostic work-up included loading tests (glucose, galactose or fructose) and in the majority of cases liver biopsy to demonstrate enzyme deficiency in liver tissue. Nowadays, definite diagnosis is most often established by non invasive investigations as measurement of enzyme activity in blood cells and/or mutational analysis.(10)
7
TYPE 0 I III IV VI IXMain clinical symptoms hypoglycemia ++ +++ ++ - + +short stature +/- + + - + +hepatomegaly - + + + + +splenomegaly - - - + - -myopathy - - + +/- - +/-
Laboratory investigations glucose ↓↓ ↓↓↓ ↓↓ N ↓ ↓lactate N ↑↑ N N N Nuric acid N ↑↑ N N N NASAT/ALAT N ↑ ↑↑↑ ↑↑ ↑ ↑ketones ↑ ↓↓ ↑↑ ↑ ↑ ↑CK N N ↑↑ N N NLipids N ↑↑↑ ↑ N ↑ ↑
Abdominal ultrasound enlarged kidneys - + - - - -cirrhosis - - - + - -
Genetics mode of inheritance AR AR AR AR AR AR/XLgene symbol(s) GYS2 G6PC AGL GBE1 PYGL PHKA2
G6PT PHKBPHKG2

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
1.3 GSD VI and IXHepatic GSD caused by a defective phosphorylase system can be the result of a deficiency of liver glycogen phosphorylase (Pase) (GSD VI) or a deficiency of the phosphorylase b-kinase enzyme (Phk) (GSD IX).(18) Pase, the rate limiting enzyme of GLY, is activated by Phk to the active form. Defects in one of these enzymes results in a reduced ability to mobilize glucose from glycogen in the liver. In young patients this may lead to symptomatic hypoglycemia and hyperketosis after long periods of fasting. In adult patients there is a mild tendency to fasting hypoglycemia. Hepatomegaly is due to abnormal amounts of glycogen storage in the liver. Furthermore, elevation of serum concentrations of triglycerides and cholesterol are suggested to be the result of increased synthesis from excess of acetyl CoA and decreased serum lipid clearance.(19) Growth retardation is thought to be one of the long term complications.(3,20) Because the clinical phenotypes of these patients are very similar, it is impossible to differentiate between patients with GSD VI and GSD IX in the absence of a family history suggesting X-linked inheritance.(17) Specific work-up by enzyme assays in leukocytes and erythrocytes might be helpful, but to establish accurate diagnosis DNA analysis is necessary.(21,22)
1.4 GeneticsLiver Pase is encoded by the PYGL gene on chromosome 14. It is a dimeric enzyme composed of two identical subunits; a regulatory domain and a catalytic domain.(23,24) Molecular analysis of the PYGL gene in patients with GSD VI shows that most mutations are missense mutations.(25-29) Liver Phk is a large hexadecameric complex. It comprises four copies each of four subunits (α, β, γ and δ). The γ-subunit contains the active catalytic site, while the α- and β-subunits have a regulatory function that is controlled by phosphorylation. The δ-subunit mediates the binding with Ca2+.(30) The complexity of the enzyme leads to complexity of inheritance. The α subunit is encoded on the X chromosome while other subunits are encoded by autosomal genes on chromosome 16.(1) Mutations in the PHKA2 gene encoding the α-subunit cause X-linked GSD IX (XLG), the most common hepatic variant of GSD. Defect in the β-subunit of Phk is the consequence of mutations in the PHKB gene, resulting in deficiency of Phk in both, liver and muscle. The incomplete holoenzyme that lacks the β-subunit, may possess residual activity which could be the explanation for the surprisingly benign phenotype.(31-33) The liver isoforms of the γ-subunit is encoded by PKHG2, which results in destabilizing of the enzyme. These mutations have been linked to a particularly severe phenotype.(34) To date, deficiency of Phk has not been associated with mutations in one of the three genes (CALM1, CALM2 and CALM3) encoding the identical δ-subunit.(35)
1.5 ManagementTreatment consists of preventing hypoglycemia using a carbohydrate-enriched diet and frequent feedings. In older patients a late evening meal is unnecessary, although it might be required for young patients.(1,36) Under special conditions of increased metabolism (i.e. fever with or without decreased intake) polycose or fruit juice should be given orally. If oral intake is not tolerated and the patient presents with hypoglycemia, an IV with initial glucose bolus followed by 10% dextrose should be started. In case of acute or elective surgery an IV glucose infusion should be started preoperatively and should be continued until the patient tolerates the usual diet.
8

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Overall, the main goal of dietary treatment is to maintain normoglycemia and reduce fasting ketosis to prevent psychomotor developmental delay and to improve growth to reach a normal final height.(1,20)
1.6 Long term complicationsIn the majority of patients with GSD VI and IX the disease course is considered to be benign.(37) Hepatomegaly usually disappears around puberty. Symptomatic hypoglycemia and ketosis is unusual in adult patients, except after prolonged fasting or strenuous physical exercise.(3) Other clinical signs and biochemical abnormalities seems to improve with age, although liver transaminases, triglycerides and cholesterol in blood can remain mildly elevated.(1,16,38) However, growth retardation is a major concern to patients and their parents. A study of 51 male patients with X-linked GSD IX shows a specific growth pattern with initial growth retardation, a late growth spurt and complete catch-up in final height at a later age than usually seen.(12) Other uncommon clinical phenotypes that have been described include splenomegaly, doll-like face, renal dysfunction with proximal renal tubular acidosis, central nervous system abnormalities (seizures, delayed cognitive and speech abilities, peripheral sensory neuropathy), polycystic ovaries, osteopenia/osteoporosis and liver cirrhosis.(3,37,39) Recently, a case report was published describing a patient with GSD VI complicated with a hepatic benign tumor.(40) Increased risk of osteoporosis is seen in patients with different types of GSD. Although several mechanisms have been proposed in different types of GSDs, the pathophysiology remains unsolved.(1,7,15,20,41-43) Moreover, it was concluded that correction of vitamin D could prove beneficial in maintaining normal bone mineral density in these patients.(44) There has been one study measuring bone mineral density in patients with GSD IX: 4 adult patients underwent dual-energy X-ray absorptiometry (DEXA) and one presented with low bone mineral density (BMD).(45)Overall, as a result of the high variability in clinical phenotype it is difficult to predict long term complications in patients with GSD VI and IX.
9

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
2. Aim of the study
There is little information about the natural course of GSD type VI and IX until adulthood.(20) The goal of this study is to identify the frequency of long-term clinical problems. Moreover, based on findings during a cross sectional study we want to provide guidelines for the long-term follow-up during the disease course. Therefore, we describe the natural course of 20 patients from 14 families with GSD VI and IX. The results of this study are important in providing optimal care in older patients and enable genetic counseling for patients and their families.
10

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
3. Materials and methods
3.1 PatientsThirty patients from 24 families were identified from the hospital records from the Section of Metabolic Diseases, Beatrix Children’s Hospital, of the University Medical Center Groningen (UMCG), University of Groningen, the Netherlands. In all patients, suspicion of GSD VI or IX was initially based on clinical features and further investigated by tolerance tests, enzyme assays and/or DNA analysis. All patients and their families were informed about the nature of the study and received a written invitation for out-patient follow-up. After contacting them to arrange a date for the extra visit, 20 patients from 14 families participated in this study. Subsequently, retrospective analysis on diagnosis, presenting symptoms and medical history during follow-up was conducted. Collected clinical data included symptoms and biochemical findings, global growth pattern and development. If a patient had not achieved the developmental milestones such as crawling and walking when expected, this was reported as motor developmental delay. Delayed puberty in females was defined as lack of breast development and/or lack of pubic hair at age 14 years and/or lack of menarche by 16 years. In males puberty is considered delayed if there is a lack of pubic hair by 15 years and/or testicular enlargement does not occur by 15 years.(47) Mental development was regarded as ‘normal’ when patients were able to attend normal school.(13) In thirteen out of 15 patients diagnosis was confirmed by blood cell enzyme assay: in one patient deficiency was found in leukocytes and in the other 12 patients in erythrocytes. In two patients, who are siblings, results of enzyme assays were normal and diagnosis was strongly suspected based on galactose loading test. Four patients underwent liver biopsy, 3 showed glycogen storage and in one PhK deficiency was confirmed. In four patients results of DNA analysis were already available. One patient, in whom GSD IX was suspected based on family history, had a mutation in the PHKA2 gene (c.3614 C>T). The same mutation was found in two other patients, a father and his daughter. In the fourth patient GSD VI was presumed based on family history, and sequencing of the PYGL gene identified two nucleotides changes including one novel mutation (c.131 G>A (p.Arg44His)/c.1900 G>C (p.Asp634His)). To show the X-chromosomal inheritance of GSD type IX, a large Dutch pedigree comprising more than 200 individuals was published in 1969.(46) At the time of retrospective analysis, five of the included patients were known to belong to this pedigree.
3.2 Follow-up investigationsPatients were invited for an outpatient follow-up including history, physical examination, biochemical analysis, abdominal ultrasound and bone density measurement.
3.2.1 Medical history and physical examinationDuring out-patient follow-up history included questions about the current medical situation, social and family history and dietary treatment or use of other drugs at the moment. Then general physical examination was performed. Height was measured barefoot with a Harpender stadiometer. Evaluation of liver size was performed by palpation of the lower border below the right costal margin at the midclavicular line (MCL). Hepatomegaly was defined as a liver palpable more than 2 cm below the right costal margin in MCL.(13)
11

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
3.2.2 Biochemical analysisRandom serum and urine samples were obtained during the visit. Blood investigation included haematological parameters, liver tests, kidney function, creatine kinase, thyroid stimulating hormone (TSH), free thyroxine (FT4), HbA1c, alpha-fetoprotein (AFP) and carcinoembryonic antigen (CEA) concentrations and total 25-hydroxyvitamin D (25(OH)D) level. Plasma concentrations of glucose, ketones, liver transaminases (ASAT/ALAT), lactic and uric acid, cholesterol and triglycerides along with urinary excretion of lactate and ketones were measured as parameters of metabolic control. Reference values were corrected for age and gender, as they are used in the laboratory of the UMCG.
3.2.3 Abdominal ultrasoundAbdominal ultrasound was performed to evaluate the aspect of the liver, with special attention for lesions suspect for adenoma or other tumors. In addition patients were screened for ultrasonic characteristics suggesting nefrocalcinosis or cysts, and in female patients for polycystic ovaries.
3.2.4 Bone density measurementPatients underwent bone mineral measurement by dual-energy X-ray absorptiometry (DEXA) for lumbar vertebrae, radius and proximal femur. Bone mineral density (BMD) values were expressed as Z- and T-scores. The Z-score represented the number of standard deviations (SD) matched for age, gender and race. According to the World Health Organization (WHO) these scores were used in children and adolescents until the age of 20 years. Osteopenia was defined as a Z-score between -1 and -2,5 SD and osteoporosis was defined as a Z-score below -2,5 SD.(48) In addition, in adults T-scores were determined based on peak bone mass (as reached on the age of 20 to 30 years) matched for gender and race. T-scores declined parallel with the age-related drop in bone mass. This is the reason T-scores were used for clinical decision making.(49) The WHO defined osteopenia as a T-score ranging from -1 to -2,5 SD and osteoporosis was defined as a T-score below -2,5 SD.(50)
3.3 DNA analysisAfter informed consent, DNA-analysis was initiated, when not performed before. Selection of genes to be sequenced was guided by the severity of the symptoms, family history and the results of enzymatic assays. DNA was extracted from peripheral blood leukocytes using standard procedures. Mutation screening was performed by the laboratory of Sheffield Children’s NHS Trust, Section; Sheffield Molecular Genetics Service, United Kingdom, according to Beauchamp et al.(16,25)
3.4 Construction of pedigreeThe large Dutch pedigree (46) was extended with the patients who participated in this study. Based on family history, PASS Pedigree® (Pass clinical 3.3. HealthCare Pro Active Software Solutions) was used to draw the novel branches.
12

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
3.5 Feedback of resultsFour weeks after the outpatient follow-up, all patients received a phone call to inform them about the results of the investigations. Furthermore, during the annual event ‘a day for patients with GSD’, overall results were presented. Because results of DNA analysis will be available after at least four months, patients will be acquainted with these results after six months.
3.6 Statistical analysisStatistical analysis of data was performed using SPSS19.0. for Windows software. Most of the results were descriptive. Results were summarized as frequencies and percentages or as mean and standard deviation. Because there was a lack of normal distribution, non-parametric correlation (Spearman’s correlation coefficient) was used to determine degrees of association. To evaluate the strength of correlation, linear regression analysis was performed.
13

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
4. Results
Twenty out of 30 patients from 14 families were included in this cross sectional study. Two families contained two affected children and one four. The majority of patients (17/20) were male. One out of 3 female patients originated from a family with a known X-linked inheritance pattern. At the time of investigations, mean age of the patients was 21,3 years (range 5–51 years). Eleven patients were adults, 2 females and 9 males. Among the nine children and adolescents who participated there were 1 female patient and 8 male patients.
4.1 Retrospective clinical data
4.1.1 Presenting symptomsFrom two patients clinical data at time of diagnosis were not available. In 18 patients the mean age of onset of clinical symptoms was 12,8 months with variation from 1 to 45 months. At the time of diagnosis all patients (18/18) presented with a protuberant abdomen with hepatomegaly. Other presenting symptoms included hypoglycemia (13/18) and failure to thrive (7/18). Biochemical abnormalities included an increase in serum transaminase activities (16/18), elevated serum uric acid (4/18), hypertriglyceridemia (16/18) and hypercholesterolemia (4/18).
4.1.2 Medical history during follow-upTable 3 shows the frequency of symptoms and biochemical abnormalities during follow-up. Thirteen patients experienced at least one hypoglycemic event, most often during an infection. Statural growth retardation was present in 14 cases and mild motor developmental delay in 9 patients. Delayed puberty was present in 2 of 15 patients, both were male. Standardized staging of sexual development was not performed. A normal fasting tolerance was generally observed, except in rare cases.
Table 2. Symptoms and biochemical abnormalities in patients with GSD VI and IX.
Clinical feature Frequency Percentage
Hepatomegaly 19/20 95%
Growth retardation 14/20 70%
Motor developmental delay 9/20 45%
Hypoglycemic events 13/20 65%
Elevated liver transaminases 18/20 90%
Hypertriglyceridemia 18/20 90%
Hypercholesterolemia 6/20 33%
Elevated uric acid 9/20 50%
14

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
4.2 Outpatient follow-up
4.2.1 HistoryDuring out-patient follow-up 18 out of 20 patients reported that the current medical situation was satisfactory. One male patient, 5 years of age, was recently diagnosed and presented with a protuberant abdomen, failure to thrive and mild motor developmental delay. In a 14-year-old female patient the major concern was persistent growth retardation. At present, an individually tailored enriched carbohydrate diet and frequent feedings was followed by 7 younger male patients with age ranged from 5 to 18 years. In 50% of the patients a late evening meal was used to prevent early morning hypoglycemia. Thirteen patients are of diet, although in 8 of them the use of frequent feedings was a daily habit. Allopurinol® (xanthine-oxidase inhibitor) was used by 25% of the patients and one patient was using atorvastatine® (cholesterol synthesis inhibitor) together with vitamin D supplements.In general mental development was normal. Of the patients under 15 years of age, all (7/7) were able to follow normal general education. Of the patients above 15 years of age, four were still following normal general education and 8 patients had normal employment. One patient, a 23-year-old man, followed special education and needed special work. This was not related with a higher incidence of hypoglycemia during lifetime. However, as a result of multiple events in childhood he had psychosocial developmental problems and lived in multiple foster homes during adolescence. At present, he lives in an institute with daily supervision.
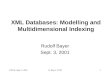
4.2.2 Physical examinationIn all children and adolescents who participated, standard deviation score (SDS) of height were calculated by comparing it with sex- and age-matched controls. In all nine patients with a mean age of 11.7 years (range 5 to 18 years), SDS for height was below normal values with a mean SDS of -1,40 (±0,97). There was no correlation of height with age. One 14-year-old girl presented with persistent unexplained growth retardation and a SDS of -3,43.At the time of follow-up, in 35% of the patients the liver was enlarged more than 2 centimeters under the right costal margin in MCL. Hepatomegaly showed a correlation with age (rs = -0.808, P<0.01). The regression slope of hepatomegaly against age is -2.89 cm/year (95% CI -4.254 to -1.526). Decrease in liver size with aging is shown in Figure 3.
4.2.3 Biochemical analysis and associated complicationsIn all patients parameters of haematology and kidney function were normal as well as HbA1c and the tumormarkers AFP and CEA. Serum TSH concentration was elevated in 5 out of 20 patients, all together with normal values for FT4. One of these patients presented with complaints of fatigue and additional determination of serum anti-thyroid peroxidase showed a raised concentration. Four male patients presented with mildly increased serum creatine kinase concentration. The age of these patients ranged from 7 to 51 years and values that were found were between 210 and 248 U/l with a reference value of 200 U/l. Random plasma glucose concentration was normal, hypoglycemia was not reported. One patient, a 5-year-old boy who was recently diagnosed, presented with hyperketosis along with lactic acidosis in blood and ketonuria.
15

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Fig.3. Linear regression line with 95% confidence interval drawn on scatter diagram relating age and hepatomegaly in 20 patients with glycogen storage disease type VI or type IX.
Liver transaminases (ASAT/ALAT) were raised in 5 out of 20 patients. There was a correlation with size of the liver (rs = -0.704, p = 0.01) and with age (rs = 0.682, p = 0.01). Mean serum triglycerides concentration was 1.86 mmol/l (range 0.48 to 4.47 mmol/l) with a fasting reference value of 2.00 mmol/l. In six male patients concentrations were elevated. No correlation was found with age or size of the liver. Overall, cholesterol concentration was not raised, except for one patient who presented with metabolic derangement at the time of follow-up. Another patient, in whom family history was positive for familiar hypercholesterolemia, was using cholesterol synthesis inhibitors. At the time of the study cholesterol concentration was normal. Complications due to hyperlipidemia were not reported. Serum uric acid concentrations ranged from 0,17 to 0,50 μmol/l with a mean of 0.31 (±0.08) μmol/l. Used reference values were dependent on age and gender. Two patients presented with elevated concentration. They were siblings, respectively male (23 years) and female (20 years). Both did not use xanthine-oxidase inhibitors. There was no significant difference in uric acid concentration between the patients who were using xanthine-oxidase inhibitors and those who were not. Complications due to hyperuricemia (renal calcifications, kidney stones etc) were not reported, except for one 42-year-old man who had had frequent attacks of gouty arthritis.Serum concentration of 25-hydroxyVitamin D (25(OH)D) were below 50 nmol/l in 45% of the patients. None of the patients had hypocalcaemia or hypercalciuria. One patient was using vitamin D supplements and presented with normal vitamin D concentration.
4.2.4 Abdominal ultrasonographyIn 19 patients abdominal ultrasound was performed. 53% of the patients presented with increased echogenicity of the liver. In a 5-year-old male, who presented with metabolic derangement, a focal lesion described as an anatomical variant not suspected for adenoma, was reported. The patient intensified the dietary treatment during a 3 weeks hospitalization. After 6 weeks abdominal ultrasound showed reduced size of the lesion, associated with improved parameters for metabolic control. In another patient, a 29-year-old male, three focal lesions in the right part of the liver were reported. In our cohort, ultrasonic characteristics for nefrocalcinosis were not observed.
16

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
One male patient, 42 years old, presented with a small cyst (8mm) in the cortex of the right kidney. In two female patients who underwent the abdominal ultrasound no polycystic ovaries were detected.
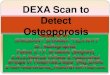
4.2.5 Bone mineralizationDEXA-scan was performed in 18 patients. Seven out of 8 children and adolescents had normal BMD. One 14-year-old female patient presented with low BMD (whole body Z-score -4,0 SD). Because this patient presented with persistent growth retardation and skeletal age was not matched with the real age, Z-scores were regarded not reliable and therefore she was excluded from this analysis. Of the ten patients above the age of 20 years who underwent DEXA-scan, 7 presented with low BMD. T-scores were determined for radius, lumbar vertebrae and proximal femur. According to WHO classification(50) one patient presented with one site of osteopenia; the proximal femur. Another patient had osteopenia of lumbar vertebrae. In both patients T-scores for other sites were normal. Furthermore, osteopenia of two sites, proximal femur and lumbar vertebrae, was found in another patient. Four patients presented with low BMD of all three assessed sites. Of these four patients, two male patients, 23 and 29 years old, presented with T-scores for the lumbar vertebrae of -2,7 SDS and -3,3 SDS respectively, which was classified as osteoporosis.(Fig.4) There was no correlation with age or weight or serum 25(OH)D for either of the T-scores.
Osteopenia according to WHO
Osteoporosis according to WHO
Male patiento Female patient
17

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Fig.4. T-scores of 10 patients with glycogen storage disease type VI or type IX for radius, lumbar vertebrae and proximal femur.
18

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
4.3 DNA-analysisIn sixteen patients from 11 families gene analysis was initiated. During out-patient follow-up 8 patients appeared to belong to the historical pedigree and sequencing of the PHKA2 gene in these patients identified a known mutation (c.3614 C>T).(51) The same mutation was found in one other patient. In this case, family history was suggestive for X-linked GSD IX, but there were no leads suggesting that this patient belongs to the pedigree. In 10 other patients DNA analysis was initiated and results are pending.
4.4 PedigreeFigure 5 in the appendix shows a large pedigree with cases of X-linked GSD IX as it was published in 1969.(46) Family history assembled at the out-patient follow-up resulted in the addition of three more patients. The pedigree was extended with a novel branch and the next generation of patients was added to the particular branches.
19

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
5. Discussion
Limited information is available about the natural course until adulthood of patients with GSD VI and IX. These types of GSD are assumed to be the mildest. The goal of this study was to identify the frequency of long-term clinical problems. Moreover, based on findings during a cross sectional study we want to provide guidelines for the long-term follow-up during the disease course.
We are aware of the fact that the number of patients included in our study is small. This reflects that GSD VI and IX are rare disorders and our study was restricted to one health centre only. In addition, in our cohort of patients the majority (85%) were male, obviously due to the X-linked inheritance of the most common hepatic variant of GSD. There was high variability in age at the time of the study, with smaller numbers of patients older than 30 years. This may be due to loss to follow-up as a consequence of the supposed benign clinical course. Furthermore, as a result of the study design it is difficult to conclude causal inference. Despite these limitations, we were able to describe the clinical course of 20 patients from 14 families with GSD VI and IX. Moreover, our results showed unexpectedly high incidences of several long term complications. As described previously, we show that clinical symptoms in patients with GSD VI and IX were most pronounced during childhood, including the incidence of hypoglycemic events, reduced growth velocity, hepatomegaly and biochemical abnormalities.(1,12,13,37) Furthermore, in agreement with previous observations(8,36) we concluded that younger patients were more likely to use an individual diet and a late evening meal compared to adult patients, of which the majority was of-diet. In addition, as a result of the relatively low incidence of (mild) hypoglycemic events, mental development in these patients was normal. This is in line with previous findings.(15,20) Moreover, the initial growth retardation and improvement of growth after puberty as described in these patients(1,12,52), was established by our findings that all younger patients presented with SDS for height below normal, and all adult patients had reached normal final height. Figure 3 presents a decrease of hepatomegaly with ageing in our cohort of patients. First, it needs to be emphasized, that standardized assessment of liver size by physical examination is a matter of debate itself. We used the palpatory method, estimating protrusion of the liver below the right costal margin at the MCL. Alternatively, one may measure liver span, obtained by either percussion-palpation or by percussion-percussion method. These methods determine the upper and lower borders of the liver and show strong correlation with results obtained by X-ray findings.(53,54) Despite these considerations, our data strongly supported the previous observations reporting that the hepatomegaly gradually disappeared with increasing age.(3,37) In addition, we found that raised serum concentrations of liver transaminases (ASAT/ALAT) correlated with size of the liver and with age, suggesting these parameters could be useful in evaluation of hepatomegaly in these patients. However, interpretation of these parameters is difficult, because values are non specific and are highly dependent of the clinical context of the patient.(55) Although improvement of the concentration of liver transaminases along with a decrease in liver size has been described(37), these biochemical values alone are not sufficient to evaluate the severity of hepatomegaly.
20

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Remarkable, we found elevated serum TSH concentration together with normal values for FT4 in 25% of our patients. We measured serum anti-thyroid peroxidase, a thyroid autoantibody, in one of these patients which was substantially increased, suggesting auto-immune thyroid disease.(56) In unselected populations, approximately 5% of women and 3% of men have subclinical hypothyroidism (raised TSH together with normal FT4)(57), meaning there is an increased incidence in our cohort of patients. Thyroid autoimmunity has been described in patients with GSD I.(58) It was hypothesized that damage of thyroid tissue might be caused by a toxic effect of lactic acid excess.(59) In our cohort of patients serum lactate concentrations were normal, suggesting there might be another cause. Additional investigations to evaluate possible (auto-immune) subclinical hypothyroidism in patients with GSD VI and IX would be of great interest. Furthermore, measurement of thyroid function should be included in regular follow-up of these patients. Evaluation of serum lipids in our patients showed no significant abnormalities, although mild hypercholesterolemia and hypertriglyceridemia are described as long term complications in these patients.(13,16,38) It should be noted that collection of blood samples were random, so fasting values were not available and the interpretation of results are biased. Nevertheless, these findings are in agreement with findings of Geberhiwot et al.(60) Overall, it is important to realize that there is high variability in degree of hyperlipidemia in patient with GSD VI and IX, but nevertheless it is an important parameter for metabolic arrangement.(61)In contrast to other hepatic GSDs, serum uric acid concentrations are assumed to be normal in patients with GSD VI and IX. However, in this study of 20 patients, 5 patients were using a xanthine-oxidase (XO) inhibitor and 2 other patients had elevated uric acid concentrations. One of the patients on XO inhibitors reported multiple attacks of gouty arthritis. In patients with GSD I, hyperuricemia is thought to be the result of both, increased production and decreased clearance. Increased production is suggested to be caused by ATP depletion and decreased intra-hepatic phosphate concentration which leads to increased degradation of adenine nucleotides to uric acid. Decreased renal clearance is caused by competitive inhibition of uric acid excretion by lactate.(1) Our two patients with hyperuricemia did not present with elevated lactate concentration in blood or urine. Because 4 of the 5 patients using XO-inhibitors were siblings, like the 2 patients with hyperuricemia, we cannot exclude that additional modifying genes determine the genetic susceptibility to develop hyperuricemia in our patients. Nevertheless, hyperuricemia is a risk factor for the development of renal calcification and kidney stones.(8) Therefore, in patients with GSD VI and IX complicated with hyperuricemia, XO-inhibitors should be started to prevent urate nephropathy. Our study presented seven out of 17 patients with osteopenia at one or multiple sites investigated by DEXA scanning, in two young male patients BMD of the lumbar vertebrae was even classified as osteoporosis.(Fig.4) Decrease of bone mineralization has been reported in patients with different types of GSD.(1,7,15,20) There has been one study measuring BMD in patients with GSD IX; 1 out of 4 patients presented with low BMD.(45) Possible causes may include poor dietary calcium intake, hypercalciuria, poor metabolic control, decreased physical activity and hypovitaminosis D.(41-44) Although dietary intake of calcium was not registered, the majority of other options were excluded in our patients, as they were in good metabolic control, without hypocalcaemia or hypercalciuria. However, 45% of our patients had 25(OH)D concentrations below 50 nmol/l, which is a risk factor for bone fractures in later life.(50)
21

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
The underlying mechanism, described for patients with GSD I and III, suggested that inappropriate vitamin D causes secondary hyperparathyroidism and bone loss, leading to osteoporosis and potential fractures.(1,43) Moreover, the appearance of delayed bone maturation in these patients was suggested to increase the risk for reduced BMD.(42,45) In patients with GSD I correction of vitamin D is regarded to be beneficial in maintaining normal BMD.(44) Therapeutic intervention to improve calcium intake, if indicated in combination with vitamin D supplementation, needs to be started at an early age. Furthermore, in adult patients DEXA-scan should be performed every two years to assess BMD status. There has been one case report(40) describing a hepatic tumor in a patient with GSD VI. During our study we detected liver tumors in 2 out of 19 patients sonographically. In the first patient, the size of the lesion reduced after intensifying dietary treatment. In the second patient, multiple focal lesions in the liver were reported. The role of ultrasound investigation in patients with hepatic GSD has been discussed, concluding it should be used to detect the patients at risk of developing tumors.(62) However, based on ultrasonic findings it is likely to erroneously interpret lesions as adenomas as it could be focal fatty infiltration, focal fatty sparing or focal nodular hyperplasia as well. (62-64) Hepatic tumors are a known complication in patients with GSD I, III and IV. (1,65) It has been hypothesized that tumor formation implicates disordered fatty acid metabolism in these patients, suggesting chronic hypertriglyceridemia could be a sign of hepatic tumor development.(65) Liver adenomas, most common hepatic tumors in GSD I and III, may cause mechanical problems and acute hemorrhage. Although rare, they may develop into carcinomas.(66,67) Serum AFP and CEA can be used to screen for malignant transformation. In addition, to further investigate increase in size of nodules or loss of definition of their margins, CT scan or MRI is used. (1,68) In general, regular ultrasonography to detect patients at risk for hepatic tumors should be performed. DNA analysis showed that 9 out of 20 patients carry one founder mutation in the PHKA2 gene (c.3614 C>T) causing X-linked GSD IX. Interestingly, one of these patients was a female. Although mild expression of the disease in female carriers of XLG has been described(37), this patient presented with severe persistent growth retardation. Sequencing of the PHKA2-gene of the mother of the patient ruled out that there was homozygosity for the mutation. Probably, she represents a hemizygote with pronounced inactivation of the PHKA2-gene of the second X-chromosome. This supports the theory that the X-linked gene coding for Phk is subject to lyonisation.(69)
A longitudinal study with a larger sample size to provide more power and a better distribution of age would be beneficial in the analysis of multiple clinical parameters in patients with GSD VI and IX. Furthermore, in other types of GSD mouse models, recapitulating typical histological and physiological features of human, are used to reflect the spectrum of disease(70) and to evaluate the effect of gene therapy.(71) A mouse strain with muscle specific XLG and a rat strain with Phk deficiency caused by mutations in the γ-subunit (PHKG2) has been studied intensively.(7) Moreover, somatic cells of rodents were analyzed to localize the mutation on chromosome 14 responsible for GSD VI.(72) The use of a mouse model representing the clinical phenotype of GSD VI and hepatic XLG would be of great interest to further investigate long term complications and their underlying pathophysiology.
22

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
6. Conclusion
This study confirmed that the majority of clinical signs in patients with GSD VI and IX seem to improve with age. However, there were several findings, based on which current guidelines for follow-up and treatment will be changed. Annual follow-up of biochemical parameters in adult patients, including 25(OH)D, is strongly recommended. Additional evaluation of thyroid function should depend on clinical symptoms and concentrations of TSH and FT4. Furthermore, as we found that focal lesions in the liver are a long term complication in these patients as well, we advise the use of ultrasonography to detect the patients at risk of developing tumors. In addition, this data presents a surprisingly high incidence of osteopenia and osteoporosis, its cause and treatment require further investigation. We advise to optimize calcium intake and, if indicated, start supplementation of vitamin D at an early age. We believe that DEXA scan would be a useful adjunct in the monitoring of patients with GSD VI and IX and should be performed every two years to assess BMD status.
Despite the majority of gene analyses are still pending, we underline the fact that DNA analysis is of great value in establishing accurate diagnosis and identifying the pattern of inheritance permitting adequate genetic counseling.
23

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
References
(1) Smit GPA, Rake JP, Akman S, DiMauro S. The glycogen storage diseases and related disorders. In: Fernandes J, Saudubray JM, Van dan Berghe G. Inborn metabolic diseases. 4th rev ed. Heidelberg: Springer; 2006. p. 101-119.
(2) Roach PJ. Glycogen and its metabolism. Curr Mol Med 2002 Mar;2(2):101-120. (3) Wolfsdorf JI, Weinstein DA. Glycogen storage diseases. Rev Endocr Metab Disord 2003 Mar;4(1):95-102. (4) Ozen H. Glycogen storage diseases: new perspectives. World J Gastroenterol 2007 May 14;13(18):2541-
2553. (5) Applegarth DA, Toone JR, Lowry RB. Incidence of inborn errors of metabolism in British Columbia, 1969-
1996. Pediatrics 2000 Jan;105(1):e10. (6) Cori GT. Glycogen structure and enzyme deficiencies in glycogen storage disease. Harvey Lect 1952 -
1953;48:145-171. (7) Chen YT. Glycogen storage diseases. In: Scriver CR, Beaudet AL, Sly WS, Vale D, Childs B, Kinzler KW, et al,
editors. The metabolic & molecular basis of inherited diseases New York: McGraw-Hill; 2001. p. 1521-1552.
(8) Rake JP, Visser G, Smit GPA. Disorder of carbohydrate and glycogen metabolism. Berlin: Springer; 2006; 2006. p. 161-181.
(9) Roe T.F., Won N.G., Smit G.P.A. Disorders of carbohydrate and glycogen metabolism. In: Blau N, Duran M, Blaskovics ME. Physician's guide to the laboratory diagnosis of metabolic diseases. 2nd ed. Berlin: Springer; 2003. p. 335-716.
(10) Mayatepek E, Hoffmann B, Meissner T. Inborn errors of carbohydrate metabolism. Best Pract Res Clin Gastroenterol 2010 Oct;24(5):607-618.
(11) Hoffmann GF, Engelmann G. Liver Disease. In: Hoffmann GF, Zschocke J. Inherited metabolic diseases: a clinical approach. Heidelberg: Springer; 2010. p. 89-108.
(12) Schippers HM, Smit GP, Rake JP, Visser G. Characteristic growth pattern in male X-linked phosphorylase-b kinase deficiency (GSD IX). J Inherit Metab Dis 2003;26(1):43-47.
(13) Smit GP, Fernandes J, Leonard JV, Matthews EE, Moses SW, Odievre M, et al. The long-term outcome of patients with glycogen storage diseases. J Inherit Metab Dis 1990;13(4):411-418.
(14) Maichele AJ, Burwinkel B, Maire I, Sovik O, Kilimann MW. Mutations in the testis/liver isoform of the phosphorylase kinase gamma subunit (PHKG2) cause autosomal liver glycogenosis in the gsd rat and in humans. Nat Genet 1996 Nov;14(3):337-340.
(15) Dagli AI, Weinstein DA. Glycogen Storage Disease Type VI. In: Pagon RA, Bird TD, Dolan CR, Stephens K, editors. GeneReviews Seattle (WA): University of Washington, Seattle. All rights reserved; 1993-2011.
(16) Beauchamp NJ, Dalton A, Ramaswami U, Niinikoski H, Mention K, Kenny P, et al. Glycogen storage disease type IX: High variability in clinical phenotype. Mol Genet Metab 2007 Sep-Oct;92(1-2):88-99.
(17) Hendrickx J, Willems PJ. Genetic deficiencies of the glycogen phosphorylase system. Hum Genet 1996 May;97(5):551-556.
(18) Nyhan WL. Work-up of the patient with hypoglycemia. In: Hoffmann GF, Zschocke J. Inherited metabolic diseases: a clinical approach. Heidelberg: Springer; 2010. p. 39-43-386.
(19) Bandsma RH, Smit GP, Kuipers F. Disturbed lipid metabolism in glycogen storage disease type 1. Eur J Pediatr 2002 Oct;161 Suppl 1:S65-9.
(20) Goldstein J, Austin S, Kishnani P, Bali D. Phosphorylase Kinase Deficiency. In: Pagon RA, Bird TD, Dolan CR, Stephens K, editors. Gene Reviews Seattle (WA): University of Washington, Seattle. All rights reserved; 1993-2011.
(21) Maire I, Baussan C, Moatti N, Mathieu M, Lemonnier A. Biochemical diagnosis of hepatic glycogen storage diseases: 20 years French experience. Clin Biochem 1991 Apr;24(2):169-178.
(22) Dahan N, Baussan C, Moatti N, Lemonnier A. Use of platelets, mononuclear and polymorphonuclear cells in the diagnosis of glycogen storage disease type VI. J Inherit Metab Dis 1988;11(3):253-260.
(23) Newgard CB, Fletterick RJ, Anderson LA, Lebo RV. The polymorphic locus for glycogen storage disease VI (liver glycogen phosphorylase) maps to chromosome 14. Am J Hum Genet 1987 Apr;40(4):351-364.
(24) Rath VL, Ammirati M, LeMotte PK, Fennell KF, Mansour MN, Danley DE, et al. Activation of human liver glycogen phosphorylase by alteration of the secondary structure and packing of the catalytic core. Mol Cell 2000 Jul;6(1):139-148.
(25) Beauchamp NJ, Taybert J, Champion MP, Layet V, Heinz-Erian P, Dalton A, et al. High frequency of missense mutations in glycogen storage disease type VI. J Inherit Metab Dis 2007 Oct;30(5):722-734.
24

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
(26) Burwinkel B, Bakker HD, Herschkovitz E, Moses SW, Shin YS, Kilimann MW. Mutations in the liver glycogen phosphorylase gene (PYGL) underlying glycogenosis type VI. Am J Hum Genet 1998 Apr;62(4):785-791.
(27) Tang NL, Hui J, Young E, Worthington V, To KF, Cheung KL, et al. A novel mutation (G233D) in the glycogen phosphorylase gene in a patient with hepatic glycogen storage disease and residual enzyme activity. Mol Genet Metab 2003 Jun;79(2):142-145.
(28) Chang S, Rosenberg MJ, Morton H, Francomano CA, Biesecker LG. Identification of a mutation in liver glycogen phosphorylase in glycogen storage disease type VI. Hum Mol Genet 1998 May;7(5):865-870.
(29) Davit-Spraul A, Piraud M, Dobbelaere D, Valayannopoulos V, Labrune P, Habes D, et al. Liver glycogen storage diseases due to phosphorylase system deficiencies: Diagnosis thanks to non invasive blood enzymatic and molecular studies. Mol Genet Metab 2011 May 17.
(30) Brushia RJ, Walsh DA. Phosphorylase kinase: the complexity of its regulation is reflected in the complexity of its structure. Front Biosci 1999 Sep 15;4:D618-41.
(31) Burwinkel B, Moses SW, Kilimann MW. Phosphorylase-kinase-deficient liver glycogenosis with an unusual biochemical phenotype in blood cells associated with a missense mutation in the beta subunit gene (PHKB). Hum Genet 1997 Dec;101(2):170-174.
(32) Chan KF, Graves DJ. Isolation and physicochemical properties of active complexes of rabbit muscle phosphorylase kinase. J Biol Chem 1982 May 25;257(10):5939-5947.
(33) Hinrichsen A, Bockl HJ, Schramm HJ. Electron microscopical examination of different aggregation and decomposition states of phosphorylase kinase. Identification and computer averaging of the alpha gamma delta fragment. Biol Chem Hoppe Seyler 1989 Feb;370(2):125-133.
(34) Burwinkel B, Rootwelt T, Kvittingen EA, Chakraborty PK, Kilimann MW. Severe phenotype of phosphorylase kinase-deficient liver glycogenosis with mutations in the PHKG2 gene. Pediatr Res 2003 Dec;54(6):834-839.
(35) Fischer R, Koller M, Flura M, Mathews S, Strehler-Page MA, Krebs J, et al. Multiple divergent mRNAs code for a single human calmodulin. J Biol Chem 1988 Nov 15;263(32):17055-17062.
(36) Nakai A, Shigematsu Y, Takano T, Kikawa Y, Sudo M. Uncooked cornstarch treatment for hepatic phosphorylase kinase deficiency. Eur J Pediatr 1994 Aug;153(8):581-583.
(37) Willems PJ, Gerver WJ, Berger R, Fernandes J. The natural history of liver glycogenosis due to phosphorylase kinase deficiency: a longitudinal study of 41 patients. Eur J Pediatr 1990 Jan;149(4):268-271.
(38) Morava E, Wortmann SB, van Essen HZ, Liebrand van Sambeek R, Wevers R, van Diggelen OP. Biochemical characteristics and increased tetraglucoside excretion in patients with phosphorylase kinase deficiency. J Inherit Metab Dis 2005;28(5):703-706.
(39) Lee PJ, Patel A, Hindmarsh PC, Mowat AP, Leonard JV. The prevalence of polycystic ovaries in the hepatic glycogen storage diseases: its association with hyperinsulinism. Clin Endocrinol (Oxf) 1995 Jun;42(6):601-606.
(40) Ogawa A, Ogawa E, Yamamoto S, Fukuda T, Sugie H, Kohno Y. Case of glycogen storage disease type VI (phosphorylase deficiency) complicated by focal nodular hyperplasia. Pediatr Int 2010 Jun;52(3):e150-3.
(41) Dunger DB, Holder AT, Leonard JV, Okae J, Preece MA. Growth and endocrine changes in the hepatic glycogenoses. Eur J Pediatr 1982 May;138(3):226-230.
(42) Rake JP, Visser G, Huismans D, Huitema S, van der Veer E, Piers DA, et al. Bone mineral density in children, adolescents and adults with glycogen storage disease type Ia: a cross-sectional and longitudinal study. J Inherit Metab Dis 2003;26(4):371-384.
(43) Soejima K, Landing BH, Roe TF, Swanson VL. Pathologic studies of the osteoporosis of Von Gierke's disease (glycogenosis 1a). Pediatr Pathol 1985;3(2-4):307-319.
(44) Banugaria SG, Austin SL, Boney A, Weber TJ, Kishnani PS. Hypovitaminosis D in glycogen storage disease type I. Mol Genet Metab 2010 Apr;99(4):434-437.
(45) Cabrera-Abreu J, Crabtree NJ, Elias E, Fraser W, Cramb R, Alger S. Bone mineral density and markers of bone turnover in patients with glycogen storage disease types I, III and IX. J Inherit Metab Dis 2004;27(1):1-9.
(46) Huijing F, Fernandes J. X-chromosomal inheritance of liver glycogenosis with phosphorylase kinase deficiency. Am J Hum Genet 1969 May;21(3):275-284.
(47) Rosen DS, Foster C. Delayed puberty. Pediatr Rev 2001 Sep;22(9):309-315. (48) Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee.
1995;854. (49) National Osteoporosis Foundation, Washington DC. Physician’s Guide to Prevention and Treatment of
Osteoporosis. 2003.
25

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
(50) Prevention and management of osteoporosis: report of a WHO Scientific Group. Geneva: World Health Organization; 2003.
(51) Hendrickx J, Dams E, Coucke P, Lee P, Fernandes J, Willems PJ. X-linked liver glycogenosis type II (XLG II) is caused by mutations in PHKA2, the gene encoding the liver alpha subunit of phosphorylase kinase. Hum Mol Genet 1996 May;5(5):649-652.
(52) Dunger DB, Leonard JV, Preece MA. Patterns of growth in the hepatic glycogenoses. Arch Dis Child 1984 Jul;59(7):657-660.
(53) Naveh Y, Berant M. Assessment of liver size in normal infants and children. J Pediatr Gastroenterol Nutr 1984 Jun;3(3):346-348.
(54) Deligeorgis D, Yannakos D, Panayotou P, Doxiadis S. The normal borders of the liver in infancy and childhood. Clinical and x-ray study. Arch Dis Child 1970 Oct;45(243):702-704.
(55) American Gastroenterological Association. American Gastroenterological Association medical position statement: evaluation of liver chemistry tests. Gastroenterology 2002 Oct;123(4):1364-1366.
(56) Ghoraishian SM, Hekmati Moghaddam SH, Afkhami-Ardekani M. Relationship between Anti-Thyroid Peroxidase Antibody and Thyroid Function Test. Iran J Immunol 2006 Sep;3(3):146-149.
(57) Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab 2002 Feb;87(2):489-499.
(58) Melis D, Pivonello R, Parenti G, Della Casa R, Salerno M, Lombardi G, et al. Increased prevalence of thyroid autoimmunity and hypothyroidism in patients with glycogen storage disease type I. J Pediatr 2007 Mar;150(3):300-5, 305.e1.
(59) Pomorski L, Bartos M, Matejkowska M, Kuzdak K. The influence of a single acetic acid and lactic acid injection on rat normal thyroid tissue. Cesk Patol 2002 Jul;38(3):107-112.
(60) Geberhiwot T, Alger S, McKiernan P, Packard C, Caslake M, Elias E, et al. Serum lipid and lipoprotein profile of patients with glycogen storage disease types I, III and IX. J Inherit Metab Dis 2007 Jun;30(3):406.
(61) Rosenfeld EL, Chibisov IV, Karmansky IM, Tabolin VA, Chistova LV, Leontiev AF. Serum lipoproteins of patients with glycogen storage disease. Clin Chim Acta 1980 Mar 14;102(1):99-104.
(62) Lee P, Mather S, Owens C, Leonard J, Dicks-Mireaux C. Hepatic ultrasound findings in the glycogen storage diseases. Br J Radiol 1994 Nov;67(803):1062-1066.
(63) Takamura M, Mugishima H, Oowada M, Harada K, Uchida T. Type La glycogen storage disease with focal nodular hyperplasia in siblings. Acta Paediatr Jpn 1995 Aug;37(4):510-513.
(64) Lee PJ, Leonard JV, Dicks-Mireaux C. Focal fatty liver change in glycogenosis type 1 A. Eur J Pediatr 1995 Apr;154(4):332.
(65) Lee PJ. Glycogen storage disease type I: pathophysiology of liver adenomas. Eur J Pediatr 2002 Oct;161 Suppl 1:S46-9.
(66) Labrune P, Trioche P, Duvaltier I, Chevalier P, Odievre M. Hepatocellular adenomas in glycogen storage disease type I and III: a series of 43 patients and review of the literature. J Pediatr Gastroenterol Nutr 1997 Mar;24(3):276-279.
(67) Lee PJ, Leonard JV. The hepatic glycogen storage diseases--problems beyond childhood. J Inherit Metab Dis 1995;18(4):462-472.
(68) Bianchi L. Glycogen storage disease I and hepatocellular tumours. Eur J Pediatr 1993;152 Suppl 1:S63-70. (69) Migeon BR, Huijing F. Glycogen-storage disease associated with phosphorylase kinase deficiency: evidence
for X inactivation. Am J Hum Genet 1974 May;26(3):360-368. (70) Akman HO, Sheiko T, Tay SK, Finegold MJ, Dimauro S, Craigen WJ. Generation of a novel mouse model that
recapitulates early and adult onset glycogenosis type IV. Hum Mol Genet 2011 Sep 13. (71) Grinshpun A, Condiotti R, Waddington SN, Peer M, Zeig E, Peretz S, et al. Neonatal gene therapy of
glycogen storage disease type Ia using a feline immunodeficiency virus-based vector. Mol Ther 2010 Sep;18(9):1592-1598.
(72) Billingsley GD, Cox DW, Duncan AM, Goodfellow PJ, Grzeschik KH. Regional localization of loci on chromosome 14 using somatic cell hybrids. Cytogenet Cell Genet 1994 66(1):33-38
26

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Appendices
I. Invitation letter
II. Pedigree
III. Abstract (Dutch)
27

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
I. Invitation letter
Beatrix KinderkliniekHanzeplein 1
Postbus 30001
9700 RB Groningen
Universitair Medisch Centrum Groningen
KindergeneeskundeSectie: metabole ziektenHoofd sectie: Prof.dr. G.P.A. Smit
Aan:Dhr/Mw. …
Betreft: uitnodiging extra poliklinische controle
Groningen, 7 april 2011
Geachte meneer/mevrouw, danwel ouder/verzorger van bovengenoemde
patiënt(e),
Binnen de afdeling metabole ziekten van het Beatrix Kinderziekenhuis wordt onderzoek gedaan naar levergebonden glycogeenstapelingsziekten (GSD). De afdeling staat bekend als internationaal expertisecentrum voor patiënten met diverse vormen van GSD.
Er is nog relatief weinig bekend over het natuurlijk beloop van GSD type VI (fosforylase deficiëntie) en type IX (fosforylase b-kinase deficiëntie) op langere termijn. Mede om toekomstige patiënten beter voor te kunnen lichten en te behandelen is het belangrijk om wetenschappelijk onderzoek te blijven doen. Omdat u bij onze afdeling bekend bent (geweest) met deze vormen van GSD, wordt u van harte uitgenodigd om deel te nemen aan deze (extra) uitgebreide poliklinische controle, die onderdeel is van een onderzoeksproject.
Er wordt een dezer dagen telefonisch contact met u opgenomen voor deze poliklinische controle. Wij zullen proberen zoveel mogelijk familieleden op dezelfde dag uit te nodigen. Als u reeds een afspraak heeft staan in de maanden mei, juni of juli verandert er niets.
Tijdens dit poliklinische bezoek zal een vragenlijst worden afgenomen en wordt er lichamelijk onderzoek uitgevoerd. Tevens zal er aanvullend onderzoek
28

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
plaatsvinden in de vorm van bloedafname, urineonderzoek, het maken van een echo van de buik en een botdichtheidsmeting. Individuele uitslagen zullen 4 weken na het polikliniek bezoek worden besproken op het telefonisch spreekuur. Zodra de gezamenlijke gegevens bekend zijn, zullen wij die terugkoppelen tijdens de eerstvolgende jaarlijkse GSD patiënten bijeenkomst in ons ziekenhuis. Mocht u nog vragen hebben dan kunt u ten aller tijde contact opnemen met onze secretaresse op telefoonnummer 050-3614944.
Hopende u op deze manier voldoende geïnformeerd te hebben en vertrouwend op uw medewerking, verblijven wij,
Met vriendelijke groeten,
Dr TGJ Derks,Kinderarts fellow metabole ziekten
Mw A Muller,Semi-arts onderzoeker metabole ziekten
Prof dr GPA Smit,Kinderarts metabole ziekten
29

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
II. Pedigree
Fig.5. Pedigree as it was published in 1969 by Huijing and Fernandes.(46) The red boxes indicate index patients from whom the branches are extended with their novel descendants.
Fig.5.a-b. Pedigree with cases of X-linked GSD IX. a novel branch of the pedigree; three descendants of patient V-5 were included; b extension of the branch from heterozygous patient IV-13 with a female patient. Patient and her father were included.
30

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
31
Fig.
5c. e
xten
sion
of th
e pe
digr
ee w
ith th
e ne
xt g
ener
ation
of d
esce
ndan
ts fr
om h
eter
ozyg
ous p
atien
t IV
-8. S
ix p
atien
ts w
ere
incl
uded
.

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
III. Abstract (Dutch)
Achtergrond Glycogeenstapelings ziekten (GSD) zijn erfelijke stofwisselingsziekten waarbij vooral de lever en skeletspieren zijn aangedaan. Er bestaan verschillende vormen van levergebonden GSD’s, waarvan wordt verondersteld dat GSD type VI en IX de mildste vormen zijn. Deficiëntie van de enzymen fosforylase en fosforylase b-kinase veroorzaakt een beperkte mogelijkheid tot het vrijmaken van glucose uit glycogeen dat is opgeslagen in de lever. Dit veroorzaakt dat patiënten zich presenteren met hypoglycemie tijdens periodes van vasten, hepatomegalie, een vertraagde lengtegroei en biochemische afwijkingen. Er bestaat een grote variabiliteit in klinisch fenotype bij patiënten met GSD VI en IX en er is weinig bekend over de lange termijn complicaties. Het doel van deze studie is meer inzicht te krijgen in het klinisch beloop en de frequentie van lange termijn complicaties zodat er aanbevelingen kunnen worden gedaan voor de behandeling en follow-up van volwassen patiënten. Wanneer er geen aanwijzingen zijn voor een X-gebonden overervingspatroon is DNA analyse de enige mogelijkheid om onderscheid te maken tussen GSD VI en IX, aangezien het klinisch beeld van beide GSD’s veel overeenkomsten vertoont. Ten behoefte van het verlenen van optimale zorg bij oudere patiënten en het geven van adequate (genetische) voorlichting beschrijven wij het natuurlijk beloop van patiënten met GSD VI en IX.Methode Het eerste deel van de studie bestond uit een retrospectieve analyse van de medische dossiers. Aansluitend werd cross-sectioneel onderzoek verricht. Dit onderzoek bestond uit een (extra) poliklinische controle met anamnese, lichamelijk onderzoek, laboratorium onderzoek, een echo abdomen en een botdichtheidsmeting. Twintig patiënten met GSD VI en IX, afkomstig uit 14 gezinnen, werden geïncludeerd. Tevens werd bij 16 patiënten DNA analyse ingezet.Resultaten Retrospectieve analyse bevestigde dat klinische kenmerken zoals, hepatomegalie, hypoglycemie, vertraagde lengtegroei en achterblijven van motorische ontwikkeling meer op de voorgrond stonden bij jongere patiënten. Er bleek sprake te zijn van een sterk verband tussen hepatomegalie en leeftijd. Hiernaast werden bij laboratoriumonderzoek verhoogde concentraties van TSH (25%), lever transaminasen (25%), triglyceriden (30%) en urinezuur (35%) gevonden en een lage concentratie van vitamine D (45%). Het gebruik van XO-remmers bleek een gunstig effect te hebben op verhoogde urinezuur concentraties. Middels echo abdomen werden bij 2 patiënten focale laesies in de lever gevonden en op basis van de gevonden T-scores bij DEXA-scan werd bij 41% van de patiënten de diagnose osteopenie danwel osteoporose gesteld. Bij 9 van de 20 patiënten werd dezelfde mutatie van het PHKA2-gen op het X-chromosoom gevonden (c.3614 C>T).Conclusie Dit onderzoek bevestigde dat de meerderheid van de klinische kenmerken verbeteren wanneer patiënten ouder worden. Toch wordt, gezien diverse opvallende bevindingen, jaarlijkse follow-up van volwassen patiënten met GSD VI en IX sterk aanbevolen. Gericht laboratoriumonderzoek, inclusief de bepaling van 25(OH)D, wordt geadviseerd. Aanvullende evaluatie van de schildklierfunctie moet alleen worden uitgevoerd op indicatie. De behandeling van verhoogde urinezuur concentraties bestaat uit XO-remmers. Een echo abdomen voor de detectie van focale laesies in de lever wordt geadviseerd. Gezien de hoge incidentie van osteopenie en osteoporose wordt optimalisatie van de calciumintake met, wanneer geïndiceerd suppletie van vitamine D, aanbevolen. DEXA-scan ter controle van de botdichtheid zou tweejaarlijks moeten worden uitgevoerd.
32

GSD VI and IX; additional recommendations for follow-up and treatment beyond childhood
Hiernaast is DNA analyse van belang voor het stellen van de juiste diagnose en voor het kunnen verstrekken van adequate voorlichting over erfelijkheid van GSD VI en IX.
33