Embed Size (px)
Citation preview

Identification of immunotherapeutic targets in
melanoma
Lycke WoittiezS1418165
Research Internship2 February 2009 – 26 June 2009
The Wistar Institute, Philadelphia, USACancer immunology
Local supervisor: Shyam Somasundaram(Senior scientist)
Principal Investigator: Professor D.V.M. HerlynFaculty supervisor: Dr. W.M. Smit

ContentsSummary...................................................................................................................................31. Introduction........................................................................................................................4
1.1 Melanoma...................................................................................................................4
1.2 Immunology and melanoma.......................................................................................4
1.3 Immunotherapy in melanoma.....................................................................................5
1.4 Modified peptides.......................................................................................................6
1.5 Improving the immune response................................................................................7
1.6 BRAF mutation...........................................................................................................7
1.7 Goal and hypothesis...................................................................................................8
2 Material and methods........................................................................................................92.1 Patients.......................................................................................................................9
2.2 Cell lines.....................................................................................................................9
2.3 Determination of the HLA-A2 status...........................................................................9
2.4 Determination of the BRAF mutation status.............................................................10
2.4.1 DNA purification................................................................................................10
2.4.2 Polymerase Chain Reaction (PCR)...................................................................10
2.4.3 Gel electrophoresis...........................................................................................11
2.4.4 TOPO cloning....................................................................................................12
2.4.5 Miniprep.............................................................................................................14
2.4.6 Restriction digestion..........................................................................................14
2.4.7 Sequencing.......................................................................................................15
2.5 Peptide binding assay..............................................................................................15
2.6 PLG-encapsulation...................................................................................................16
2.7 T cell proliferation assay...........................................................................................16
2.8 Phenotyping of T-cells..............................................................................................18
2.9 Cytotoxicity assay.....................................................................................................19
1

3 Results.............................................................................................................................203.1 Determination of the HLA-A2 status.........................................................................20
3.2 Determination of the BRAF mutation status.............................................................21
3.2.1 DNA Purification................................................................................................21
3.2.2 Polymerase Chain Reaction..............................................................................21
3.2.3 Gel electrophoresis...........................................................................................22
3.2.4 TOPO cloning....................................................................................................22
3.2.5 Miniprep.............................................................................................................22
3.2.6 Restriction digestion..........................................................................................22
3.2.7 Sequencing.......................................................................................................23
3.3 Peptide binding assay..............................................................................................24
3.4 T-cell proliferation assay...........................................................................................25
3.5 Phenotyping of T-cells..............................................................................................26
3.6 Cytotoxicity assay.....................................................................................................27
4 Discussion.......................................................................................................................304.1 Determination of the HLA-A2 status.........................................................................30
4.2 Detection of the BRAF mutation status....................................................................30
4.3 Peptide binding assay..............................................................................................31
4.4 T cell proliferation assay...........................................................................................31
4.5 Phenotyping of T-cells..............................................................................................31
4.6 Cytotoxicity assay.....................................................................................................32
4.7 General conclusion...................................................................................................32
5. List of abbrevations..........................................................................................................346. Citations...........................................................................................................................357. Word of thanks.................................................................................................................378. Summary of research in Dutch........................................................................................38
2

Summary
IntroductionMelanoma is a common malignant tumor of the skin, with a bad prognosis when disseminated disease is present. Conventional therapies are of little benefit because most tumor cells are relatively chemoresistant. Lymphocyte infiltrates in or around the melanoma are associated with prolonged survival, suggesting a cellular immune response against melanoma. Active immunotherapy has been shown to stimulate the immune response and has been subject of previous studies as therapeutic modality in malignant melanoma. Tumor antigenic peptides can stimulate the immune response. Modification of these peptides may result in a stronger binding to HLA molecules, resulting in an increased immune response. Previous studies showed that peptides spanning the BRAFV600E mutation, a mutation in the Map-kinase pathway that is present in 70% of melanoma cells, were immunogenic. In this study we determined whether modified BRAFV600E peptides that bind stronger to HLA molecules, may induce a stronger immune response than unmodified BRAFV600E peptides in melanoma.
Material and methodsTwenty-three melanoma patients were included in this study. The HLA-A2 status was determined by flow cytometry. Genomic DNA was isolated from tumor cells and used to determine the BRAFV600E mutation status by amplification in a Polymerase Chain Reaction (PCR), followed by sequencing of the amplified DNA fragment using the primer SP6 and reverse primer T7, and M13 forward and M13 reverse primer. A T2 peptide binding assay was performed to determine the binding ability of modified peptides to T2 cells, to select the peptides with a high binding ability. A standard lymphocyte proliferation assay (3HT-thymidine incorporation assay) was used to determine the extent of proliferation of T-cells cultured with various peptides. Proliferating lymphocytes were phenotyped to determine whether it were CD4 (Th) or CD8 (CTL) cells. The proliferating cells were expanded further in the presence of IL-2 and used in a cytotoxicity assay, to determine whether they were efficient in killing tumor cells.
ResultsLymphocytes of 14 out of 23 patients were tested for their HLA-A2 status. Four (29%) of those patients were HLA-A2 positive, and thus could be used for further experiments. Another nine patients were tested positive for HLA-A2 before and were therefore included in this study.Four of the 11 patients tested for their BRAF status, had the V600E mutation. The T2 binding assay showed a strong binding of modified peptide 4, which is altered in both anchor residues, compared to the unmodified peptides. The lymphocyte proliferation assay showed a low proliferation in all tested cells, except WM35. The phenotype of the proliferating lymphocytes was mostly of the CD8 subtype. The cytotoxicity assay gave inconsistent results, with no significant difference in cytotoxicity of the modified peptides compared to the unmodified peptides.
Conclusion Modified melanoma peptide 4 bound stronger in a peptide binding assay than the unmodified peptides and may therefore be a good candidate for further studies with specific cellular immunotherapy in patients with malignant melanoma.
3

1. Introduction
1.1 MelanomaMelanoma is a malignant tumor of the skin. It is the 6th most common malignancy in men and the 7th most common in women. The incidence of melanoma has risen markedly during the second half of the 20th century (1, 2).Melanoma is divided in four stages. Stage I and II represent localized disease, stage III involves regional nodal metastases and stage IV indicates the presence of distant metastases. The stage of melanoma at presentation is an important determinant of the prognosis. If melanoma is detected early it is highly curable, with a 5-year survival rate of localized disease of 99%. When distant metastases are present, the 5 year survival rate is only 15%. Approximately 3% of the patients present with distant metastases. The survival of melanoma patients has not changed in the past 35 years. This is mostly due to the fact that there have not been any true advances in the treatment strategy for melanoma (1, 2). The current management options for melanoma are surgery, radiation, chemotherapy and immunotherapy. Those therapies can be used individually or in combination (2, 3). Surgery is the treatment of choice for the resection of solitary lesions or solitary metastatic disease and can significantly improve survival in these patients. Radiotherapy can be effective for palliation in patients with brain metastases, spinal cord compression or painful bone metastases (3).Dacarbazine is the only approved chemotherapeutic agent for metastatic melanoma in the USA. The response rate is 15-20%. The combination of different chemotherapeutic regimens has approximately the same response rate. Major disadvantages of chemotherapy are the toxic side effects that often occur and the chemoresistance of the cancer cells (2, 3).Traditionally, anti-cancer drugs are designed to interfere with DNA-synthesis and the cell cycle. This method affects rapidly dividing cells, like cancer cells, more than normal cells. However, these therapies have many side effects because other rapid dividing cells in the body, such as bone marrow cells, are also affected. A new generation of experimental drugs targets signaling pathways and DNA repair enzymes. Drugs targeting the Map kinase pathway are currently tested in clinical trials. Another new treatment strategy for melanoma is the use of immunotherapy.
1.2 Immunology and melanomaThe concept of immunosurveillance indicates that the immune system can recognize precursors of cancer. In most cases, the immune system will destroy those malignant precursor cells. However, sometimes cancer does develop, despite the immune response (4).The immune system identifies tumor cells through the recognition of tumor associated antigens (TAA) that are presented as short peptides in the context of HLA class I or II. These complexes can be expressed on the tumor cell itself, resulting in direct priming of T cells upon recognition, or on professional antigen presenting cells (APCs) that have picked up antigens and processed it for indirect priming of T-cells. Melanoma associated antigens (MAAs) can generate both humoral and cell-mediated immune responses (5, 6). The immune response in melanoma patients can cause spontaneous regression of melanomas, probably due to infiltrating T cells. T cell infiltrates in primary melanoma are prognostic of disease outcome, and tumor infiltrating lymphocytes (TILs) have been associated with regression of established metastases in 15-30% of the patients. Antigen-specific CD8+ T-lymphocytes are the major subpopulation of TILs (5, 7-10). Disease free status in melanoma patients was associated with a strong T-cell reaction.
4

Unfortunately, the spontaneous T-cell response against melanoma associated antigens is rather weak in most patients (9).The above mentioned observations illustrate the important role of the immune system in the prevention and regulation of cancer. Therefore, investigators hypothesized that therapeutic modalities that induce or modulate the immune response might be beneficial for melanoma patients. This led to the introduction of immunotherapy as treatment modality for melanoma patients.
1.3 Immunotherapy in melanomaImmunotherapy is a relatively new treatment strategy for melanoma. Tumor-specific T cells, spontaneous regression of primary tumors and regression of metastatic lesions induced by immune-modulatory therapies have been shown in humans in clinical trials (8). Immunotherapy can be specifically targeted to tumor tissues, leaving normal tissues intact (11). The most attractive targets for immunotherapy are cell characteristics on which cancer cells are dependent for progression and survival (12). Immunization can be performed both passive and active. The most common strategy used in melanoma is active immunization. There are two main forms of active immunization, i.e. the administration of whole tumor cells or tumor cell lysates, and vaccination with peptides. Vaccination with whole tumor cells can be performed with both autologous and allogeneic cells. The tumor cells are irradiated to make them unable to replicate, and then re-administered to the patient with an immune adjuvant. The advantage of this method is that both humoral and cellular immunity are generated. However, developing the vaccine is a very time-consuming and difficult procedure (13). Anti melanoma-associated antigen response is generated in a fraction of the vaccinated patients. The response rate in early clinical trials was less than 10% without a clear correlation with the induced immune response (5, 7).A more common form of vaccination, and the one used in this study, is the use of peptide or protein based vaccines. These vaccines are made of well defined melanoma associated antigens (MAA) peptide epitopes (5). After administration of the peptide, it is endocytosed by professional antigen presenting cells. Those cells present the peptides on MHC class II molecules to CD4+ cells and on MHC class I molecules to CD8+ cells. The T cells are activated and recognize antigens presented by MHC class I molecules on tumor cells. After recognition of the tumor cells, the cytotoxic T cell will attack and kill the melanoma cells (figure 1).Different tumor-optimized peptide analogs have been identified. However, each peptide based vaccine is limited to a particular HLA subtype. Furthermore, this therapy only targets a limited number of epitopes. Gene mutation leading to antigen loss can be a problem in this form of vaccination because tumor cells will escape the immune response. Therefore it is critical to identify and target tumor antigens that are vital to maintaining a malignant phenotype (9, 13).
5

Figure 1: mechanism of CTL activation after peptide vaccination. Source: www.medscape.com
Vaccines have shown effect in other forms of cancer, such as immunotherapy targeting EGFRvIII in patients with malignant melanoma (14), and a monoclonal antibody targeting HER2/neu in breast cancer patients (15). In previous studies in melanoma the HLA-A2 molecule was shown to be important for the melanoma cell recognition by autologous T-lymphocytes. HLA-A2 is a MHC class I molecule, that is present in most Caucasian people (16, 17).There have been many trials using peptide based vaccines in melanoma patients, but the immune responses were detected inconsistently (13, 18). 10-30% Of the patients receiving melanoma peptides had partial or complete tumor regression (19). In some patients a detectable peptide-specific immune response was associated with regression of single metastases (5, 18). Unfortunately, the tumor response does not correlate well with the T-cell response measured in peripheral blood lymphocytes (5, 13, 20). Objective regression and long term stabilization of metastatic melanoma have been observed in a number of vaccine trials in individual patients. In most cases, tumor regression is associated with a detectable immune response to the vaccine. But the immune responses were also induced in the population without a measurable clinical benefit (18). Therefore, cancer vaccination in patients with melanoma needs further investigation.
1.4 Modified peptidesBecause peptide immunogenicity correlates well with the peptide binding affinity for MHC, an effective strategy to improve the immune response is converting low affinity peptides into high affinity forms (9, 19). These modified peptides can be considerably more immunogenic in vitro and in vivo due to enhanced binding affinity to HLA molecules and slower dissociation rate (9, 19, 21). Single amino acid changes can be enough to significantly alter the binding of peptides.T cell responsiveness to an epitope is affected not only by the affinity for the presenting MHC molecule but also by the affinity of the MHC-peptide complex for the T-cell receptor (TCR). Natural tumor antigens elicit relatively weak T cell responses. Amino acid substitutions can increase the stability of the MHC-peptide-TCR complex and can make the immune response significantly more potent (18, 22-24). In this study we will use both modified and unmodified peptides, to evaluate their effect on the immune response.
6

1.5 Improving the immune responseImmunotherapy is not (yet) as effective as the initial studies reported. There have been many clinical trials with peptide vaccination, but only rarely a response rate higher than 20% was found (9). This might have several reasons. The first reason is the presence of regulatory T cells. There is an important role for CD4+CD25+FoxP3+ regulatory T cells (Tregs) in limiting the anti tumor immune response in vivo. Regulatory T cells can suppress the activation of tumor antigen-specific CD8+ effector T cells in vitro, and high levels of Treg cells correlate with poor survival. The tumor uses many other immune suppressive mechanisms (25, 26).Cancer cells downregulate or lose their expression of HLA class I molecules. This abrogates antigen recognition and tumor cell killing by CD8+ CTL, and is considered the most common strategy exploited by tumor cells to escape T-cell control. Partial or complete loss of class I HLA expression can be detected in up to 67% of metastatic melanomas (9). Furthermore, downmodulation of molecules involved in antigen processing and presentation, such as peptide transporters associated with antigen processing and proteasome subunits has been reported (4, 9, 27). Other mechanisms of tumor cells to evade the immune response are the downregulation of tumor-associated antigens, the development of mechanisms to avoid being killed by T cells, the downregulation of death receptors, a lack of costimulatory molecule expression, the secretion of immunosuppressive substances, the expression of pro-apoptotic molecules and the blockage of the apoptosis pathway (4, 9, 25, 27).The most important strategies to overcome the tolerance of cancer cells for the immune system and thus to improve the efficacy of vaccination, are the co-injection of cytokines, the use of co-stimulatory molecules, depletion of the lymphocytes pre-vaccination, immunomodulation by antineoplastic drugs, or blockage of the negative co-stimulatory molecules with anti-CTLA-4 AB (13). One of the main approaches is the combination of immunotherapy with chemotherapy, called biochemotherapy. Chemotherapy has direct effects on the tumor or host environment, such as induction of tumor cell death, elimination of Tregs and/or enhancement of tumor cell sensitivity to lysis by CTL. These may account for the enhanced effect of immunotherapy in combination with chemotherapy. However, in phase III studies, no clear improvement of overall survival was seen with biochemotherapy (3, 23, 28). Other therapies that are being used are IL-2 and IFN-α, that are approved as immunotherapeutic targets for melanoma in the USA. Those therapies modulate the immune response against melanoma. Furthermore, CLTA4 blockade, tremelimumab, other anti-CTLA4 monoclonal antibodies and TLR9 agonsists are used in the treatment of melanoma (7). CLTA4 is a negative costimulatory molecule, so by blocking this molecule the immune response will be improved.
1.6 BRAF mutationThe RAS-RAF-MEK-ERK-MAP kinase pathway mediates cellular responses to growth signals (29, 30). RAF is a point of regulation in the MAP kinase pathway. There are different RAF kinases, all are activated by the RAS small GTPase regulatory phosphorylation events and scaffolding proteins. Different RAF isoforms combine common ad unique mechanisms to regulate RAF kinase activity (31). Mutated BRAF proteins have an elevated kinase activity, which is a crucial step in the initiation of neoplasia (30). BRAF can act as a potent oncogene in the early stages of melanoma development (32). BRAF stimulates constitutive ERK signaling, stimulating proliferation and survival and providing essential tumor growth and maintenance functions. It contributes to neo-angiogenesis and is implicated in several aspects of melanoma induction and progression (12). Melanomas are dependent on the activation of the RAS-MAP kinase pathway for replication and survival (33).
7

The BRAF mutation is present in 66% of melanomas but also in 82% of benign nevi (12, 30, 32, 34). Thus BRAF mutation alone is insufficient for melanoma initiation (12). It is possible that the mutation in concert with other oncogenic events will promote tumor formation in nevi (29). A single substitution in the kinase domain (V600E) accounts for 80%-95% of these mutations (29, 30, 35). Somatic mutations in the BRAF proto oncogene are present in a wide variety of malignancies, namely melanoma, papillary thyroid cancer and colon cancer (36). Because of its tumor specificity and expression in the majority of melanomas, BRAFV600E is a potential immunotherapeutic target in melanoma. Following knockdown with RNA interference methods, melanoma cells showed profound inhibition of the MAP kinase cascade and a diminished proliferative activity. Potential methods to target BRAF function are kinase inhibition and protein depletion. Knockdown of BRAF expression and inhibition of downstream signaling in human melanoma cells causes growth arrest, promotes apoptosis and prevents colony formation (36). Increased apoptosis when BRAF expression is downregulated supports a role for oncogenic BRAF driven MEK/ERK over activation (22).Because it is expressed intracellularly and not on the surface of tumor cells, BRAF is a target for T cells but not for B cells (antibodies). Anchors for HLA class I and class II are expressed in close vicinity of the mutation, suggesting that both CD8+ and CD4+ T lymphocytes can be induced. There is a positive correlation between BRAFV600E mutation status in melanoma lesions and the immune responses to the mutated epitope (35). Lymphoproliferative responses to BRAFV600E are HLA-A2 restricted. The proliferating lymphocytes are cytotoxic against HLA-A2+/BRAFV600E melanoma cells. The high prevalence (approximately 50%) of HLA-A2 among melanoma patients renders HLA-A2-restricted BRAFV600E peptides attractive candidate vaccines for these patients (35, 37). Much research has been conducted with agents that specifically target BRAF. Unfortunately, they all met with limited success. In this study, we use modified BRAFV600E peptides to induce an immune response in HLA-A2+ patients.
1.7 Goal and hypothesisThe goal of this translational study is to determine whether modified BRAFV600E peptides may induce a stronger immune response than unmodified BRAFV600E peptides against melanoma cells in vitro. The project goal is to determine whether modified BRAFV600E vaccines can be used in the treatment of melanomas. The hypothesis for this study is that an increased binding affinity to HLA molecules will result in better antigen presentation, and hence better immune responses will be induced. Thus, modified BRAFV600E peptides will induce a stronger immune response than unmodified BRAFV600E peptides in melanoma patients.
8

2 Material and methods
2.1 PatientsTwenty three melanoma patients were included in this study. These patients were selected because their blood samples were available in the lab. All human blood and tumor samples were obtained under informed consent.
2.2 Cell linesOne melanoma cell line (WM35) was established from a patient with a primary melanoma. The other 22 cell lines (PD 2027, JB 2008, 2035, 3539, MS 2009, 3542, GT 03, NC 02, 3473, 047437207, 2038, 3700, TF 1011, 1039, 3457, 3451, 3623, 3681, 3705, 3502, 3622, BRAF-CS) were established from patients with metastatic melanomas. All melanoma cell lines were maintained in melanoma medium containing MCDB-153 medium (Sigma, St. Louis, MO) with L-15 medium (Sigma).
2.3 Determination of the HLA-A2 status. In previous studies the immune response to BRAFV600E appeared to be HLA-A2 specific (35). Therefore, we selected HLA-A2 positive patients for our study. Flow cytometry was used to determine the HLA-A2 status.
Flow cytometry is also called FACS (Fluorescence-Activated Cell Sorting). Cells in suspension flow one at a time through a focused laser beam at rates up to several thousand particles per second. Light scattered and fluorescence emitted by the cells is collected, filtered, digitized and sent to a computer for analysis. Flow cytometry measures the binding of specific fluorochrome-labeled probes to specific epitopes of cells and compares the resultant fluorescence to the background fluorescence of the unstained cells. This allows the detection of these epitopes.
We collected Peripheral Blood Mononuclear Lymphocytes or used transformed Epstein - Barr virus B (PBML/EBV-B) cells which were not HLA typed before from 14 melanoma patients. After thawing, the cells we cultured in RPMI 1640 (GIBCO, Invitrogen, Carlsbad, CA) + 10% Fetal Bovine Serum (FBS) (PAA Laboratories GmbH, Pasching, Austria).
After expansion of sufficient amounts of cells, the cell suspension was distributed in 1.5 ml tubes. They were spun down, the supernatant was removed and the cells were resuspended in 50µl FACS buffer (PBS (Phosphate Buffered Saline, Gibco), FBS 5% (PAA laboratories), Na-azide 0.02%).From each patient three samples were tested, i.e. one with control antibody (BD Pharmingen (San Jose, CA) PE mouse IgG1), one with anti-CD45 antibody (BD Pharmingen, PE mouse anti-human CD45) and one with anti HLA-A2 PE conjugated antibody (BD Pharmingen, PE mouse anti-human HLA-A2). The cells were incubated with the antibodies for 30-40 minutes, then they were washed with FACS buffer and resuspended in 400µl of FACS buffer. Finally, the samples were tested with the FACS CyAn ADP (DakoCytomation, Glostrup, Denmark) or the EPICS XL-MCL (Beckman Coulter, Fullerton, CA) machine. Data were analyzed using FlowJo software (Tree Star Inc., Ashland, OR).
The HLA-A2 status of the 9 other patients was determined earlier.
9

2.4 Determination of the BRAF mutation status We tested the BRAF status of patients 3473 and 3457 in cell lines, and we used tumor tissue to determine the BRAF mutation status for patient 3700. Patients without the mutation will have the Wild type BRAF in both DNA strands. Patients with the mutation will most likely have the mutation in one DNA strand, while the other strand is wild type. Only very rarely, both DNA strands are mutated.
2.4.1 DNA purificationDNA purification is a technique used to isolate DNA from cells. After lysing the cells and nuclei with a lysis solution and removal of the cellular proteins with a salt precipitation step, the DNA is concentrated and desalted by isopropanol precipitation. The result of this procedure is only the DNA without the cells and cell contents.
We performed DNA purification of the three samples, using the Wizard Genomic DNA Purification Kit (Promega (Madison, WI)), according to the prescribed protocol (38). Melanoma cells were cultured in melanoma medium (MCDB-153 medium (Sigma) with L-15 medium (Sigma)). In case of sufficient amounts of cells, we collected 1.5 ml of the cell solution, spun this down and washed the cells once with PBS (Gibco). Then we added 600µl Nuclei Lysis solution and we pipetted until no visible clumps remained. We added 3µl of RNAse solution to eliminate RNA, mixed the sample and incubated the mixture 60 minutes at 37°C. We let the sample cool down to room temperature, added 200µl of Protein Precipitation Solution and vortexed the samples at high speed for 20 seconds. Then we cooled the samples on ice for 5 minutes. We centrifugated the samples down and transferred the supernatant containing the DNA to a clean 1.5 ml microcentrifuge tube containing 600µl of room temperature isopropanol. We gently mixed the solution by inversion until the DNA formed thread-like strands. We centrifuged the tubes again and discarded the supernatant. Then we added 600µl 70% ethanol, gently inverted the tubes several times and centrifuged again. We inverted the tube on absorbing paper to air-dry the pellet for 10-15 minutes. The final step was to add 100µl of DNA Rehydration Solution and rehydrate the DNA by incubating at 65°C for 1 hour, while periodically mixing the solution.
After purification of the DNA we tested the samples for DNA content using a spectrophotometer. A spectrophotometer measures the amount of light that a sample absorbs. A beam of light is passed through the sample and the intensity of light is then measured. We used the Nanodrop® ND-1000 Spectrophotometer (Thermo Fisher Scientific Inc, Pittsburgh, PA). This is a full spectrum photometer, meaning that it uses both UV light and visible light (220-750nm). The instrument uses two optical fibers for the measurements. We loaded 2µl of each sample on the machine, and measured the DNA content of each sample using the ND-1000 v3.5.2 software.
2.4.2 Polymerase Chain Reaction (PCR)The polymerase chain reaction is a sensitive, selective and extremely rapid method of amplifying a desired sequence of DNA. Two different oligonucleotide primers hybridize to complementary sequences on opposite strands of DNA and flank the target sequence, which makes this method very specific. The DNA sample is first heated to separate both DNA strands. Then the primers can bind to the DNA, and the strands are copied by DNA polymerase. Repeated cycles of heat denaturation, annealing of the primers and extension of the annealed primers with DNA polymerase results in exponential amplification of DNA segments of defined length (39).
10

To amplify the amount of the DNA fragment with the BRAF coding region, we performed a PCR of the genomic DNA samples. The results of the Nanodrop were used to determine how much DNA solution had to be added to the reaction. We used either 200ng or 500ng of DNA. Table 1 shows the contents of the PCR tubes.
Table 1: Contents of PCR reaction tubes.50µl reaction Control SamplesBuffer 5 µl 5 µl dNTP (deoxyribonucleotide triphosphate) 2 µl 2 µlMgSO4/MgCl 1 µl 1 µlDNA 0 µl 1-5 µlPolymerase/Immunolase 1 µl 1 µlPrimers (1.5+1.5) 3 µl (1.5+1.5) 3 µlH2O 38 µl 33-37 µlTotal 50 µl 50 µl
We performed PCR multiple times to optimize the reaction. We changed the primers, the number of PCR cycles and the annealing temperature (table 2). The chosen primers were known to overlap the region containing the BRAF coding region. To select the primers we used the National Center for Biotechnology Information (NCBI) Basic Local Alignment Search Tool (BLAST).The sequence of the used primers is shown in table 3.
Table 2: Used primers and institution of PCR machineForward primer Reverse primer Expected
length of DNA fragment
Amount of cycles
Annealing temperature
Human BRAF S4
3BRAF kinase fusion
236 bp 30 48°C
Exon5BRAF Exon3BRAF 120 bp 30 48°CExon5 Exon3 119 bp 35 45°C
Table 3: Sequence of used primersPrimer SequenceHuman BRAF S4 5’- CTC TTC ATG GGC TAT TCC -3’3BRAF kinase fusion 5’- CGG TGC TCG AGT TAT CAA GCA TAC AGA CTA AAA TCT
TCT GTT TGG -3’Exon5BRAF 5’- ATA TAT TTC TTC ATG AAG ACC TCA C -3’Exon3BRAF 5’- CAA TCC ACA AAA TAG ATC CAG -3’ Exon5 5'- ATA TAT TTC TTC ATG AAG ACC TCA C -3'Exon3 5'- CCA TCC ACA AAA TAG ATC CAG -3'
2.4.3 Gel electrophoresisTo control whether the desired DNA fragment was obtained, we determined the length of our DNA fragments using agarose gel electrophoresis. This is a method to separate DNA or RNA molecules by size. The DNA is placed into a gel, immersed within an electrophoresis buffer that provides ions to carry a current and a buffer to maintain the pH at a relatively constant value. The gel electrophoresis tray is connected with a positive and a negative electrode, with the negative electrode closest to the DNA. Each DNA molecule possesses a net negative charge resulting from the phosphate group. When loaded in a gel, DNA will migrate through the gel towards the positive electrode with the smaller fragments moving faster than the larger ones. Ethidium bromide is a fluorescent dye that is incorporated in the agarose gel and intercalates between bases of nucleic acids. It can be visualized when it is intercalated in
11

DNA or RNA fragments with an ultraviolet transilluminator. Thus, it allows detection of DNA fragments in gel. The tracking dye added to the DNA samples has a slightly negative charge and thus will travel in the same direction as the DNA. Therefore, the dye is useful for tracking the migration of the DNA (40).
We prepared a 1.2% agarose gel by dissolving agarose powder (Invitrogen) in 1x TBE (Tris-borate-EDTA) buffer and heating this mixture in the microwave for 2 minutes to dissolve the powder in the solution. After allowing the solution to cool down to about 55°C, Ethidium bromide was added in a concentration of 0.5µg/ml. The gel tray was sealed with tape and the comb with multiple wells (lanes) was placed in the tray. After pouring the gel in the gel tray, we allowed it to cool and solidify for 30-60 minutes. Then we removed the comb and the tape, placed the tray in the electrophoresis chamber and covered the gel with electrophoresis buffer 1xTBE. After adding 6µl of tracking dye (Bromophenol Blue) to 50µl of the DNA samples and mixing well, the solutions were loaded in the corresponding lanes of the gel. We ran the gel for 2 hours at 50mV, regularly checking the migration of the tracking dyes.We evaluated the gel using Gel Logic 200 Imaging System (Kodak, Rochester, NY) and Kodak Molecular Imaging Software v.4.0.5.
To isolate the Ethidium bromide stained DNA from the gel, we used the QIAquick Gel Extraction Kit (Qiagen, Valencia, CA), according to the prescribed protocol (41). We cut the bands with the desired length out of the gel using an UV-transilluminator to locate the bands. The pieces of gel were put in 1.5 ml tubes and weighted. We added 3 volumes of Buffer QG to 1 volume of gel. The gel was incubated at 50ºC for 10 minutes, until the gel was completely dissolved. We checked if the color of the mixture was yellow, and then added 1 gel volume of isopropanol and mixed. We added the solution to a QIAquick spin column in a 2 ml collection tube and centrifuged this for 1 minute. We discarded the flow-through and placed the spin column back in the collection tube. Then 0.5 ml of Buffer QG was added to the column and centrifuged for 1 minute. After discarding the flow-through we spun the column for another 1 minute. Then we placed the QIAquick column into a clean 1.5 ml microcentrifuge tube and added 50µl of Buffer EB to the center of the QIAquick membrane. We centrifuged again for 1 minute.
We used Nanodrop to determine the amount of DNA in the tubes as described earlier. The DNA was either sent to sequencing or saved in the freezer.
2.4.4 TOPO cloningTOPO cloning is a technique in which DNA fragments acquired through PCR are inserted into a plasmid vector. Topoisomerase I binds to DNA at specific sites and cleaves the phosphodiester backbone after 5’-CCCTT in one strand. The Topoisomerase I binds to the 3’ T overhangs of the vector. The 3’ A overhangs of the PCR product complement the 3’ T overhangs of the vector and allow for fast ligation (figure 2).
12

Figure 2: Mechanism of TOPO cloning. Source: www.invitrogen.com
Afterwards the plasmid can be transformed into competent bacterial cells. One of the features of the vector is the resistance for ampicillin and kanamycin which facilitates a quick selection of bacterial colonies that take up the plasmid vector during transformation on plates containing these antibiotics. Another useful feature is the EcoR I sites on either side of the insert that enable the insert to be easily removed by EcoR I restriction enzymes (figure 3) (39, 42, 43).
Figure 3: map of pCR®II-TOPO, www.invitrogen.com
For TOPO cloning we used the pCR®II-Blunt-TOPO® kit (Invitrogen, Carlsbad, CA) according to the prescribed protocol.We used the PCR products acquired by using primers Exon3 and Exon5, after checking the correct length of the DNA fragments with gel electrophoresis and purifying the DNA out of the gel. We checked the DNA content using NanoDrop. To produce the Blunt-End PCR products
13

we added 4µl of the PCR products in 1.5ml tubes. Then 1µl Salt Solution and 1µl pCR®II-Blunt-TOPO® solution were added. The solution was mixed and incubated for 10 minutes at room temperature. After this, the tubes were stored at ice and we proceeded to the transformation of cells.
We used the One Shot® TOP10 Chemically Competent E. Coli according to the prescribed protocol. We thawed one vial of One Shot® TOP10 chemically competent cells for each transformation. We added 3µl of DNA solution obtained in step 1 of the TOPO cloning into each vial and mixed gently. We incubated the vials on ice for 30 minutes, and afterwards heat-shocked them for 30 seconds at 42°C. After heat-shocking the vials were put on ice for 2 minutes. We added 250µl of room temperature SOC medium (Super Optimal broth with catabolite repression through added glucose), then the vials were put in the shaking incubator and we let them shake at 37°C for 1 hour.Then we spread the samples on agar plates containing kanamycin. Each sample was spread on 2 plates, with on one plate 20µl and on the other 200µl of solution. The agar plates were put in the incubator for 48 hours. After 48 hours the colonies were collected and transferred to tubes containing 5ml lysogeny broth (LB) medium with 50µg/ml kanamycin. The solution was put in the shaking incubator at 37°C overnight.
2.4.5 MiniprepTo isolate the plasmid DNA from the bacteria we used The Manual FastPlasmidTM Mini Kit from 5Prime (Gaithersburg, MD), according to the prescribed protocol (44).The tubes with bacteria from the TOPO cloning were collected after they incubated overnight. We estimated the amount of bacterial growth by judging how turbid the fluids were. If the fluid was turbid, we spun the solution down at 8000rpm for 5 minutes. Then the medium was removed by decanting. We added 400µl of ice cold Complete Lysis Solution and mixed thoroughly by constant vortexing at highest speed for 30 seconds. Then we incubated at room temperature for 3 minutes.After incubation the lysate was transferred to a Spin Column Assembly by decanting, and centrifuged at maximum speed for 60 seconds. We added 400µl of diluted Wash Buffer and centrifuged again 60 seconds at maximum speed. We decanted the filtrate from the Waste Tube, replaced the Spin Column in the Waste Tube and centrifuged 60 seconds at maximum speed again. Then the Spin Column was transferred to a Collection Tube, and 50µl of Elution Buffer was added directly to the center of the Spin Column membrane. The Collection Tube was capped over the Spin Column and was centrifuged at maximum speed for 60 seconds again. Then we removed and discarded the Spin Column. The eluted DNA was used immediately or stored at -20°C.
2.4.6 Restriction digestionRestriction digestion is the process of cutting DNA molecules into smaller pieces with specific enzymes called restriction endonucleases. These enzymes recognize specific sequences in the DNA molecule and cut the DNA wherever that sequence occurs. EcoR1 is an endonuclease enzyme isolated from strains of E. Coli. It is used in isolation and restriction of bacterial plasmid DNA (39). Because the plasmid used in the TOPO cloning has an EcoR1 site on either side of the insert (figure 3), EcoR1 is very suitable to remove the insert from the plasmid.
To extract the DNA fragment from the plasmid we used EcoR1 cutting (New England Biolabs, Ipswich, MA). 15µl Of the purified plasmid, produced by Miniprep was added to a 1.5ml tube. In every tube 5µl EcoR1 buffer and 1µl EcoR1 enzyme were added, and the
14

volume was filled till 50µl by adding distilled water. The restriction endonuclease was incubated at 37°C for 2 to 18 hours. After incubation, we performed gel electrophoresis to determine whether the correct DNA sequence was available in the solution.
2.4.7 SequencingTo determine whether the mutation was present we performed DNA sequencing. This is a technique used to determine the nucleotide sequence of a given piece of DNA. Four different fluorescent labels, one representing each nucleotide, are used. The DNA is multiplied into strands that differ in just 1 nucleotide in length and are organized according to size. The fluorescent labels bind to the last nucleotide. The DNA strands then flow through the laser beam, the biggest first and the smallest last. Each fluorescent label emits a specific signal when excited by a laser beam, and because this label binds to the final nucleotide the order of the nucleotides can be recorded.
We performed the nucleotide sequencing twice. The primers were selected based on the TOPO vector map (figure 3). The first time we used forward primer SP6 and reverse primer T7. The second time we used the M13 forward primer and M13 reverse primer. For sequencing the Solexa Genome Analyzer (Illumina Inc, San Diego, CA) was used.
We tested the BRAF status of 3 patients (3473, 3457 and 3700) in our lab. We received the information about the BRAF status of the other patients from a different lab that also controlled the BRAF determination of the patients tested in our lab.
2.5 Peptide binding assay In a peptide binding assay, live cells expressing sub optimally loaded HLA-class I proteins are incubated with medium and diluted synthetic peptides. The used cells are T2 cells, lymphoma cells expressing HLA-A2. These cells are TAP (Transport Associated Protein) deficient and lack the ability to translocate peptides into the endoplasmatic reticulum. The instability of the HLA-class I expression is due to a lack of endogenous peptide. Surface HLA-class I molecules become conformationally unstable shortly after peptide dissociation.The binding of an exogenous peptide can stabilize the surface class I molecule, prevent conformational instability and thus increase class I surface expression in an allele specific manner (45). The binding ability of peptides to T2 cells can be determined by flow cytometry. Peptides with a high binding affinity are thought to give a better immune response.
We performed a HLA-A2/peptide complex stability assay to determine the maximum binding affinity and dissociation rate of peptide/MHC complexes. T2 cell were cultured in RPMI 1640 medium (Gibco, Invitrogen) with 10% fetal bovine serum (FBS), and incubated with 5% CO2 at 37°C. 105 T2 cells were washed 2 times with Dulbecco’s Modified Eagle Medium (DMEM, Gibco) and distributed into 1.5ml tubes. We incubated the T2 cells in DMEM with 1µl/ml β2-microglobulin (Sigma-Aldrich, St. Louis, MO) and peptide for 3 hours and overnight in the concentrations as noted by table 4. The used peptides are described in detail in table 5.
15

Table 4: Peptides and controls for T2 binding assay.Peptide added Amount Antibody added Amount
1 Negative control - Control antibody 2 µl2 Positive control Control peptide 2,5 µl FITC mouse anti-
human HLA-A21 µl
3 Control without peptide
- FITC mouse anti-human HLA-A2
1 µl
4 Unmodified peptide 2
Unmodified peptide 2
12,5µl (100mM) FITC mouse anti-human HLA-A2
1 µl
5-11 Modified peptide 1-7
Modified peptide 1-7
12,5µl (100mM) FITC mouse anti-human HLA-A2
1 µl
After incubating the cells with β2-microglobulin we harvested the cells after 3 hours and after 18 hours. We washed the cells with FACS buffer (PBS, FBS and 0.02% Na azide). We used control antibody (BD PharmigenTM, FITC labeled mouse IgG1) and FITC mouse anti-human HLA-A2 (BD PharmigenTM, 0.5 mg/ml) to stain the cells. We incubated the cells 30-40 minutes with the antibody. After the incubation the cells were washed with FACS buffer, dissolved in FACS buffer and brought to facilities for the analysis of the FACS. We used the both the CyAn ADP (DakoCytomation) and the EPICS XL-MCL (Beckman Coulter) machines.
The ability of the peptide to combine with HLA-A2 was calculated as follows (46): A1 = (MFI1 – MFI0)/(MFI2 – MFI0)A1 = affinity index for HLA-A2MFI1 = mean fluorescence index (MFI) of cells treated with the peptideMFI2 = mean fluorescence index (MFI) of cells without the peptideMFI0 = MFI of T2 cell staining with the isotype immunoglobulin
Peptides with high binding affinity were selected for PLG encapsulation and used for autologous monocyte pulsing.
2.6 PLG-encapsulation.Biodegradable microspheres based on poly (D,L-lactide-co-glycolide)/poly (D,L-lactide) (PLGA/PLA) have the potent capacity of eliciting both humoral and cell mediated immune responses in vivo. They are composed of a spherical shaped polymeric matrix. Enclosed proteins are continuously released at a low level during biodegradation. Macrophages and dendritic cells are competent for cross presentation. They present exogenous microencapsulated antigens to both MHC class I and class II restricted T cells in vitro. The microspheres provide a continuous supply of peptide ligands for newly synthesized MHC class I molecules. Thus they are thought to give a better stimulation of the immune response (47-50).
We used PLG encapsulation to provide a better peptide stimulation of the monocytes. The PLG encapsulation was performed by a colleague at the lab.
2.7 T cell proliferation assay. After determining the BRAF mutation status we used the HLA-A2+ PBMC for further analysis. We pulsed autologous monocytes with PLG encapsulated peptides to determine which peptides gave the best stimulation of T cell proliferation. We determined the proliferation of the lymphocytes using a 3H-thymidine assay. In this assay, radioactive labeled thymidine will be incorporated into DNA of dividing cells. Thus, the more cell divisions, or the higher the proliferation rate, the more radioactivity will be incorporated into the DNA. The cells are
16

harvested using distilled water. The cells and organelles burst and set the DNA free. The solution is passed through a glass fiber membrane. Intact DNA is too big to pass the filter and is collected on the membrane. The higher the proliferation rate, the more DNA is collected on the filter. The filter membrane is dried and the amount of radioactivity is counted in a scintillation counter.
For the T-cell proliferation assay we used cells of 10 patients (WM35, WM3457, 3451, NC02, 3623, 3681, 3705, 3502, CS and 3622). We could only use these 10 cell lines because cell lines of other patients were not available. We plated 100µl of Peripheral Blood Mononuclear Cells (PBMCs) in RPMI 1640 + 2,5% FBS in 96 well U-bottom plates and incubated them overnight at 37°C. The next day we inspected the wells under the microscope and mixed and aspirated 100µl of cell solution to remove the non-adherent lymphocytes. The fluid was collected in a tube and set aside in the incubator.
In the wells were peptides would be added, we added 100µl RPMI 1640 + 2,5% Δ human AB serum. We added the peptides and proteins to pulse the monocytes. The used peptides and proteins are described in table 5. The amount and concentration of the added substances are described in table 6. After adding the peptides and proteins, we incubated the cells overnight at 37°C.
Table 5: Peptides used for PBMC pulsingPeptide # Residues 597-606 Peptide amino acid
sequenceHLA binding score
1 Modified BRAFV600E (position 2) LATE1KSRWS 132 Modified BRAFV600E (position 2) LMTE1KSRWSG 133 Modified BRAFV600E (position 2) LLTE1KSRWSG 154 Modified BRAFV600E (position 2 +
10)LLTE1KSRWSV 25
5 Modified BRAFV600E (position 10) LATE1KSRWSI 176 Modified BRAFV600E (position 10) LATE1KSRWSL 197 Modified BRAFV600E (position 10) LATE1KSRWSV 19- Unmodified BRAF V600E 1 LATE1KSRWS 8- Unmodified BRAF V600E 2 LATE1KSRWSG 9- Wild type LATVKSRWS 6- Wild type LATVKSRWSG 7- Control peptide KALEEKKGNY 91Valine (V) substituted by Glutamic acid (E). 2Bold letters indicate anchor residuesBold letters indicate HLA-A*0201 anchor residues.The HLA binding score is based on a database developed by Rammensee et al (www.syfpeithi.de).
17

Table 6: substances added to 96-well platesSubstance added Concentration Amount addedMonocytesModified V600E peptide 1-7 25µg/ml 10µlUnmodified V600E peptide/PLG 1 and 2 25µg/ml 2.5µlUnmodified wild type BRAF peptide 1 and 2 25µg/ml 2.5µlNegative control peptide 25µg/ml 2.5µlBRAF V600E protein/liposomes 10µg/ml 3µlWild type BRAF protein/liposomes 10µg/ml 2µlTh8 10µlTh9 10µlTh10 10µlMonocytes + T-cellsOnly T-cellsHIV SO55 negative control 2.5µl
The next day, the plates were irradiated at 5000 rads. We removed 75µl of supernatant per well to remove excess peptide. Then we added the non-adherent PBMC (1x105 cells/200l/well in RPMI 1640 + 5% human AB) to the pulsed monocytes and cocultured for 5 days. On days 2 and 4, 50µl of supernatant was removed per well and frozen for cytokine determinations. Furthermore, we mixed and transferred 50µl/well to a new 96 well plate to perform the 3H-thymidine proliferation assay. Radioactive thymidine (3HTdR) was added to the new plates (1Ci/l) and incubated for 12hr at 37oC. After incubation the cells were harvested using a semiautomatic cell harvester (Skatron, Corston, UK). The glass fiber was dried, and then dissolved in Insta-Fluor Plus (Perkin Elmer, Waltham, MA). The amount of radioactivity was counted using a Liquid Scintillation Analyzer (TriCarb 2800 TR, PerkinElmer).
The initial plates were restimulated with ½ original concentration of protein and then cultured in Tissue Culture Medium (TCM) + 2.5U/ml rIL-2. We continued culturing the cells and restimulated with ½ the original concentration of protein weekly and with peptide/PLG as needed.
2.8 Phenotyping of T-cellsTo determine whether the proliferating lymphocytes were of the CD8 or the CD4 subtype, we performed phenotyping of the lymphocytes using flow cytometry.
The cells were grown in 96-well plates as described in the previous section (T-cell proliferation assay). When we saw clusters of proliferating cells, we transferred the fluid to a 24-well plate. If the cells formed clusters and proliferated in the 24 well plates, we aspirated 500µl of the cell suspension. We spun the cells down, discarded the supernatant and added 50µl of FACS buffer to each tube. We incubated the cells with control antibody (BD Pharmingen, PE mouse IgG1), anti-CD4 antibody (BD Pharmingen, PE anti-human CD4) and anti-CD8 antibody (BD Pharmingen, PE anti-human CD8). The cells were incubated with antibody for 30-40 minutes, then washed with FACS buffer and resuspended in 400µl of the buffer. The samples were tested using the EPICS XL-MCL, Beckman Coulter machine, and data were analyzed using FlowJo software (Tree Star Inc.).
18

2.9 Cytotoxicity assayIn a cytotoxicity assay target cells are labeled with radioactive 51Cr which binds tightly to most intracellular proteins. After washing, the cells are incubated with immune effector cells. During incubation, labeled proteins are released into the culture supernatant due to plasma-membrane damage. The target cell lysis can be determined by measuring the radioactivity released into the supernatant (51, 52).
A CTL assay was done for patient 35 using lymphocytes stimulated with wt BRAF protein/liposomes, wt BRAF peptide 1/PLG, negative control peptide/PLG, modified BRAFV600E peptide 6/PLG and BRAF class II peptide 10/PLG. A CTL assay was done for patient 3622 using only lymphocytes stimulated with modified BRAFV600E peptide. The target cells used for the CTL assay are:
WM 35 (HLA-A2+, wt+, V600E+) WM 3457 (HLA-A2+, wt+, V600E+) WM 3623 (HLA-A2+, wt+, V600E-) WM 3248 (HLA-A2-, wt+, V600E-)
We labeled target cells with 51Cr (25µci/ml) and plated 2x103 cells/well/100µl in 96 well U-bottom plates in RPMI +10% FBS or melanoma medium, depending on what medium the cell lines normally use. The cells were incubated over night at 37°C. The target cells where washed 3 times with warm RPMI. Per well we added 100µl of melanoma medium or RPMI + 10% FBS. The effector cells were added with an effector to target ratio of 50:1, 25:1 or 12.5:1 in 100µl/well T-cell medium plus 40U/ml rIL-2. We brought the maximum and spontaneous release wells up to 200µl/well.The plates were incubated for 6hr. we collected 75µl/well supernatant and counted in the counter machine. The wells to determine spontaneous released contained just the target cells without any added peptides. The maximum release wells were lysed with H2SO4, mixed and transferred in the tube for counting. The plates were incubated overnight and after 18 hours we collected 75µl/well supernatant again and counted.
The % of specific lysis was determined by the formula:((Experimental release – spontaneous release)/(maximum release – spontaneous release)) x 100.
19

3 Results
3.1 Determination of the HLA-A2 status. We tested 14 patient samples to determine their HLA-A2 status. Four of these samples (29%) were HLA-A2 positive. In figure 4 the histogram of patient 047437207 is shown. The purple line shows the cells stained with the negative control antibody, the blue line shows the cells stained with CD45 antibody which is a positive control because CD45 is a marker for lymphocytes. The black line represents the cells stained with HLA-A2 antibody. The percentage of HLA-A2+ cells is higher than the negative control, but lower than the positive control.
Figure 4: determination of HLA-A2 status of patients 047437207 using flow cytometry.
In table 7 the flow cytometry data from all patients are summarized. Values above 5% are regarded positive. Furthermore we looked at the mean intensity of fluorescence (MnX). The mean intensity values represent the number of molecules per cell.
20

Table 7: determination of the HLA-A2 status using FACs analysis. Patient Machine used Control CD45 HLA-A2 Conclusion
% Cells
Mn X % Cells
MnX % Cells
Mn X
PD 2027 EPICS XL-MCL 0.10 3.50 NegativeJB 2008 EPICS XL-MCL 0.38 2.81 Negative2035 EPICS XL-MCL 0.03 2.23 Negative3539 EPICS XL-MCL 0.11 2.56 NegativeMS 2009 EPICS XL-MCL 0.07 2.00 Negative3542 EPICS XL-MCL 0.04 2.14 NegativeGT 03 EPICS XL-MCL 3.19 3.53 64.0 9.34 4.04 8.69 NegativeNC 02 EPICS XL-MCL 0.95 4.68 97.7 97.9 93.8 10.9 Positive3473 EPICS XL-MCL 1.05 5.02 54.9 5.28 2.26 4.03 Negative047437207 EPICS XL-MCL 1.05 3.64 99.5 148.1 98.7 14.5 Positive2038 CyAn ADP 1.09 27.79 99.35 800.96 0.76 26.62 Negative3700 CyAn ADP 1.07 38.18 99.92 41.04 96.17 204.87 PositiveTF 1011 CyAn ADP 1.05 22.47 99.93 1259.37 98.31 132.4 Positive1039 CyAn ADP 5.83 18.79 NegativeEPICS XL-MCL, Beckman Coulter machine: % of cells is the percentage of cells in B-area. CyAn ADP, DakoCytomation: % of cells: percentage of cells in R2 region For both machines: the MnX: mean intensity of fluorescence per cell
Apart from the 14 cells tested here, we had cells available from 9 other patients, that had earlier been tested HLA-A2 positive but whose cells had never been used for further analysis.
3.2 Determination of the BRAF mutation status.We used tumor samples of patients 3700, 3473 and 3457 for the determination of the BRAF status. All the DNA used was genomic DNA.
3.2.1 DNA PurificationAfter the DNA purification the DNA content of the samples as measured with Nanodrop was as noted in table 8.
Table 8: Results of Nanodrop measurements after DNA purification.Sample DNA (ng/µl) 260/280 260/2303700 227.75 ng/µl 1.87 1.213473 577.56 ng/µl 1.92 1.883457 1208.15 ng/µl 2.00 2.09
We considered a DNA content above 200ng/µl as enough. Therefore, all 3 samples contained enough DNA.
3.2.2 Polymerase Chain ReactionWe performed PCR several times to optimize the reaction. We changed the primers, the numbers of PCR cycles and the annealing temperature. The results are noted in table 8.
Table 8: results for PCR with different primer pairs.Forward primer Reverse primer ResultsHuman BRAF S4 3BRAF kinase fusion Did not work Exon5BRAF Exon3BRAF Did not workExon5 Exon3 Worked well
21

3.2.3 Gel electrophoresisAfter PCR and EcoR1 cutting we determined the length of our DNA molecules by gel electrophoresis. Figure 5 shows the photo of the gel after we performed a PCR of the original DNA from DNA purification. The primers we used were Exon 5 and Exon 3. All 3 samples show a clear band at approximately the 120bp region, which is the estimated length of the DNA fragment containing the BRAF mutation. This means that the desired DNA fragment is present in the samples.
Figure 5: Gel electrophoresis after PCR with primers Exon5 and Exon3 of original DNA from DNA purification.
All 3 samples show a band at the 120bp region, which means that the desired DNA fragment containing the BRAF mutation is present in the samples.
Gel electrophoresis was also performed after EcoR1 cutting, and light but positive bands were shown at the 120bp region. We performed Nanodrop analysis after cutting the bands out of the gel of figure 5. The DNA content of these samples was approximately 16ng/µl, which is considered enough in this case.
3.2.4 TOPO cloningTo determine the presence of the V600E mutation, the DNA fragment was cloned using the TOPO cloning kit. We performed TOPO cloning several times. The colonies grew well and we got plenty of cells following every cloning procedure.
3.2.5 MiniprepAfter TOPO Cloning we performed Miniprep for plasmid DNA isolation. We did the Miniprep a couple of times, because at first we did not manage to get the correct DNA fragment out of the cells. After the last Miniprep the DNA content of the samples, as determined by Nanodrop, was between 400 and 900 ng/µl, which is more than enough for further analysis.
3.2.6 Restriction digestionEcoR1 cutting was performed a couple of times. The first times it did not seem to work, as evaluated by gel electrophoresis. However, when we allowed the enzyme to incubate overnight, the right DNA fragment appeared to be present in the sample. The gel electrophoresis showed light but positive bands at the 120bp region.
1kb 0.5kb empty Cont 3700 3474 3457
600bp
100bp50bp
22

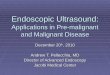
3.2.7 SequencingWe performed sequencing on the HLA-A2 positive samples twice, to determine the BRAF mutation status of these samples. The first time we tried forward primer SP6 and reverse primer T7. All samples showed a lot of background. However, 3473 seemed not mutated, and both 3700 and 3457 might be mutated. To confirm the results we performed the sequencing a second time. We used the M13 forward primer and M13 reverse primer. Figure 6 shows the results of the sequencing with the M13 forward primer and the M13 reverse primer of sample 3457. Both figure 6a and 6b show the V600E mutation. Figure 7 shows the results of the sequencing with primer T7 of sample 3473. In this sample, the mutation is not present.
Figure 6: Sequence electropherogram of sample 3457, mutation V600E.
A: Primer M13 Forward, mutation at base 142, indicated with the arrow. Wild type: ACA GTG AAA. V600E mutation: ACA GAG AAAB: Primer M13 Reverse, mutation at base 167, indicated with the arrow. Wild type: TTT CAC TGT. V600E mutation: TTT CTC TGT
Figure 7: Sequence electropherogram of sample 3473, wild type.
Primer T7, no mutation at base 125, indicated with the arrow. Wild type: TTT CAC TGT.
The sequencing was repeated in another lab to confirm our results. In this lab the mutation status of the other samples was determined as well. The BRAF mutation status of 11 patients was tested. The mutation status of 3 other patients (TF1011, 047437207 and 3705) could not be tested because we could not get access to tissues or cell lines from these patients. From the 11 tested patients 4 (36%) had the V600E mutation. The BRAF mutation status of all samples is noted in table 9.
A B
23

Table 9: BRAF mutation statusSample number HLA-A2 BRAF mutation status3700 + Wild-type3473 - Wild-type3457 + V600E + Wild-typeWM 35 + V600E + Wild-type3451 + Wild-type3623 + Wild-type3681 + Wild-type3502 + V600E + Wild-type3622 + Wild-typeBRAF-CS + V600E + Wild-typeNC 02 + Wild-type
3.3 Peptide binding assayWe performed the peptide binding assay 7 times. Table 10 shows the fluorescent index of the 4 times the T2 binding assay worked best.
Table 10: Fluorescent Index of T2 binding assay at 4 different measurements.Sample FI
1st time FI 2nd time
FI 3rd time
FI 4th time
Mean
Positive control 2.42 3.49 21.75 12.12 9.945Unmodified 2 1.04 0.62 1.75 0.86 1.0675Modified 1 0.98 0.49 1.5 1.19 1.04Modified 2 1.22 0.58 0.75 0.73 0.82Modified 3 0.99 0.46 1 1.2 0.9125Modified 4 1.33 2.66 20 2.19 6.545Modified 5 1.11 0.54 0.25 1.18 0.77Modified 6 1.36 0.5 0.5 0.09 0.6125Modified 7 1.15 0.47 1.25 1.16 1.0075
FI = fluorescent index, measured as A1 = (MFI1 – MFI0)/(MFI2 – MFI0). A1 = affinity index for HLA-A2MFI1 = mean fluorescence index (MFI) of cells treated with the peptide. MFI2 = mean fluorescence index (MFI) of cells without the peptide. MFI0 = MFI of T2 cell staining with the isotype immunoglobulin
From the table it is clear that modified peptide 4 binds MHC molecules the strongest. Other peptides that bind strong are unmodified peptide 2, modified peptide 1 and modified peptide 7. In figure 8 the shift in fluorescence index is shown using flow cytometry. Compared to the control without peptide, the sample with modified peptide 4 (M4, shown in black) is clearly shifted to the right, which means there is an increase in mean intensity.
24

Figure 8: FlowJo analysis of FACS data for A2-binding assay.
The black line, modified peptide 4, is clearly shifted to the right as compared to the control without peptide.
3.4 T-cell proliferation assayWe performed the T cell proliferation assay in 10 patients. All assays were done in triplicate and the results are given as average count per minute (cpm) values and standard error. If one of the measurements was more than a 2 fold different from the other measurements, we removed this measurement from our further calculations. Figure 9 shows the results for patient 35, whose tumor has the BRAFV600E mutation. The bars show the amount of 3HTdR incorporated in the cells and the standard error.
Figure 9: 3HT dR incorporation assay of patient 35.
none
PBL only
Mono +
PBL
Unmod
. P1/P
LG
Unmod
. P2/P
LG
mod. P
1/PLG
mod. P
2/PLG
mod. P
3/PLG
mod. P
4/PLG
mod. P
5/PLG
mod. P
6/PLG
mod. P
7/PLG
wt P1/P
LG
wt P2/P
LG
neg.
ctr. p
ep/PLG
V600E
prote
in/lip
o
wt BRAF pr
otein/
lipo
cl. II
P8/PLG
cl.II P
9/PLG
cl. II
P10/PLG
0100002000030000400005000060000700008000090000
46 1028
19387
77971
24481
3983238016
22007
69875
510218038
44950
1174921843
35953
850 26310950
48982
4037
35 PBMC (BRAFV600E+)
Stimulants
3HT
dR in
corp
orat
ion
(cpm
)
We used the T-test to determine the p values, using Excel. Table 11 shows the p-values when comparing monocytes and PBL with the different tested peptides. We only determined the P-value of the peptides showing clear proliferation.
25

Table 11: p-values of comparing tested samples with the control sample Monocytes and PBL.Tested samples P-valueUnmodified peptide 1/PLG 0.005653Unmodified peptide 2/PLG 0.201163Modified peptide 1/PLG 0.01503Modified peptide 2/PLG 0.015029114Modified peptide 3/PLG 0.327724396Modified peptide 4/PLG 0.0016002Modified peptide 7/PLG 0.008468625Wild type peptide 2/PLG 0.3253232Negative control peptide 0.018976Cl II peptide 9/PLG 0.005438
We determined the p-values of the samples compared to the negative control as well, as shown in table 12.
Table 12: P-values compared to negative control peptide.Tested samples P-valueUnmodified peptide 1/PLG 0.013614Modified peptide 1/PLG 0.25009Modified peptide 2/PLG 0.440752164Modified peptide 4/PLG 0.0046165Cl II peptide 9/PLG 0.040741
From these results it is clear that only modified peptide 4 gives a significant proliferation compared to both the monocytes and PBL and the negative control peptide. The other differences are not significant.
The other tested cell lines showed no significant proliferation at all. Cell lines NC02, 3623, 3622 (all wild type) and 3502 and BRAF-CS (both V600E mutation) showed very low proliferation in all wells. Cell line 3457 (V600E+) showed proliferation when stimulated with wild type peptide 2/PLG (p-value when compared to monocytes and PBL 0.02). However, since the proliferation was very low in all wells, the results are not clinically relevant. Cell line 3451 (Wild type) showed proliferation in the wells with wild type peptde2/PLG, V600E protein/liposomes and peptide 8/PLG, but also in the well with the negative control peptide. There was no significant difference in proliferation of cells stimulated with peptides compared to the negative control.Cell line 3681 (Wild type) showed a high proliferation in the well with only monocytes and peripheral blood lymphocytes, so no conclusions could be drawn from the other wells with high proliferation. Cell line 3705 showed high proliferation in the well stimulated with unmodified peptide 2, but with a very high standard error, so no conclusions could be drawn.
3.5 Phenotyping of T-cellsWe only performed phenotyping of the rapidly proliferating cells in the lymphocyte proliferation assay. Table 13 shows the result of the phenotyping.
26

Table 13: Results of the phenotyping of cells. Patient Tested Wells CD4 % cells MnX CD8 % cells MnXWM 35 Wt prot 93.2
98.230.419.6
37.33.62
8.8931.8
Neg 52.454.5
15.711.8
9491.6
172.3166.4
Wt1 59.64.482.94
3.0964.822.8
98.796.297.4
333.1180.5182.6
Th10 49.941.444.5
58.931.523.7
50.956.564.8
191.1140.082.5
M6 49.0 32.5 50.9 122.93451 Wt1 77.3
58.435.812.2
12.717.5
1.891.83
3623 UM V600E 2 25.7 17.5UMwt1 1.48 6.93 78.9 80.5
3681 V600E 99.9 65.7 10.3 2.483705 Th10 27.5 12.9 15.2 58.1
UM1 1.8 8.54 99.6 82.9WT BRAF 12.8 54.3 85 84.3
3502 UM V600E 98.3 20.1 0.74 35.93622 BRAF M1 74.2 40.4 18.8 270.3The percentage of cells is the percentage of the cells in the B-region of the histogram.
CD8+ cells constitute about 35% of the peripheral T-lymphocytes (53). We considered a percentage of CD8+ cells above 40% as sign of proliferation of CD8+ lymphocytes. Therefore we concluded that there is proliferation of CD8+ cells in the wells containing WM35 neg, WT1, Th10 and M6, in 3623 UMwt1 and in 3705 UM1 and WT BRAF.
3.6 Cytotoxicity assayWe performed a cytotoxicity assay of just two patients, WM35 and 3622. The cells of the other patients had not proliferated enough to perform the cytotoxicity assay. The target cells used for the CTL assay are:
WM 35 (HLA-A2+, wt+, V600E+) WM 3457 (HLA-A2+, wt+, V600E+) WM 3623 (HLA-A2+, wt+, V600E-) WM 3248 (HLA-A2-, wt+, V600E-)
The % of specific lysis, or the % cytotoxicity, was determined by the formula: ((Experimental release – spontaneous release)/(maximum release – spontaneous release)) x 100.
Figure 10 shows the results of the cytotoxicity assay of 35 PBMC stimulated with negative control peptide/PLG after 18 hours.
27

Figure 10: Results of cytotoxicity assay of 35 PMBC stimulated with negative control peptide/PLG after 18 hours.
12.5 25 50
-40
-20
0
20
40
60
80
35 PBMC (HLA-A2+, wt+, V600E+) stimulated with negative control peptide/PLG (18hr 51Cr release assay)
WM 35 (HLA-A2+, wt+, V600E+)
WM 3457 (HLA-A2+, wt+, V600E+)
WM 3623 (HLA-A2+, wt+, V600E-)
WM 3248 (HLA-A2-, wt+, V600E-)E:T ratio
% c
ytot
oxic
ity
Figure 11 shows the results of the cytotoxicity assay of 35 PMBC stimulated with BRAFV600E peptide 6/PLG. WM 3457 was killed very well.
Figure 11: Results of cytotoxicity assay of 35 PBMC stimulated with BRAFV600E peptide 6/PLG after 18 hours.
12.5 25 50-200
20406080
100120140
35 PBMC (HLA-A2+, wt+, V600E+) stimulated with modified BRAFV600E peptide 6/PLG (18hr 51Cr release assay)
WM 35 (HLA-A2+, wt+, V600E+)
WM 3457 (HLA-A2+, wt+, V600E+)
WM 3623 (HLA-A2+, wt+, V600E-)
WM 3248 (HLA-A2-, wt+, V600E-)E:T ratio
% c
ytot
oxic
ity
Figure 12 shows the results of the cytotoxicity assay of 35 PBMC stimulated with Wild Type BRAF peptide 1/PLG after 18 hours. Again, WM 3457 is killed best, and WM 3623 is killed very well too.
28

Figure 12: results of the cytotoxicity assay of 35 PBMC stimulated with Wild Type BRAF peptide 1/PLG after 18 hours
12.5 25 500
20
40
60
80
100
35 PBMC (HLA-A2+, wt+, V600E+) stimulated with wild type BRAF peptide 1/PLG (18hr 51Cr release assay)
WM 35 (HLA-A2+, wt+, V600E+)
WM 3457 (HLA-A2+, wt+, V600E+)
WM 3623 (HLA-A2+, wt+, V600E-)
WM 3248 (HLA-A2-, wt+, V600E-)
E:T ratio
% c
ytot
oxic
ity
Figure 13 shows the results of the cytotoxicity assay of 3622 PBMC stimulated with modified BRAFV600E peptide 1/PLG after 18 hours. Target WM 3457 is killed very well by the effector cells, with a cytotoxicity of 121% when the effector: target ratio is 50. The target cells of 3623 are killed very well too.
Figure 13: Results of cyotoxicity assay of 3622 PBMC (HLA-A2+, WT+, V600E-) stimulated with modified BRAFV600E peptide 1/PLG after 18 hours.
12.5 25 50-200
20406080
100120140
3622 PBMC (HLA-A2+, WT+, V600E-) stimulated with modified BRAFV600E peptide 1/PLG (18hr 51Cr release assay)
WM 35 (HLA-A2+, wt+, V600E+)
WM 3457 (HLA-A2+, wt+, V600E+)
WM 3623 (HLA-A2+, wt+, V600E-)
WM 3248 (HLA-A2-, wt+, V600E-)E:T ratio
% c
ytot
oxic
ity
29

4 DiscussionThe goal of this study was to determine whether modified BRAF peptides induce a better immune response than unmodified peptides. The hypothesis was that an increased binding affinity to HLA molecules will result in better antigen presentation and hence in a better immune response.
4.1 Determination of the HLA-A2 status.The immune response to BRAFV600E peptides is HLA-A2 specific. Therefore we selected HLA-A2 positive patients for this study. In our experiment only 29% of the patients were HLA-A2 positive. This percentage is lower than we expected. According to the literature HLA-A2 is expressed in ~50% of melanoma patients and 28% of healthy individuals (35, 54). So the percentage we found is closer to the expected percentage in healthy individuals than in patients with melanoma.
There are two possible explanations for this finding. The first explanation is that in Philadelphia, the percentage of melanoma patients being HLA-A2 positive is lower than in other regions of the USA, where previous studies about HLA-A2 positivity took place. In the area of Philadelphia, the percentage is always around 25%. This has been confirmed, but not published, by others on the campus of the University of Pennsylvania.
Another explanation is the feature mentioned in other studies, that many human tumors appear to express greatly reduced levels of MHC-I (HLA-I) antigens. In melanoma, there are selective changes in the expression of HLA-A2 that range from reduction to loss of HLA expression. Since HLA-A2 is important for lysis by CTL, the down regulation of this molecule might be an important mechanism by which melanoma cells can escape the immune recognition. However, the mechanisms responsible for the loss of HLA alleles are poorly understood (9, 16).
4.2 Detection of the BRAF mutation status. To determine the BRAF mutation status we used multiple molecular techniques.
We used the Nanodrop to determine the amount of DNA of samples. We used the ratio of 260/280, the ratio of DNA/protein, as a measure for the purity of the DNA. A ratio of ~ 1.8 is generally accepted as pure for DNA, and because all samples had a ratio close to 1.8 we considered them pure for DNA. The ratio of 260/230 is the ratio of DNA/lipids and other contamination, which is a secondary measure for the nucleic acid purity. The values are generally between 2.0-2.2. Only sample 3457 had a 260/230 ratio in this range. Both other samples have a lower ratio, which suggests contamination with proteins and lipids. This could have an influence on the PCR reaction. However, because our PCR worked well we think the contamination was not relevant for the rest of the experiments.
The polymerase chain reaction had to be performed several times before we got a good result. The first primer pair we used was Human BRAF S4 and 3BRAF kinase fusion. Retrospective, this was not a good primer pair for this particular DNA. The target sequences were quite far from the mutated BRAF, and there are many introns in the genomic DNA between the target sequence and the desired BRAF coding region. This means that the PCR fragment would get really big, which could cause many errors in the reaction.
30

The second PCR was done with Exon5BRAF and Exon3BRAF. This PCR did not work either. This could have been due to several reasons. We either added too little DNA, we used too few cycles or we had a wrong annealing temperature. Since another sample from a colleague did not work with this programme as well, the most likely cause was the wrong annealing temperature. Another possibility is that the sample got DNAse in it during the process. This enzyme catalyzes a cleaving reaction of DNA, which destroys the DNA. The enzyme can enter the reaction in different ways, one of them is via the hands of the researcher.
During the restriction digestion we let the samples incubate for 2 hours, but this was not enough for the enzyme to cut the DNA. When we let the enzyme incubate overnight, this gave a better result.
This part of the experiments took a lot of time and work. Since the final sequencing results were similar to the results obtained in another lab, we considered the determination of the BRAF status as successful.
4.3 Peptide binding assayWe used the peptide binding assay to determine the binding affinity of peptides to T cells. With the peptide binding assay we found that modified peptide 4 binds MHC molecules the strongest. Other peptides that bind strong are unmodified peptide 2, modified peptide 1 and modified peptide 7.The assay worked better if we incubated the antibody in the presence of the peptides. This is probably due to a rapid dissociation rate of the peptides.
4.4 T cell proliferation assayWith the T cell proliferation assay we determined the proliferation of lymphocytes after stimulation with different peptides, using a 3H-thymidine assay. However, all cells showed very low proliferation rates and the negative control showed a significant amount of proliferation compared to the control with only monocytes and PBL.Unmodified peptide 1 and 2 have been used in previous research (35). In this research, patient 35, 3457 and CS were tested, and all showed significant proliferative responses to stimulation with unmodified BRAFV600E peptides. In our current research, we could only confirm the above results in patient 35. The cells from the other patients showed low proliferation. This makes it impossible to compare the results of stimulation with unmodified peptides with modified peptides. The experiments should be performed again to reconfirm the proliferation when stimulated with the unmodified peptides and to determine the proliferation with modified peptides.
4.5 Phenotyping of T-cellsTo determine whether the proliferating lymphocytes were of the CD8 or the CD4 subtype, we performed phenotyping. We used single cell suspensions and performed one staining per tube because this is the easiest method. However, when adding the percentage of CD4+ cells to the percentage of CD8+ cells, the result is sometimes more than 100%. This can have multiple possible reasons. The first reason is that the cells might not be mature enough. Young lymphocytes are often double positive for CD4 and CD8. However, this is not very likely, since blood lymphocytes are usually either CD4 or CD8 positive and not double positive anymore.Another possibility is that too much antibody was added. When a surplus of antibody is used, it loses part of its specificity and could bind to other membrane proteins as well. However,
31

since we always used 2µl of antibody, which is the recommended amount, this possibility is an unlikely reason for the findings.The most likely reason is that we used two different samples for staining, one for CD8 and one for CD4. The CD8 antibody is slightly sensitive for CD4 as well, and the CD4 antibody can bind CD8, although they do not bind the other receptor as well as their own receptor.
To get better results, the samples should be double stained, using both PE and FITC to determine CD4 and CD8 in the same sample. Furthermore, this double staining should be done just before the cells are used for the cytotoxicity assay, so that you really know the phenotype of the cells you use for the assay.
4.6 Cytotoxicity assayWe performed a cytotoxicity assay to determine whether the T-cells stimulated with the different peptides were cytotoxic to the melanoma cells. Unfortunately, this assay did not give any significant results. The cells from patient 35 were tested most extensive. When this cell line was stimulated with negative control peptide/PLG (figure 11) we expected very little killing of the target cells, because the effector cells were stimulated with the negative control. However, the percentage of cytotoxicity of the target cells WM 3623 was almost 69% with an effector: target ratio of 50.When we stimulated 35 PBMC with BRAFV600E peptide 6/PLG (figure 12), we expected the cells to be especially cytotoxic against WM 35 and WM 3457 target cells, since the cells of patient 35 are HLA-A2+ and V600E+, and those target cells are HLA-A2+ and V600E+ too. From the figure it shows that WM 3457 was killed very well. However, WM 35 is not killed as well as we expected. WM 3623 was killed better than WM 35 at most effector: target ratios, although WM 3623 is V600E-. When 35 PBMC was stimulated with Wild Type BRAF peptide 1/PLG (figure 13) we expected WM 35 to be killed very well. However in this case the WM 35 is killed worse than WM 3457 and WM 3623.When 3622 PBMC was stimulated with modified BRAFV600E peptide (figure 14), we did not expect the cells to show much lysis since the cells of patient 3622 are HLA-A2+, wild type+ and V600E-. Therefore, they are not expected to show much lysis when stimulated with a BRAFV600E peptide. However, target WM 3457 is killed very well.
As shown above, the results are not consistent with what we expected. Because we only tested two cell lines and they give inconsistent results, we cannot draw any conclusions from this experiment. Since the proliferation did not go very well either, this could be due to a bad condition of the lymphocytes. Further experiments should be performed to determine whether the cells are really not giving significant results or if there was an error in our measurements.
4.7 General conclusionBecause the final experiments did not give any significant results, it is impossible to draw any conclusions from this research. We planned the experiments well, but had some setbacks which caused the delay so that we could not finish the experiments as planned. The first delay was that we had to wait for all the cell lines to be present before we could start with the experiments. When the cell lines were present we started with the lymphocyte proliferation assay. We expected the cells to grow quickly, however they expanded very slow. We performed phenotyping whenever the cells were expanded sufficiently. However, we had to wait for multiple cell lines to be expanded enough before we could determine the results of the proliferation assay.
32

After this determination we had to wait several weeks again, before the cells had grown sufficiently to perform the cytotoxicity assay. When we got the results of the cytotoxicity assay it was clear that we could not draw conclusions from this. However, we did not have enough time left to start over from the lymphocyte proliferation again, since that would cost us at least another 5 weeks. When I left Philadelphia, the cells were still expanding slowly.
The goal of this study was to determine whether modified BRAFV600E peptides may induce a stronger immune response than unmodified BRAFV600E peptides against melanoma cells in vitro. The hypothesis for this study was that an increased binding affinity to HLA molecules will result in better antigen presentation, and hence better immune responses will be induced. Thus, we hypothesized that modified BRAFV600E peptides will induce a stronger immune response than unmodified BRAFV600E peptides in melanoma patients.
Unfortunately, we can not determine whether our hypothesis was correct. The fact that modified peptide 4 showed a very strong binding in the peptide binding assay suggests that this modified peptide might induce a stronger immune response than the unmodified peptides. However, we were not able to confirm this in the proliferation assay and the cytotoxicity assay. Both experiments should be repeated.
Although this research did not give any significant results, I still believe I learned a lot by performing the experiments and participating in research. Before I started I had never been in a laboratory, so I had to become familiar with all the different techniques. Because we used many different techniques, I now have experience with research protocols I had never heard of before entering the lab. Next to getting familiar with all the different lab techniques, I also did an extensive literature search. And I participated in the research meetings and journal clubs organized by the lab, and presented some journal clubs myself too.
33

5. List of abbreviations
APC Antigen Presenting CellBLAST Basic Local Alignment Search ToolCPM Count per minuteCTL Cytotoxic T-lymphocyteDMEM Dulbecco’s Modified Eagle MediumDNA Deoxyribonucleic AcidEBV-B Epstein-Barr Virus-BEDTA Ethylenediaminetetraacetic acidFACS Fluorescence-Activated Cell SortingFBS Fetal Bovine SerumHLA Human Leukocyte AntigenLB Lysogeny BrothMAA Melanoma Associated AntigenMHC Major Histocompatibility ComplexNCBI National Center for Biotechnology InformationPCR Polymerase Chain ReactionPBMC Peripheral Blood Mononuclear CellsPBML Peripheral Blood Mononuclear LymphocytesPBS Phosphate Buffered SalinePLG PolyCLactide-co-GlycolideRNA Ribonucleic AcidSOC Super Optimal broth with catabolite repression through added glucoseTAA Tumor associated antigenTAP Transport Associated ProteinTBE Tris-borate EDTA bufferTCM Tissue Culture Medium
34

6. Citations
1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer Statistics 2008. CA: A Cancer Journal for Clinicians2008;58(2):71-96.
2. Tsao H, Atkins MB, Sober AJ. Management of cutaneous melanoma. N Engl J Med2004 Sep 2;351(10):998-1012.
3. Atallah E, Flaherty L. Treatment of metastatic malignant melanoma. Current Treatment Options in Oncology2005;3(6):185-93.
4. Zitvogel L, Tesniere A, Kroemer G. Cancer despite immunosurveillance: immunoselection and immunosubversion. Nature reviews, Immunology2006;6(10):715-27.
5. Parmiani G, Castelli C, Rivoltini L, Casati C, Tully G, Novellino L, et al. Immunotherapy of melanoma. Seminars in cancer biology2003;13(6):391-400.
6. Boon T, Coulie P, Eynde BVd, Bruggen Pvd. Human T cell responses against melanoma. Annual review of immunology2006;24:175-208.
7. Kirkwood J, Tarhini A, Panelli M, Moschos S, Zarour H, Butterfield L, et al. Next generation of immunotherapy for melanoma. Journal of clinical oncology2008;26(20):2445-55.
8. Fischer W, Straten Pt, Terheyden P, Becker J. Function and dysfunction of CD4(+) cells in the immune response to melanoma. Cancer immunology, immunotherapy1999;48(7):363-70.
9. Rivoltini L, Carrabba M, Huber V, Castelli C, Novellino L, Dalerba P, et al. Immunity to cancer: attack and escape in T lymphocyte-tumor cell interaction. Immunological reviews2002;188:97-113.
10. Halliday G, Patel A, Hunt M, Tefany F, Barnetson R. Spontaneous regression of human melanoma/nonmelanoma skin cancer: association with infiltrating CD4+ cells. World journal of surgery1995;19(3):352-8.
11. Mocellin S, Rossi C, Lise M, Marincola F. Adjuvant immunotherapy for solid tumors: from promise to clinical application. Cancer immunology, immunotherapy2002;5(11-12):583-95.
12. Gray-Schopfer V, Wellbrock C, Marais R. Melanoma biology and new targeted therapy. Nature Reviews Immunology2007;445(7130):851-7.
13. Terando A, Faries M, Morton D. Vaccine therapy for melanoma: current status and future directions. Vaccine2007;25, Sup 2:B4-16.
14. Sampson J, Archer G, Mitchell D, Heimberger A, Bigner D. Tumor-specific immunotherapy targeting the EGFRVIII mutation in patients with malignant glioma. Seminars in immunology2008;20(5):267-75.
15. Baselga J, Tripathy D, Mendelsohn J, Baughman S, Benz C, Dantis L, et al. Phase II study of weekly intravenous trastuzumab (Herceptin) in patients with HER2/neu-overexpressing metastatic breast cancer. Seminars in oncology1999;26(4):78-83.
16. Pandolfi F, Boyle L, Trentin L, Kurnick J, Isselbacher K, Gattoni-Celli S. Expression of HLA-A2 antigen in human melanoma cell lines and its role in T-cell recognition. Cancer research1991;51(12):3164-70.
17. Castelli C, Rivoltini L, Mazzocchi A, Parmiani G. T-cell recognition of melanoma antigens and its therapeutic applications. International journal of clinical & laboratory research1997;27(2):103-10.
18. Jäger E, Jäger D, Knuth A. Clinical cancer vaccine trials. Current opinion in immunology2002;14(2):178-82.
19. Lazoura E, Apostolopoulos V. Insights into peptide-based vaccine design for cancer immunotherapy. Current medicinal chemistry2005;12(13):1481-94.
20. Yamshchikov G, Barnd D, Eastham S, Galavotti H, Patterson J, Deacon D, et al. Evaluation of peptide vaccine immunogenecity in draining lymph nodes and peripheral blood of melanoma patients. International journal of cancer2001;92(5):703-11.
21. Borbulevych O, Baxter T, Yu Z, Restifo N, Baker B. Increased immunogenicity of an anchor-modified tumor-associated antigen is due to the enhanced stability of the peptide/MHC complex: implications for vaccine design. The journal of immunology2005;174(8):4812-20.
35

22. Eisen T, Ahmad T, Flaherty K, Gore M, Kaye S, Marais R, et al. Sorafenib in advanced melanoma: a Phase II randomised discontinuation trial analysis. The British journal of cancer2006;95(5):581-6.
23. Smalley K, Flaherty K. Integrating BRAF/MEK inhibitors into combination therapy for melanoma. The British journal of cancer2009;100(3):431-5.
24. Rivoltini L, Squarcina P, Loftus D, Castelli C, Tarsini P, Mazzocchi A, et al. A superagonist variant of peptide MART1/Melan A27-35 elicits anti-melanoma CD8+ T cells with enhanced functional characteristics: implication for more effective immunotherapy. Cancer research1999;59(2):301-6.
25. Gajewski T, Meng Y, Harlin H. Immune suppression in the tumor microenvironment. Journal of Immunotherapy2006;29(3):233-40.
26. Srivastava P. Therapeutic cancer vaccines. Current opinion in immunology2006;18(2):201-5.27. Castelli C, Rivoltini L, Andreola G, Carrabba M, Renkvist N, Parmiani G. T-cell recognition of
melanoma-associated antigens. Journal of cellular physiology2000;182(3):323-31.28. Zhang T, Herlyn D. Combination of active specific immunotherapy or adoptive antibody or
lymphocyte immunotherapy with chemotherapy in the treatment of cancer. Cancer immunology, immunotherapy2009;58(4):475-92.
29. Wooster R, Futreal A, Stratton M. Sequencing analysis of BRAF mutations in human cancers. Methods in Enzymology2006;407:218-24.
30. Davies H, Bignell G, Cox C, Stephens P, Edkins S, Clegg S, et al. Mutations of the BRAF gene in human cancer. Nature2002;417(6892):949-54.
31. Chong H, Vikis HG, Guan KL. Mechanisms of regulating the Raf kinase family. Cell signalling2003;15(5):463-9.
32. Wellbrock C, Ogilvie L, Hedley D, Karasarides M, Martin J, Niculescu-Duvaz D, et al. V599E B-RAF is an oncogene in melanocytes. Cancer research2004;64(7):2338-42.
33. McDermott D, Sosman J, Gonzalez R, Hodi F, Linette G, Richards J, et al. Double-blind randomized phase II study of the combination of sorafenib and dacarbazine in patients with advanced melanoma: a report from the 11715 Study Group. Journal of clinical oncology2008;26(13):2178-85.
34. Sharkey M, Lizée G, Gonzales M, Patel S, Topalian S. CD4(+) T-cell recognition of mutated B-RAF in melanoma patients harboring the V599E mutation. Cancer research2004;64(5):1595-9.
35. Somasundaram R, Swoboda R, Caputo L, Otvos L, Weber B, Volpe P, et al. Human leukocyte antigen-A2-restricted CTL responses to mutated BRAF peptides in melanoma patients. Cancer research2006;66(6):3287-93.
36. Tuveson D, Weber B, Herlyn M. BRAF as a potential therapeutic target in melanoma and other malignancies. Cancer cell2003;4(2):95-8.
37. Andersen M, Fensterle J, Ugurel S, Reker S, Houben R, Guldberg P, et al. Immunogenicity of constitutively active V599EBRaf. Cancer research2004;64(15):5456-60.
38. Promega Technical Manual Wizard Genomic DNA Purification Kit. Madison: Promega; 2009.39. Murray RK, Granner D, Rodwell V. Harper's Illustrated Biochemistry: Mc. Graw-Hill
Companies Inc; 2006.40. Bowen RA. Biomedical Hypertexts. 2000.41. QIAquick Spin Handbook2008.42. Invitrogen Introduction TOPO cloning. 2003; Available from: www.invitrogen.com.43. Campbell N. Biology. 4th ed: The Benjamin/Cummigs Publishing Company, Inc.; 1996.44. 5Prime. Manual FastPlasmidTM Mini Kit. 2007.45. Hansen T, Myers N. Peptide induction of surface expression of class I MHC. Current protocols
in immunology2003;Chapter 18.46. Wang Y, Sin WF, Xu G, Yang H, Wong T, Pang X, et al. T-Cell Epitopes in Severe Acute
Respiratory Syndrome (SARS) Coronavirus Spike Protein Elicit a Specific T-Cell Immune Response in Patients Who Recover from SARS Journal of Virology2004;78(11):5612-18.
47. Waeckerle-Men Y, Groettrup M. PLGA microspheres for improved antigen delivery to dendritic cells as cellular vaccines. Advanced Drug Delivery Reviews2005;57(3):475-82.
36

48. Johansen P, Men Y, Merkle H, Gander B. Revisiting PLA/PLGA microspheres: an analysis of their potential in parenteral vaccination. European journal of pharmaceutics and biopharmaceutics2000;50(1):129-46.
49. Men Y, Audran R, Thomasin C, Ebert G, Demotz S, Merkle H, et al. MHC class I- and class II-restricted processing and presentation of microencapsulated antigens. Vaccine1999;17(9-10):1047-56.
50. Lima K, Rodrigues J. Poly-DL-lactide-co-glycolide microspheres as a controlled release antigen delivery system. Brazilian journal of medical and biological research1999;32(2):171-80.
51. Flow Cytometry Protocols. 2nd ed.52. Cytotoxicity assay methods.53. Levinson W. Review of medical microbiology and immunology. 2006.54. Marincola F, Shamamian P, Rivoltini L, Salgaller M, Cormier J, Restifo N, et al. HLA
associations in the antitumor response against malignant melanoma. Journal of immunotherapy with emphasis on tumor immunology1995;18(4):242-52.
37

7. Word of thanks
I would like to express a word of thanks. When I started my research, I did not know anything about working in a laboratory. The people in the Herlyn laboratory have been very helpful and friendly. My supervisor, Shyam Somasundaram, has explained all the laboratory techniques with a lot of patience. Rolf Sowoboda, the other senior scientist in the laboratory, was strict, but taught me a lot about molecular biology. Dorothee Herlyn, the principal investigator, encouraged me to prepare journal clubs. So great thanks to all these people who made my stay at the Wistar Institute a wonderful time. Furthermore, I would like to thank my Dutch supervisor, Dr. Wim Smit, for being available for all questions and critically reading my report.
38

8. Summary of research in Dutch
IntroductieMelanomen zijn veel voorkomende huidtumoren. Bij uitgebreide ziekte hebben melanomen een zeer slechte prognose. Conventionele therapieën helpen vaak onvoldoende omdat veel tumorcellen relatief resistent voor chemotherapie zijn. Een lymfocyten infiltraat in of rond het melanoom is geassocieerd met een betere overleving. Dit suggereert een cellulaire immuunrespons tegen melanomen. Het is aangetoond dat actieve immunotherapie de immuunrespons stimuleert en er zijn onderzoeken gedaan naar deze vorm van therapie bij melanomen. Tumor antigeen peptiden kunnen de immuunrespons stimuleren. Het modificeren van deze peptiden kan ervoor zorgen dat zij sterker aan HLA moleculen binden, waardoor de immuunrespons versterkt wordt. Eerdere onderzoeken toonden aan dat peptiden die de BRAFV600E mutatie omvatten immunogeen zijn. Dit is een mutatie in de MAP-kinase route en deze is aanwezig in 70% van de melanoomcellen. In deze studie bepalen we of gemodificeerde BRAFV600E peptiden die sterker aan HLA moleculen binden een sterkere immuunrespons opwekken dan ongemodificeerde BRAFV600E peptiden bij melanomen.
Materiaal en methodenDrieëntwintig patiënten met een melanoom werden in deze studie geïncludeerd. De HLA-A2 status werd bepaald met flow cytometry. Uit de tumorcellen werd DNA geïsoleerd en gebruikt om de BRAFV600E mutatie status te bepalen met behulp van een polymerase chain reaction, gevolgd door sequencing van het DNA met primers SP6 en T7 en M13 forward en reverse. Er werd een eiwit binding assay gedaan om de binding van gemodificeerde peptiden aan T2 cellen te bepalen, zodat de peptiden met een hoge bindingsaffiniteit geselecteerd konden worden. Hierna gebruikten wij een lymfocyten proliferatie assay met 3HT-thymidine om de mate van proliferatie van T-cellen gekweekt met verschillende peptiden te bepalen. Van de prolifererende lymfocyten werd bepaald of zij CD4 of CD8 cellen waren. De prolifererende cellen werden verder gekweekt met IL-2 en vervolgens gebruikt in een toxiciteits assay, om te bepalen of ze tumorcellen konden doden.
ResultatenVan 14 van de 23 patiënten werden de lymfocyten getest op hun HLA-A2 status. Vier (29%) hiervan waren HLA-A2 positief en konden gebruikt worden voor verdere experimenten. Negen andere patiënten waren al eerder positief getest en werden daarom in deze studie geïncludeerd. Vier van de 11 patiënten die getest werden op BRAF status hadden de V600E mutatie. De peptide binding assay liet een sterke binding van gemodificeerd peptide 4 zien. Dit peptide is gemodificeerd in beide ankerresiduen. De lymfocyten proliferatie assay toonde een lage proliferatie bij alle geteste cellen, behalve WM35. Het fenotype van de geteste cellen was voornamelijk van het CD8 type. De cytotoxiciteits assay gaf inconsistente resultaten, met geen duidelijk verschil in toxiciteit tussen de gemodificeerde en ongemodificeerde peptiden.
ConclusieGemodificeerd peptide 4 bond in de peptide binding assay sterker dan de ongemodificeerde peptiden en zou daarom een goede kandidaat zijn voor verdere studies naar actieve immunotherapie bij patiënten met een melanoom.
39