Embed Size (px)
Citation preview

OPHTHALMIC YEAR BOOK V I S U A L T R A C T S A N D C E N T E R S
C H A R L E S P . S M A L L , M. D .
CHICAGO, I L L I N O I S
This section reviews the literature of the subject from May, 1918, to June, 1919. For previous literature see American Journal of Ophthalmology, vol. 1, July, p. 133, and August, p. 145.
BIBLIOGRAPHY.
Abelsdorff, G. Bilateral Central Scotoma with Normal Visual Fields after Occipital Wound. Klin. M. f. Augenh., v. 56, pp. 172-176. Abst., Ann. d'OeuI., v. 156, p. 117.
Adson, A. W. Hypophyseal Tumors thru the Intradural Approach. Jour. Amer. Med. Assn., v. 71, p. 721.
Allen, F. J. An Optical Phenomenon. Na-ture, Lond., 1917, p. 324.
Aseher, K. W. Secondary Impulse in Depth Perception, and the Habit of Monocular Vision. Graefe's Arch. f. Ophth., v. 94, p. 275.
Barrie, T. S. Factors in Stereoscopic Vi-sion. Brit. Jour. Ophth., v. 3, pp. 186-187.
Behr, C. Homonymous Hemianopic De-fects. (9 ill.) Klin. M. f. Augenh., v. 56, pp. 161-168. Abst., Brit. Jour. Ophth., v. 3, p. 178. Ann. d'Ocul., v. 156, p. 116.
Beritens, G. Is Vision Possible Without Eyes? Med. Ibera, v. 6, p. 55.
Berry, G. A. Disturbances of Visual Ori-entation. Brit. Jour. Ophth., v. 2, pp. 597-607.
Best, F. Hemianopsia and Mind Blindness ■with Injury to Brain. (39 ill.) Graefe's Arch. f. Ophth., v. 93, p. 49.
Bramwell, B. "Crossed" Aphasia (Mirror Writing). Edinburgh Med. Jour., v. 20, p. 220.
Brodman, K. Position of Optic Centers. Miinchen med. Wochenschr., 1918, v. 45, p. 887.
Buckley, W. Ocular Complications in Gun-shot Wound of Head. Lancet, April 13, 1919, p. 537.
Bussy. Transitory Amaurosis Caused by Concussion. Ann. d'Ocul., v. 155, p. 423.
Camp, C. D. Hysterical Blindness. Tr. d i n . Soc. Univ. Michigan, Ann Arbor, 1916-17, v. 8, pp. 135-137.
Caralt. Tumor of Hypophysis. Arch, de Oft. Hisp.-Amer., v. 18, p. 450.
Cave, C. J. P. An Optical Phenomenon. Na-ture, Load., 1917, p. 284.
Clegg, j . G. Homonymous Lateral Hemi-anopsia, Trans. Ophth. Soc. United Kingdom, v. 38, p. 182.
Colored Hearing. Abst in Med. Record, v. K p. 71.
Conlon, F. A. Bitemporal Hemianopsia Due to Sinus Disease. Amer. Jour. Ophth., v. 2, pp. 92.95.
Culbertson, L. R. Cause of Defective Ori-entation or Equilibrium. Annals Otol. Rhin. and Laryngol., v. 27, p. 187.
Daw8on, S. The Theory of Binocular Col-or Mixture. Brit. Jour. Psychol., v. 9, pp. 1-22.
Dercum, F. X. Hemianopsia. Phila. Neu-roL Soc., March 27, 1918. Abst., Med. Record, v. 94, p. 88.
Eaton, E. M. Stereoscopic Vision and Esti-mation of Distance. (4 ill.) Brit. Jour. Ophth., v. 3, pp. 63-78.
Engler. Congenital Word-Blindness. Mediz. Klinik., Nov., 1917, p. 1220. Abst, Klin. M. f. Augenh., v. 60, p. 283.
Fernandez Sanz. Hemianopsia. Espafia Oft, v. 4, p. 113. Abst. Jour. Amer. Med. Assn., v. 72, p. 904.
Freund, C. S. Aneurism of Carotid and Homonymous Hemianopsia. (2 ill., 1 col. pi.) Klin. M. i. Augenh., v. 56, pp, 468-472.
Fridenberg, P. Visual Factors in Equili-bration and Vertigo. Internat. Jour. Sur-gery, v. 31, p. 115.
Fruchte. Central Scotoma after Disease of Accessory Sinuses and After Blow on Skull. (2 ill., Bibl.) Klin. M. f. Augenh., v. 58, pp. 261-272.
Gartin, S. Sense of Orientation in the At-mosphere. Zeitschr. f. Augenh., v. 39, part 5-6, p. 368.
Gordon, A. Diminutive Visual Hallucina-tions. Jour. Nerv. and Mental Dis., v. 47, p. 434.
Goudge, M. E. A Qualitative and Quantita-tive Study of Weber's Illusion. Amer. Jour. Psychol., Worcester, 1918, v. 29, pp. 81-119.
Guijarro. Hysterical Amaurosis. Med. Ibera, v. 6, p. 26. Abst. J. A. M. A., v. 72, p. 904.
Hegner, C. A., and Zange, J. Translabyrin-thine Operation on Tumor of the Ponto-cerebellar Angle. Klin. M. f. Augenh., v. 56, pp. 176-192.
rier-chen, S. E. Center for Vision. Abst., Klin. M. f. Augenh., v. 60, p. 653.
Hensen, H Hemicrania Ophthalmica. (2 ill., Bibl.) Klin. M. f. Augenh., v. 61, 1918, pp. 129-137.
Holmes, G. Disturbances of Visual Orienta-tion. (21 ill., Bibl.) Brit. Jour, of Ophth., v. 2, pp. 353, 449, 506. Disturbances of Ocular Movements and
Nystagmus in Cerebellar Injuries. Brain, v. 40, p. 500. -
Holmes, G., and Horrax, C. Orientation with Loss of Stereoscopic Vision. Arch. of Neurol. and Psychiat, v. 1, p. 385.

186 VISUAL TRACTS AND CENTERS
Hurst, A. F., and Symms, J. L. M. Narrow and Spiral Fields of Vision in Hysteria, Malingering, and Neurasthenia. (5 ill.) Brit. Jour. Ophth., v. 3, pp. 17-21.
Igersheimer. Hemianopsia. (87 ill., Bibl.) Graefe's Arch. f. Ophth., v. 97, pp. 105-167.
Jackson, E. Neurobiotaxis. Amer. Jour. Ophth., v. 1, p. 527.
Kappers, C. U. Phenomena of Neurobio-taxis in the Visual Apparatus. Amer. Jour. Ophth., v. 1, p. 518.
Keen, W. W. and Ellis. Ocular Complica-tions in Brain Tumor. Jour. Amer. Med. Assn., v. 70, pp. 1905 and 1908.
Landwehr. Visual Fields in Anisometropia. (2 ill.) Klin. M. f. Augenh., v. 61, pp. 231-252.
Lemiere, L. Transitory Amblyopia with Shock. Ann. d'Ocul., v. 155, p. 108.
Lewis, F. P. Hypophysis Cerebri and Its Morphologic Influence. Trans. Amer. Academy of Ophth. and Oto.-Laryn., 1917-18, pp. 45-53.
Libby, G. F. Cystic Brain Tumor with Pa-pilledema. Amer. Jour. Ophth., v. 1, p. 424.
Lloyd, J. H. Sensory Aphasia with Right Homonymous Hemianopsia. Med. and Surgery, March, 1918.
Lloyd, R. I. Blocking of Maeular Arterloles. Cause of Scotoma of Maeular Bundle Type. Amer. Jour. Ophth., v. 1, p. 406.
Loeb, C. Deep X-ray Treatment in Tumors of Hypophysis. Amer. Jour. Ophth., v. 1, p. 397.
Mai ret, A., and Durante, G. Modification of Visual Field from Shell Concussion. Presse M<5d., v. 26, p. 611; Abst. New York Med. Jour., March 8, 1919, p. 432.
Marque, A. M. Cerebral and Cerebellar Tu-mors. (3 111.) Rep. Ophth., Hosp., Buenos Aires, v. 1, p. 123.
Marx, E. Limits of Visual Field. Nederl. Tijdschr. v. Geneesk., v. 2, p. 858.
Mayou, M. S. Sympathetic Paralysis Asso-ciated with Cervical Rib. Trans. Ophth. Soo. United Kingdom, v. 38, p. 178.
Meyerhof, M. Hemianopsia after Shot Wounds. (4 ill.) Klin. M. f. Augenh., y. 56, pp. 62-65.
Mirallie, C , and Denes. Mirror Writing. BulL de l'Acad. de M6d., v. 80, p. 638. Abst , Jour. Amer. Med. Assn., v. 72, p. 626.
Morax, V. Hypothesis regarding the Corti-cal Connections with the Maeular Fasci-culus. Ann. d'Ocul., v. 156, pp. 25-35.
Morax, Moreau, and Castelain. Alterations In Maeular Vision after Occipital Injury. (13 111.) Ann. d'Ocul., v. 156, pp. 1-25.
Pacheco Luna, R. Total Hysterical Amau-rosis. Arch, de Oftal. Hisp.-Amer., v. 18, p. 335.
Pagenstecher, A. H« Recognition of Entop-tic Scotoma. Arch. f. Augenh., v. 38, 1918, p. 14. Abst., Klin. M. f. Augenh., v. 60, p. 686.
Posey, W. C. Permanent Quadrant and Hemianopic Lesions with Migrain. Penn. Med. Jour., v. 21, p. 541. Amer. Jour. Ophth., v. 1, p. 449.
Potzl, O. Inhibitory Phenomena Resulting from Lesions of the Occipital Lobe. Wien. med. Woch., No. 36, 1916.
Prompt. Certain Causes of Optical Illu-sions. Bull, d l'Acad. de Med. Sept. 24, 1918, v. 80, p. 266. Abst., Jour. Amer. Med. Assn., v. 71, 1918, p. 1864.
Pusey, B. A Case of Quadrantic Blindness. Jour. Nerv. and Ment. Dis., v. 47, p. 217.
Rasquin, E. Hemianopsias. (1 pi., Bibl.) Arch. M6d. Beiges, Jan., 1918.
Ribas Valero. Process of Visual Exteriori-zation. Arch, de Oftal. Hisp.-Amer., v. 19, pp. 1-12.
Roelofs, Central Visual Acuity. (Dis.) Amer. Jour. Ophth., v. 1, p. 430.
Roelofs, C. O., and Zeeman, W. P. C. Binocular Clearness of Perception. (6 ill.) Graefe's Arch. f. Ophth., v. 92, p. 527.
Rbnne, H. Behr's Work on Unilateral Hem-ianopsia. Klin. M. f. Augenh., v. 56, pp. 501-504. Abst , Brit. Jour. Ophth., v. 3, p. 175. Ann. d'Ocul., v. 156, p. 123.
Saenger, A. Changes in Visual Centers thru War Wounds. Deutsche Zeitschr. f. Nervenh., 1918, v. 59, pp. 192-230.
Salus, R. Symmetric Scotoma in Uremic Amaurosis. Deutsche med. Wochenschr., Leips. u. Berl., 1917, v. 43, p. 1183.
Sanz, E. F. See Fernandez Sans. Sarnowskl, V. X. Visual Troubles Follow-
ing Injury to Brain. Breslau Thesis. Abst , Clin. Opht, v. 22, pp. 683-84.
Schleich, G. von. Limitation of Function in Synchronous Hemianopsia. Klin. M. f. Augenh., v. 58, pp. 506-507.
Shaw, W. R. Optical Illusion with Fatal Consequences. Science, v. 48, p. 45.
Souques and Odler. Localization of Corti-cal Macula in Hemianopsia. Rev. Neurol., 1917, p. 45. Abst., Arch. d'Opht, v. 36, p. 62.
Stauffer, F. Tumor of the Optic Chiaam. Trans. Amer. Academy of Ophth. and Oto-Laryn., 1917-18, pp. 510-11.
Stein, O. J. Decompression Operation on Hypophysis by Nasal Route. Laryngo-scope, v. 28, p. 376.
Stevens, G. T. Righthandedness in its Re-lation to Visual Conditions. New York Med. Jour., Aug. 17, 1918, p. 269.
Stieren, E. Hypophyseal Tumor with Tem-poral Constriction of Visual Fields. (4 ill.) Trans. Amer. Acad. Ophth. and Oto-Laryn., 1917-18, pp. 54-57.
Strebel. Disturbances of Visual Fields. Schweiz. Arch. f. Neurol. u. Psychiat, 1918, p. 173.
Terrien, F. Ocular Symptoms with Skull Wounds. Paris MeU, v. 8, p. 277, 1918. Abst, Jour. Amer. Med. Assn., v. 72, p. 75.
Tyson, H H. Transient Left Homonymous Hemianopsia (2 ill., Dis. p. 859.) Amer. Jour. Ophth., v. 1, pp. 831-834.

DIGEST OF THE LITERATURE 18'i
Velter, E. Ocular Troubles with Cranial Injuries. (10 pi.) Arch. d'Opht, v. 36, pp. 17-91.
Wechsler, I. S. Homonymous Hemianop-eia and Central Scotoma. New York Med. Jour., v. 109, pp. 624-626.
Weeks, J. E. Homonymous Quadrant De-fects of the Fields of Vision. (Dis.) Arch. of Ophth., v. 48, pp. 163-163.
Yealland, L. R. Hysterical Disorders of Vi-sion. Brit. Jour. Ophth., v. 2, p. 545.
Young, G. Threshold Tests. (7 111.) Brit.
ANATOMY, NEUROBIOTAXIS. The the-ory of neurobiotaxis, as presented be-fore the London International Medical Congress by Kappers, was recognized as of most profound biologic signi-ficance. Jackson comments, it was provocative of reflection rather than discussion, and the value of such a con-ception will be shown by what grows out of it. The location and relation of nerve centers and nerve tracts often seem extremely complex. Kappers' in-vestigations began with a surprise be-cause of the peculiar place which the nuclei of the ocular muscles of some fishes occupy. His observations have been carried out in fishes and some of the lower animals. Kappers' paper cannot be intelligently abstracted here, but it clearly shows that the gap be-tween such a theoretic hypothesis as neurobiotaxis, and the practical ques-tions of ophthalmic practice, is not so great as might at first appear. He has effectively used the relations of the cell groups and nerve tracts concerned with vision, to illustrate and support his hypothesis, that the arrangement of the nuclei is determined by the com-mon or habitual association of sensa-tions and movements.
LOCALIZATION OF VISUAL CENTERS. Henschen defends his theory of the
centers of sight from the attack of Monakow and his followers, and claims that his opponents' views are contrary to anatomic facts. He argues that be-cause of the difference in structure of the periphery and center of the lobe they are affected differently. He claims that the upper border of the calcarine cortex corresponds to the lower half of
Jour. Ophth., v. 2, p. 384-430. Amer. Jour. Ophth., v. 1, p. 503.
Zeemann, W. P. C. Binocular Perception of Brightness. Nederl. Tijdschr. v. Geneesk., 1917, p. 265. Amer. Jour. Ophth., v. 1, p. 368. Conflict of the Field of Vision. Nederl.
Ophth. Soc, June 9, 1918. Klin. M. f. Augenh., v. 61, 1918, p. 142.
Zeemann, W. P. C, and Tumbeleka. Central and Peripheral Vision of Congenitally Blind Cat. Graefe's Arch. f. Ophth., v. 91, Part 2.
the retina, and that the lower half cor-responds to the upper half of the retina. Small defects in the cortex produce scotomas. The macula is represented in a certain area in the cortex. Hen-schen, after destroying the cortex of animals' brains, corresponding to the centers of sight, found that the geni-culate body degenerates. The geni-culate body contains numerous types of cells, the function of which has never been determined. Small lesions in the geniculate body produce scotomas in the visual fields.
Zeemann examined the eyes of a congenitally blind cat, nine months old. The eyes were hardened in formol and opened after enucleation, and stained by the hematoxylin-eosin and Weigert-Gieson method. The anterior portions of the globe showed no important changes. Microscopic examination dis-closed no vestige of optic nerve, no opening in the sclera, and entire ab-scence of pial sheath, nerve, glia, or primary optic stem. The choroid was also a closed capsule. The retina was detached and appeared to be rolled around the vitreous membranes. I t showed only two layers, a nuclear layer and a reticular, which was poor in nuclei. Nerve fibres, ganglion cells, rods and cones, were entirely absent, and no blood vessels were in evidence.
The brain of the cat was examined by R. Tumbeleka. He found an en-tire absence of the optic nerves. The lateral corpus geniculatum had no cap-sule, and was much reduced in size. The laminae medullares were hardly visible. The corpora quadrigemina were normal but reduced in size, which was also true of the visual cortex. The
DIGEST OF T H E LITERATURE.

188 DIGEST OP THE LJTERATURE
condition was apparently due to an ar-rested development together with some pathologic influences which destroyed the retina secondarily. The disturb-ance must have occurred at about the fifth or sixth week of fetal life.
Morax, Moreau and Castelain have studied the visual defects of eighty-six cases with wounds of the occipital re-gion with both the perimeter and by the method of Haitz. Special attention was paid to the effect of these injuries on macular and central vision.
The observers were able to follow their cases thru a long period of time, and to study them two or three years
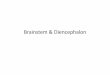
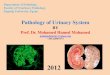
Fig. 1. Homonymous Hemianopsia, Typical. (Morax, Moreau and Castelain.)
after the injury was received. They classify their cases into seven groups, depending upon the type of defects found in the visual fields. (Charts represent whole field and macular field.)
1. Homonymous hemianopsia, typi-cal. Fig 1., 20 of the 86 cases (30%) in this group. The border of the hem-ianopsia is in the vertical meridian, passing from 5° to 10° from the verti-cal in the macular region, (a) Macular region not affected, (b) Macular region more or less affected on the blind side. Visual acuity normal excepting 2 cases, V. = 5/10. In all cases fusion,
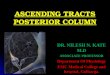
stereoscopic and diploscopic tests nor-e mal. i 2. Homonymous hemianopsia and - scotomas. (Fig. 2.), 15 of 86 cases, 14 e in inferior sector. In the homonymous
types the sectors are triangular. The e apex of the triangle approaches or is t in the macular region. In 8 of the cases
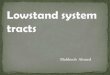
the macular region was affected. f 3. Hemianopic Scotomas. (Fig. 3.) i 20 of the 86 cases. The frequency of 3 this type of defect in occipital lesions
is striking. Vision apparently normal / and subject is often unconscious of :, any defect. Fusion defective in 5 of i the cases.
Fig. 2. Homonymous Hemianopsia and Scotomas.
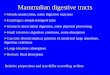
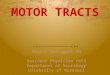
4. Homonymous hemianopsia and scotoma, hemianopsia on opposite side. (Fig. 4), 14 of the 86 cases. In 10 cases macular region was involved, due to lesions of both sides of head. Vision good. Stereoscopic and diploscopic tests normal.
5. Double hemianopic scotomas. (Fig. 5.) Sometimes called annular scotoma, 2 cases seen.
6. Homonymous hemianopsia with central scotoma involving the whole macular region. In this type the verti-cal boundary does not recede from the fixation point as in the former cases, but includes it and involves the entire

VISUAL TRACTS AND CENTERS 189
half of the macular field. The vision in the case observed was 1/100.
7. Complete blindness on account of occipital lesions. This type is uncom-mon and only one case of this type was seen. Both occipital lobes were in-jured and complete obliteration of both fields resulted. From the study of their cases they conclude, that more often in macular visual disturbances follow-ing injuries to the brain, only one-half of the macular area is suppressed.
Morax concluded that the macular region is divided into 2 halves that are homonymous in the visual center. The
visual centers of the occipital regions are not the same for the macula as for the periphery. The central area for the macula is in the posterior extremity of the lobe. Conservation of normal visual acuity is compatible with destruction of one of the visual cen-ters.
Ronne concludes: 1. That incon-gruence due to errors of observation in perimetry may be avoided by using a series of test-objects. 2. That true incongruence is present when the le-sion is at a part of the optic path where the fibres from corresponding retinal points are not yet associated. This is more likely to be the case the further forward the lesion is. Ronne believes
that a pronounced incongruence in hemianopsia indicates a lesion of the tract near its junction with the chias-ma. 3. That, owing to the normally greater extent of the temporal field, its outer part is not associated with any
Fig. 4. Homonymous Hemianopsia and Scotoma. Hemianopsia on opposite side.
part of the nasal field of the other eye, but remains unpaired. Incongruence may thus exist in so far as the temporal defect in one field may be greater than the nasal defect in the other, to the ex-
Fig. 3. Hemianopic Scotomas.
tent of the unpaired portion of the for-mer. 4. That incongruence may occur in respect of an upward divergence of the vertical margins of hemiopic fields. This symptom is not concerned with the arrangement of the nerve fibres,

190 DIGEST OF THE LITERATURE
but with the fact that the hemianopic symmetric plane does not fall exactly in line with the sagittal plane of the eyes. 5. According to Wilbrand, the cortical representation of correspond-ing points may be irregularly arranged, and thus incongruence in the fields may be produced. 6. The sparing of the macula or overflowing field of Wil-brand is another form of incongruence. Ronne concludes that this is due to a purely peripheral interweaving of the nerve-fibres in the retina. At the same time a difference in the two sides in this respect must in all probability be referred to an irregularity in the ar-rangement of the cortical representa-tion.
Cases illustrating the various forms of incongruence are described, and numerous charts are given. Ronne concludes that individual irregular-ities in the arrangement of the nerve-fibre bundles may exist. Altho this explanation may not be considered very satisfactory, he sees no other way out of the difficulty. The mixing of the fibres is in the great majority of cases extremely regular.
Meyerhof believes that in cases which have incongruent hemianopsia the condition is due to an arrange-ment of the nerve fasciculi in the oc-cipital lobe in an unusual manner, and not according to rule. He reports two cases with fields of that type, in both of which the wounds were in the occipital region of the head.
Igersheimer records his observations in defects of the visual fields due to various causes. The article is illus-trated with eighty-seven interesting cuts which simplify the text. From the study of his cases the author concludes that the ordinary method of taking the visual fields, with the perimeter, is the most reliable means of studying de-fects that may be encountered, and ad-vises the use of more delicate instru-ments for measuring macular and peri-macular vision.
He urges the more careful study of the blind spot, especially to determine early the presence of bitemporal and homonymous hemianopsia. Special study should also be made to ascertain
the relation of the defect to the macula and fovea centralis.
From the author's wide experience, both clinical and experimental, he con-cludes that the probable reason that the macular vision is saved in some cases of injury in which hemianopsias are present, is due to the presence of a double blood supply of the portion of the occipital lobe which represents the macular area. In addition to the cal-carine artery, the second artery found in some cases, is the posterior temporal which is a branch of the posterior cere bral. This temporal branch of the pos-terior cerebral in some cases is the chief artery to the posterior pole of the occipital lobe in which the macular cortical centers are located. . PHYSIOLOGY.—Visual Fields. Land-wehr adds a worthy contribution to our knowledge of anisometropia. His con-clusions are based upon the results found in the examination of seventy-two anisometropes. The three features of special interest in (this condition which he investigated a re : binocular clearness, the preponderance of the visual fields, and the localization of direction and depth. In regard to bin-ocular clearness, the less ametropic eye, in the large majority of cases, plays the more prominent part. The same is true in regard to the visual fields, altho after correction,. both eyes act more equally. Each of both halves of the visual field is dominated by the homonymous eye, even if this eye is the more ametropic. Depth-vision, in most anisometropes, is de-creased, altho in low grades there is a certain amount.
High degrees of fusion capacity are found among corrected anisometropes, altho, as in the case of normal eyes, strong individual differences occur. A not unimportant increase of the fusion-power may follow permanent correc-tion. In certain cases where total cor-rection of the ametropia has been at-tempted, it has resulted in earache, epiphora, nausea and other reflex symptoms. The cause seems to be the prismatic action brought about by the patient looking thru both upper and lower parts of the lenses, which pro-

VISUAL. TRACTS AND CENTERS 191
duces an unequal displacement of the visible objects. In general, however, total correction of anisometropia is recommended.
Zeemann, with the assistance of Roe-lofs, experimented regarding binocu-larly observed brightness, and the im-pressions which each eye received separately, especially when these im-pressions had an unequal brightness. Cartoons which could be quickly changed, were placed in a stereoscope. On all. these cartoons there was a gray of more brightness on the right side than on the left. The gray which was perceived was darker than the light and lighter than the dark field. The experi-ments seemed to prove the significance of the outlines, giving the impression that the figure attracts the attention, thus giving a preponderant significance to the retinal image in the concerned eye. Experiments were then made, so that the influence of the outline in dif-ferent parts of the visual field were different. The results of these obser-vations are: (a) If a gray of unequal brightness is seen by each eye, the im-pressions will fuse, (b) The binocu-lar impression is not of constant qual-ity. (c) In particular, the outlines give a preponderant significance to one of the retinal images, (d) This in-fluence does not depend on light, con-trast, etc., but on force wherewith it directs the attention on one of the retinal images or parts thereof.
For the purpose of making clinical tests for the threshold of light and color, Young uses standard inks and produces fixed dilutions of over a thou-sand degrees. He places a circle of color on each leaf of a small album. The leaves are turned, fairly rapidly, in view of the patient. By this method it has been possible to quickly discover the existence of scotomata and to es-tablish a certain relationship between color perception and certain eye dis-eases. For instance, in the retinitis of pregnancy, perception for yellow is markedly reduced, while in the album-inuric retinitis of trench fever, it is not reduced.
Lloyd calls attention to the unsatis-factory and even erroneous results ob-
tained by the use of the perimeter in attempting to outline central defects in the retina. We are familiar with the classic picture produced by a block-ing of the' central retinal artery, but when a branch of the artery is affected the signs and symptoms change so quickly, it is difficult, after a month or two, to know what has happened un-less one has followed the case from the beginning. For this class of cases, Lloyd finds the stereoscopic ca;npi-meter slate a much more reliable means of obtaining an accurate outline of both form and color scotomata. He believes it seems reasonable to say that the usually accepted conditions which pro-duce central or paracentral scotomata, toxic neuritis, sphenoidal disease, mul-tiple sclerosis, hereditary neuritis and glaucoma, we should add the condition of blocked macular arterioles.
Fridenberg discusses the importance of careful ocular tests in the examina-tion of aviators. He shows that visual factors enter largely into the conditions of equilibration and vertigo. It has been taken for granted that if the labyrinth, being the principal organ of balance, is normal, the subject might fly safely. He warns against this hypothesis, and believes that it is of equally high importance to deter-mine a normal condition of vision, ocu-lar muscle balance, and binocular fixa-tion, to be assured of a state of normal equilibration when under the unusual conditions of flying in high altitudes.
Stevens believes that the custom of righthandedness has a decided influ-ence upon vision. Resulting from the more general use of the right hand, the anterior portion of the left cerebral hemisphere, which controls these movements, is correspondingly more developed than the right side, and the left orbit is thus pushed outward and the axis of the cavity changed from a vertical to an oblique direction. The globe of the eye is thereby tilted, its vertical meridian leaning outward toward the temple. This leaning is so common that its absence suggests, al-tho it does not prove, lefthandedness. It can be readily seen that a certain confusion of vision must result when

192 DIGEST OF THE LITERATURE
the meridians are not in their normal relations. Unless they are parallel in the primary position, there cannot be such harmony of action of the two eyes as to give simultaneous impressions on exact corresponding points of the two retinas in any position. Stevens urges the importance of bringing up the child to be ambidextrous.
PSYCHOLOGY OF VISION. — Colored hearing, the most common of the syn-esthesias, now has a large literature, but few truths can be uttered in re-spect to it, on account of its individual-istic and impressionistic character. About a dozen years ago, Blanchard assisted at a concert in London, in which, while a piano was played in the dark, each note was represented by flashing an incandescent light in a spe-cially colored bulb. The same note was always indicated by the same color. Many of the audience spectators pro-fessed to experience the same pleasure from the harmony of colors that others felt from the harmony of sounds. More recently a similar concert was held, when there was a demonstration of an organ in which pressure on the keys caused colored lights t:> iiash on a screen. The organist executed color symphonies which gave to s tme of the spectators pleasure analogous to that of musical symphonies. Ribas Vallero made an extensive study of visual ex-teriorization and discusses the various classifications.
MIRROR WRITING.—Bramwell refers to a case, which he recorded several years ago, in which a sudden vascular cerebral lesion, apparently embolism of the left middle cerebral artery, in a man, who from birth had been strongly left-handed, but who had been taught to write only with the right hand, pro-duced right-sided hemiplegia and marked and persistent aphasia. This condition he termed "crossed" aphasia. In a recent publication he considers in detail the explanation of "crossed" aphasia, and points out the two forms of impressions involved and stimulated to effect the phenomenon of "mirror-writing."
In his extensive thesis on the theory of binocular color mixture, Dawson
goes over in detail the theories which have been propounded by Haldat, Helmholtz, Wheatstone, Meyer, Her-ing, Dove and many others. He states that while no wholly satisfactory ex-planation of binocular rivalry has been put forward, that which seems to fit the facts best is the attention theory.
Mirallie and Denes report that a woman stricken suddenly with right hemiplegia and motor aphasia, began at once to write with the left hand, be-ginning at the right side. Her .writing was thus of the mirror type, and she never noticed that it was not her usual way of writing. Figures as well as words and phrases were of this mirror type, but when she added or subtracted figures, she began at the correct point at the right. They regard the case as confirming the view that mirror writ-ing is Ihe normal form of writing with the left hand.
Because the examination of the vis-ual acuity is often considered to be the same as an examination for the "min-imum separabile," Roelofs has made the examination with a number of objects of different widths and lengths. The results show that the minimum separ-abile, the angle under which the small-est recognizable interspace between two objects is seen, is not constant. I t may be, however, that the observation width is still constant, altho the interspace itself is not. If two squares, the diameters of which are equal to the interspace, are used, the entire length will appear to be three perception cir-cles. The true length does not neces-sarily agree with this. When a row of squares .was used for this test, the di-ameter of a perception circle, in an emmetropic eye, was found to be SO seconds. When a series of lines was used instead of squares, the percep-tion width was about 40 seconds.
VISUAL ORIENTATION.—Holmes, dis-cussing cases of disturbances of vis-ual orientation, says : Cases could not be reported satisfactorily owing to the injuries being so severe and the mental processes so disturbed that a satisfac-tory examination could not be made.
There was no paralysis, limb move-ments normal, no ataxia, right plantar

VISUAL TRACTS AND C E N T E R S 193
reflex was extensor. Tactile and pain-ful stimuli were appreciated ccrrectly, no loss of sense of position, no (ptic neuritis.
Entrance wound twenty-three centi-meters behind nasion, and seven centi-meters to right of middle line. The ball could be felt under the scalp four centimeters behind and four centi-meters above the margin of attachment of the left pinna. Reflexes became nor-mal. He had been an intellectual and educated man, and he rapidly regained his intellectual faculties. Memory for the past was fair, the period immedi-ately preceeding the wound blank; this gradually diminished.
His behavior was that of an intelli-gent child, was too facile, laughed un-necessarily and inappropriately, could carry out complicated orders, never used wrong words, could read and comprehend short sentences, could not write or even draw a short line. This was due to apraxia of his arms rather than to a specific agraphia. He showed bilateral ideomotor apraxia, t n a t is, he could not perform simple Purposive actions or use objects or in-struments with which he was familiar. th i s was not due to weakness, ataxia or sensory disturbances in his limbs.
His visual disturbances were as fol-lows:
He could not seize or touch anything Presented to him, or extend his hand in the proper direction toward it, tho he could perceive and recognize it. He could not look at an object, but would I0.1' his eyes in an irregular manner. Vision was 6 /6 ; disc normal. Fields "ear normal, but some amblyopia in ooth lower right quadrants. Red and green fields were normal. He could move eyes correctly to command, or 'OCate a nf>Uf> Knf r n n U n n t An «rv othe
a noise, but could not do so rwise except after several at-
* e m Pts . He could not keep the eyes fixed °n a spot when the head was turned passively. There was no with-drawal of the head or closing of the ^ s when a feint at striking him was ofth' n ° . c o n v e r g e n c e , no contraction
the pupii s to accommodation, no ag-osia, that is, inability to recognize jects. Visual memory was good,
visual retentiveness poor. On attempt-ing to pick up an object he would grope for it like a man in the dark. There was great difficulty in localiz-ing objects in space when they were outside the line of fixation, often fail-ing to recognize moving objects by ex-tracentral vision, tho they were outside that portion of the visual fields which were amblyopic. He could not recog-nize the relative position of objects within his field of vision.
When he could touch the objects he could correctly orient them, but could not tell which was the shorter of the two lines or the relative size of the objects. Stereoscopic vision was un-affected. The attention to visual im-pressions seemed to be arrested or oc-cupied by any object that, at the mo-ment, was in his central vision. He could not count coins on a table but could do so if he could take them in his hand.
His walking was not ataxic, but he walked with shuffling steps, and would run into objects tho aware that they were present. He would run into a wall. This was due to the visual im-pressions not exciting attention to the objects. He could not find his way about the ward in which he had been for weeks;" with eyes closed he could walk correctly towards a sound.
Summarizing the visual disturbances of this case, they are as follows:
Central vision intact; except for slight amblyopia in right lower quad-rants the fields of vision were uncon-tracted. Owing to disturbance of vis-ual attention he frequently failed to perceive objects moving within his range of vision.
Remaining symptoms may be grouped in two classes : (1) Disturb-ance of ocular movements, difficulty of fixing objects or of maintaining fixa-tion on moving objects, absence of ac-curate convergence and accommoda-tion, and the visual blinking reflex. (2) Disturbance in visual loealization and orientation in space, inability to touch or indicate directly the position of objects seen. There were errors in all directions, but most prominent in the estimation of the distance of objects

194 DIGEST OF THE LITERATURE
from him. He could not distinguish the relative position of objects in space or the relative size of objects.
Results of these disturbances are as follows: Difficulty in exploring- sur-face with his eyes, difficulty in counting similar objects placed in series or scat-tered about in his field of vision, and difficulty in reading, the latter being due partly to difficulty in fixation, and partly to difficulty in appreciating rel-ative positions. He ran into objects when walking because the retinal images did not excite his attention, and he could not assign the objects to their relative positions in space as regards himself.
Several other cases are reported with approximately the same symptoms.
In summarizing, the following ob-servations are made : The symptoms cannot be due to defects of visual per-ception as the central vision was nor-mal, or approximately so. In the ex-amination of many cases with central and paracentral scotoma due to gun-shot injuries of the brain, it was f^uncl that spacial perception was not af-fected, or in this sense affected by hem-ianospia, or other large losses in the field of vision, whether they be due to corti-cal, subcortical, or tract lesions.
The affection of visual orientation was obvious in several tests. The pa-tient was unable to touch objects with-in his range and vision, tho the move-ments of the arms were intact. He collided with visible objects in walk-ing and had difficulty in finding his way around them. He could not recog-nize the relative position of two sim-ilar objects in space. In attempting to touch an object, he made errors in all three dimensions of space, particularly in the estimation of distance.
Our power of recognizing the rela-tive position of objects in space de-pends upon the mosaic images of them to the central image, since it is from the macula that we measure the dis-tances of the objects from each other. Analogous cutaneous signs enable us to locate any point on the surface of the body that is touched. In certain lesions of the central nervous system, these cutaneous signs are abolished
and the same condition obtains with the retina, but retinal stimuli suggest only magnitude and relative positions of objects in a bi-dimensional plane.
To obtain correct knowledge of the relation of the objects to ourselves, the different impulses from the ocular and neck muscles and tendons inform us of the direction of the visual axis. The knowledge of the position of our head is also necessary.
The estimation of distance depends largely on the perceptive impulses from the ocular muscles, especially those of accommodation and convergence. Fa-miliarity with the size of the object, light intensity, etc., also are concerned. Thus the estimation of distance being the most complicated process, it is na-tural that this should be the most af-fected. This accounts for these pa-tients colliding with objects, walls, screens, etc.
In attempting to touch seen objects, they were at fault for the same reason. We acquire our knowledge of space from visual experiences, tho muscular, tactile, or other impressions also con-tribute to it. The memory of spacial relations was disturbed, also. I t is probable that the cerebral mechanisms, by which the spacial percepts received thru the different senses are associated and assimilated with past experiences, were involved.
The inability to read and to count a number of similar objects was due to this cause. The relative position of the words or objects were disturbed and h e could not tell whether he had al-ready seen the words or objects, (such as a number of coins in front of him and in his field of vision) or had not as yet noted them.
These patients could recognize words as words without difficulty, but when the many words were together, as on a page, then the spacial relation being disturbed, confusion resulted.
Disturbance of visual attention was marked, tho the sensibility of the ret-inae was intact. Thus they did not perceive objects directly in front of them until they had their attention di-rected to them. Several complained

VISUAL TRACTS AND CENTERS 195
that they could only see one thing at a time.
This disturbance of visual attention is so commonly associated with loss of visual orientation that it might be included in the syndrome; only they are not interdependent. The former may occur unilaterally when the lat-ter is no way affected.
The ocular symptoms; include the difficulty which all the patients had in fixing objects visible to them, their failure to accommodate and to con-verge, and the absence of the blinking reflex.
The impairment of fixation resulted from impairment of spacial orientation. The reason for this is, that when the position of the object which throws the image on the retina is not appreciated, the globes cannot be rotated so as to throw the image on the fovea.
In all these cases the wounds in-volved the angular gyrus or its neigh-borhood, a region of the cortex where it is generally understood that centers for ocular movements exist. I t may consequently be assumed that one function of this part of the brain is the reflex adjustment of the eyes to peri-pheral stimuli, or the coordination or integration of the different impressions, which, thru these different centers, evoke appropriate ocular movements in response to retinal excitations. It is assumed that bilateral lesions are nec-essary to produce these symptoms. The lesions in most of the cases in-volved the angular and supramarginal gyri, and extended into the adjoining, occipital, temporal, and parietal con-volutions in the region of the splenium.
CONGENITAL WORD BLINDNESS.— Engler describes a case of congenital imbecility with especial weakness in regard to reading and writing. It d id . not appear to be a local symptom but a "partial idiocy." The diagnosis could not be said to be congenital word blind-ness, and a congenital aplasia of a cer-tain part of the brain could not be proved.
FACTORS IN STEREOSCOPIC VISION.— Eaton calls attention to the importance of a correct estimation of distance as
essential in every department of life, and which has assumed a peculiar im-portance in the life of the aviator. The belief that a single eye gives a certain amount of appreciation of three dimen-sions, often referred to as the "sense of depth," is surely general. This term ought rightly to be included in the term "Stereoscopic vision." The dif-ference between the "sense of depth" and the "sense of solidity," is merely that the former is more realistic in reference to the intervals between ob-jects, and the latter in reference to the objects themselves. Apart from the fusion sense, the chief factor whereby we perceive solidity thru vision, is the shape of the retinal images of symmet-ric objects. There are also the alter-ations of definition according to dis-tance, lighting effects, in the case of very near objects, there is the sense of ocular convergence; and if the observer is moving, there is parallax, etc. A one-eyed man sees stereoscopically in the only valid sense of that word. He will always say that he sees things solid, not flat.
If a pair of stereoscopic photographs be reversed so that the left hand card is seen before the right eye and vice versa, the view should be reversed in the third dimension, making objects in the foreground appear in the dis-tance. This, however, will not be found to occur. The other factors in stereoscopic vision dominate the fusion sense. If the card is reversed, top to bottom and right to left, the fusion sense acts normally, but owing to the unusual view the sense of perspective and the appreciation of shadows are almost wholly in abeyance. Our fusion sense, therefore, appears to be extreme-ly elastic and readily capable of com-promise or even suppression. A painted picture does not appear flat to us, yet our fusion sense ought to make it so, for the two retinal images are similar.
Barrie does not agree with Eaton in his factors in stereoscopic vision, and the visual estimation of distances. If an ordinary stereoscopic photograph view be divided into two halves, he says, and the left half be placed in the

196 DIGEST OF THE LITERATURE
stereoscope opposite the left eye, he sees it double. The view seen by the left eye is projected well towards the right, while the portion of the picture seen by the right eye is projected to-wards the position which the picture actually occupies. With the right half of the picture before the right eye, duplication occurs again, the projection being as already described. The two views in each case show distance and solidity very clearly, the erroneously projected picture being lighter than the other. If now the left half of the pic-ture be placed in the stereoscope be-fore the left eye, and the right half of the picture brought forward so that the projected view of the left is overlapped by the correctly placed view of the right eye, the resultant view shows depth and solidity well marked.
If the right half of the picture is in-verted and placed before the left eye in the stereoscope, it is seen double again, but in this case the sense of per-spective is faulty. The foreground is not thrown into the distance, nor dis-tant objects brought forward when the inverted and reversed halves of a ster-eoscopic picture are seen in a stereo-scope, but a new view is seen in which the fusion sense has full play in the ordinary acceptation of the term. As a consequence, the experiment does not support the contention that "our fusion sense appears to be extremely elastic and readily capable of compromise or even suppression."
FUNCTIONAL AND TRANSIENT BLIND-NESS.—A case of transient left homon-ymous hemianopsia, occurring in a heavy cigarette smoker, following a forty-eight-hour spree, is reported by Tyson. Visual acuity, muscles, tension and pupillary reactions were all prac-tically normal, but the fields of vision showed incomplete left homonymous hemianopsia, with form field contracted to within eight degrees of fixation. The color fields were contracted to fixation in the horizontal meridian. Elimina-tion and light diet, with abstinence of alcohol and tobacco were ordered, and nine days later, color and form fields were quite normal. About eight months later the patient had another
attack, following another spree. The visual fields showed left homonymous superior quadrant anopsia, incomplete; the apex of the angle extending to within five degrees of fixation for form, while that for colors was contracted to fixation. In two weeks his form fields had widened to within ten degrees of normal, while his color fields remained contracted in left 'superior quadrants to about fixation, constituting a left homonymous superior quadrant achro-matopsia. As to the localization of the site of the lesion in these cases, the re-searches of Beevor and Collier indi-cate that it is an occlusive lesion of the right posterior calcarine artery, causing destruction of the inferior third of the cuneus, including all the cortex above and below the calcarine fissure, with the exception of a small point anterior-ly. Alcohol and tobacco were probably the exciting cause of the cerebral an-gioneurosis.
Claiborne, in discussing this paper, reported the case of a young man of sixteen who had been taken suddenly blind, and at the same time the right arm and the entire right side were numb. Ten days later the hemianopsia had disappeared. This transient fuga-cious hemianopsia had never been ob-served before, in so young a person.
HYSTERIA.
Yealland divides hysteric disorders clinically, into two groups: (1) Conditions in which contraction of antagonists could be demonstrated; (2) those in which this could not be demonstrated. By contraction of an antagonistic group of muscles he means the contraction of a group which should be relaxed during the perform-ance of a given movement, as illustrated in blepharospasm, ptosis and spasm of accommodation. The phenomenon of contraction of antagonists cannot be demonstrated in such conditions as lim-itation of the visual fields and ambly-opia, but in these conditions, contrac-tion of antagonists in some other part of the body could be observed. The treatment is one of suggestion and should be completed ,<at one sitting. In his experience it produced complete

VISUAL TRACTS AND CENTERS 197
relief of the physical disability, tho much could not be hoped for in im-provement of the mental state.
Pacheca Luna reports a case of total hysteric blindness in a woman, who had had hysteric convulsions and chorea which lasted for several days. She had been treated for bilateral blindness before. On focusing a powerful light into the eyes, no pupil-lary reaction was perceived. The pupils were permanently contracted. There was a clonic blepharospasm with 130 contractions a minute, which continued while 'the patient was sleeping, as well as with the eye bandaged. Anes-thesia of the bulbar conjunctiva. There was no sensation to pain and heat. Ophthalmoscopic examination nega-tive. No error of refraction. Nose and teeth negative. The tendon re-flexes were negative. There was anes-thesia of palate and uvula. Under treat-ment by suggestion and elimination of toxins, the patient regained normal vision in six months. The blepharo-spasm remained and the fields of vision were slightly constricted.
Guijarro's patient was a young woman who had never presented appreciable signs of hysteria and the family was normal. The bilateral amaurosis developed suddenly after emotional stress—passing under the tree where her brother had hanged himself not long before. Deafness ac-companied the amaurosis at first, but soon subsided. Vision improved un-der suggestion, but several months elapsed before recovery was complete.
TRANSIENT CONCUSSION AMBLYOPIA. —Lemiere describes the case of a sol-dier who after a severe bombardment found that he could not see. Examin-ation showed dilated pupils, severe blepharospasm, normal pupillary re-flexes, slightly blurred disc on the right side, V. = counting fingers with diffi-culty. Very pronounced concentric contraction of the visual field. With no treatment except rest, the vision rose to normal and the visual fields re-turned to normal in one month. The author considers it a case of concus-sion vasomotor disturbance of the oc-cipital lobes.
Bussy records two cases of transi-tory blindness occurring in soldiers following the explosion of shells. The first case had in addition to the blind-ness blepharospasm, mydriasis and ab-sence of pupillary reaction to light. The optic nerve was pale and the retinal vessels were extremely narrow. The patient recovered full vision after re-maining in a dark room for three days. The second case had the same eye symptoms, vision returned to normal in three or four days but the accommo-dation was not recovered for three months. The author attributes these symptoms to vasomotor disturbance dependent upon a retinal anemia and shock to the sympathetic.
OPHTHALMIC MIGRAIN. — Posey re-ported a series of cases under his observa-tion, in which permanent quadrant and hemianopic lesions followed so-called migrainous attacks. He says there is ample evidence in the literature to the effect that migrain may be the fore-runner of organic brain disease, and that an area of softening of the brain may follow, which may manifest itself by a permanent paralysis, aphasia, or hemianopsia. While such lesions usual-ly occur in individuals predisposed in consequence of disease of the walls of the blood vessels, it would seem that in certain cases the vascular lesions may occur in young persons and even in some adults with healthy vessels.
Posey also gave notes of a case of recurrent oculomotor palsy, or oph-thalmoplegic migrain, occurring in a girl of 13; the first attack, with implica-tion of the eye muscles occurring when she was but 6 years of age.
The case of a physician which was observed fourteen years ago was also recalled. He presented almost com-plete ptosis of his right upper eyelid, and a paretic condition of the inferior oblique and internal rectus muscle of the same eye. His ocular symptoms coincided with spells of dimness of vision, associated with flashes of light upon the side affected and followed by headache and nausea. These seizures apparently were typical attacks of migrain.

198 DIGEST OF THE LITERATURE
Pagenstecher reports two cases of scintillating scotoma. He comes to the conclusion that they are not as harm-less as they are supposed to be. Both cases commenced with typical scintil-lating scotoma; later they developed homogeneous defects of vision which remained. In the more severe cases an exact n e u r o l o g i c examination should be made which may show that this condition may originate in disease of the brain. He recommended to such patients that they take great care of themselves, and avoid anything which might prove deleterious to the vascular system.
Hensen saw four cases of complete* internal ophthalmoplegia in migrain. The attacks came on during the menses; and the author believes that the lesions are nuclear, and due to the presence of cysts or small aneurisms in the region of the nerve centers, which are enlarged by the congestion that occurs at that period. Hensen thinks it possible that the paralysis of the internal eye muscles might be toxic but believes that it is improbable. In the cases of blindness associated with migrain the optic nerve is probably the seat of the trouble or a hysteric element might play some part, especial-ly when the blindness lasts over a rather long period of time.
ILLUSIONS, HALLUCINATIONS. — Shaw calls attention to an optical illusion he has encountered among inexperienced swimmers. A person swimming with the wind, and consequently with the waves which travel in the same direc-tion faster than it is possible to swim, receives the impression of being car-ried backward by the water. In the absence of knowledge covering the case, most persons under these condi-tions immediately think of "undertow," become panic stricken, and needlessly exhaust themselves in an effort to reach the shore.
Prompt discusses the accommoda-tion for perspective, the perception of objects in relief, of the acute angle, etc. His conclusions as to certain features of physiologic vision suggest an ex-planation for a number of optical il-
lusions, including the "canals" on Mars.
Cave refers to the optical phenomena in the experiments of Aitken with ro-tating discs. The discs were divided into about twenty-four sectors, white and black alternately, and with end-less bands of paper with black bars painted across them. A convenient way of viewing the appearances was to look at a sheet of mottled paper after looking at the rotating disc, when the markings on |the paper appeared to move in a contrary direction to the ex-citing impression. If, after viewing the rotating disc, another similar disc be looked at, the second disc appears to rotate in a contrary direction to the first; but if the second disc is larger than the first, this extension will en-tirely destroy all appearance of rota-tion, and the disc will appear at rest. He asks if these experiments do not suggest that the seat of the illusion is deeper than the retina.
Allen believes that the seat of this illusion begins at the retina, but in-volves all the intricate labyrinth of nerve tissue from the retina to the highest sensory and motor centres. Be-cause, when the objects in a given visual field are moving in different di-rections, or some of them not moving, the eye usually fixes on one of the ob-jects, regarding it as stationary, and treating the others as moving. This requires both a muscular and a nervous effort involving the coordinating mechanism of the higher nerve centers; and when the stimulus ceases or changes, the reciprocal after effects in these centres are apparently inter-preted as opposite motion. A change to nerve-muscle coordination is neces-sary to accommodate the eye to a changed stimulus.
Gordon reports four cases in which visual hallucinations were present. All occurred in middle aged women during the involutional period. In each case the visual hallucinations were in the form of children. The author believes that the underlying cause was toxic in three of his cases; and the fourth was precipitated by hysteric paroxysms.

VISUAL TRACTS AND CENTERS 19C
INHIBITION OF VISIONS.—Apart from h y s t e r i c amblyopia, Hurs t and Symms report that they have never seen patients with hysteric symp-toms, who spontaneously complained of disabilities resulting from a narrow field of vision. They have examined numerous soldiers suffering from var-ious war neuroses, but have never found any retraction of their field of vision until they were tested with the perimeter. They claim that the peri-meter invariably resulted in the sug-gestion of a narrowed field. If the ex-amination was continued after the first field had been marked out, a spiral field was always obtained, identical with that which has hitherto been regarded as a stigma of hysteria. This has not been found oftener in hysteric cases, simply because it has not been looked for. An outward spiral is always ob-tained instead of an inward one, if the white disc of the perimeter is moved outwards instead of inwards, as is com-monly done.
In the course of some investigations on "Experimental Malingering," twen-ty-seven individuals, who were pre-tending that they were paralyzed on the right side as a result of a railway accident, were asked whether they could see as well with the right eye as with the left. Seven replied that they had noticed some impairment of vision in the right eye. On testing the field of vision with the finger, no narrowing was observed, but when tested with the perimeter, all of the seven showed a narrowing on the right side, and one had a slight .narrowing on the left.
LESIONS OF OPTIC CHIASM.—Physi-ologic experimentation and clinical ob-servation, according to Lewis, strongly indicate that the hypophysis cerebri when normally functioning exercises a controlling influence not only over the skeletal and muscular structures, but °ver the nutrition and development as well as over all of the tissues having an epiblastic and mesoblastic origin. I t follows that its aberrations of function will find their expression in the less commonly recognized forms of dyspitu-rtarisrn, and in a wide range of atrophies and dystrophies which have
been vaguely relegated to congenital deficiencies or other equally indefinite causes. I t is already known that be-tween the advanced forms of hyper-pituitary activity, and in dyspituitarism in retarded development, both physical and mental, is the entire gamut of pos-sibilities in which vital physical dis-turbances occur; without there being of necessity any discoverable alteration either in the organ itself or in the bony cavity in which it rests. The thera-peutic employment of thyroid and thymus gland substance is of value, but must be used with judgment and caution, as at times they produce pro-found effects.
Hypophyseal tumors, when repre-senting a local manifestation of a constitutional condition, syphilis for example, may be treated by the recog-nized specific therapy. If, however, an X-ray picture shows an enlargement of the sella turcica, we must have re-course to some other form of treatment, Loeb calls attention to X-ray treat-ment, in those cases where, from var-ious conditions, it is impracticable to resort to surgery. ' A number of cases thus treated show as good results as cases where decompression or removal of the tumor has been done. X-ray treatment is especially favorable in that class of tumors where the symp-toms are due to compression, especially of the optic nerves. Here the X-ray is useful in all stages, particularly the early ones, before atrophy of the nerves has developed.
In cases where the symptoms are especially manifest in the bony skel-eton, organic lesions already establish-ed, cannot, of course, be made to dis-appear. In the later stages of this condition, where the hyperfunction has given place to insufficiency of secretion, this treatment is contraindicated. He describes a case of his own in a woman 38 years of age, who had been suf-fering from headaches for five years, gradual lowering of vision, dizziness, nausea, etc. An X-ray picture of the head showed an increase in the area of the sella turcica. The method of giving the X-ray treatment is fully described. Almost from the beginning of the

200 DIGEST OF THE LITERATURE
treatment there was an alleviation of the headaches. The improvement from an ocular standpoint has not kept pace with the improvement in her general condition.
Considering the vast amount of liter-ature published in recent years on ocular complications in nasal accessory sinus disease, bitemporal hemianopsia is of extremely rare occurrence. In a collection of 315 cases of bitemporal hemianopsia made by Bogatsch in 1912, only one of them was considered due to postnasal sinus disease. A case of this kind is reported by Conlon, where the perimetric chart showed typical bitemporal hemianopsia. A submucous resection of the septum which was markedly deviated to the left side, im-pinging upon the middle turbinate, and both posterior ethmoids and sphenoids were exenterated. A polyp was also removed from the region of the right ethmoid. Within a month there was a rapid return of the fields for white, but the color perception was absolutely lost for about seven months, when there be-gan a gradual improvement. The author calls attention to the fact that the topographic relationship of the chiasm to the sphenoid sinus is not as usually described; that only rarely are they in such close relationship, which would explain the comparative immun-ity of the chiasm to retrobulbar neuritis as commonly associated with post-nasal suppuration.
In that class of hypophyseal tumors which are accompanied by visual dis-turbances, Adson has met with marked success, by surgical treatment thru the intradural approach. Six patients have been thus operated upon, the technic of the operation being described. In two of this group there was very defin-ite bitemporal hemianopsia, with more or less loss of vision in the left eye; one had a complete loss of vision in the right eye for a period of ten years, and a left temporal hemianopsia; one presented a typical acromegalic syn-drome and a temporal color hemianop-sia and constricted object field; one had bitemporal hemianopsia with more or less distorted fields in the left eye, and one had blindness in the right eye.
Postoperative convalescence was un-eventful and rapid in all but one case in which the patient died on the second day. In two cases there was complete restoration of vision, in two, marked improvement of vision, and in one a relief from headache. The author points out the advantage of this method of operation over others.
The operation for decompression of the pituitary body may be carried out by the transtemporal, the transfrontal, or the transphenoidal route, the last named being used thru the mouth, thru the antrum of Highmore, and thru the nose. Stein strongly advocates the method by the nasal route, as with the technic now employed, it g i v e s ample room for working with minimum tissue loss, and to the rhinologist in particular this operation offers an ex-ceptionally favorable avenue by which to approach the floor of the sella tur-cica, after opening up the way by a submucous septal resection. He can easily and rapidly open widely into the sphenoid cavities, which then gives easy access to the sella floor and the gland that lies within. The ideal anes-thesia is morphin-hyoscin or scopola-min-morphin with flake cocain locally on the septum and sphenoid.
An absolute knowledge of the top-ographic anatomy of the region is of supreme importance, as the anterior or or middle cerebral fossae might be en-tered, jeopardizing the chiasm or the cavernous sinus. But whatever an-atomic conditions may be present it is always necessary for the operator to keep working in the median line to escape injury to nerve, ' artery and cavernous sinus. This in itself is a strong argument in favor of the septal route, as one is always working in the median line from the beginning. An ad-vantage of working submucously is that the entire operation is confined be-tween two mucoperiosteal flaps and with proper aseptic technic these flaps can be brought together at the end of the operation, thereby avoiding any danger of afterinfection.
Stauffer reported the case of a ten year old boy, phenomenally bright in mathematics, but unreliable, untruthful

VISUAL. TRACTS AND CENTERS 201
and early developing criminal habits. He had been blind for the past three years. A diagnosis of tumor of the pituitary gland had been made, and he was operated upon but died on the operating table. Necropsy showed an absence of the pituitary gland and its place taken up by a tumor of the optic commissure, probably a sarcoma. The doubtful question of importance and interest was whether the condition of the boy was due entirely to the absence of the pituitary gland, or whether her-edity played an important part in his case.
Stieren reports the case of a man 33 years old who complained of im-paired vision and some disturbance of mental functions. Examination showed bitemporal hemianopsia, nearly com-plete on the right side and within 10° of fixation on the left. X-ray examina-tion revealed enormous enlargment of the sella. Acromegalic enlargment of the head, hands and feet had been pro-gressing for seven years. Under local anesthesia the sphenoidal sinus was opened and found to be almost obliter-ated by the depression of the sella floor. Pathologic report of the tissues re-moved from the sella showed the growth to be carcinoma. Considerable enlargment! of the visual fields, im-provement in vision and his mental condition followed the operation.
Priichte had a case which developed a central scotoma which varied in ex-tent on different days. The condition subsided after draining the ethmoidal sinuses. He also saw a case with cen-tral scotoma which followed a fall from a horse, which the author attributes to a hemorrhage into the optic nerve pro-ducing pressure on the papillo macu-lar fibres. The author encourages the use of the Bjerrum method far mapping out defects of the visual fields.
LESIONS OF OPTIC TRACTS.—Keen and Ellis report the successful removal of a fibroma of the brain, which is of spe-cial interest because of the fact that it was the first operation of this kind that they had performed, and also because the patient lived for thirty years after the operation. The diagnosis was made of pressure on the anterior lobe of the
left hemisphere involving the third con-volution and extending backward, due to exostosis, tumor, or possibly only thickening of the dura. Later, and be-fore the operation, the diagnosis was more definitely limited to a tumor. He had become totally blind, and aphasia was marked. He had numerous epilep-tic attacks. The tumor after removal weighed almost a quarter of a pound. His vision became improved so that he was able to go about until about three years ago. Midway between the time of the operation and the time of his death, an examination by de Schweinitz, showed postpapillitic op-tic atrophy. R. V. hand movements, L. V. 1/30. Vertical nystagmus.
Libby reports a case of cystic tumor with papilledema, occurring in a youth of 18. Many signs of meningitis were present and others absent. On the other hand, while a beginning optic neuritis suggested both meningitis and brain tumor, yet there were no localiz-ing signs of cerebral pressure. Distinct optic neuritis soon developed, the papil-la being edematous and hyperemic, but no further retinal edema or hemorrhages were observed. Autopsy disclosed an area of softening about the size of a hen's egg near the left lateral ventricle, and a cyst filled with straw-colored fluid.
Freund saw a case in which homony-mous hemianopsia was associated with tabes. The postmortem findings in the case revealed an intradural aneur-ism of the left internal carotid artery which pressed on the left optic tract, and degeneration of the nerve fibres on the outer portion of the left nerve and the inner portion of the right. The hemianopsia was plainly independent of the tabes.
Hegner and Zange agree that in ab-scesses or tumors of the pontocerebel-lar angle, the clinical symptoms are such that the patient nearly always seeks an oculist first, because the first symptom is a disturbance of vision.. A choked disc is a characteristic symp-tom of these tumors. Motor disturb-ances of the eye, including disturbance of the abducens muscle, will aid in lo-cating the position of the tumor. Later

202 DIGEST OF THE LITERATURE
there are disturbances of hearing. They discuss the technic and dangers of Kraus' operation.
LESIONS OF CORTICAL CENTERS.—As a symptom of ocular migrain, momen-tary hemianopia is well known. As a phenomenon lasting for days or weeks and then ceasing, it is very rare. In regard to the pathology of migrain the theory most generally held is that it is due to a nerve storm of the cere-bral cortex akin to epilepsy, but there is another that it is the result of spasm in a cerebral artery. Stieren reports a case in support of the latter theory, but altho the patient gave a history of occasional attacks of migrain from the age of 8 to the age of 23, these had ceased five years before the hemianopic attacks began, and the connection may have been fortuitous. That the cause of the hemianopsia in this case was the temporary occlusion of the posterior calcarine artery, is supported by a case recorded by Beevor and Collier in 1904, in which a permanent left superior quadrantic hemianopsia was proved by autopsy to be due to a softening of the whole lower half of the right visual cortex, caused by an occlusion of that vessel.
Cases of transient hemianopsia re-sulting from severe concussion of the cerebral cortex following upon vounds o r the occipital region have recently been noted, in which more or less com-plete recovery took place, the recovery for color vision always lagging behind that for form vision. In cases of quad-rantic hemianopsia from war wounds, it is usually the lower quadrant that is affected.
Fernandez Sanz reported three cases of .hemianopsia, two in old men, fol-lowed hemorrhages in the cerebrum, the third case occurred in a young man, age 37, following la grippe. The author believes that the last case was due en-tirely to la grippe.
Wechsler reports two cases of hom-onymous hemianopsia and central sco-toma in patients where the complexity of the findings made the seat of the le-sion obscure. In the first case the le-sion was apparently in the left cuneus near the calcarine fissure which extended
sufficiently inward to include a few of the association fibres going to the hand center for writing, as the patient had mild paragraphia, and very dubious alexia. The other symptoms could be explained by the little understood phenomenon known as von Monakow diaschisis.
In the second case there was a sud-denly oncoming right hemiplegia and right supranuclear facial paralysis, some aphasia and a sudden impoverish-ment of vision in the left eye. The sudden scotoma is not easy to explain. If this followed an intracranial lesion, then little could be done; if, however, it was due to a retrobulbar neuritis consequent upon a local inflammatory condition, vision might have been saved.
Dercum presented a man 67 years old, who became aware, rather sud-denly, of loss of vision in the right visual field of each eye, without other accompanying symptoms. The blood-pressure was high, and the superficial vessels were tortuous and resistant. Wassermann reaction was negative and there were no visible changes in the fundi. Under treatment with potassium iodid, improvement was taking place in vision. The conclusion was reached that there had been a tem-porary occlusion of the blood supply to the cuneus on the left side of the brain.
Lloyd reports a case of sensory aphasia associated with right lateral homonymous hemianopsia, in a man sixty years of age, who had been struck by a motor truck and sustained a V-shaped fracture of the orbital plate of the left frontal bone, as shown by the X-ray. The patient had no object blindness, as he could name many things held before his eyes, but he had a very decided astereognosis, as well as anesthesia of his right fore-finger and thumb, and a coarse tremor of his right hand. He could not recognize nor name simple objects held in his right hand. He was unable to write, either by copying or by dictation, when asked to write with his left hand, he made a capital " E " reversed, as in mir-ror-writing, but got no further. As to the localization of a lesion that could

VISUAL TRACTS AND CENTERS 203
produce all these symptoms, the coin-cidence of word-deafness and word-blindness seemed to point to a sub-cortical lesion within the temporo-oc-cipital lobes in the left cerebral hemis-phere. This could extend deep enough to involve the optic radiatons, also the ascendng sensory fibres to the superior parietal lobule, which would account for the hemianopsia, hemianalgesia, and astereognosis with tremor. The patient failed rapidly and died in a few weeks. Autopsy revealed two lesions in the white substance of the left hem-isphere. One was located above the posterior part of the corpus callosum, bordering upon the posterior median fissure. The other one was just be-neath the cortex at the junction of the parietal, temporal and occipital lobes. The larger lesion proved to be an endo-thelioma.
Weeks reported two cases of ho-monymous quadrant defects of the fields of vision. In one case an absolute sco-toma was found in the right inferior quadrant of both fields with a relative defect extending thru a sector about 30° above the horizontal plane in the upper right quadrant of both fields. T h e d iagnosis in this case is a subcortic lesion either hemorrhage or thrombus affecting the optic radiations on the left side in the dorsal aspect, almost en-tirely, the lesion being located quite close to the cortical visual area.
In the second case the fields of vision showed defects in the upper right quadrant of both fields, but reach-ing the center and shading off gradu-ally toward the periphery below the horizon. The diagnosis is a subcortic lesion on the left side affecting the op-tic radiations, particularly in the lower aspect, not involving the macular bundle of fibers. The lesion is far-ther removed from .the cortic visual area than the first case. History points to hemorrhage.
Pusey reported a case of quadrantic blindness in the lower right fields. A week before the patient had severe pain in the head and in the afternoon of the same day noticed that he could not see distinctly. The patient had agraphia and his memory- was some-
what affected. His previous history and Wassermann were negative. Clegg reported a case of homonymous lateral hemianopsia.
The percent of function lost in syn-chronous hemianopsia is greater than 33}^%. Von Schleich, the author. places it as high as 50%.
Uhthoff holds that 3 3 ^ % of function is lost in synchronous hemianopsia. The percent is about the same as that for unilateral blindness. The syn-chronous hemianopics cannot engage in the trades of commissaries, tech-nicians, buyers, or manufacturers effi-ciently. They are not able to take up work that the one-eyed can and do take up.
W A R INJURIES—HEMIANOPSIA AFTER TRAUMA.—The observations of Morax Moreau and Castelain have been, re-ferred to under Anatomy, p. 187. As chief of the eye department of the Bel-gian Hospital at Havre, Rasquin had the opportunity of observing a large number of cases of hemianopsia en-countered among the wounded. He classifies them according as the indi-vidual requires the aid of another per-son, or not. He found that a gap in the visual fields is more disabling the closer it is to the point of fixation. He gives a colored plate showing the eight different parts of the visual field that may be lost, and the relative disability from each.
Sarnowski has studied the cases of six soldiers who received wounds of the head, in the occipital region. He describes the effects upon the nervous system, and the modification in the visual fields which resulted. All but one of the men showed hemianopsia, and there were marked retractions of the fields.
Behr had two cases with injury to the pituitary body in which the patient survived. The first case was due to a small-bore revolver bullet, which en-tered the right temporal region. When first seen both pupils were widely di-lated and there was complete amauro-sis. One month after the injury there was complete right and partial left oph-thalmoplegia. She was completely blind. Six weeks after the injury the left pupil

204 DIGEST OF THE LITERATURE
showed pseudoparadoxic light reac-tion, contracting considerably after closing of the lids. Pupils contracted with extreme abduction, with the retin-oscope, definite accommodation was noted when there was a fixing on near point in the left.' None of these effects were seen on the right side.
In the second case a blow had been received on the head from a club. For a month after the injury there was loss of memory, alexia, and sensory aphasia, paresis of the left oculomotor nerve. and atrophy of the left optic nerve. There was a right sided hemianopsia. This improved later to a defect in the right temporal field, but left a typical bitemporal color hemianopsia with the dividing line passing thru the point of fixation. The oculomotor paresis re-covered and vision in both eyes was 6/6 six months after the injury. In both cases dystrophia adiposa devel-oped.
Mairet and Durante note that upon repeated examinations of the visual field at a single sitting, the successive fields obtained differ slightly in size— usually by not more than three or four degrees. In certain nervous patients they obtained progressively diminish-ing fields, imparting to the curve the form of a convergent spiral. This pe-culiarity is manifestly not due to focal brain disease, nor was it associated with hysteria. All the patients pre-sented a markedly increased fatigabil-ity, but this is held not to be the main factor of the convergent field, for the sign was only unilateral. I t is be-lieved best accounted for as being a condition of insufficient blood supply or defective innervation of the part, whereby all sustained effort is rendered difficult. The sign seems to be allied to the vascular disturbances described in shell shock, which may involve but one side of the body and sometimes be-come manifest in vasomotor crises of the Jacksonian type.
Velter published an article, with case histories and illustrations of the various eye symptoms following cranial injur-ies. The symptoms depend on the lo-cation of the cranial wounds, but in general, the penetrating wounds of the
cranium produce symptoms which he classifies as follows:
1. Motor troubles.—(a) Motility of the lids; paralysis of the orbicularis, usually unilateral, and most often sec-ondary to complete facial paralysis. (b) Paralysis of one or all of the ex-trinsic eye muscles, due to injury of their motor nerve, diplopia present. (c) Nystagmus, (d) Conjugate devi-ation of head and eyes, (coexisted with a complete hemiplegia in reported case), deviation to opposite side from hemiplegia.
2. Pupillary findings. (a) Mydri-asis most common. When total, usually associated with massive lesions of the head and brain, which frequently re-sult in death, (b) Miosis associated with deep lesions and often associated with bleeding and general intense con-tractures and convulsions, (c) Un-equal pupils not common.
3. Disturbances of sensibility. 4. Lesions of other cranial nerves. 5. Papillitis. (a ) Simple papillitis.
(b) Papillary pseudostasis. (c) True papillary stasis.
Souques and Odier observed the symptoms which developed in a sol-dier who had been injured in the oc-ciput by fragments from a shell. After regaining consciousness, the man was totally blind. The blindness gradually diminished and two months later only a hemianopsia remained. Two sco-tomas were found, one situated in the paramacular field extending into the left macular field as far as the point of fixation. Another scotoma in the right was paramacular, reaching to the edge of the right macular field. The re-mainder of the field had normal visual acuity. The X-ray showed that the skull had been fractured and fragments entered the right occipital lobe with involvment of the macular portion of the lobe. The authors conclude that the macular area is in the posterior portion of the occipital lobe.
Buckley reports the case of a soldier who received a shrapnel wound which fractured the parietal bone on the left side. The dura was torn and the sur-face of the brain bruised. A small pul-

VISUAL TRACTS AND CENTERS 205
sating swelling developed under the operative flap on the twelfth day, which subsided two weeks later. There was a blurring of both optic discs a few days after the operation, and the patient suf-fered from double vision for seven weeks. The right temporal field of vision was absent.
Abelsdorff reports a case with para-central bilateral scotoma, occurring after a wound in the region of the oc-cipital protuberance. The patient had normal vision. There also was a hem-ianopic scotoma of the left field. The small paracentral scotomas were 4° in diameter.
Terrien calls attention to the diag-nostic importance of three symptoms occurring in wounds of the skull, which reveal hypertension, diplopia, restric-tion of the visual field, and choked disc. These conditions subside after lumbar puncture, and if this is not done ir-reparable damage may result. This explains the transient visual dis-turbances sometimes observed long af-ter trephining, which occur more fre-quently when the trephining opening is small. I t also emphasizes the neces-sity for caution in closing gaps in the skull with metal plates or cartilage.
COLOR VISION
BURTON CHANCE, M. D.
PHILADELPHIA This section covers the literature on the subject from June, 1918, to July, 1919. For
previous literature, see volume 1 of the Journal, September, p. 146.
BIBLIOGRAPHY.
Baumann, C. Subjective appearance of Col-ors. Arch. f. d. Ges. Physiol., Ber., 1918, 171, 496-499.
Best. Color Disc Test. Heidelberg Ophth. Cong., Aug. 5, 1918. Abst, Klin. M. f. Augenh., v. 61, p. 344. Munch, med. Woch., 1917, p. 475.
Collins, G. L. Color Blindness. Pub. Health Bull., No. 92. 1918. Amer. Jour. Med. Sc, v. 157, p. 303.
Dangerous and Harmless Color Blindness. Editorial, Jour. Amer. Med. Assn., v. 71, P. 164.
Hess, C. Evolution of Light and Color Sense. Abst., Brit. Jour. Ophth., v. 2, p. 574.
Ishihara. Congenital Color Blindness. Nip-pon Gank. Zassni, Dec, 1917.
von Kries, J. Physiologic Remarks on Ost-•wald's Color Primer. Zeit. f. Phychol. u. Physiol. d. Sehorg., v. 50, pp. 117-136.
Liebermann, P., and Mark, E. Sharpness of Perception In Normal Eye for Color Differentiation. Zeit. f. Psychol. u. Physiol. d. Sinnesorg., v. 45, pp. 103-108. Abst., Klin. M. f. Augenh., v. 61, p. 364.
Luckiesh, M. Retiring and Advancing Col-ors. Amer. Jour. Psychol., v. 29, p. 182.
Oguchi. Transitory Red and Green Blind-ness. Nippon Gank. Zassni., July, 1917.
Oloff. Color Sense in German Army. Hei-delberg Ophth. Cong., Aug. 5, 1918; Klin. M. f. Augenh., v. 61, p. 337A
Ostwald, W-- A Color Primer. Zent. f. Physiol., v. 33, p. 343.
Schibtz, I. Color Perception and Color Blindness in Man and Animals. Med. Rev., Bergen, 1917, p. 425.
Shlosl. Unilateral Congenital Disturbance of Color Sense. Nippon Gank. Zassni, Feb., 1918.
Tests for Color Blindness. N. Y. Med. Jour., Aug. 17, p. 295.
Verry-Westphal, A. The Anomaloscope and Examination of Color Perception. (5 ill.) Clin. Opht., v. 22, pp. 697-706.
Weill, G. Stilling's Isochromatlc Chart for Testing Color Sense. Leipslg, 1918, Thieme. Bert. klin. Woch., 1918, v. 55, p. 648.
DIGEST OF THE LITERATURE
COMPARATIVE COLOR PERCEPTION.— rately known to the human eye under Hess gives the details of experiments different conditions. carried out upon various animals in . In testing vertebrates, by the use of which he used spectral colors, the lu- grains of rice on a black surface which Riinosity of which is sufficiently accur- he illuminated by the spectrum, he