Embed Size (px)
Citation preview

Vertebral Artery Occlusion Following
Hyperextension and Rotation of the HeadBY S. OKAWARA, M.D., AND D. NIBBELINK, M.D.
Abstract:VertebralArteryOcclusionFollowingHyper-extensionandRotationof theHead
• This is a case report of a lateral medullary syndrome of Wallenberg following occlusion ofone vertebral artery and stenosis of the opposite artery precipitated by combined motion ofhyperextension, rotation, and lateral flexion of the head within physiological limits. Sufficientduration of such head position appeared to initiate thrombus formation following stenosis orocclusion of the vertebral artery at the level of the atlanto-occipital joint. Propagation of thisthrombus obstructed the posterior inferior cerebellar artery causing infarction of the lateralmedullary region. The pathogenesis of this mechanism is discussed.
Additional Key Words Wallenberg syndrome vertebral artery thrombosisposterior inferior cerebellar artery atlanto-occipital joint
• Medullary or upper cervical spinal cord infarctionsyndrome following traumatic occlusion of thevertebral artery has been described with cervical frac-ture,1"3 cervical manipulation,47 and calisthenics.8
Decreased blood flow through the vertebral arterywithout cervical fracture or dislocation is presumed tooccur with hyperextension8 and/or excessive rotation9
beyond physiological limits by external forces.1- "•9
However, the mechanism of arterial occlusion, throm-bosis, and infarction has not been clarified from post-mortem or clinical findings.6
This article presents a description of a lateralmedullary syndrome following sustained physiologicalhyperextension, rotation, and lateral flexion move-ments of the head for a period of several hours. Theangiographical survey demonstrated completeobstruction of the right vertebral artery associatedwith severe stenosis of the vertebral artery on the left.The clinical course and angiographical abnormalitiesprovide an interesting sequence of events whichsuggest a probable mechanism of progression for thistype of vascular occlusion.
Case ReportA 43-year-old left-handed male draft designer experiencedoccasional nonvertiginous dizziness for two years. OnMarch 21, 1974, he painted the ceilings of two rooms in hishome, beginning in the early morning and finishing in thelate afternoon. While painting, he used a roller or brush inhis left hand. Therefore, his head was maintained inhyperextension, rotated to the left, and tilted to the right.Occasionally he used his right hand while his head remainedhyperextended, rotated to the right, and tilted to the left.During that afternoon, he noted occasional dizziness as heused his right hand. The remainder of the day was not un-usual and he was in no particular distress. The next morning,
From the Division of Neurosurgery, Department of Neurology,University of Iowa College of Medicine, Iowa City, Iowa 52242.
however, on March 22, 1974, he experienced an abrupt onsetof severe headache, unsteadiness, numbness of the right sideof his face, difficulty swallowing, and loss of taste on theright side of the tongue. As he attempted to climb into bed,he fell to the floor with marked loss of balance, but noted nochange in level of consciousness. On March 23rd he was ad-mitted to a local hospital where his ataxia and headache in-creased gradually. On admission to University of IowaHospitals on March 28th, examination revealed an alert andwell-oriented man with a blood pressure of 140/80 mm Hg.The cranial nerve examination revealed absence of cornealreflex, and marked impairment of sensation to touch and pinprick along the entire distribution of the trigeminal nerve onthe right side. There was marked impaired sense of taste tosalt and sweet substances on the right side of the tongue. Thesalpingo-pharyngeus muscles moved less on the right, andthe tongue deviated to the right upon voluntary protrusion.His voice was nasal, although speech articulation was clear.There was no weakness or sensory impairment of the ex-tremities, and the deep tendon reflexes were normal. NoBabinski sign was present. There was severe disturbance onfinger-to-nose testing on the right and his gait was markedlyataxic with a tendency to fall to the right.
Hematological evaluation revealed a hematocrit of 47and white blood count of 9,100 with a normal differential.Sedimentation rate was 26 mm per hour and the urinalysiswas normal. Serum-extracted cholesterol was 222 mg/dland triglycerides were 230 mg/dl. The serum lipoproteinelectrophoresis showed mild elevation of the pre-albuminpattern. Tc" brain scan, x-rays of the skull, and computer-assisted tomography were normal. Audiometric evaluationwas also normal. On April 3rd transfemoral vertebral andcarotid angiography revealed a threadlike narrowing of theright vertebral artery for 1 cm, followed by completeobstruction at the atlanto-axial level (fig. I). The leftvertebral artery showed marked stenosis at the level of theforamen magnum, but the intracranial portion of the leftvertebral and basilar arteries appeared normal (figs. 2A andB). A short stem of the right vertebral artery wasdemonstrated. The large left posterior inferior cerebellarartery, bilateral anterior inferior cerebellar arteries,bilateral superior cerebellar arteries, and bilateral posterior
640 Stroke, Vol. 5, September-October 1974
by guest on May 11, 2018
http://stroke.ahajournals.org/D
ownloaded from

VERTEBRAL ARTERY OCCLUSION
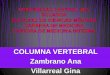
FIGMIl
Right lateral vertebral angiogram performed on thirteenth dayfollowing the onset of neurological symptoms. Threadlike narrow-ing and occlusion are shown at atlanlo-axial level. No intracranialcirculation is demonstrated.
cerebral arteries were well demonstrated. The carotidangiogram was normal. He was treated conservatively withdexamethasone and he showed slow but gradual improve-ment. Examination on May 1st revealed marked improve-ment of speech and swallowing difficulties, but the ataxicgait and loss of facial sensation persisted.
DiscussionThe vertebral artery has a characteristic anatomicalcourse through six foramina transversaria of the cer-vical vertebrae, passing through the groove on the sur-face of the arch of the atlas, and then penetrating twostrong membranes (atlanto-occipital membrane andcervical dura mater) before entering the cervical sub-arachnoid space. This artery is particularly susceptibleto injury or occlusion following cervical fracture dis-location,2 cervical traction,3 hyperextension,6 andhyperrotation.4'10 Three main sites of compressionassociated with fracture dislocation have beendescribed at the level of the fifth and sixth cervicalvertebrae, atlanto-axial joint, and atlanto-occipitaljoint.1 However, stenosis and/or occlusion of theartery with hyperextension and hyperrotationmovements without fracture dislocation are locatedprimarily at the atlanto-occipital joint, atlanto-axialjoint," and the foramen magnum." At the atlanto-axial joint the vertebral artery can be narrowed nor-mally or even occluded during normal head rotation tothe opposite side as shown by postmortemangiographical studies.12
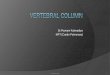
FIOURI 2
Left vertebral angiogram performed on thirteenth day following the onset of neurological symptoms. Theanteroposterior film shows the small distal end of the right vertebral artery. Both films show narrowing ofthe left vertebral artery at the foramen magnum level.
Slmkt, Vol. 5, Stpttmbtr-Octobw 1974 641
by guest on May 11, 2018
http://stroke.ahajournals.org/D
ownloaded from

OKAWARA, NIBBELINK
The vertebral artery is directly covered by m.obliquus capitis inferior and m. intertransversariusbetween the two foramina transversaria of the atlasand axis. The artery can be compressed by either ofthese two muscles between the atlas and axis duringrotatory movements as it ascends obliquely justmedial to the attachments of these muscles at theatlas.13 The artery then passes through a slit of thestrong atlanto-occipital membrane as it travelsmedially and ventrally in the groove of the atlas, andcan be compressed by the membrane between the atlasand occiput during hyperextension. The ischemic syn-drome of the brain stem or spinal cord can result fromone or more of the following conditions: (1) occlusionof both vertebral arteries, (2) occlusion of onevertebral artery with insufficient contralateral flow inthe opposite artery by way of one of its majorbranches or basilar artery, and (3) thrombosis, em-bolism or atresia of the posterior communicatingarteries or nearby collateral circulation. This ischemicsyndrome has been observed immediately followingabrupt hyperextension or excessive rotatory move-ment of the head without fracture or dislocation.4'e Inpostmortem findings, the presence of thrombus in thedistal vertebral-basilar system4' •• '•10' u suggests thatthe vertebral arteries can be sufficiently compromisedto initiate a propagating thrombus. The distalpropagation of a thrombus in an occluded vertebralartery has been well documented in patients withvertebral artery ligation for other reasons.16
In the patient described in this report, the move-ment of the head was neither forced nor powerful, butsufficiently long-lasting so that he had to maintain hishead in a hyperextended position, rotated to the left,and tilted to the right while painting the ceiling withhis left hand. This position apparently obstructed hisright vertebral artery at the atlanto-axial joint asdemonstrated by Tatlow,12 while the patient remainedwithout symptoms while the left vertebral artery couldsupply the right posterior inferior cerebellar artery.However, he occasionally used his right hand for ashort period and kept his head hyperextended, rotatedto the right, and tilted to the left. This maneuver ap-parently obstructed the blood flow in the left vertebralartery. The unsteadiness he experienced in the after-noon as he used his right hand could be interpreted asthe result of disturbed blood flow through the leftvertebral artery, since in all probability the rightvertebral artery was thrombosed. The thrombus hadnot yet propagated to the origin of the right posteriorinferior cerebellar artery at this point. At the end ofthe day he appeared to have an occluded rightvertebral artery at the atlantal level and a stenoticvertebral artery on the left. During the following 12hours, the thrombus in the right vertebral arterypropagated distally because of occlusion proximally.The obstructed blood flow to the right posterior in-ferior cerebellar artery produced the lateral medullarysyndrome the next morning. Propagation of the
642
thrombus could have been enhanced by such factors aslow oxygen saturation, structural changes, and a lackof effective collateral circulation as suggestedpreviously by Lindenberg.11
Although the significance of his dizziness in thepast is not clear, such symptoms should be regarded asa warning against sustained self-induced or externallyapplied hyperextension or rotation of the head in arelatively young patient.
AcknowledgmentsThe authors thank Mrs. B. Miller for her devoted assistance inpreparing this manuscript.
References1. Carpenter S: Injury of neck as cause of vertebral artery
thrombosis. J Neurosurg 18:849-853, 19612. Schneider RC, Schemm GW: Vertebral artery insufficiency in
acute and chronic spinal trauma, with special reference tothe syndrome of acute central cervical spinal cord injury. JNeurosurg 18:348-360, 1961
3. Suechting RL, French LA: Posterior inferior cerebellar arterysyndrome following a fracture of the cervical vertebrae. JNeurosurg 12:187-189, 1955
4. Ford FR, Clark D: Thrombosis of basilar artery withsoftenings in cerebellum and brain stem due to manipulatiorof the neck. Bull Johns Hopkins Hosp 98:37-42, 1956
5. Mehalic T, Farhat SM: Vertebral artery injury frorrchiropractic manipulation of the neck. Surg Neurol 2:125129, 1974
6. Pratt-Thomas HR, Berger KE: Cerebellar and spinal injurie;after chiropractic manipulation. JAMA 1 33:600-603, 1947
7. Schwartz GA, Geiger JK, Spano AV: Posterior inferioicerebellar artery syndrome of Wallenberg after chiropractiimanipulation. Arch Int Med 97:352-354, 1956
8. Nagler W: Vertebral artery obstruction by hyperextension othe neck: A report of three cases. Arch Phys Med Rehat54:237-240, 1973
9. Ford FR: Syncope, vertigo and disturbance of vision resultingfrom intermittent obstruction of the vertebral arteries due t(defect in the odontoid process and excessive mobility of thisecond cervical vertebra. Bull Johns Hopkins Hosp 91:168173, 1952
10. Holzer FJ: Verschluss der Wirbelsaulen Schlagader anKopfgelenk mit nachfolgender Thrombose durclSeitwartsdrehen des Kopfes. Dtsch Z Ges Gerichtl Me<44:422-426, 1955
11. Lindenberg R: Compression of brain arteries as pathogenetifactors for tissue necrosis and their areas of predilection.Neuropath Exp Neurol 14:223-243, 1955
12. Tatlow TWF, Bammer HG: Syndrome of vertebral artercompression. Neurology 7:331-340, 1957
13. Husini EA, Bell HS, Storer J: Mechanical obstruction of thvertebral arteries. JAMA 196:475-478, 1966
14. Krayenbiihl H: L'aspect angiographic de la thrombose dI'artere cerebellause posterieure et inferieure dans le syrdrome dit de Wallenberg. Neurochir 1:45-51, 1955
15. French LA, Haines GL: Unilateral vertebral artery ligatiorreport of a case ending fatally with thrombosis of the basilcartery. J Neurosurg 7:156-158, 1950
16. Simeone FA, Goldberg HI: Thrombosis of the vertebral arterfrom hyperextension injury to the neck. Case report.Neurosurg 29:540-544, 1968
Stroke, Vol. 5, September-October 197
by guest on May 11, 2018
http://stroke.ahajournals.org/D
ownloaded from

S. OKAWARA and D. NIBBELINKVertebral Artery Occlusion Following Hyperextension and Rotation of the Head
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1974 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.5.5.640
1974;5:640-642Stroke.
http://stroke.ahajournals.org/content/5/5/640World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 11, 2018
http://stroke.ahajournals.org/D
ownloaded from