Embed Size (px)
Citation preview
PROLONGED CEREBRAL ISCHEMIA/ATo/a/a 277
models of brain ischemia. Stroke 7: 14-17, 19769. Reivich M, Jehle J, Sokoloff L, Kety SK: Measurement of
regional cerebral blood flow with antipyrine - U C in awakecats. J Appl Physiol 27: 296-300, 1969
10. Hossmann K-A, Zimmermann V: Resuscitation of the monkeybrain after 1 hour complete ischemia. I. Physiological andmorphological observations. Brain Res 81: 59-74, 1974
11. Ponte J, Purves M: The role of the carotid body chemo-receptors and carotid sinus baroreceptors in the control ofcerebral blood vessels. J Physiol 237: 315-340, 1974
12. Ellis CH, Colville KI: Effect of current intensity on cardiovas-cular response to transcranial stimulation. Dis Nerv Sys 19:54-57, 1958
13. Lind B, Snyder J, Safar P: Total brain ischemia in dogs:Cerebral physiological and metabolic changes after 15 minutesof circulatory arrest. Resuscitation 4: 97-113, 1976
14. Weinberger LM, Gibbon MH, Gibbon JH Jr: Temporaryarrest of the circulation to the central venous system. ArchNeurol Psych 43: 615-634, 1940
15. Brockman SK, Jude JR: The tolerance of the dog brain to totalarrest of circulation. Bull Johns Hopkins Hosp 106: 74-80,
196016. Cantu RC, Ames A, DiGiacinto G, Dixon J: Hypotension: A
major factor limiting recovery from cerebral ischemia. J SurgRes 9: 525-529, 1969
17. Heymann C, Bouckert JJ, Jourdan F, Nowak SJG, Farber S:Survival and revival of nerve centers following acute anemia.Arch Neurol Psych 38: 304-309, 1937
18. Hossmann K-A, Sakaki S, Kimoto K: Cerebral uptake ofglucose and oxygen in the cat brain after prolonged ischemia.Stroke 7: 301-305, 1976
19. Hossmann, K-A, Sakaki S, Zimmermann V: Cation activitiesin reversible ischemia of the cat brain. Stroke 8: 77-81, 1976
20. Wolin LR, Massopust LC Jr, Taslitz N: Tolerance to arrest ofcerebral circulation in the rhesus monkey. Exp Neurol 30:103-115, 1971
21. Miller JR, Myers RE: Neurological effects of systemic circula-tory arrest in the monkey. Neurology (Minneap) 20: 715-724,1970
22. Safar P, Stezoski W, Nemoto EM: Amelioration of braindamage after 12 minutes cardiac arrest in dogs. Arch Neurol33: 91-95, 1976
Occlusion of the Vertebral or Basilar Artery
Follow Up Analysis of Some Patients with Benign Outcome
Louis R. CAPLAN, M.D.
SUMMARY Ten patients with angiographically verified occlusion of the basilar or vertebral artery havebeen followed for an average of 2.75 years. None has developed further ischemia after the initial stroke, and 4patients survived without any clinical deficit. In occlusive disease of the posterior circulation, the critical periodfor deficit acquisition is at the time of occlusion. Extent of the deficit depends on the rapidity of development ofadequate collateral circulation, and the presence of distal embolization at the time of occlusion. Some patientssurvive basilar occlusion without permanent deficit.
Stroke Vol 10, No 3, 1979
OCCLUSION of the basilar artery is generally con-sidered a very serious event incompatible with normalsurvival. Kubik and Adams1 described 18 patientswith brainstem infarction due to occlusion of thebasilar artery discovered at postmortem examinationand emphasized the abrupt onset and frequent fataloutcome. Marshall2 subsequently pointed out thatmany untreated patients with the clinical picture ofposterior circulation vascular disease do not developserious deficits; however, the underlying vascularpathology in this group of clinical patients was un-known. Occlusion of the vertebral artery, the mostfrequent cause of lateral medullary infarction iden-tified at postmortem examination,3 has usually beenassociated with a relatively benign clinical course.4 In-frequent studies have attempted to correlate theseverity of the neurological deficit with angio-graphically verified vascular pathology in the posterior
From the Department of Neurology, Beth Israel Hospital andHarvard Medical School, Boston, MA.
Reprints: Louis R. Caplan, M.D., Chairman, Department ofNeurology, Michael Reese Hospital, 29th St. and Ellis, Chicago, IL60616.
circulation.46 No reference could be found on followup of patients with angiographically documentedvertebrobasilar occlusive disease.
The author's files, and those of the Harvard StrokeRegistry,7 were searched for patients meeting thefollowing criteria: 1) patients who were examined andfollowed carefully by the author during hospitaliza-tion for acute stroke; 2) technically satisfactoryangiograms taken during the stroke whichdocumented an occlusion of either a vertebral or thebasilar artery; 3) patients who survived the acutestroke and had been followed by the author more than6 months. The temporal profile of illness and clinicaloutcome in this group of patients gave insights into thepathogenesis of the clinical deficit and mechanisms ofcompensation.
Results
Case Material
Ten patients (8 male, 2 female) from 26-71 years ofage (average 52.2 years) were studied clinically andangiographically. Six had occlusion of the basilarartery (2 proximal and 4 midportion beyond the
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from
278 STROKE VOL 10, No 3, MAY-JUNE 1979
AICA branching). Four had an occluded vertebralartery. All basilar occlusion cases had collateral cir-culation involving the long circumferential cerebellarvessels (PICA, AICA, SCA) with late filling of thedistal segment of the basilar artery. Patients with ver-tebral occlusion had a patent contralateral vertebralartery and basilar artery. Six patients had transientischemic attacks (TIAs) prior to strokes. The timebetween the initial TIA and the stroke ranged from 1week to 1 year (average 15 weeks). The last TIAalways occurred within 1 month of the stroke (5 or 6within 1 week). TIAs were usually multiple (range1-30, average 11).
After onset of stroke, 8 patients had either progres-sion of the deficit over a 2 or 3 day period, or had fluc-tuations of their clinical deficit during the first 2
weeks. In 4 of these 8 patients the clinical deficit fluc-tuated with alteration of position in bed (3 whenelevated, 1 when turned to the left side). Two patientsleft the hospital without neurological abnormalities, 3had slight deficits, 4 moderate and 1 severe.
Follow up ranged from Vi to 6 years (average 2.75years). No patient developed a late increase in deficitreferable to the posterior circulation, and in 6 patientsclinical deficits improved during the period of followup. Two patients with a slight deficit upon hospital dis-charge subsequently returned to normal. Six patientshave been treated with long-term warfarin; 2 patientshad temporary anticoagulant treatment (1 heparin for2 weeks, 1 warfarin for 6 months). No patient has hada new stroke, but 1 patient died of a myocardial in-farction 4 years after his pontine infarction.
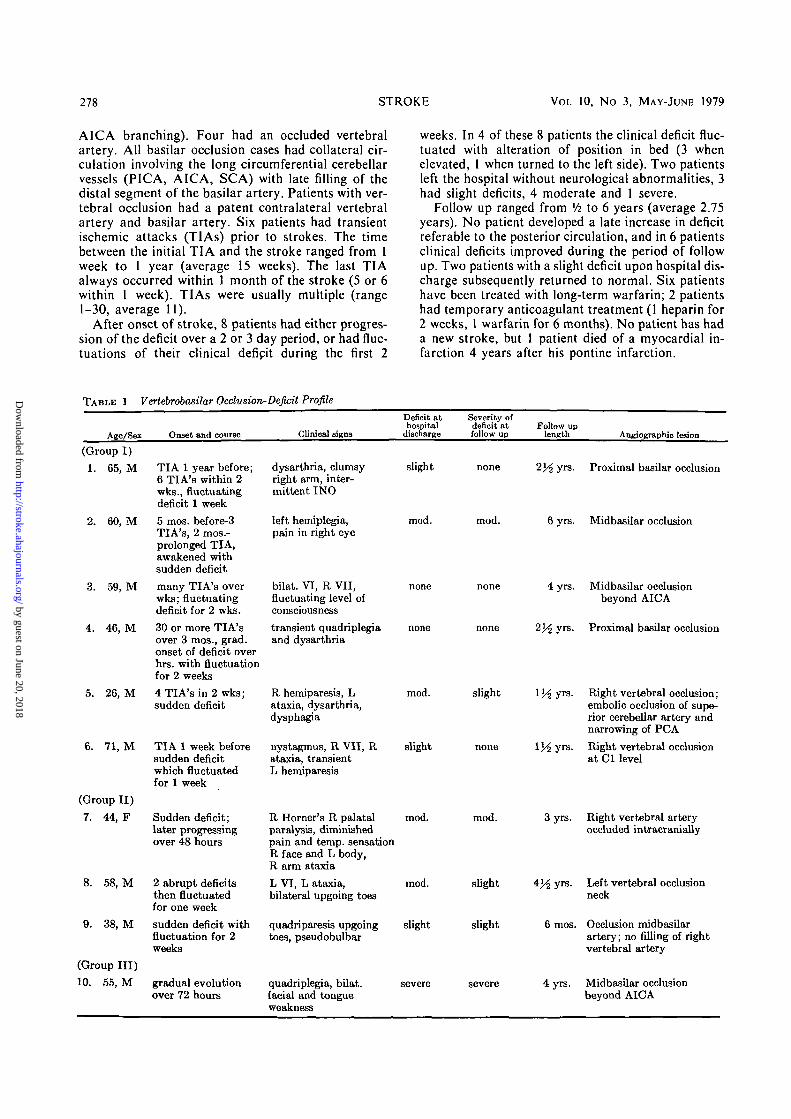
TABLE 1 Vertebrobasilar Occlusion-Deficit Profile
Age/Sex Onset and course Clinical signs
Deficit athospital
discharge
Severity ofdeficit atfollow up
Follow uplength Angiographic lesion
(Group I)1.
2.
3.
4.
5.
6.
65, M
60, M
59, M
46, M
26, M
71, M
(Group II)
7.
8.
9.
44, F
58, M
38, M
(Group III)
10. 55, M
TIA 1 year before;6 TIA's within 2wks., fluctuatingdeficit 1 week
5 mos. before-3TIA's, 2 mos.-prolonged TIA,awakened withsudden deficit
many TIA's overwks; fluctuatingdeficit for 2 wks.
30 or more TIA'sover 3 mos., grad.onset of deficit overhrs. with fluctuationfor 2 weeks
4 TIA's in 2 wks;sudden deficit
TIA 1 week beforesudden deficitwhich fluctuatedfor 1 week
Sudden deficit;later progressingover 48 hours
2 abrupt deficitsthen fluctuatedfor one week
sudden deficit withfluctuation for 2weeks
gradual evolutionover 72 hours
dysarthna, clumsyright arm, inter-mittent INO
left hemiplegia,pain in right eye
bilat. VI, R VII,fluctuating level ofconsciousness
transient quadriplegiaand dysarthria
R hemiparesis, Lataxia, dysarthria,dysphagia
nystagmus, R VII, Rataxia, transientL hemiparesis
R Homer's R palatalparalysis, diminishedpain and temp, sensationR face and L body,R arm ataxia
L VI, L ataxia,bilateral upgoing toes
quadriparesis upgoingtoes, pseudobulbar
quadriplegia, bilat.facial and tongueweakness
slight
mod.
none
none
mod.
slight
mod.
mod.
slight
severe
none
mod.
none
none
slight
none
mod.
slight
slight
severe
2^yr s .
6yrs.
4 yrs.
2}/2 yrs.
l ^ y r s .
l ^ y r s .
3 yrs.
4 ^ yrs.
6 mos.
4 yrs.
Proximal basilar occlusion
Midbasilar occlusion
Midbasilar occlusionbeyond AICA
Proximal basilar occlusion
Right vertebral occlusion;embolic occlusion of supe-rior cerebellar artery andnarrowing of PCA
Right vertebral occlusionat Cl level
Right vertebral arteryoccluded intracranially
Left vertebral occlusionneck
Occlusion midbasilarartery; no filling of rightvertebral artery
Midbasilar occlusionbeyond AICA
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from
VERTEBRAL, BASILAR OCCLUSION/Cap/an 279
The patients fitted into 3 different patterns of onsetand course (table). 1) The majority (6) (patients 1-6)had TIAs prior to stroke. The TIAs were usually mul-tiple and increased in frequency as the stroke ap-proached, with 5 of 6 patients having a TIA within aweek of the stroke. The stroke usually began in themorning on rising, and symptoms and signs ofbrainstem, cerebellar and posterior cerebral arteryterritory dysfunction fluctuated for a period rangingbetween 2 days and 3 weeks. Clinical fluctuations werevery sensitive to postural change. After a period of 2-3weeks, the clinical deficit stabilized and no furtherdeterioration occurred. 2) A second group of 3patients (patients 7-9) had sudden onset deficits withonly minor subsequent fluctuations over a period of2-3 days. All had unilateral vertebral occlusionsangiographically. 3) One patient (No. 10) had aprogressive course over 3 days without TIAs orsudden onset.
Illustrative Cases
1. Patient 4
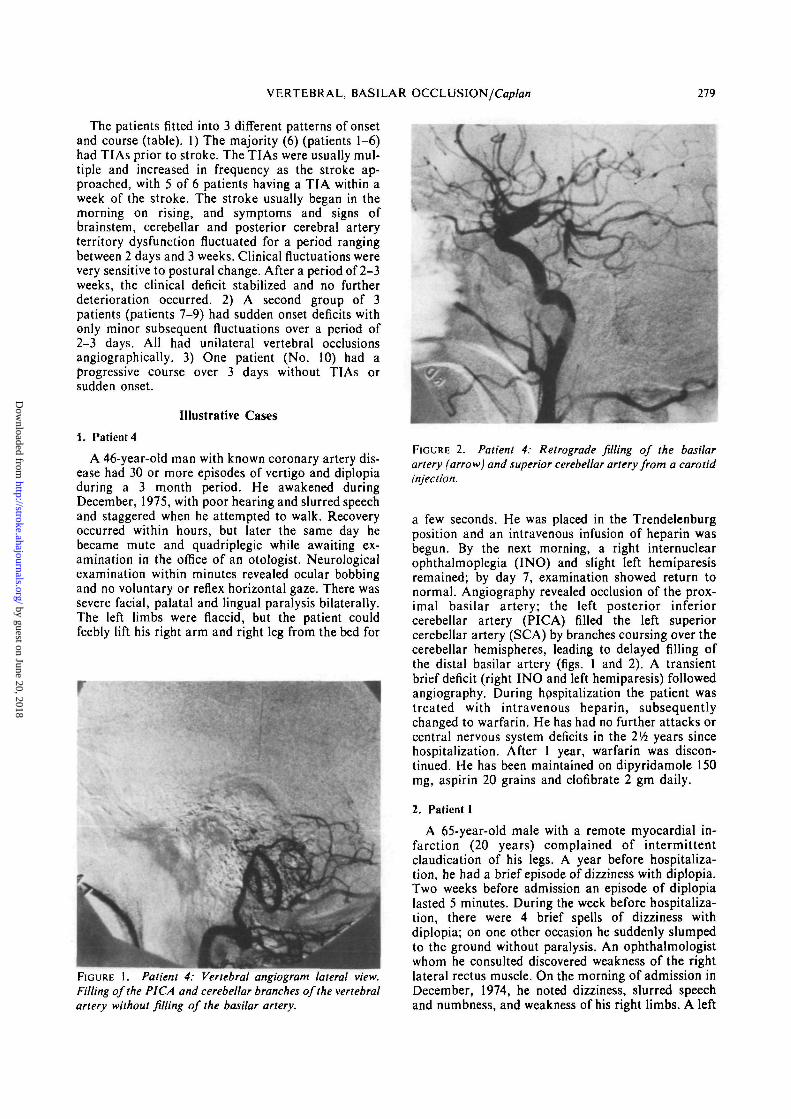
A 46-year-old man with known coronary artery dis-ease had 30 or more episodes of vertigo and diplopiaduring a 3 month period. He awakened duringDecember, 1975, with poor hearing and slurred speechand staggered when he attempted to walk. Recoveryoccurred within hours, but later the same day hebecame mute and quadriplegic while awaiting ex-amination in the office of an otologist. Neurologicalexamination within minutes revealed ocular bobbingand no voluntary or reflex horizontal gaze. There wassevere facial, palatal and lingual paralysis bilaterally.The left limbs were flaccid, but the patient couldfeebly lift his right arm and right leg from the bed for
FIGURE I. Patient 4: Vertebral angiogram lateral view.Filling of the PICA and cerebellar branches of the vertebralartery without filling of the basilar artery.
FIGURE 2. Patient 4: Retrograde filling of the basilarartery (arrow) and superior cerebellar artery from a carotidinjection.
a few seconds. He was placed in the Trendelenburgposition and an intravenous infusion of heparin wasbegun. By the next morning, a right internuclearophthalmoplegia (INO) and slight left hemiparesisremained; by day 7, examination showed return tonormal. Angiography revealed occlusion of the prox-imal basilar artery; the left posterior inferiorcerebellar artery (PICA) filled the left superiorcerebellar artery (SCA) by branches coursing over thecerebellar hemispheres, leading to delayed filling ofthe distal basilar artery (figs. 1 and 2). A transientbrief deficit (right INO and left hemiparesis) followedangiography. During hpspitalization the patient wastreated with intravenous heparin, subsequentlychanged to warfarin. He has had no further attacks orcentral nervous system deficits in the 2Vi years sincehospitalization. After 1 year, warfarin was discon-tinued. He has been maintained on dipyridamole 150mg, aspirin 20 grains and clofibrate 2 gm daily.
2. Patient 1
A 65-year-old male with a remote myocardial in-farction (20 years) complained of intermittentclaudication of his legs. A year before hospitaliza-tion, he had a brief episode of dizziness with diplopia.Two weeks before admission an episode of diplopialasted 5 minutes. During the week before hospitaliza-tion, there were 4 brief spells of dizziness withdiplopia; on one other occasion he suddenly slumpedto the ground without paralysis. An ophthalmologistwhom he consulted discovered weakness of the rightlateral rectus muscle. On the morning of admission inDecember, 1974, he noted dizziness, slurred speechand numbness, and weakness of his right limbs. A left
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from
380 STROKE VOL 10, No 3, MAY-JUNE 1979
Horner's syndrome, left horizontal rotatorynystagmus, and right limb ataxia were present on ex-amination. During the initial 3 weeks of hospitaliza-tion there was considerable fluctuation of his symp-toms and signs, often after elevation of his head. Onday 5, transfemoral vertebral angiography demon-strated complete occlusion of the proximal basilarartery with reflux from the left vertebfal artery fillingthe right vertebral. Both PICAs were opacified. Treat-ment with intravenous heparin had been institutedshortly after hospitalization, but had to be stopped onday 14 when a large retroperitoneal hemorrhagedeveloped. Upon hospital discharge at 4 weeks, thepatient's only residual neurological deficit was slightinstability of gait. He has had no transient episodes orstrokes during the 7>Vi years since hospitalization andhas been able to return to work in a restaurant. He hasbeen maintained on aspirin 15 grains daily.
3. Patient 5
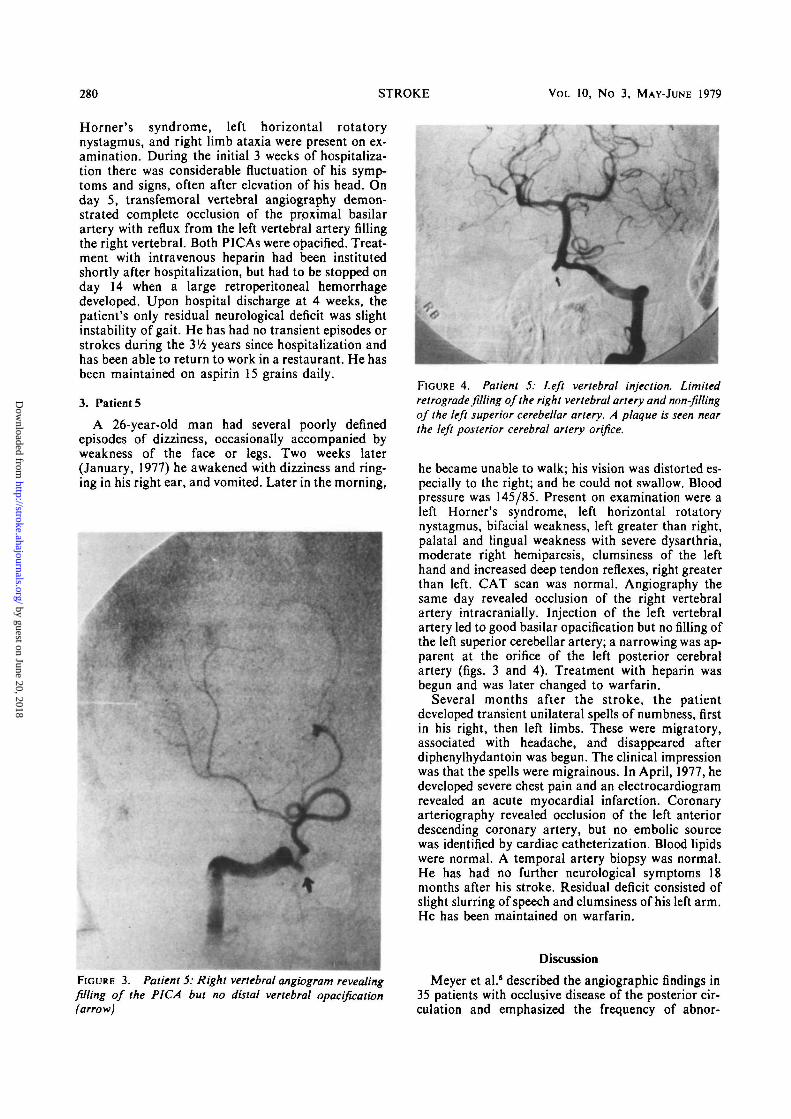
A 26-year-old man had several poorly definedepisodes of dizziness, occasionally accompanied byweakness of the face or legs. Two weeks later(January, 1977) he awakened with dizziness and ring-ing in his right ear, and vomited. Later in the morning,
FIGURE 3. Patient 5: Right vertebral angiogram revealingfilling of the PICA but no distal vertebral opacification(arrow)
FIGURE 4. Patient 5: Left vertebral injection. Limitedretrograde filling of the right vertebral artery and non-fillingof the left superior cerebellar artery. A plaque is seen nearthe left posterior cerebral artery orifice.
he became unable to walk; his vision was distorted es-pecially to the right; and he could not swallow. Bloodpressure was 145/85. Present on examination were aleft Horner's syndrome, left horizontal rotatorynystagmus, bifacial weakness, left greater than right,palatal and lingual weakness with severe dysarthria,moderate right hemiparesis, clumsiness of the lefthand and increased deep tendon reflexes, right greaterthan left. CAT scan was normal. Angiography thesame day revealed occlusion of the right vertebralartery intracranially. Injection of the left vertebralartery led to good basilar opacification but no filling ofthe left superior cerebellar artery; a narrowing was ap-parent at the orifice of the left posterior cerebralartery (figs. 3 and 4). Treatment with heparin wasbegun and was later changed to warfarin.
Several months after the stroke, the patientdeveloped transient unilateral spells of numbness, firstin his right, then left limbs. These were migratory,associated with headache, and disappeared afterdiphenylhydantoin was begun. The clinical impressionwas that the spells were migrainous. In April, 1977, hedeveloped severe chest pain and an electrocardiogramrevealed an acute myocardial infarction. Coronaryarteriography revealed occlusion of the left anteriordescending coronary artery, but no embolic sourcewas identified by cardiac catheterization. Blood lipidswere normal. A temporal artery biopsy was normal.He has had no further neurological symptoms 18months after his stroke. Residual deficit consisted ofslight slurring of speech and clumsiness of his left arm.He has been maintained on warfarin.
Discussion
Meyer et al.5 described the angiographic findings in35 patients with occlusive disease of the posterior cir-culation and emphasized the frequency of abnor-
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

VERTEBRAL, BASILAR OCCLUSION/Cap/an 281
malities in the basilar artery itself. Clinical course andfollow up data were not included in the report, whichexcluded "critically ill patients" or those with severebrainstem infarction. Nonetheless, angiography in 2patients revealed clinically unsuspected completeocclusion of the basilar artery. Archer andHorenstein6 discussed the angiographic findings in 20patients with basilar occlusion. Their clinical groupconsisted of patients with severe clinical deficits incontrast to Meyer's criteria for selection.3 Fifteen ofArcher and Horenstein's patients were stuporous orcomatose at the time of angiography and 2 were"locked-in"; 15 patients died, 4 were severely disabledand 1 patient had a moderately severe deficit(hemiparesis). These authors defined the locus ofocclusion and the pathways of collateral circulationand sought to correlate the anatomy of the clinicaldeficit with angiographic findings. Caplan and Rosen-baum4 pointed out the utility of vertebrobasilarangiography in differentiating severe obstructive dis-ease of the vertebral or basilar artery from "smallvessel" disease within the posterior circulation, andemphasized the frequent benign outcome of manypatients with clinical vertebrobasilar symptoms whohad no major vascular lesions seen angiographically.Caplan and Rosenbaum also pointed out that patientswith known basilar occlusion may survive without dis-abling neurological sequelae. The present report seeksto extend and explain that finding.
The initial period of TIAs, in group 1 patients,likely represents diminished flow referable to vascularstenosis. When occlusion of the vertebral or basilarartery becomes complete, a hemodynamically un-stable situation develops in which collateral circula-tion must develop quickly or there will occur irreversi-ble ischemia of brainstem, cerebellum, or posteriorcerebral territory hemispheral tissue. During thisperiod of development of collateral circulation (1-21days), hemodynamic changes (arrhythmia, bleeding,or hypotension) and alteration of position may becritical.8'9 The slight changes in cerebral blood flowwhich occur on sitting may be enough in these patientswith marginal vascular compensation to produceclinical ischemia. Positional ischemia has been limitedto patients with basilar or bilateral vertebral occlusionand has not been seen in patients with unilateralvertebral occlusion, presumably because of an ade-quate contralateral vertebral supply. As thrombosisoccurs, embolization distally within the vertebro-basilar system may lead to sudden posterior circula-tion clinical deficit. Embolization distally is thepresumed mechanism of presentation in our group 2patients with sudden onset deficits, and in patient 5with a sudden deficit following TIAs in whom nonfill-ing of the left superior cerebellar artery (a clinicallyaffected vascular territory) favored an embolicmechanism. Embolization in the posterior circulationhas been documented on postmortem examination byothers.10 Meyer et al.6 and Sundt, Whisnant et al.9
have also emphasized the role of emboli arising fromproximal vertebrobasilar occlusion. After a period ofseveral weeks, a stable collateral circulation develops
(sometimes after death of cerebral tissue, i.e., stroke)which is generally resistant to further hemodynamiccrises. In addition, stabilization of the clot (days toweeks) is usually associated with a cessation of lateemboli arising from the region of thrombosis.
In some patients, e.g., group 3 (patient 10) throm-bosis may produce a progressive clinical course overdays without preceding TIAs. In our experience, inpatients with progressing stroke due to lacunar infarc-tion or internal carotid artery occlusion, the prognosisis poorer than for those patients with TIAs or fluctuat-ing course. The recovery phase of a TIA or fluctuat-ing thrombotic stroke may be due, at least partially, tothe presence of adequate collateral circulation.Progressing stroke may indicate poor collateral poten-tial, and so a worse prognosis. The single patient ingroup 3 in this report had the most severe deficit ofany of our 10 patients.
Jones, Millikan and Sandok11 described the tem-poral profile of 37 patients with a clinical diagnosis ofvertebrobasilar system infarction. None of thepatients had angiographic definition of the underlyingvascular pathology, but all 10 patients who died hadocclusion of a vertebral or basilar artery at post-mortem examination. Twenty-two of their 37 patientshad reached maximum deficit within 24 hours, andsome other patients progressed over a period of 4days. No patient had progression of signs after 1week, and there were no known late exacerbations.
Since little data exist concerning the clinical tempoof angiographically verified vertebrobasilar occlusion,it will be useful to compare the clinical course of ourpatients with that of patients with known occlusion ofthe internal carotid artery (a vessel of comparable sizeand length). Fourteen patients, personally examined,with angiographically documented occlusion of the in-ternal carotid artery were followed an average of 3years. Eight had TIAs, 2 sudden onset deficits, and 4gradually progressive onset over days. Fluctuations ofclinical deficit occurred during the first 2 weeks but thepatients remained stable thereafter irrespective oftreatment (8 untreated). Two of these patients had late(greater than 1 year post-stroke) episodes ofamaurosis fugax; each, in addition to the carotidocclusion, had severe stenosis of the ipsilateral exter-nal carotid artery and 1 had, in addition, stenosis c{the ophthalmic artery. No patient developed a latepermanent or transient central nervous system deficiton the side of prior carotid occlusion. Barnett andAldis12 specifically studied the question of delayedcerebral ischemia distal to occlusion of a majorcerebral artery. Of 426 patients, there were only 12 oc-currences of subsequent events, 4 within the first 2weeks (1.9% late occurrence). Of the late occurrences3 were amaurosis fugax alone, 6 were cerebral aloneand 3 were amaurosis fugax and cerebral. One patienthad common carotid stenosis ipsilateral to an internalcarotid artery occlusion but episodes ceased aftercomplete common carotid artery occlusion. In 3patients documented hemodynamic changes occurred(2 postural hypotension and 1 ventricular arrhythmia).Barnett13 subsequently reported that 25 of 235 patients
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

282 STROKE VOL 10, No 3, MAY-JUNE 1979
enrolled in a cooperative study of antiplatelet aggrega-tion drugs had cerebral ischemia subsequent to knownocclusion. One of these patients had a basilar arteryocclusion, and another a bilateral vertebral arteryocclusion in the neck. Barnett and Aldis12 andBarnett13 expressed the belief that late episodesrepresented embolic material breaking off from thetop of the prior occlusion, or, more commonly, em-bolization from diseased external or common carotidcollateral supply. In other series of patients withcarotid occlusion reported in the literature lateepisodes occasionally occurred but insufficient detailswere given regarding the nature and locus of the lateischemia.
The patient population reported herein represents aselected group of patients with vertebrobasilar disease— all were angiographically studied with documentedocclusion of the vertebral or basilar arteries and allsurvived long enough for follow up. During the sameperiod, 5 patients with angiographically documenteddisease died, and 10 patients with severe brainstem in-farction died without angiography. In addition, ourpatients' course does not represent the natural courseof illness since 8 patients have received temporary orlong term anticoagulation. Nevertheless, 2 conclu-sions seem warranted from our clinical material:
1) Some patients with occlusion of the basilarartery survive with little or no deficit.
2) In occlusive disease of the posterior circulation,just as is true in patients with occlusion of the internalcarotid artery, the critical period for acquisition of acentral nervous system deficit is at the time of occlu-sion. The degree of deficit depends primarily on thedevelopment of adequate collateral circulation and thepresence of distal embolization at the time of occlu-sion.
Our data suggest that in the group of patients withdocumented occlusion of the basilar artery a period ofbedrest in the supine position, with maintenance ofsystemic blood pressure, is important. Occlusion of avertebral artery, in the presence of a patent con-tralateral vertebral artery, usually is associated with anonprogressive clinical course unless distal emboliza-tion occurs in the weeks after occlusion. Short term
(weeks or a few months) anticoagulation may behypothetically useful in preventing embolization oracute extension of the clot. A clinical trial of conserva-tive medical therapy with short term anticoagulationor agents which decrease platelet agglutination (e.g.,aspirin, dipyridamole, or sulfinpyrazone) seemsworthy of consideration as opposed to the presentpractice in many centers of long term warfarintherapy. Intracranial bypass grafts (e.g., occipital toPICA shunts) might be reserved for those unusualpatients with documented extensive stenosis of majorvertebral or basilar vessels with repeated episodes ofischemia unresponsive to conservative treatment.
References
1. Kubik CS, Adams RD: Occlusion of the basilar artery — aclinical and pathological study. Brain 69: 73-121, 1946
2. Marshall J: The natural history of transient ischemic cerebro-vascular attacks. Quart J Med 33: 309-324, 1964
3. Fisher CM, Karnes W, Kubik C: Lateral medullary infarction,the pattern of vascular occlusion. J Neuropathol Exp Neurol20: 323-379, 1961
4. Caplan L, Rosenbaum A: Role of cerebral angiography invertebrobasilar occlusive disease. J Neurol NeurosurgPsychiatry 38: 601-612, 1975
5. Meyer JS, Sheehan S, Bauer R: An arteriographic study ofcerebrovascular disease in man. 1. Stenosis and occlusion of thevertebrobasilar arterial system. Arch Neurol 2: 27-45, 1960
6. Archer C, Horenstein S: Basilar artery occlusion; clinical andradiological correlation. Stroke 8: 383-390, 1977
7. Mohr J, Caplan L, Melski J, et al: The Harvard CooperativeStroke Registry: A prospective registry, Neurology (Minneap)28: 754-762, 1978
8. Caplan L, Sergay S: Positional cerebral ischemia. J NeurolNeurosurg Psychiatry 39: 385-391, 1976
9. Sundt T, Whisnant J, Piepgras D, Campbell J, Holman C: In-tracranial bypass grafts for vertebrobasilar ischemia. MayoClin Proc 53: 12-18, 1978
10. Castaigne P, Lhermitte F, Gautier JC, et al: Arterial occlusionin vertebrobasilar system: A study of 44 patients with post-mortem data. Brain 96: 133-154, 1973
11. Jones HR, Millikan CH, Sandok B: Temporal profile of acutevertebrobasilar system infarction. Stroke 9: 109, 1978 (abs)
12. Barnett HJM, Aldis E: Delayed cerebral ischemic episodes dis-tal to occlusion of major cerebral arteries. Neurology(Minneap) 25: 370, 1975
13. Barnett HJM: Delayed cerebral ischemic episodes distal toocclusion of major cerebral arteries. Neurology (Minneap) 28:769-774, 1978
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from

L R Caplanoutcome.
Occlusion of the vertebral or basilar artery. Follow up analysis of some patients with benign
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1979 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.10.3.277
1979;10:277-282Stroke.
http://stroke.ahajournals.org/content/10/3/277World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 20, 2018http://stroke.ahajournals.org/
Dow
nloaded from