Embed Size (px)
Citation preview

Despite our increasing knowledge of the neuropsychopathology of drug use and addiction, drug-specific treatments for dif-ferent abuse scenarios (for example, reversal of drug overdose, cessation of drug use and relapse prevention) are still lacking. Among the traditional pharmacotherapies, small-molecule drug mimetics endeavour to displace drug molecules from neuronal sites, whereas anti-addiction medications modulate monoamine or opioid signal-ling. Consequently, either treatment may be inherently addictive. One contemporary and medically viable alternative, immuno-pharmacotherapy, does not produce these unwanted neurological effects or cognitive impairment, and this is particularly relevant to the patient who abstains from drug use1. Instead, drug-specific antibodies terminate a drug-induced ‘high’ by sequestering drug molecules outside the central nervous sys-tem. Before their clinical use, prospective active and passive vaccine candidates will require improvements in their immuno-genicity and validation of their medical applicability, respectively. This Perspective highlights scientific approaches that are cur-rently underway to advance drug-targeting vaccines through the pharmaceutical pipe-line, as well as the ethical complications that may arise with their implementation into programmes for treating drug addiction.
Tailoring antibodies for successImmunopharmacotherapy offers a flexible platform for optimizing the anti-drug treat-ment strategy for the specific indication. Although active vaccination of the patient may confer long-term protection against addictive behaviours, the same vaccine may
also be applied to the large-scale pharmaceu-tical development of drug-specific antibodies. These antibody-based passive vaccines permit the treatment of time-sensitive drug use scenarios, such as rapid detoxification (FIG. 1).
Initial barriers to the clinical implement-ation of passive vaccines included the challenge of manufacturing human or humanized monoclonal antibodies in suf-ficient quantities, the immunogenicity of non-human monoclonal antibodies and uncertainties regarding their medically safe use. However, with the advent of transgenic mice and phage-display technology came the ability to engage in high-throughput screening and large-scale production of monoclonal antibodies. As a result, by 2008, seven human monoclonal antibodies had received US Food and Drug Administration (FDA) approval in the United States, three were under FDA review, seven were in late-stage development and eighty-one were in early-stage development2. Furthermore, the number of human monoclonal antibodies in clinical trials continues to grow, which illustrates the expansion of this class of therapeutics to the treatment of many differ-ent indications. With respect to drug abuse, high-affinity monoclonal antibodies have been developed against cocaine, nicotine, amphetamines, phencyclidine (PCP), opiates (for example, heroin and morphine) and benzodiazepines; these monoclonal anti-bodies have demonstrated preclinical efficacy as antidotes for drug overdose, as prophyl-actic therapies for attenuating drug effects and as addiction cessation medications3–21.
Given the mixed clinical efficacy of active vaccines in blunting addictive behaviours, the aforementioned advantages of passive
vaccines endorse their continued refinement in anticipation of clinical study. Supporting this pursuit, antibody engineering has evolved into its own field that focuses on tailoring antibodies for in vivo targets. Through large-scale screening of antibody libraries or polyclonal sera for antibodies with higher antigen-binding affinity and improved specificity, superior clones are rapidly identified out of a large ‘chemical-binding space’ and used as starting templates for rounds of in vitro affinity maturation, molecular evolution and site-directed mutagenesis. These techniques permit the high-throughput refinement of antibody size, isoelectric point (pI), Fc region and variable-domain sequences, such that the optimal pharmacodynamic and pharmaco-kinetic (PD/PK) properties for a specific drug abuse indication may be achieved in a single monoclonal antibody (TABLE 1).
As a representative example, the cocaine-specific monoclonal antibodies GNC92H2 (Kd = 2 nM; by kinetic exclusion assay22), GNCgzk (Kd = 0.18 nM; K.D.J. and J.B.T., unpublished observations) and 2E2 (Kd = 4 nM23) possess optimal binding kinetics; further refinement of their antigen-binding sites is not anticipated to substantially improve their ability to sequester cocaine in vivo. However, truncation of their IgG scaffold to generate smaller drug-binding fragments aligns their PD/PK profile with the time constraints placed on cocaine scavenging during overdose12,17,20,21,24. It follows that preclinical tests comparing the GNC92H2 IgG format with the monomeric antigen-binding fragment (Fab), the dimeric antigen-binding fragment (F(ab’)2) and the single-chain variable domain (scFv) con-firmed the superior therapeutic capability of the Fab format to prevent cocaine-induced lethality (TABLE 1). This finding is corrobo-rated by similar studies on the benefits of using smaller antibody formats as immuno-therapeutic antidotes for exogenous toxins, other abused drugs and prescription medications25–27.
A key tenet of pharmacology states that the free drug concentration in serum drives the biodistribution of the drug between blood and tissue. Before passive immuniza-tion, the serum drug concentration shows approximately equal distribution between protein-bound and unbound states28,29. Following the administration of a mole-equivalent dose of a drug-specific IgG or drug-specific Fab, serum drug levels spike 10- to 100-fold above control levels. In gen-eral, an antibody-mediated increase in drug concentration in serum correlates inversely
S C I E N C E A N D S O C I E T Y
Vaccines targeting drugs of abuse: is the glass half-empty or half-full?Kim D. Janda and Jennifer B. Treweek
Abstract | The advent of vaccines targeting drugs of abuse heralded a fundamentally different approach to treating substance-related disorders. In contrast to traditional pharmacotherapies for drug abuse, vaccines act by sequestering circulating drugs and terminating the drug-induced ‘high’ without inducing unwanted neuromodulatory effects. Drug-targeting vaccines have entered clinical evaluation, and although these vaccines show promise from a biomedical viewpoint, the ethical and socioeconomic implications of vaccinating patients against drugs of abuse merit discussion within the scientific community.
P E R S P E C T I V E S
NATURE REVIEWS | IMMUNOLOGY VOLUME 12 | JANUARY 2012 | 67
© 2012 Macmillan Publishers Limited. All rights reserved

Nature Reviews | Immunology
Passive vaccineBrain
Blood–brain barrier
Active vaccine
Patient receives antibodies specific for drug
Drug activates reward circuitry in brain
Drug
Patient is vaccinated to induce an endogenous immune response against the drug
Blood
Vaccine promotes diffusion of drug from brain to blood and blunts the drug’s rewarding effects
Antibody prevents drug from entering brain
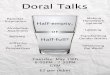
Figure 1 | Active and passive drug vaccines. Immunopharmacotherapy encompasses both active immunization with drug-specific vaccines and the passive transfer of preformed antibodies. The therapeutic efficacy of either vaccination approach hinges on its capacity to confer sufficient antibody titres to neutralize an administered drug dose and terminate the drug-induced ‘high’. Specifically, the drug-binding or drug-degrading antibodies should sequester all drug molecules in the peripheral circulation, thereby reversing the drug concentration gradient across the blood–brain barrier to favour drug efflux from the central nervous system.
with the extent of biodistribution of the administered antibody or antibody deriva-tive. The biodistribution of an antibody or antibody derivative is related to its size, such that the biodistributions of the common formats are in the following order: scFv > Fab > F(ab’)2 > IgG29–31. However, contrary to expectations, all mono clonal antibody formats appear to cause dramatic shifts in serum and tissue drug concentrations, with nearly 100% of serum drug entering the protein-bound state24,29,32. Although this antibody-mediated change in drug distribution lacks a pharmacological expla-nation, the beneficial therapeutic effect of treatment is readily observable. For example, the PCP-binding Fab caused the greatest increase in PCP serum concentra-tion and renal elimination relative to other monoclonal antibody formats, thereby resulting in the most significant attenuation of acute PCP toxicity21,24,28.
A final barrier to the translation of immuno therapeutic monoclonal antibodies to the clinic has been the perception that antibody-mediated targeting of small molecules required an equivalent molar ratio between the antibody binding capacity and the drug dose33. This has been refuted for PCP and cocaine, as submolar antibody doses effectively antagonize these drugs20,21. Also, because the effector functions conferred by the Fc region are superfluous to drug detox-ification, conversion of the IgG molecule to a smaller format permits an equivalent molar dose of the immunotherapeutic to be administered at a reduced infusion volume and protein load25,34,35.
Determinants for a viable vaccineThe adaptability of antibody-based agents to specific scenarios of abuse through the refinement of their PD/PK profiles makes them promising clinical candidates for niche
indications. However, the treatment of addic-tive behaviours and relapse requires long-term protection, for which frequent monoclonal antibody injections would prove expensive and inefficient. Active vaccination not only confers prolonged immunoresponsiveness to a drug target, but also provides a continuously high level of circulating drug-specific antibodies if the patient receives booster vaccinations at yearly or even longer intervals.
The mixed clinical efficacies of immuno-therapies for nicotine and cocaine abuse has precipitated a renewed interest in the more subtle and often underappreciated aspects of vaccine design5,6,36,37. Three vaccine components are subject to optimization: the hapten, the carrier protein and the adjuvant. Traditionally, research has focused on the chemical identity of the drug-like hapten and, by extension, its site of attachment to the carrier moiety. Whereas effective hapten presentation has a direct influence on the drug-binding affinity and specificity of the elicited antibodies, the primary importance of adjuvants as immune potentiators was not fully appreciated until recent decades, despite their inclusion in vaccine formulations for over a century38. Since realizing that the adjuvant biases the type and potency of the immune response to phenotypically distinct subpopulations of CD4+ T cells, scientists have channelled more effort into the development of novel adjuvants and the elucidation of their mechanisms of action39,40. Likewise, the carrier protein, whose former role was that of a hap-ten vehicle, came under scrutiny as a second inroad to customizing the immuno genicity, stability and distribution of the injected vaccine. A well-designed carrier protein will accurately display the immunogenic epitope of the hapten to antigen-presenting cells for a prolonged period, thereby maintaining robust antibody titres. The following is a discussion of the ways in which these vaccine compo-nents may be manipulated to elicit an optimal drug-specific immune response.
Behind every great vaccine is a great adjuvant. Discovered in the 1920s, aluminium salts (alum) are among the most widely used adju-vants in human vaccines39. Alum is ideally suited for drug vaccines in that it promotes humoral immunity, but its inability to elicit a cellular immune response and the hetero-geneity of vaccine formulations containing alum have encouraged the search for clinic-ally safer alternatives41,42. Many potential candidates, such as water-in-oil emulsions, have been identified as robust activators of cell-mediated immunity, but their application to human usage was suspended owing to their
P E R S P E C T I V E S
68 | JANUARY 2012 | VOLUME 12 www.nature.com/reviews/immunol
© 2012 Macmillan Publishers Limited. All rights reserved

extreme toxicity (TABLE 2). Conversely, oil-in-water adjuvant substitutes, such as TiterMax and the Ribi Adjuvant System, appear to be well tolerated in laboratory animals, but they still require additional preclinical and clinical testing before their promotion to human vaccines15,16,43,44.
It follows that a new class of immune potentiator, the function of which is more akin to that of an adjuvanting immuno-conjugate than that of an inert carrier protein, represents another conduit to achieving superior vaccines. Two relevant candidates — the adenovirus-based vaccine platform and bacteriophage Qβ — efficiently induce strong B cell and cytotoxic T cell responses that are specific for virus proteins as well as for an inserted foreign epitope or transgene-encoded protein45,46. These immune responses are robust and long-lived in rodents, dogs and non-human primates, often without the use of a separate adjuvant46. Already a successful vaccine delivery system for numerous infec-tious agents, the adenovirus human serotype 5 (AdHu5) vector was recently explored as an immunogenic vaccine vehicle for exogenous small molecules via its covalent coupling to a cocaine hapten, wherein it evoked high titres of cocaine-specific antibodies47. Despite
these promising preclinical results, the previ-ous exposure of most humans to adenovirus infections may detract from the immuno-genicity of these vaccines. In parallel, a nicotine vaccine formulated via the coupling of a nicotine hapten to virus-like particles (VLPs) of bacteriophage Qβ evoked strong titres of drug-specific antibodies in preclini-cal tests with or without alum, but its success in clinical trials was variable46. Nevertheless, these highly immunogenic conjugate vaccines represent worthwhile avenues of investigation while scientists work to identify alternative adjuvants that are not only capable of matching the clinical efficacy of alum but also of exerting greater control over the relative contributions of the humoral versus cellular arms of the immune response.
Behind a great adjuvant may be an out-dated carrier protein. As Arthur Kornberg eloquently stated, “V. Do not waste clean enzymes on dirty substrates” and “VI. Depend on viruses to open windows”48. The previous section highlighted the immune-potentiating effects of viral vaccine vehicles and VLP-based carriers. However, most preclinically and clinically tested drug immuno conjugates use refined,
‘clean’ haptens with ‘dirty’ carrier-proteins (such as bovine serum albumin8,43, keyhole limpet haemocyanin1,4,44,49, cholera toxin B5,37, tetanus toxin50 and Pseudomonas aeruginosa exoprotein A9,18). The long history of safe use of such immunoconjugates has potentially constrained experimentation on methods to improve their immunostimulatory or pharmacokinetic properties. Of the three nicotine vaccines5,51 and one cocaine vac-cine6,37 that have advanced through Phase I and Phase II clinical trials, all have struggled to elicit consistently high titres in vaccinated subjects. Furthermore, the magnitude and affinity of drug-binding polyclonal anti bodies were often inadequate to confer a therapeutic effect6,37. It follows that the attachment of drug haptens to more dynamic, self-adjuvanting carriers, many of which have been tested in other human vaccines, may significantly enhance the magnitude, quality, rapidity or duration of the elicited immune response5,40. Such carriers include high molecular weight natural polymers, polymeric microspheres and liposomes (TABLE 2). Moreover, append-age of both ‘carrier’ components (that is, the haptenated protein and the polymer) could maximize antibody production in vivo by the concurrent induction of distinct
Table 1 | The pharmacodynamic and pharmacokinetic profiles of antibody-based immunotherapies
Property Molecular structure of antibody or derivative Methods for optimization
IgG F(ab’)2 Fab or Fab’ scFv
Size (kDa) 150 110 50–55 25 Multimers, Fc conjugation
Half-life Long (~21 days) Shorter than IgG, longer than Fab or Fab’
Shorter than F(ab’)2,
longer than scFvShort (<1 hour) Modify size or pI, mutate Fc region,
PEGylate
Binding affinity for drug target
Highest affinity, highest target retention
Highest affinity, highest target retention
High affinity, faster off-rates
Lower affinity, fastest off-rates
Affinity maturation, add bispecificity, enhance stability
Biodistribution* Capillary plasma compartment
Capillary plasma compartment
Cell-associated space
Not retained in organs or extravascular space
Variable according to size, half-life, pI and stability of immunotherapy
Clearance rate Slow Slow Rapid Immediate Variable according to size, half-life, pI and stability of immunotherapy
Clearance site Gut Gut Kidney Kidney Variable according to size, half-life, pI and stability of immunotherapy
Application Long-term protection or addiction management, relapse prevention
Overdose reversal, detoxification, short-term treatment for drug use
Overdose reversal, detoxification, short-term treatment for drug use
Detoxification?‡ Potential to address most drug use indications
Examples in the literature
Numerous drug-specific IgGs against: cocaine, nicotine, methamphetamines, opiates, phencyclidine
Cocaine20 Cocaine20, phencyclidine14
Cocaine20, methamphetamines17
Anti-idiotypic cocaine vaccines19, optimized cocaine-specific scFv fragments13, nicotine-specific polyclonal and monoclonal IgGs10, optimized methamphetamine-specific scFv fragments7, phencyclidine-specific mouse–human chimeric IgGs11
Fab, monomeric antigen-binding fragment; Fab’, monomeric antigen-binding fragment with the C-terminal amino acids (including cysteine) of the hinge region; F(ab’)
2, dimeric antigen-binding fragment; pI, isoelectric point; scFv, single-chain variable domain. *Compartment where the antibody derivative shows the
greatest mean residence time. ‡The therapeutic utility of scFv fragments in drug abuse treatment remains to be determined.
P E R S P E C T I V E S
NATURE REVIEWS | IMMUNOLOGY VOLUME 12 | JANUARY 2012 | 69
© 2012 Macmillan Publishers Limited. All rights reserved

Table 2 | Experimental and clinical vaccine formulations*
Vehicle or immunostimulatory agent
Composition Activity Efficacy and side effects
Liposomes Transferomes, proteasomes, archaesomes, nisosomes, cochleates, liposomes, virosomes (for example, immunopotentiating reconstituted influenza virosomes (IRIVs))
•Serve as a delivery vehicle for antigen•Direct mode of antigen interaction
with APCs to preferentially activate MHC class II or MHC class I pathway
•Elicit balanced TH1/T
H2-type immune
responses
Pros: enhance humoral and cellular immunity; extend antigen half-life for long-term presentation by APCs
Cons: issues with stability, manufacturing and quality assurances prevent human use
Polymeric microspheres
Nanoparticles, often coated with various substances (for example, gold, polystyrene, silica, biodegradable polymers or non-toxic carbohydrates (see below))
•Stimulate a humoral response with a T
H1-type bias
•Induce antibody titres on par with alum
Pros: control the kinetics of antigen release; stimulate mucosal and systemic immunity
Cons: still in preclinical or clinical development
Carbohydrates Polysaccharides (for example, dextran and glucans) and natural carbohydrates (for example, inulin-derived)
•Activate alternative complement pathway
•Elicit both TH1- and T
H2 -type immune
responses58
Pros: enhance humoral and cellular responses with minimal local or systemic toxicity; biodegradable and well-tolerated
Cons: still in clinical development
Mineral salts Aluminium phosphate or hydroxide; calcium, iron and zirconium salts
•Induce TH2-type immune responses42
•Enhance antigen-specific T cell clonal expansion and splenic B cell priming41
•Activate the NLRP3 inflammasome
Pros: production of neutralizing antibodies (IgE, IgG1 or IgG2)59; simple; cost-effective; good safety record in humans38
Cons: poor cellular immune response, poor reproducibility of alum-based vaccine preparation60
Emulsions Oil-in-water (o/w): MF59, Ribi Adjuvant System (RAS)‡
•Improve APC recruitment and activation•Enhance antigen presentation (o/w) •Stimulate localized inflammation
(w/o) •Elicit T
H1-type (CFA) and T
H2-type (IFA)
responses
Pros: induce potent humoral and cellular responses; MF59 approved for human vaccines
Water-in-oil (w/o): incomplete Freund’s adjuvant (IFA) or complete Freund’s adjuvant (CFA); TiterMax§
Cons: IFA and CFA too toxic for human use; most substitutes still in development
Bacterium-derived adjuvants
Cell wall peptidoglycan, lipopolysaccharide or monophosphoryl lipid A of Gram-negative bacteria; cholera toxin; bacterial flagellin; immunostimulatory sequences of microbial DNA (CpG DNA)
•Activate TLRs •Stimulate humoral and cellular
responses, primarily TH1-type
cytokines and IgG2a •Elicit T
H2-type responses (cholera
toxin) or TH1-type responses (flagellin)
Pros: induce cellular responses; TH1- and
TH2-type adjuvant; well-tolerated in clinical
trials; MPL approved for human use
Cons: broader applications of technology still in preclinical development
Viral vectors Adenoviruses45: 51 human serotypes (most notable: AdHu5 and AdHu2), 27 simian serotypes
•Trigger cytokine release and transduce immature dendritic cells via their expressed PAMPs
•Achieve long-lasting antigen presentation and robust transgene-specific antibody titres
•Elicit mixed TH1/T
H2-type response,
predominated by TH1-type help
Pros: outperform many other vaccine vectors in antibody production and CD8+ T cell frequencies; activate innate and adaptive immune system
Attenuated or inactivated viruses (for example, poxvirus vector)
Cons: still in preclinical development; pre-existing immunity from natural adenoviral infections may suppress immune response to AdHu5 vector and transgene
Tensoactive agents Saponins (for example, Quil A): tensoactive glycosides containing a hydrophobic nucleus of triterpenoid structure with carbohydrate chains linked to the nucleus
•Enhance antigen presentation to APCs•Stimulate cell-mediated immunity:
induce CTL production (TH1- and
TH2-type cytokines)
Pros: improve cellular response — thus used in human vaccines for life-threatening illnesses (such as HIV)
Cons: high reactogenicity severely limits human use
Imidazoquinolines Synthetic organic compounds that mimic TLR receptor ligands (for example, imiquimod and resiquimod)
•Bind TLR7 and TLR8 •Elicit strong antiviral T cell responses
Pros: augment T cell response and duration of protection
Cons: still in preclinical or clinical development
Cytokines IFNγ, GM-CSF and various others •Enhance cellular responses through various mechanisms51
Pros: control of immunological effect; DNA vaccines express the cytokine in the same vector as the antigen
Cons: toxicity; immunogenicity to heterologous cytokines; frequent dosing
APC, antigen-presenting cell; GM-CSF, granulocyte–macrophage colony-stimulating factor; IFNγ, interferon-γ; NLRP3, NOD-, LRR- and pyrin domain-containing 3; PAMP, pathogen-associated molecular pattern; T
H, T helper; TLR, Toll-like receptor. *The activity of vaccine carriers may range from vaccine vehicle or depot (top of
table) to immunostimulatory agent (bottom of table) (for a review, see REF. 40). ‡An o/w emulsion containing the detoxified endotoxin MPL and mycobacterial cell wall components (total dissolved solids and cell wall skeleton) in 2% squalene; Sigma-Aldrich. §A CytRx Corporation proprietary w/o adjuvant consisting of proprietary block copolymer CRL-8941, squalene, a metabolizable oil and a unique microparticulate stabilizer.
P E R S P E C T I V E S
70 | JANUARY 2012 | VOLUME 12 www.nature.com/reviews/immunol
© 2012 Macmillan Publishers Limited. All rights reserved

Nature Reviews | Immunology
20020
5
10
15
20
25
30
35
2003Year
Tobacco Illicit drugs
Perc
ent o
f US
popu
lati
on u
sing
dru
gs
2004 2005 2006 2007 2008 2009
> US$467.7 billion: cost of drug abuse to US government in 2005
immune signalling pathways. For example, dextran-conjugated serum albumin spurs robust, concurrent T helper 1 (TH1) and TH2 cell responses52 (TABLE 2). Simple, structural modifications that alter the in vivo pharmaco-kinetics of carriers could also improve their depot effect and their functioning in hapten presentation. Thus, the redesign of existing carriers may transform current vaccines into clinically successful, FDA-approved ‘clean’ immunotherapeutics.
The tortoise and the hareIs the scientific progress within immuno-pharmacotherapy moving faster than society’s awareness of the ethical ‘quagmire’53 and socioeconomic dilemmas that await the medical implementation of addiction vaccines? A central concern is patient consent: can governments compel convicts to be vac-cinated? Can parents compel their children to receive ‘standard’ drug immunizations as a preventive measure? Can physicians compel at-risk individuals, such as pregnant drug addicts and babies who were exposed to drugs in utero, to be vaccinated? Likewise, can current addicts accurately gauge the severity of their own addiction and subsequently adhere to a course of treatment? From the assumption that immunotherapy would directly benefit the patient, as well as indirectly benefit the family and society, the court, legal guardian and/or the physician may find themselves torn between their moral obliga-tion to impose anti-drug treatments and the patient’s legal right to refuse. Fortunately, the law has already addressed similar issues involving the administration of provocative medical treatments to non-consenting indi-viduals or minors. These include, but are not limited to, a parent’s authority to vaccinate their children against human papillomavirus, the chronic administration of controlled, addictive drugs to minors (for example, amphetamines and opiate painkillers) and the coercive medical treatment of convicts. Thus, establishing the legal precedence for consent may pose less of a challenge than overcoming the ethical issues associated with immunotherapy for drug abuse.
Another important consideration is the stigma attached to vaccination against drugs. Like the childhood immunizations against tetanus or measles, mumps and rubella (MMR), anti-drug vaccination becomes both a permanent medical record and a traceable immunological marker in one’s blood54. State laws in the United States permit urine drug testing as a prerequisite for employment, as well as for the receipt of unemployment benefits, public housing, food stamps and
welfare. Theoretically, these policies could be extended to drug screening via blood sam-pling, wherein an immunological record of anti-drug vaccination could prove detrimen-tal to the economic situation of an ‘admitted’ drug addict. It symbolizes the patient’s poten-tial to relapse or to engage in risky behaviour and, akin to how banks use low-credit scores, a record of an anti-drug vaccination may become a measure of one’s personal respon-sibility and could have detrimental financial consequences for the patient.
Of greater consequence is the adverse effect of drug-targeting vaccines on the patient’s perception of drug abuse. Although an open forum on their clinical availability may demystify the allure of drugs to younger gener-ations, the negative cultural view of addiction may leave vaccinated patients with a sense of social ostracism or self-deprecation, in a similar manner to Hester Prynne’s scarlet ‘A’55. These factors could undermine a patient’s recovery or even spur relapse. Conversely, patients who receive prophylactic immunotherapy to avoid future addiction may gain a false sense of pro-tection against the effects of drug exposure. This could promote social risk-taking, drug experimentation under peer pressure or even a pointed effort by vaccinated individuals to surmount the drug-binding capacity of antibody titres via drug binges.
A final stigma worthy of mention is that there exists an economic component to the dilemma of anti-drug vaccination. In the emergency room setting, who decides whether the patient displaying signs of acute
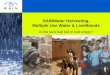
drug toxicity receives a monoclonal antibody-based antidote costing several thousand US dollars? In the treatment of addiction, is insurance required to offer health-care cover-age for this condition? Are poorer patients automatically denied access to certain forms of immunotherapy, such as prophylactic boosting to maintain titres of drug-specific polyclonal anitbodies or more expensive monoclonal antibody-based treatments? At what point does the price of immunotherapy exceed the socioeconomic cost of drug abuse, if ever? The development and clinical imple-mentation of drug vaccination is expensive; however, with an expenditure greater than US$467.7 billion seen in the United States in 2005 alone56, the cost of drug abuse to federal, state and local governments is staggering. Furthermore, current medications targeting drug addiction have done little to curb soci-ety’s appetite for drugs, as illustrated by the constant levels of drug use from 2002 to 2009 (FIG. 2). These legal, ethical and socioeconomic dilemmas surrounding immunopharmaco-therapy must be openly discussed by scientists, physicians and the public before this medical intervention for drug misuse reaches pharmacy shelves.
Kim D. Janda and Jennifer B. Treweek are at the Departments of Chemistry and Immunology,
The Scripps Research Institute, 10550 North Torrey Pines Road, BCC 582, La Jolla, California
92037‑1000, USA. Correspondence to K.D.J.
e‑mail: [email protected]
doi:10.1038/nri3130
Published online 16 December 2011
Figure 2 | Incidence of drug use. The use of tobacco products (blue) and illicit drugs (red) by persons residing in the United States aged 12 or older between 2002 and 2009. The y axis represents average drug use for any given month within the year. Illicit drugs include marijuana, cocaine, heroin, hallucino-gens, inhalants and prescription-type psychotherapeutics used for non-medical purposes. Data were accessed from the Substance Abuse and Mental Health Services Administration website57.
P E R S P E C T I V E S
NATURE REVIEWS | IMMUNOLOGY VOLUME 12 | JANUARY 2012 | 71
© 2012 Macmillan Publishers Limited. All rights reserved

1. Stowe, G. N. et al. A vaccine strategy that induces protective immunity against heroin. J. Med. Chem. 54, 5195–5204 (2011).
2. Nelson, A. L., Dhimolea, E. & Reichert, J. M. Development trends for human monoclonal antibody therapeutics. Nature Rev. Drug Discov. 9, 767–774 (2010).
3. Anton, B. et al. Vaccines against morphine/heroin and its use as effective medication for preventing relapse to opiate addictive behaviors. Hum. Vaccin. 5, 214–229 (2009).
4. Carrera, M. R. et al. Cocaine vaccines: antibody protection against relapse in a rat model. Proc. Natl Acad. Sci. USA 97, 6202–6206 (2000).
5. Cerny, E. H. & Cerny, T. Vaccines against nicotine. Hum. Vaccin. 5, 200–205 (2009).
6. Haney, M., Gunderson, E. W., Jiang, H., Collins, E. D. & Foltin, R. W. Cocaine-specific antibodies blunt the subjective effects of smoked cocaine in humans. Biol. Psychiatry 67, 59–65 (2010).
7. Harvey, B. R. et al. Engineering of recombinant antibody fragments to methamphetamine by anchored periplasmic expression. J. Immunol. Methods 308, 43–52 (2006).
8. Kantak, K. M. et al. Evaluation of anti-cocaine antibodies and a cocaine vaccine in a rat self-administration model. Psychopharmacology 148, 251–262 (2000).
9. Keyler, D. E., Roiko, S. A., Earley, C. A., Murtaugh, M. P. & Pentel, P. R. Enhanced immunogenicity of a bivalent nicotine vaccine. Int. Immunopharmacol. 8, 1589–1594 (2008).
10. Keyler, D. E. et al. Monoclonal nicotine-specific antibodies reduce nicotine distribution to brain in rats: dose- and affinity-response relationships. Drug Metab. Dispos. 33, 1056–1061 (2005).
11. Lacy, H. M., Gunnell, M. G., Laurenzana, E. M. & Owens, S. M. Engineering and characterization of a mouse/human chimeric anti-phencyclidine monoclonal antibody. Int. Immunopharmacol. 8, 1–11 (2008).
12. McClurkan, M. B., Valentine, J. L., Arnold, L. & Owens, S. M. Disposition of a monoclonal anti-phencyclidine Fab fragment of immunoglobulin G in rats. J. Pharmacol. Exp. Ther. 266, 1439–1445 (1993).
13. McKenzie, K. M. et al. Identification and characterization of single chain anti-cocaine catalytic antibodies. J. Mol. Biol. 365, 722–731 (2007).
14. Owens, S. M. & Mayersohn, M. Phencyclidine-specific Fab fragments alter phencyclidine disposition in dogs. Drug Metab. Dispos. 14, 52–58 (1986).
15. Pentel, P. R. et al. A nicotine conjugate vaccine reduces nicotine distribution to brain and attenuates its behavioral and cardiovascular effects in rats. Pharmacol. Biochem. Behav. 65, 191–198 (2000).
16. Peterson, E. C. et al. Using hapten design to discover therapeutic monoclonal antibodies for treating methamphetamine abuse. J. Pharmacol. Exp. Ther. 322, 30–39 (2007).
17. Peterson, E. C., Laurenzana, E. M., Atchley, W. T., Hendrickson, H. P. & Owens, S. M. Development and preclinical testing of a high-affinity single-chain antibody against (+)-methamphetamine. J. Pharmacol. Exp. Ther. 325, 124–133 (2008).
18. Roiko, S. A. et al. Combined active and passive immunization enhances the efficacy of immunotherapy against nicotine in rats. J. Pharmacol. Exp. Ther. 325, 985–993 (2008).
19. Schabacker, D. S., Kirschbaum, K. S. & Segre, M. Exploring the feasibility of an anti-idiotypic cocaine vaccine: analysis of the specificity of anticocaine antibodies (Ab1) capable of inducing Ab2β anti-idiotypic antibodies. Immunology 100, 48–56 (2000).
20. Treweek, J. B., Roberts, A. J. & Janda, K. D. Immunopharmacotherapeutic manifolds and modulation of cocaine overdose. Pharmacol. Biochem. Behav. 98, 474–484 (2011).
21. Pitas, G., Laurenzana, E. M., Williams, D. K., Owens, S. M. & Gentry, W. B. Anti-phencyclidine monoclonal antibody binding capacity is not the only determinant of effectiveness, disproving the concept that antibody capacity is easily surmounted. Drug Metab. Dispos. 34, 906–912 (2006).
22. Ohmura, N., Lackie, S. J. & Saiki, H. An immunoassay for small analytes with theoretical detection limits. Anal. Chem. 73, 3392–3399 (2001).
23. Paula, S., Tabet, M. R., Farr, C. D., Norman, A. B. & Ball, W. J. J. Three-dimensional quantitative structure-activity relationship modeling of cocaine binding by a novel human monoclonal antibody. J. Med. Chem. 47, 133–142 (2004).
24. Valentine, J. L., Arnold, L. W. & Owens, S. M. Anti-phencyclidine monoclonal Fab fragments markedly alter phencyclidine pharmacokinetics in rats. J. Pharmacol. Exp. Ther. 269, 1079–1085 (1994).
25. Covell, D. G. et al. Pharmacokinetics of monoclonal immunoglobulin G1, F(ab’)2, and Fab’ in mice. Cancer Res. 46, 3969–3978 (1986).
26. Holliger, P. & Hudson, P. J. Engineered antibody fragments and the rise of single domains. Nature Biotech. 23, 1126–1136 (2005).
27. Eddleston, M. & Persson, H. Acute plant poisoning and antitoxin antibodies. J. Toxicol. Clin. Toxicol. 41, 309–315 (2003).
28. Valentine, J. L. & Owens, S. M. Antiphencyclidine monoclonal antibody therapy significantly changes phencyclidine concentrations in brain and other tissues in rats. J. Pharmacol. Exp. Ther. 278, 717–724 (1996).
29. Proksch, J. W., Gentry, W. B. & Owens, S. M. Anti-phencyclidine monoclonal antibodies provide long-term reductions in brain phencyclidine concentrations during chronic phencyclidine administration in rats. J. Pharmacol. Exp. Ther. 292, 831–837 (2000).
30. Shelver, W. L. et al. Effects of recombinant drug-specific single chain antibody Fv fragment on [3H]-desipramine distribution in rats. Biochem. Pharmacol. 51, 531–537 (1996).
31. Keyler, D. E., Le Couteur, D. G., Pond, S. M., St. Peter, J. V. & Pentel, P. R. Effects of specific antibody Fab fragments on desipramine pharmacokinetics in the rat in vivo and in the isolated, perfused liver. J. Pharmacol. Exp. Ther. 272, 1117–1123 (1995).
32. Butler, V. P. J. et al. Effects of digoxin-specific antibodies and their Fab fragments on digoxin pharmacokinetics in dogs. J. Clin. Invest. 59, 345–359 (1977).
33. Scherrmann, J. M. et al. Immunotoxicotherapy: present status and future trends. J. Toxicol. Clin. Toxicol. 27, 1–35 (1989).
34. Bird, R. E. et al. Single-chain antigen-binding proteins. Science 242, 423–426 (1988).
35. Holton, O. D. et al. Biodistribution of monoclonal IgG1, F(ab’)2, and Fab’ in mice after intravenous injection. Comparison between anti-B cell (anti-Lyb8.2) and irrelevant (MOPC-21) antibodies. J. Immunol. 139, 3041–3049 (1987).
36. Cornuz, J. et al. A vaccine against nicotine for smoking cessation: a randomized controlled trial. PLoS ONE 3, e2547 (2008).
37. Martell, B. A. et al. Cocaine vaccine for the treament of cocaine dependence: a randomized double-blind placebo-controlled efficacy trial. Arch. Gen. Psychiatry 66, 1116–1123 (2009).
38. Glenny, A. T., Pope, C. G., Waddington, H. & Wallace, U. Immunological notes. XXIII. The antigenic value of toxoid precipitated by potassium alum. J. Pathol. Bacteriol. 29, 38–39 (1926).
39. Grun, J. L. & Maurer, P. H. Different T helper cell subsets elicited in mice utilising two different adjuvant vehicles: the role of endogenous IL-1 in proliferative responses. Cell. Immunol. 121, 134–145 (1989).
40. Leroux-Roels, G. Unmet needs in modern vaccinology: adjuvants to improve the immune response. Vaccine 28, C25–C36 (2010).
41. Jordan, M. B., Mills, D. M., Kappler, J., Marrack, P. & Cambier, J. C. Promotion of B cell immune responses via an alum-induced myeloid cell population. Science 304, 1808–1810 (2004).
42. Brewer, J. M. (How) do aluminium adjuvants work? Immunol. Lett. 102, 10–15 (2006).
43. Fox, B. S. et al. Efficacy of a therapeutic cocaine vaccine in rodent models. Nature Med. 2, 1129–1132 (1996).
44. Carrera, M. R. et al. Suppression of psychoactive effects of cocaine by active immunization. Nature 378, 727–730 (1995).
45. Tatsis, N. & Ertl, H. C. Adenoviruses as vaccine vectors. Mol. Ther. 10, 616–629 (2004).
46. Maurer, P. et al. A therapeutic vaccine for nicotine dependence: preclinical efficacy, and Phase I safety and immunogenicity. Eur. J. Immunol. 35, 2031–2040 (2005).
47. Hicks, M. J. et al. Cocaine analog coupled to disrupted adenovirus: a vaccine strategy to evoke high-titer immunity against addictive drugs. Mol. Ther. 19, 612–619 (2011).
48. Kornberg, A. Ten commandments: lessons from the enzymology of DNA replication J. Bacteriol. 182, 3613–3618 (2000).
49. Carrera, M. R., Ashley, J. A., Wirsching, P., Koob, G. F. & Janda, K. D. A second-generation vaccine protects against the psychoactive effects of cocaine. Proc. Natl Acad. Sci. USA 98, 1988–1992 (2001).
50. Moreno, A. Y. et al. A critical evaluation of a nicotine vaccine within a self-administration behavioral model. Mol. Pharm. 7, 431–441 (2010).
51. Hatsukami, D. K. et al. Immunogenicity and smoking-cessation outcomes for a novel nicotine immunotherapeutic. Clin. Pharmacol. Ther. 89, 392–399 (2011).
52. Lees, A. et al. Enhanced immunogenicity of protein–dextran conjugates: I. Rapid stimulation of enhanced antibody responses to poorly immunogenic molecules. Vaccine 12, 1160–1166 (1994).
53. Katsnelson, A. Ethical quagmire awaits vaccine for cocaine addiction. Nature Med. 10, 1007 (2004).
54. Cohen, P. J. Immunization for prevention and treatment of cocaine abuse: legal and ethical implications. Drug Alcohol Depend. 48, 167–174 (1997).
55. National Research Council and Institute of Medicine. New Treatments for Addiction: Behavioral, Ethical, Legal, and Social Questions (eds Harwood, H. J. & Myers, T. G.) (The National Academies Press, Washington, District of Columbia, 2004).
56. The National Center on Addiction and Substance Abuse (CASA). Shoveling Up II: The Impact of Substance Abuse on Federal, State and Local Budgets [online], http://www.casacolumbia.org/articlefiles/380-ShovelingUpII.pdf (2009).
57. Substance Abuse and Mental Health Services Administration. Results from the 2009 National Survey on Drug Use and Health: Volume I. Summary of National Findings [online], http://www.oas.samhsa.gov/NSDUH/2k9NSDUH/2k9Results.htm (2010).
58. Silva, D. G., Cooper, P. D. & Petrovsky, N. Inulin-derived adjuvants efficiently promote both Th1 and Th2 immune responses. Immunol. Cell Biol. 82, 611–616 (2004).
59. Lindblad, E. B., Elhay, M. J., Silva, R., Appelberg, R. & Andersen, P. Adjuvant modulation of immune responses to tuberculosis subunit vaccines. Infect. Immun. 65, 623–629 (1997).
60. Lindblad, E. B. Aluminium adjuvants — in retrospect and prospect. Vaccine 22, 3658–3668 (2004).
Competing interests statementThe authors declare no competing financial interests.
FURTHER INFORMATIONKim D. Janda’s homepage: http://www.scripps.edu/chem/janda/Substance Abuse and Mental Health Services Administration: http://www.samhsa.gov
ALL LINKS ARE ACTIVE IN THE ONLINE PDF
P E R S P E C T I V E S
72 | JANUARY 2012 | VOLUME 12 www.nature.com/reviews/immunol
© 2012 Macmillan Publishers Limited. All rights reserved