Embed Size (px)
Citation preview

10/24/13
1
The Throwing Athlete Biomechanics Function & Dysfunction
R. Scott Cook, DO, FAOASM Director, St. Joseph Sports Medicine Fellowship
Commonwealth Orthopaedic Associates
Presentation Goals
! Provide an understanding of normal Scapular Function and Motion. ! Discuss the importance of the Scapula within the kinetic chain of the
throwing athlete. ! Describe clinical examination techniques for evaluation of scapular
function. ! Define Scapular Dyskinesis and the role it plays in shoulder injury and
pathology.
Normal Scapular Function
! Scapular Osseous Components ! Body, Spine, Coracoid Process, Acromion Process, Glenoid,
Inferior Angle. ! Arise from several ossification centers with varies stages of
coalescence: – Coracoid: 14-18yo – Acromion: 19-20yo – Inferior Angle: 18-20yo – Glenoid Fossa: 20-25yo

10/24/13
2
Normal Scapular Function
! Basic Anatomy: Scapula is enveloped by multiple muscular layers. – Anterior Scapular Muscle Attachments:
! Triceps ! Biceps (Short and Long Heads) ! Coracobrachialis ! Subscapularis ! Serratus Anterior ! Pectoralis Minor ! Omohyoid
Normal Scapular Function ! Basic Anatomy:
– Posterior Scapular Muscle Attachments: ! Triceps ! Biceps (Long Head) ! Omohyoid ! Trapezis ! Supraspinatous ! Infraspinatous ! Teres Major ! Teres Minor ! Levator Scapulae ! Latissimus Dorsi ! Deltoid ! Rhomboideus Major and Minor
Normal Scapular Function
! Scapular Bursae: ! Infraserratus Bursa (Bursa Mucosa Serrata)
– Lies between Serratus Anterior and Chest Wall – Inflammed = Inferior Angle Pain
! Supraserratus Bursa (Bursa Mucosa Angulae Superioris
Scapulae) – Lies between Subscapularis and Serratus Anterior – Inflammed = Superior Angle Pain
! Scapulotrapezial Bursa – Lies between Superomedial Scapula and Trapezius
– Contains the Spinal Accessory Nerve.

10/24/13
3
Normal Scapular Function
! Scapular Anatomic Positioning at Rest: ! Anteriorly Rotated (relative to trunk) approx 30° ! Medial Border Rotated
– Inferior Pole diverged 3-5° from Spine
! Anteriorly Tilted 20° in sagittal plane
Normal Scapular Function
! Scapulothoracic Anatomy & Function: ! Scapular Postural Support
– Levator Scapulae & Upper Trapezius
! Scapular Retraction – Middle Trapezius & Rhomboids
! Scapular Protraction – Serratus Anterior
! Upward Scapular Rotation – Serratus Anterior & Trapezius
! Scapular Elevation – Upper Trapezius & Levator Scapulae
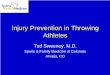
Normal Scapular Function
! A. Scapular Posterior Tilting ! B. Scapular Superior Rotation ! C. Scapular External Rotation ! D. Clavicular Elevation ! E. Clavicular Protraction

10/24/13
4
Normal Scapular Function
! Dynamic Anatomy: ! Humeral movement in relation to Glenoid. ! Glenohumeral Ligament and Labral static constraint on
Humeral Translation. ! Rotator Cuff dynamic constraint on Glenohumeral Motion.
The Scapula is intimately involved in each one of these functions.
Normal Scapular Function
! Glenohumeral Articulation ! Scapula must continually move to maintain instant center of
rotation. ! Proper glenoid alignment optimizes function of articulations
and rotator cuff to allow concentric GH-Motion. ! Scaulothoracic positioning determines position and inclination of
both Glenoid and Inferior Glenohumeral Ligament. ! Improper alignment can lead to GH Instability.
Normal Scapular Function
! Thoracic Wall Articulation ! Scapular Retraction (external rotation) facilitate cocking
position. ! Scapular Lateral Protraction (internal rotation) allows
acceleration. ! Scapular Anterior Thoracic Translation allows maintenance of
normal GH position and dissipation of deceleration forces.

10/24/13
5
Normal Scapular Function
! Acromial Elevation ! Serratus Anterior activation results in traction related superior
acromial elevation. ! Occurs during cocking and acceleration phases of throwing,
and during arm elevation. ! Allows for reduction of impingement and coracoacromial arch
compression.
Normal Scapular Function
! Kinetic Chain ! Scapula serves as a link in Proximal-to-Distal sequencing of
Velocity, Energy, and Forces of shoulder function. – Generation, Summation, Transference
– Scapula serves as pivotal link of transference of large forces/high energy from lower body/core to the arm/hand. ! Also allows arm stabilization to absorb force loads through long-lever
dynamics to reduce injury.
Scapular Motion
! Normal Scapular Dynamics: ! Bilateral Posterior Tilting, External Rotation, & slight
Superior Translation during elevation of arm. ! Symmetrical motion patterns. ! No prominent medial or superior scapular borders.

10/24/13
6
Scapular Dyskinesis
! Scapular Dyskinesis ! Alterations in STATIC scapular position and DYNAMIC
scapular motion resulting in scapular asymmetry in gross postural assessment and function movement.
Scapular Dyskinesis
! Scapular Dyskinesis: ! Affects normal Scapulohumeral Rhythm (SHR). ! May lead to articular and/or soft tissue shoulder dysfunction. ! May result in shoulder pathology and injury. ! May result from injury causing inhibition of scapular
stabilization.
Nonspecific Response: No specific pattern of dyskinesis is associated with a specific shoulder diagnosis.
Scapular Dyskinesis
! Contributing Factors ! Bony Posture & Injury
– Increased Thoracic Kyphosis ! ↑ Scapular Protraction ! Acromial Depression
– Clavicle Fractures – AC Joint Injury
! Disrupt normal progression of scapular rotation

10/24/13
7
Scapular Dyskinesis
! Contributing Factors ! Muscle Function Alteration
– Nerve injury ! Long Thoracic Nerve → Serratus Anterior ! Spinal Accessory Nerve → Trapezius
– Muscle Inhibition/Weakness ! Common in Glenohumeral Pathology ! Nonspecific response to shoulder pain
68% RC Abnormalities
94% Labral Tears 100% GH Instability
Scapular Dyskinesis
! Contributing Factors – Contracture/Inflexibility
! Pectoralis Minor/SH-Biceps ! Anterior Tilted Scapula
! GIRD – “Wind-Up” Effect
! Glenoid and Scapula pulled in forward-inferior direction ! May result in ↑ protraction during arm-ADDucted position
Scapular Dyskinesis
! Associated Shoulder Pathology: ! Subacromial Impingement ! Glenohumeral Instability ! Glenoid Labral Injury ! Rotator Cuff Injury

10/24/13
8
Assessing Scapular Dyskinesis
! Clinical Examination – Kinetic Chain Evaluation:
! Leg/Trunk Muscle Strength ! Lumbar Lordotic Posture ! Pelvic Alignment
! Iliac Rotations, SI Instability/Dysfunction
! Hip ROM ! Thoracic Alignment/Posture
! Thoracic Kyphosis, Scoliosis
! Cervical Posture ! Cervical Lordosis
Assessing Scapular Dyskinesis
! Clinical Examination – Examine patient from behind with arms at rest at sides. – Examine Scapular Motion as arms are elevated and
lowered within scapular plane. – Examine Scapular Motion as arms are elevated and
lowered within the sagittal plane.
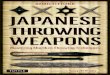
Types of Scapular Dyskinesis
! Type I ! Prominence of Inferior Medial Scapular Angle. ! Primarily abnormal rotation around a transverse axis. ! Results in excessive anterior scapular tilt.
! Type II ! Prominence of entire Medial Scapular Border. ! Results in abnormal rotation around a vertical axis. ! Associated with excessive scapular internal rotation.
! Type III ! Prominence of Superior Scapular Border. ! Results in excessive superior scapular translation.
! Type IV ! Normal, Symmetrical scapular motion.

10/24/13
9
Assessing Scapular Dyskinesis ! Observational Clinical Assessment
! 4-Type Method versus Yes/No Method ! Easily available ! Wide variance of Inter-Rater Reliability
– (4-Type) Sensitivity 10%-54%; Specificity 62%-94% – (Yes/No) Sensitivity 74%-78%; Specificity 31%-38%
! Limited assessment of multiple-plane asymmetries
! 3D EM Kinematic Analysis ! Lab-based; limited availability ! Allows for multiple-plane assessment ! Detected asymmetry may not be clinically relevant
Uhl et al; Arthroscopy, 25(11); 2009
Assessing Scapular Dyskinesis
! Yes/No Method ! Improved Inter-Rater Agreement (79%)
– Allows consideration beyond a single-plane of motion – PPV = 74%
! Displays Sensitivity (76%) & Specificity (35%) similar to other clinical shoulder exam tests.
– Clinical SLAP tests: Mean Sensitivity 57%; Specificity 41% – Clinical Instability tests: Mean Sensitivity 71%; Specificity 38% – Clinical Impingement tests: Mean Sensitivity 68%; Specificity 49%
Scapular Dyskinesis
! Prevalence of Scapular Asymmetry ! 71%-78% (3D Kinematics) of population at large ! Symptomatic vs. Asymptomatic
– Additional Factors: ! Ligamentous Laxity, Muscle Imbalance, Side Dominance
! Plane of Assessment may determine clinical relevance – Forward Flexion Motion Asymmetry increased in Symptomatic (54%)
versus Asymptomatic (14%) patients. ! Increased Serratus Anterior activity

10/24/13
10
Effects of Scapular Dyskinesis
! Loss of Retraction/Protraction – Retraction Loss
! ↓ stable “Cocking” point or base for arm elevation. ! ↑ Impingement as scapula rotates inferior and anterior.
– Protraction Loss ! ↑ deceleration forces in GH Joint. ! Functional Glenoid Anteversion.
– ↑ shear stresses on anterior stabilizing structures. – ↑ posterior impingement
Effects of Scapular Dyskinesis
! Loss of Superior Elevation – Decreased Acromial Elevation
! Predisposes Subacromial Impingement. ! Inhibition of Serratus Anterior and Lower Trapezius.
Effects of Scapular Dyskinesis
! Loss of Kinetic Chain Function – Disruption of transferal of lower extremity and core
forces to the upper extremity. ! ↓ Strength and Energy Use ! ↓ Acceleration Velocity

10/24/13
11
References ! Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy
and biomechanics. Arthroscopy 2003;19:404-420. ! Fleisig et al. Biomechanics of overhand throwing with implications for injuries. Sports Med 1996;21:421-437. ! Gaunche et al. The synergistic action of the capsule and the shoulder muscles. Am J Sports Med 1995;23:301-306. ! Glousman et al. Dynamic EMG analysis of the throwing shoulder with glenohumeral instability. J Bone Joint Surg Am
1988;70:220-226. ! Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg 2003;11:142-151. ! Kibler WB. Evaluation and diagnosis of scapulothoracic problems in the athlete. Sports Med and Arthro Rev
2000;8:192-202. ! Kibler WB. Role of the scapula in the overhead throwing motion. Contmp Orthop 1991;22:525-532. ! Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med 1998;26:325-337. ! Kibler et al. Qualitative clinical evaluation of scapular dysfunction. A reliability study. J Shoulder Elbow Surg
2002;11:550-556. ! Laudner et al. Scapular dysfunction in throwers with pathologic internal impingement. J Orthop Sports Phys Ther
2006;36:485-494. ! McQuade KJ, Dawson J, Smidt GL. Scapulothoracic muscle fatigue associated with alterations in scapulohumeral
rhythm kinematics during maximum resistive shoulder elevation. J Orthop Sports Phys Ther 1998;28:74-80. ! Myers JB, et al. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic
internal impingement. Am J Sports Med 2006;34:385-391. ! Oyama et al. Asymmetric resting scapular posture in healthy overhead athletes. J Athl Train 2008;43:565-570. ! Uhl et al. Evaluation of clinical assessment methods for scapular dyskinesis. Arthroscopy 2009;25:1240-1248.