Embed Size (px)
Citation preview

2/17/2015
1
UCL TEARS IN THE THROWING ATHLETE: FROM SURGERY TO
RETURN TO THROWING
Craig Garrison, PhD, PT, ATC, SCS
Ben Hogan Sports Medicine
Fort Worth, TX
Agenda
1. Ulnar collateral ligament (UCL) tear mechanism of injury and epidemiology
2. UCL anatomy and biomechanics
3. Presentation after UCL injury
4. Surgical interventions and associated procedures for UCL tear
5. Early post-operative management of the reconstructed UCL
6. Important milestones for early post-operative management of the UCL reconstructed elbow
7. Setting the foundation for return to throwing following reconstruction of the UCL in the throwing athlete
Objectives
1. Identify key anatomical and biomechanical factors that are involved with UCL injury in baseball players
2. Identify common characteristics associated with injury to the UCL in baseball players
3. Understand how to appropriately evaluate and diagnose UCL injury in baseball players
4. Understand the treatment options (conservative and surgical) for UCL injury in baseball players
5. Understand the principles of prevention and rehabilitation for UCL injury in baseball players

2/17/2015
2
Epidemiology and Mechanism of Injury
Epidemiology MLB UCLR 2000-2011
Adapted from Conte, 2015 ASMI
Adapted from Conte, 2015 ASMI
Epidemiology MLB UCLR 2000-2011

2/17/2015
3
Adapted from Conte, 2015 ASMI
Epidemiology MLB UCLR 2000-2011
Adapted from Conte, 2015 ASMI
Epidemiology MLB UCLR 2000-2011
Epidemiology
www.asmi.org

2/17/2015
4
Epidemiology
• Increasing rate of UCL tears in pre-adolescent and adolescent baseball players
• 192 enrolled in past 4 years – Ben Hogan
Mechanism of Injury
Mechanism of Injury

2/17/2015
5
Mechanism of Injury
• Contributing factors
– Genetics
– Work Ethics
– Mechanics
– Repetition
Adapted from John Conway, MD lecture
Mechanism of Injury
Body type
Pitch velocity
No. of pitches thrown
Type of pitches thrown
Year round play
Multiple teams/positions
Misuse / Overuse
Adapted from John Conway, MD lecture
Mechanism of Injury
Age 2006 USA Baseball Guidelines 2010 Little League Baseball Regulations
Daily Limits
17-18 N/A 105/day
15-16 N/A 95/day
13-14 75/game 95/day
11-12 75/game 85/day
9-10 50/game 75/day
7-8 N/A 50/day
Weekly Limits
15-18 N/A
31-45 pitches = 1 day rest 46-60 pitches = 2 days rest 61-75 pitches = 3 days rest 76+ pitches = 4 days rest
13-14 125/week; 1000/season; 3000/year
21-35 pitches = 1 day rest 36-50 pitches = 2 days rest 51-65 pitches = 3 days rest 66+ pitches = 4 days rest
11-12 100/week; 1000/season; 3000/year
9-10 75/week; 1000/season; 2000/year
7-8 N/A
Example limits for number of pitches thrown in games
www.asmi.org

2/17/2015
6
Mechanism of Injury
• Commonly injured during the throwing motion
– late cocking to acceleration phases of the throw
• valgus forces are high – 64 Nm
– 34.5 Nm UCL » (Fleisig et al., AJSM.,
1995)
– 64 Nm UCL » Werner et al., 1993
• UCL Tensile Failure - 13 to 32 Nm
Anatomy and Biomechanics
Anatomy and Biomechanics
• Valgus stress at elbow – majority of stress to
anterior bundle of UCL • (Fleisig et al., AJSM., 1995)
Posterior
Radius
Ulna
Humerus

2/17/2015
7
Anatomy and Biomechanics
• Valgus stress at the elbow – 300 N shear force on
medial elbow; 500 N compressive force on lateral side
• Fleisig et al., 1995
Anatomy and Biomechanics
• Valgus Extension Overload – valgus torque
elbow ext tensile stress med. compartment shear stress post. compartment compressive stress lat. compartment
Patel et al., Orthop Clin N Amer, 2014
Anatomy and Biomechanics
No significant difference between FB and CB in any FPM Sisto et al AJSM 15, 1987
Types of Pitches
Adapted from John Conway, MD lecture

2/17/2015
8
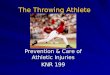
Normal
Stage 1
Delamination
Stage 2
Partial tear
Stage 3
Complete tear
Anatomy and Biomechanics
O’Driscoll AJSM 33, 2005
Pathology and Stages of MCL Tearing
Adapted from John Conway, MD lecture
Presentation after UCL Tear
Presentation after UCL Tear Stage 1 UCL Symptoms
• Warm up slow or difficult
• No pain after warm up but next day soreness frequent
• Stiff, achy but no pain
Adapted from John Conway, MD lecture

2/17/2015
9
Presentation after UCL Tear Stage 2 UCL Symptoms
• Pain throwing but still able to play
• Occasional loss of performance
• Rare lost time
• Variable duration of symptoms
Adapted from John Conway, MD lecture
Presentation after UCL Tear Stage 3 UCL Symptoms
• Concern
• Significant loss of performance
• Recurrent lost time
• Intolerable pain
• Unable to play
Adapted from John Conway, MD lecture
Presentation after UCL Tear
• UCL laxity leads to stresses on other tissues
– flexor-pronator mass • tendonitis
– ulnar nerve • neuropathy
– Patel et al., Orthop Clin N Am, 2014
Adapted from John Conway, MD lecture

2/17/2015
10
Presentation after UCL Tear
• Baseball players w/ UCL tears – changes in shoulder ROM – Garrison et al., AJSM, 2012
– deficits in TRM
– no deficits in GIRD
Control UCL P Value
GIRD -13.63±5.90 -12.53±5.98 .476
TRM 0.93±9.91 -6.67±11.82 .009*
HA -3.23±5.15 -3.00±5.01 .860
Elbow Ext. -1.17±2.76 -2.63±7.86 .339
Dom. Shdr. ER 119.70±11.77 113.30±13.95 .060
Presentation after UCL Tear
• Loss of ER shoulder ROM may be NM response– Garrison et al., AJSM,
2012
– restrictions in anterior musculature
ajs.sagepub.com/content/39/2/329/F1.large.jpg
Presentation after UCL Tear
• Baseball players w/ UCL tears – decreased LE balance – Garrison et al., JOSPT, 2013
* P = 0.001 * P = 0.001

2/17/2015
11
Presentation after UCL Tear
• Baseball players with UCL tears demonstrate decreased RC strength –
Garrison et al., In Progress 2015
– involved and uninvolved arms
Presentation after UCL Tear Hip ROM
• What we have found so far…External rotation differences
• Stance limb: • Injured hip ER: 28.9 +10.5
• Healthy hip ER 24.6 + 7.4
• P= .035*
• Lead limb: • Injured hip ER 28.5 + 10.3
• Healthy hip ER26.3 + 9.2
• P= .317
• Association between increase stance limb hip ER and UCL injury
Garrison JC, Hannon J, Conway J - Preliminary data
Presentation after UCL Tear Hip ROM
• What we have found so far…Internal rotation differences
• Stance limb • Injured hip IR: 30.6
• Healthy hip IR: 21.2
• P <.001
• Lead limb • Injured hip IR: 28.9
• Healthy hip IR: 22.4
• P<.001
• Association between increase stance and lead limb hip IR and UCL injury
Garrison JC, Hannon J, Conway J - Preliminary data

2/17/2015
12
Presentation after UCL Tear Hip ROM
• What we have found so far…total rotation differences
• Stance limb: • Injured TRM 59.5
• HealthyTRM 45.9
• P<.001
• Lead Limb
• Injured TRM: 57.5
• Healthy TRM 48.8
• P<.001
• Association between increase stance and lead limb hip TRM and UCL injury
Garrison JC, Hannon J, Conway J - Preliminary data
Presentation after UCL Tear Examination
Medial Swelling
Motion Loss
UCL Tender
Valgus Stress Painful
Valgus Laxity
Associated Findings
Adapted from John Conway, MD lecture
Presentation after UCL Tear Valgus Laxity Assessment
Stress Radiography
Adapted from John Conway, MD lecture

2/17/2015
13
Presentation after UCL Tear MUCL Insufficiency
Moving Valgus Stress Test Milking Maneuver
Adapted from John Conway, MD lecture
Presentation after UCL Tear Moving Valgus Stress Test
Very sensitive test for UCL injury – even at the molecular level
Probably not very specific
O’Driscoll AJSM 33, 2005 Adapted from John Conway, MD lecture
Presentation after UCL Tear
• Pain and dysfunction
– numbness, tingling, limits ability to throw
• Decreased performance
– loss of control, velocity
• Changes in shoulder and hip ROM
• Deficits in LE balance
• Decreased RC strength

2/17/2015
14
Surgical Intervention
Surgical Intervention
• Treatment options
– non-operative
– direct surgical repair
– reconstruction
Adapted from John Conway, MD lecture
Onlay Suture Anchors Figure 8 Docking
Docking Double Docking Button Docking
Screw Docking Button Screw Dock Double Screw

2/17/2015
15
Surgical Intervention Docking Procedure
Rohrbough J, et al. Am J Sports
Med 2002; 30(4):541-548.
Graft “docked” into ME, and proximal sutures tied over bone bridge
Courtesy David Altchek
Adapted from John Conway, MD lecture
Surgical Intervention Modified Docking Procedure
Graft Fixation:
4 Strand Graft Paletta G, et al. AJSM
2006
3 Strand Graft Koh JL, et al. Arthroscopy
2006
Paletta, G. et al. AJSM 2006;34:1594-8
Adapted from John Conway, MD lecture
Post-operative Management of UCL-R

2/17/2015
16
Early Post-operative Management of UCL-R
• Guidelines
– avoid valgus stress 1st 8 weeks
– full elbow ROM by 6 weeks
– maintain cardiovascular fitness
– normalize shoulder ROM and LE balance prior to throwing
• importance of trunk and shoulder rehab
– return to throwing program at 4 months
Early Post-operative Management of UCL-R
• Day 1 post-op to 6 weeks
– posterior splint (in neutral) and sling 1st 10 days
– 10 days - 6 weeks • restoration of elbow ROM
– full range by 6 weeks
ncmedical.com
Early Post-operative Management of UCL-R
• Day 11 post-op to 6 weeks
– initiate scapular NM re-ed
– wrist/hand ROM
– gripping and forearm strengthening
– core work
– initiation of LE balance exercises
• address pre-operative deficits

2/17/2015
17
Early Post-operative Management of UCL-R
• Full elbow ROM by 6 weeks
– patient placed on extension loss program if not achieved by this time
• Increase TERT
– Flowers et al., J Hand Ther, 1994
• stiff elbow
– Wilk et al., Clin Sports Med, 2004 www.getmotion.com
Ellenbecker et al., Sports Health, 2009
Early Post-operative Management of UCL-R
• Elbow weeks 4 to 8
– addition of light resistance – proximal
• scapular NM re-ed
• trunk/core stab
– BW l/e strength and balance
– continue aerobic conditioning
– NM re-ed • angular replication
– Manske et al., JOSPT, 2009
– restore GH mobility
Early Post-operative Management of UCL-R
• 6 to 8 weeks post-op
– initiation of shoulder strengthening exercises
• minimize valgus stress during weeks 6 to 8
• re-establish NM pathways

2/17/2015
18
Post-operative UCL-R Milestone Rationale
• 6 to 8 weeks post-op
• Scapular position for stable base = retraction and ER
– RC strength decreases as scapula is protracted
– Supraspinatus strength increases up to 24% in retraction in patients w/ shoulder pain
• Merolla et al. Musculoskelet Surg. 2010; 94; 119-125
• Tate et al. JOSPT. 2008;38:4-11
• Kibler et al. AJSM. 2006;34:1643-1647
Post-operative UCL-R
• 6 to 8 weeks post-op – Retraction – middle trap
– Depression and post tilt – low trap
– Protraction, upper rotation, ER, posterior tilt - serratus
Re-establish NM pathways
L
S
U
T
L
T
S
A
Post-operative UCL-R
• 2 to 3 months post-op
– program focused on full total body recovery
• trunk/scapula/rotator cuff strengthening
– full ER strengthening at 8 weeks
• GH ER valgus moment at elbow

2/17/2015
19
Post-operative UCL-R
• 2 to 3 months post-op
– flexor muscle mass strengthening
• may help to valgus stress due to orientation
– Davidson et al., Am J Sports Med., 1995
– initiate eccentric bicep work at end of phase
• may prevent pathologic olecranon contact with humeral fossa
– Fleisig et al., Oper Tech Sports Med, 1996
Post-operative UCL-R Rationale
• Exercises:
– should generate moderate to high muscle (EMG) activity
– should replicate function
– integration of whole-body kinetic chain approach
Reinold et al., JOSPT, 2009
Post-operative UCL-R
• 2 to 3 months post-op
Combo Flexion/Extension Squat to “W”

2/17/2015
20
Post-operative UCL-R
• 2 to 3 months post-op
Lawnmower with ER Single Leg Throwing Motion
Post-operative UCL-R
• 3 to 5 months
– “Pre-Return” to throwing phase begins at 3 months
• integrated strengthening to prepare shoulder and elbow for high forces experienced during throwing motion
Body Blade Superthrow
Post-operative UCL-R Milestone
• 3 to 5 months – “Pre-Return” to Throwing
– Normalized elbow ROM
– Shoulder TRM w/in 10°side to side
– Shoulder strength ER/IR ratio 50%
• uninvolved arm not appropriate?
– Improved scapular dyskinesis
– Neural tension under control
– Improved l/e balance

2/17/2015
21
Post-operative UCL-R
• 3 to 5 months – “Pre-Return” to Throwing – Integrated strengthening
– Plyometrics – beneficial for training the elbow
– Wilk et al, JOSPT, 1993; Wilk et al., JOSPT, 2003
• start with 2-hands → 1-hand
• perform for 4 weeks before initiating throwing program
Post-operative UCL-R
• 3 to 5 months – Pre-Return to Throwing
Wall Dribble Abduction
Post-operative UCL-R
• 3 to 5 months – Pre-Return to Throwing

2/17/2015
22
Post-operative UCL-R • 3 to 5 months – Pre-Return to Throwing
Wall Dribbles
Eccentric Catch
Setting the Foundation for Return to Throwing
Setting the Foundation for Return to Throwing
• When is my athlete ready to start throwing?
– pain?
– swelling?
– it’s been 4 mos since surgery?
• Want to use objective criteria to make evidence-based decision

2/17/2015
23
Setting the Foundation for Return to Throwing
• Between 4 and 5 months post-op UCL-R
– elbow ROM
– shoulder ROM and strength
– hip ROM
– neural tension
– scapular dyskinesis
– humeral torsion
– l/e balance
Setting the Foundation for Return to Throwing
Ulnar nerve
testing Median nerve
testing
Radial nerve
testing
Setting the Foundation for Return to Throwing
• Shoulder ROM
– GIRD < 10° • in context of torsion
– TRM < 7°
• When altered beyond certain levels, it changes GH kinematics and it is implicated in shoulder and elbow injury
• GIRD average of 28.5° in UCL deficient athletes
Dines et al., Am J Sports Med, 2009
• Greater than 25° loss predictive of shoulder and elbow injury
Shanley et al., Am J Sports Med, 2011
• No significant difference in GIRD, BUT significant different in TRM average 7°
Garrison et al., Am J Sports Med, 2012
• A more problematic motion restriction may be a loss of TRM
Manske et al., IJSPT, 2013

2/17/2015
24
Setting the Foundation for Return to Throwing
• Shoulder ROM
– GIRD < 10° • in context of torsion
– TRM < 7°
Research demonstrates greater retrotorsion in overhead athletes on their dominant limb Crockett et al., AM J Sports Med, 2002
Reagan et al., Am J Sports Med, 2002
Oshbar et al., Am J Sports Med, 2002
Meyers et al., Clin J. Sports Med, 2009
Whiteley et al., J. Orthop.Sports Phys Ther, 2009
Setting the Foundation for Return to Throwing
• Shoulder ROM
– Ex: GIRD of 15°with 12°of humeral torsion side to side diff
• majority of IR deficit explained by bony changes
Setting the Foundation for Return to Throwing
• Rotator cuff strength
– Ratio of 66% ER to IR at 0°
– Trakis et al., AJSM, 2008
• deficits present at time of UCL injury
– Garrison et al., In Progress

2/17/2015
25
Setting the Foundation for Return to Throwing
• Hip ROM
– Normalized side to side
– Red flag if < 25°in one direction
• < 50°TRM
– deficits present at time of UCL injury
» Garrison et al., In Progress
Setting the Foundation for Return to Throwing
• LE balance
– Greater than 90% composite score
• deficits present at time of UCL injury
– 89.1% - lead, 88.2% - stance
» Garrison et al., JOSPT, 2013
Stance Lead
Setting the Foundation for Return to Throwing
• LE balance
– Improved at time of return to throwing after UCL-R
– 93.6% - lead, 94.9% - stance
» Hannon et al., IJSPT, 2014

2/17/2015
26
Setting the Foundation for Return to Throwing
• LE balance
– Improved at time of release from PT after UCL-R
• similar to healthy controls
– 96.3% - lead, 96.9% - stance
» Garrison et al., Presented at 2015 CSM, Indianapolis, IN
Setting the Foundation for Return to Throwing
• Athlete has completed “pre-return” to throwing
• Criteria checked-off
– elbow ROM
– shoulder ROM and strength
– hip ROM
– neural tension
– scapular dyskinesis
– humeral torsion
– l/e balance
• Begin interval throwing program (ITP)
Setting the Foundation for Return to Throwing
• Biomechanical throwing analysis
– completed either toward middle or end of ITP
– continually monitoring changes in mechanics during ITP

2/17/2015
27
Questions?
References • Anderson MW, Alford BA. Overhead throwing injuries of the shoulder and elbow. Radiol Clin
N Am. 2010;48:1137-1154.
• Anloague PA, Spees V, Smith J, Herbenick MA, Rubino LJ. Glenohumeral Range of Motion and Lower Extremity Flexibility in Collegiate-Level Baseball Players. Sports Health: A Multidisciplinary Approach. 2012;4(1):25-30.
• Braun S, Kokmeyer D, Millet PJ. Shoulder injuries in the throwing athlete. J Bone Joint Surg Am. 2009;91:966-978.
• Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19(4):404-420.
• Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy. 2003;19(6):641-661.
• Byram IR, Bushnell BD, Dugger K, Charron K, Harrell FE, Noonan TJ. Preseason shoulder strength measurements in professional baseball pitchers. Am J Sports Med. 2010;38(7):1375-1382.
• Chambers L, Altcheck DW. Microinstability and internal impingement in overhead athletes. Clin Sports Med. 2013;32(4):697-707.
• Chuter VH, Janse de Jonge XAK. Proximal and distal contributions to lower extremity injury: a review of literature. Gait & Posture. 2012;36:7-15.
References
• Conway JE. Arthroscopic repair of partial-thickness rotator cuff tears and SLAP lesions in professional baseball players. Orthopedic Clinics of North America. 2001;32(3):443-456.
• Cordo PJ, Nashner LM. Properties of postural adjustments associated with rapid arm movements. J Neurophysiol. 1992;47:287-301.
• Cuff DJ, Pupello DR. Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. J Shoulder Elbow Surg. 2012;21:1450-1455.
• Davis JT, Limpisvasti O, Fluhme D, et al. The effect of pitching biomechanics on the upper extremity in youth and adolescent baseball pitchers. Am J Sports Med. 2009;37(8):1484-1491.
• De Mey K, Danneels L, Cagnie B, Cools AM. Scapular muscle rehabilitation exercises in overhead athletes with impingement symptoms. Effect of a 6-week training program on muscle recruitment and functional outcome. Am J Sports Med. 2012;40(8):1906-1915.
• DiGiovine NM, Jobe FW, Pink M, Perry J. An electromyographic analysis of the upper extremity in pitching. J Shoulder Elbow Surg. 1992;1(1):15-25.

2/17/2015
28
References
• Dines JS, Frank JB, Akerman M, Yocum LA. Glenohumeral internal rotation deficits in baseball players with ulnar collateral ligament insufficiency. Am J Sports Med. 2009;37(3):566-570.
• Drakos MC, Rudzki JR, Allen AA, Potter HG, Altcheck DW. Internal impingement of the shoulder in the overhead athlete. J Bone Joint Surg Am. 2009;91:2719-2728.
• Earl JE, Hertel J. Lower-extremity muscle activation during the Star Excursion Balance Tests. J Sport Rehabil. 2001;10(2):93-104.
• Edwards SL, Lee JA, Bell JE, et al. Nonoperative treatment of superior labrum anterior posterior tears. Am J Sports Med. 2010;38(7):1456-1461.
• Esposito MD, Arrington JA, Blackshear MN, Murtagh FR, Silbiger ML. Thoracic outlet syndrome in a throwing athlete diagnosed with MRI and MRA. J Magn Reson Imaging. 1997;7:598-599.
• Fleisig GS, Andrews JR, Cutter GR, et al. Risk of Serious Injury for Young Baseball Pitchers. Am J Sports Med. 2011;39(2):253-257.
• Fortenbaugh D, Fleisig GS, Andrews JR. Baseball pitching biomechanics in relation to injury risk and performance. Sports Health: A Multidisciplinary Approach. 2009;1(4):314-320.
References
• Freehill MT, Ebel BG, Archer KR, et al. Glenohumeral Range of Motion in Major League Pitchers Changes Over the Playing Season. Sports Health: A Multidisciplinary Approach. 2011;3(1):97-104.
• Garrison JC, Arnold A, Macko MJ, Conway JE. Baseball Players Diagnosed With Ulnar Collateral Ligament Tears Demonstrate Decreased Balance Compared to Healthy Controls. J Orthop Sports Phys Ther. 2013;43(10):752-758.
• Garrison JC, Cole MA, Conway JE, Macko MJ, Thigpen C, Shanley E. Shoulder range of motion deficits in baseball players with an ulnar collateral ligament tear. Am J Sports Med. 2012;40(11):2597-2603.
• Gowan ID, Jobe FW, Tibone JE, Perry J, Moynes DR. A comparative electromyographic analysis of the shoulder during pitching: professional versus amateur pitchers. Am J Sports Med. 1987;15(6):586-590.
• Gribble PA, Hertel J, Plisky PJ. Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. J Athl Train. 2012;47(3):339-357.
• Harada M, Takahara M, Mura N, Sasaki J, Ito T, Ogino T. Risk factors for elbow injuries among young baseball players. J Shoulder Elbow Surg. 2010;19(4):502-507.
References • Hariri S, Safran MR. Ulnar collateral ligament injury in the overhead athlete. Clinics in sports
medicine. 2010;29(4):619.
• Hotchkiss RN, Weiland AJ. Valgus stability of the elbow. J Orthop Res. 1987;5(3):372-377.
• Hubbard TJ, Kramer LC, Denegar CR, Hertel J. Correlations among multiple measures of functional and mechanical instability in subjects with chronic ankle instability. J Athl Train. 2007;42(3):361.
• Hurd WJ, Kaplan LD, ElAttrache NS, Jobe FW, Morrey BF, Kaufman KR. A profile of glenohumeral internal and external rotation motion in the uninjured high school baseball pitcher, part II: strength. J Athl Train. 2011;46(3):289-295.
• Hurd WJ, Kaufman KR. Glenohumeral rotational motion and strength and baseball pitching biomechanics. J Athl Train. 2012;47(3):247-256.
• Hurd WJ, Kaplan KM, EIAttrache NS, Jobe FW, Morrey BF, Kaufman KR. A Profile of Glenohumeral Internal and External Rotation Motion in the Uninjured High School Baseball
Pitcher, Part I: Motion. J Athl Train. 2011;46(3):282-288.

2/17/2015
29
References
• Kibler WB, Kuhn JE, Wilk KE, et al. The disabled throwing shoulder: spectrum of pathology - 10-year update. Arthroscopy. 2013;29(1):141-161.
• Kibler WB, Sciascia A. Kinetic chain contributions to elbow function and dysfunction in sports. Clin Sports Med. 2004;23(4):545-552.
• Kibler WB, Sciascia A, Uhl T, Tambay N, Cunningham T. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. Am J Sports Med. 2008;36(9):1789-1798.
• Knesek M, Skendzel JG, Dines JS, Altcheck DW, Allen AA, Bedi A. Diagnosis and management of superior labral anterior posterior tears in throwing athletes. Am J Sports Med. 2013;41(2):444-460.
• Koo SS, Parsley BK, Burkhart SS, Schoolfield JD. Reduction of postoperative stiffness after arthroscopic rotator cuff repair: results of a customized physical therapy regimen based on risk factors for stiffness. Arthroscopy. 2011;27(2):155-160.
• Laudner KG, Myers JB, Pasquale MR, Bradley JP, Lephart SM. Scapular dysfunction in throwers with pathologic internal impingement. J Orthop Sports Phys Ther. 2006;36(7):485-494.
References
• Laudner KG, Sipes RC, Wilsom JT. The acute effects of sleeper stretches on shoulder range of motion. J Athl Train. 2008;43(4):359-363.
• Laudner KG, Wilson JT, Meister K. Elbow isokinetic strength characteristics among collegiate baseball players. Physical Therapy in Sport. 2011.
• Leetun DT, Ireland ML, Willson JD, Ballantyne BT, McClay-Davis I. Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sports Exerc. 2004;36(6):926-934.
• Lesniak BP, Baraga MG, Jose J, Smith MK, Cunningham S, Kaplan LD. Glenohumeral findings on magnetic resonance imaging correlate with innings pitched in asymptomatic pitchers. Am J Sports Med. 2013;41(9):2022-2027.
• Lin YC, Thompson A, Kung JT, Chieh LW, Chou SW, Lin JC. Functional isokinetic strength ratios in baseball players with injured elbows. Journal of sport rehabilitation. 2010;19(1):21.
• Ludewig PM, Reynolds JF. The association of scapular kinematics and glenohumeral joint pathologies. J Orthop Sports Phys Ther. 2009;39(2):90-104.
• MacWilliams BA, Choi T, Perezous MK, Chao EYS, McFarland EG. Characteristic ground-reaction forces in baseball pitching. Am J Sports Med. 1998;26(1):66-71.
References
• MacWilliams BA, Choi T, Perezous MK, Chao EYS, McFarland EG. Characteristic ground-reaction forces in baseball pitching. Am J Sports Med. 1998;26(1):66-71.
• McClure P, Balaicuis J, Heilland D, Broersma ME, Thorndike CK, Wood A. A randomized controlled comparison of stretching procedures for posterior shoulder tightness. J Orthop Sports Phys Ther. 2007;37(3):108-114.
• McClure P, Tate AR, Kareha S, Irwin D, Zlupko E. A clinical method for identifying scapular dyskinesis, Part 1: reliability. J Athl Train. 2009;44(2):160-164.
• McMullen J, Uhl T. A kinetic chain approach for shoulder rehabilitation. J Athl Train. 2000;35(3):329-337.
• Moore SD, Uhl TL, Kibler WB. Imrovements in shoulder endurance following a baseball-specific strengthening program in high school baseball players. Sports Health: A Multidisciplinary Approach. 2013;5(3):233-238.
• Morrey BF, Tanaka S, An KN. Valgus stability of the elbow: a definition of primary and secondary constraints. Clinical orthopaedics and related research. 1991;265:187-195.
• Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006;34(3):385-391.
• Neri BR, ElAttrache NS, Owsley KC, Mohr KJ, Yocum LA. Outcome of Type II superior labral anterior posterior repairs in elite overhead athletes. Effect of concomitant partial-thickness rotator cuff tears. Am J Sports Med. 2011;39(1):114-120.
• Neuman BJ, Boisvert CB, Reiter B, Lawson K, Ciccotti MG, Cohen SB. Results of arthroscopic repair of Type II superior labral anterior posterior lesions in overhead athletes. Am J Sports Med. 2011;39(9):1883-1888.
• Noffal GJ. Isokinetic eccentric-to-concentric strength ratios of the shoulder rotator muscles in throwers and nonthrowers. Am J Sports Med. 2003;31(4):537-541.

2/17/2015
30
References
• Norris B, Trudelle-Jackson E. Hip and thigh muscle activation during the Star Excursion Balance Test. J Sport Rehabil. 2011;20:428-441.
• Olmsted LC, Carcia CR, Hertel J, Shultz SJ. Efficacy of the star excursion balance tests in detecting reach deficits in subjects with chronic ankle instability. J Athl Train. 2002;37(4):501-506.
• Petty DH, Andrews JR, Fleisig GS, Cain EL. Ulnar Collateral Ligament Reconstruction in High School Baseball Players Clinical Results and Injury Risk Factors. Am J Sports Med. 2004;32(5):1158-1164.
• Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, Elkins B. The reliability of an instrumented device for measuring components of the star excursion balance test. N Amer J Sports Phys Ther. 2009;4(2):92-99.
• Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006;36(12):911-919.
• Provencher MT, Frank RM, LeClere LE, et al. The Hill-Sachs Lesion: diagnosis, classification, and management. J Am Acad Orthop Surg. 2012;20:242-252.
• Putnam CA. Sequential motions of body segments in striking and throwing skills: descriptions and explanations. J Biomechanics. 1993;26(Suppl 1):125-135.
• Reid M, Elliott B, Alderson J. Lower-limb coordination and shoulder joint mechanics in the tennis serve. Med Sci Sports Exerc. 2008;40(2):308-315.
• Reinold MM, Curtis AS. Microinstability of the shoulder in the overhead athlete. Int J Sports Phys Ther. 2013;8(5):601-616.
References
• Reinold MM, Escamilla R, Wilk KE. Current concepts in the scientific and clinical rationale behind exercises for glenohumeral and scapulothoracic musculature. J Orthop Sports Phys Ther. 2009;39(2):105-117.
• Reinold MM, Gill TJ. Current concepts in the evaluation and treatment of the shoulder in overhead-throwing athletes, part 1: physical characteristics and clinical examination. Sports Health: A Multidisciplinary Approach. 2010;2(1):39-50.
• Reinold MM, Gill TJ, Wilk KE, Andrews JR. Current concepts in the evaluation and treatment of the shoulder in overhead throwing athletes, part 2: injury prevention and treatment. Sports Health: A Multidisciplinary Approach. 2010;2(2):101-115.
• Reinold MM, Wilk KE, Macrina LC, et al. Changes in shoulder and elbow passive range of motion after pitching in professional baseball players. Am J Sports Med. 2008;36(3):523-527.
• Robb AJ, Fleisig GS, Wilk KE, Macrina LC, Bolt B, Pajaczkowski J. Passive ranges of motion of the hips and their relationship with pitching biomechanics and ball velocity in professional baseball pitchers. Am J Sports Med. 2010;38(12):2487-2493.
• Sayde WM, Cohen SB, Ciccotti MG, Dodson CC. Return to play after Type II superior labral anterior-posterior lesion repairs in athletes. Clin Orthop Relat Res. 2012;470:1595-1600.
References
• Scher S, Anderson K, Weber N, Bajorek J, Rand K, Bey MJ. Associations among hip and shoulder range of motion and shoulder injury in professional baseball players. J Athl Train. 2010;45(2):191-197.
• Sciascia A, Cromwell R. Kinetic chain rehabilitation: a theoretical framework. Rehabilitation Research and Practice. 2012:doi:10.1155/2012/853037.
• Seroyer ST, Nho SJ, Bach BR, Bush-Joseph CA, Nicholson GP, Romeo AA. The kinetic chain in overhand pitching: its potential role for performance enhancement and injury prevention. Sports Health: A Multidisciplinary Approach. 2010;2(2):135-146.
• Shanley E, Rauh MJ, Michener LA, Ellenbecker TS, Garrison JC, Thigpen C. Shoulder range of motion measures as risk factors for shoulder and elbow injuries in high school softball and baseball players. Am J Sports Med. 2011;39(9):1997-2006.
• Terry GC, Chopp TM. Functional anatomy of the shoulder. J Athl Train. 2000;35(3):248-255.
• Thigpen CA, Padua DA, Michener LA, et al. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J Electromyogr and Kines. 2010;20(4):701-709.
• Tokish JM, Curtin MS, YK K, Hawkins RJ, Torry MR. Glenohumeral internal rotation deficit in the asymptomatic professional pitcher and its relationship to humeral retroversion. J Sport Sci Med. 2008;7:78-83.
• Trakis JE, McHugh MP, Caracciolo PA, Busciacco L, Mullaney M, Nicholas SJ. Muscle strength and range of motion in adolescent pitchers with throwing-related pain: implications for injury prevention. Am J Sports Med. 2008;36:2173-2178.