Embed Size (px)
Citation preview

CNS Drugs 2005; 19 (11): 909-922LEADING ARTICLE 1172-7047/05/0011-0909/$34.95/0
© 2005 Adis Data Information BV. All rights reserved.
The Role of Alpha-4 Integrin in theAetiology of Multiple SclerosisCurrent Knowledge and Therapeutic Implications
William A. Sheremata,1 Alireza Minagar,2,3 J. Steven Alexander3 andTimothy Vollmer4
1 Multiple Sclerosis Center, University of Miami School of Medicine, Miami, Florida, USA2 The Department of Neurology, Louisiana State University Health Sciences Center, Shreveport,
Louisiana, USA3 The Department of Molecular and Cellular Physiology, Louisiana State University Health
Sciences Center, Shreveport, Louisiana, USA4 The Barrow Neurological Institute, Phoenix, Arizona, USA
Multiple sclerosis (MS) has been recognised as a disease since the mid-19thAbstractcentury. The delineation of its CNS pathology, revealing the presence of inflam-matory demyelination and relative sparing of axons, was originally interpreted asevidence of infection. Despite many studies, a primary infectious aetiology of MShas not been found. However, the occurrence of acute demyelinating diseasefollowing a variety of infections and vaccinations, leading to MS in about a thirdof cases, provides evidence for the existence of an auto-allergic pathogenesis forthe disease.
Improved understanding of the role of the blood-brain barrier in protecting theCNS, and the mechanisms by which cells gain entry into the brain and spinal cordhas advanced the understanding of MS. Evidence of the central role of theadhesion molecule α4β1-integrin (very late activation antigen-4 [VLA-4]) forlymphocytes in endothelial transmigration into the CNS specifically, has provideda major insight into the pathogenesis of human demyelinating disease and itsexperimental model, experimental autoimmune encephalomyelitis (EAE). Thisfinding has led to a new window of therapeutic opportunity in MS.
Monoclonal antibodies to VLA-4 abrogate the development of EAE in sen-sitised animals and may actually reverse its clinical and pathological findings inmanifest disease. Natalizumab, one such monoclonal antibody, which is adminis-tered intravenously, has been found to be a promising agent in the treatment ofMS. Although single doses produced no improvement in the speed or quality ofrecovery from acute exacerbations of MS in a phase II trial, long-term administra-tion (in phase II and phase III trials) have produced significant benefits withresults showing both a marked reduction in the risk of new magnetic resonanceimaging lesions and a significant reduction in the risk of exacerbations within 2months of the initiation of therapy. Phase III double-blinded controlled trials haveprovided additional evidence of safety and a favourable impact on exacerbationrates over the 1 year of administration. Unfortunately, the success of natalizumabhas been curtailed by three cases of progressive multifocal leukoencephalopathy,which have prompted the manufacturer to voluntary withdraw the drug from the

910 Sheremata et al.
market. An independent review board is currently investigating the safety of thedrug to determine whether it should return to the market.
The demonstration that selective modulation (blocking) of the adhesion mole-cule VLA-4 by natalizumab in MS, resembling that observed in experimentaldisease, represents a major advance in rational therapy.
In the mid-19th century, Charcot[1] described the cephalomyelitis, (and its subtypes – post-infectiousclassical clinical picture of multiple sclerosis (MS) and post-vaccinial encephalomyelitis).[27-29] A viraland the cardinal elements of its pathology. The aetiology for MS has also been hypothesised on therelapsing-remitting character of the clinical mani- basis that, in approximately one-third of MS cases,festations is the principle diagnostic feature of apparent post-infectious or post-vaccinial encepha-MS.[2] The inflammatory demyelinating pathology lomyelitis may be forerunners of the relapsing-re-with relative sparing of axons remains the distinc- mitting illness typical of MS.[27] However, a similartive pathological hallmark of this disorder.[3] De- illness occurs after rabies immunisation using thespite the span of time since the first recognition of Semple vaccine, which contains spinal cord materialMS as a diagnostic entity, its aetiology remains as well as killed rabies virus.[29] This observation,unknown. However, insight into the pathogenesis of that human immunisation to CNS tissue may resultthis demyelinative disorder continues to be gained in acute disseminated encephalomyelitis, has fo-by the investigation of immunological aberrations in cused interest on the importance of immune reac-human demyelinating diseases and the experimental tions to CNS tissues as a causative factor, not only inmodel, experimental allergic encephalomyelitis acute disseminated encephalomyelitis, but also in(EAE).[4-10]
MS.[4-10,29-32]
Together with the increasing understanding ofOver several decades debate has centered on thethe process of demyelination, windows of therapeu-
question of whether antibody or lymphocytes aretic opportunity have appeared. The recognition ofresponsible for myelin damage in post infectiousthe primacy of the blood-brain barrier (BBB)[11,12]
encephalomyelitis, post-vaccinial encephalomyeli-and the active mechanisms that must be orchestratedtis, MS[4,7,20-35] and in EAE.[5-10,13] Demyelination inby inflammatory cells to breach this barrier[13-25]
vitro by serum from experimental animals and byhave led to drugs that promise to halt, or at leastMS sera was demonstrated by Bornstein et al.[6,7]
slow, this process. This review focuses on the essen-and passive transfer of disease by lymph node cellstial role of adhesion molecules – in particularin EAE alone in vivo was accomplished by Patter-α4β1-integrin (the very late activation antigen-4son.[5] More recent attention has been largely fo-[VLA-4]) [table I]. This adhesion molecule is ex-cused on the primary role of T cells in the pathogen-pressed on lymphocytes, both T and B cells, naturalesis of EAE, irrespective of the antigen used tokiller cells and macrophages, but only in low levelsinduce disease.[8-10,13,18-24] Despite a great deal ofon neutrophils.[26] VLA-4 plays an essential role instudy, the role of antibodies in MS remains to bethe egress of cells from the intravascular compart-delineated.ment, their crossing the BBB and entry into the
CNS.[13,18,21-25]A consensus has developed that T cells are the
primary effectors both in MS and in1. Multiple Sclerosis (MS): Infectious EAE.[1,3,10,17-24,30-32] The presence of B cells, plasmaAetiology or Immune Mediated Illness cells and antibodies, as well as the loss of oligoden-
drocytes in some MS plaques, has been report-Acute encephalomyelitis following recogniseded.[33-35] These recent studies of pathology in MShuman viral infections, such as rubeola, or aftershow that, despite these accompanying features, theimmunisation with vaccinia has been interpreted aspredominant cells in active lesions are macrophagesevidence that viruses may be the primary cause of
the demyelinative disorder, acute disseminated en- and lymphocytes, in particular CD4+T cells.[35]
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

The Role of Alpha-4 Integrin in Multiple Sclerosis 911
Table I. Major adhesion molecules and their terminology
Type of adhesion Common name Alternative name Ligandmolecule
Selectins
P-selectin CD62p P-selectin glycoprotein ligand-1
L-selectin CD62l Peripheral node addressin-1
E-selectin CD62e Sialyl-LewisX like sugars
Integrins
α4-familya α4β1-integrin VLA-4 VCAM-1
α4β7-integrin Lamina propria molecule-1 Mucosal addressin adhesion cell molecule
β2-familyb αLβ2 CD11a/CD18, LFA-1 ICAM-1, ICAM-2, ICAM-3, ICAM-4
αMβ2 CD11b/CD18, Mac-1,CR-3 ICAM-1, ICAM-2, C3bi, coagulation factor Xa,fibrinogen
αxβ2 CD11c/CD18, p150,95 Fibrinogen, C3bi, collagen 1
αDβ2 CD11d/CD18 ICAM-3, VCAM-1
a Natalizumab binds to both α4β1- and α4β7-integrins; however, only α4β1-integrin appears to be relevant to the pathogenesis ofmultiple sclerosis. While α4β7-integrin probably plays a pathogenic role in inflammatory gut disease and other diseases, there is noevidence for a role for α4β7-integrin in CNS disease.
b While there are several β-integrins, only one β2-integrin (leucocyte function-associated antigen-1 [αLβ2]) appears to play a role inCNS inflammatory disease.
ICAM = intercellular adhesion molecule; LFA = lymphocyte function-associated antigen; VCAM = vascular cell adhesion molecule; VLA =very late activation antigen.
The antigenic target of immune responses in MS tibodies is difficult.[36] Although the anti-MOG an-tibody may be found at the outset of MS, it ishas been actively studied in models of EAE. Mostcommon in relapsing MS[38,39] and T cell responsesstudies of EAE have been carried out using theto MOG are ubiquitous.[40] Anti-MOG responseswhole spinal cord, purified myelin or myelin basicmay act as co-stimulatory factors, or they may inprotein.[10] Other investigations have explored thefact, not have any relevance in MS.[40] From therelevance of other myelin proteins, notably prote-types of experiments described in this section, andolipid protein and myelin-oligodendrocyte glyco-taking into account the newly recognised aspects ofprotein (MOG).[10] While experimental disease canmolecular mimicry,[41,42] it would be difficult tobe induced with the proteolipid protein of myelin,select any specific antigenic reactivity to block in anand antibodies as well as T cells reactive to thiseffort to alter the disease process in MS.antigen are found in MS plaques, no role for sen-
sitisation to proteolipid protein has been established2. Blood-Brain Barrierin MS. However, recent investigations using MOG
to induce disease in marmosets have suggested that For decades it was thought that, in the absence ofdemyelinating disease in this primate experimental an inflammatory state, immune cells did not crossmodel may be antibody mediated.[36,37] Although the BBB and gain access to the CNS. However,passive transfer of the disease by serum from sen- Hickey et al.[17] showed that in the experimentalsitised animals to naive animals has been accom- situation, under ‘normal’ conditions, antigen-specif-plished, the immunology of the model is com- ic activated lymphocytes, but not naive lympho-plex.[36] In MOG-induced experimental autoimmune cytes, are capable of entering the CNS. In humanencephalomyelitis, T cells (CD4+ T helper-2 [Th-2] disease it is clear that activated T cells do cross thecells) may be the primary mediators of myelin dam- BBB.[28] CNS endothelial cells, including those inage.[37] T cells reactive to myelin basic protein are the venules, possess tight junctions that are impervi-present in these animals coincidentally with the anti- ous to intravascular fluids and cellular ele-MOG antibody. These T cells themselves may pro- ments.[11,12] These cells are also surrounded by astro-duce EAE, thus interpreting the significance of an- cytic foot processes that further support and main-
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

912 Sheremata et al.
tain the integrity of the BBB. All molecules, sialylated and fucosylated glycoproteinincluding proteins, as well as the cellular elements, ligands.[13,34,35] Selectin-mediated bonds are notmust be actively transported across this physical strong enough to arrest cells at the vessel wall andbarrier to gain access to the CNS but these processes are reversible. To stop rolling and arrest the cells onare still not understood.[11] In health, this physical the endothelium, these low affinity interactions mustbarrier is actively maintained, but egress of the be supplemented by integrins, which provide highintravascular elements into the CNS may occur as a affinity adhesion between the leucocyte and theresult of the failure of BBB maintenance.[11,12] In endothelial surface. The integrins, includingordinary circumstances, the BBB is an actual physi- α4β1-integrin, are membrane glycoproteins consist-cal barrier that may be breached only in an organised ing of two subunits – α and β. Although α4 in-and well orchestrated fashion.[11,13,17-25] The mecha- tegrins, as well as selectins, can contribute to rollingnisms of cellular transmigration across the BBB the predominant function of the β2-integrin leuco-have been extensively studied and although the cyte function-associated antigen-1 (LFA-1) and α4structure of the BBB is now well understood as a integrins (α4β1-integrin/VLA-4 and α4β7-integrin)result of decades of concerted effort, the mecha- in tissues is to reduce the velocity of rolling bynisms that maintain them are not.[11]
binding to their respective ligands – the intercellularEvidence has accumulated that in acute dissemi- adhesion molecule-I (ICAM-1) and the vascular cell
nated encephalomyelitis and MS, activated lympho- adhesion molecule (VCAM-1).[36-38] However, thecytes (T cells) have been sensitised to myelin anti- role of selectins in animal models as a requirementgens by contact with antigenic epitopes on myelin for integrin activation and cellular egress into theconstituents or by molecular mimicry.[10,41,42] The
CNS is less clear than in other tissues.[18,21,22,26]encounter of T cells with a CNS antigen, or another
VCAM-1, the ligand for α4β1-integrin, is a memberstimulating molecular epitope, induces a prolifera-of the immunoglobulin superfamily.[14-16]
tion of T cell clones – both memory and effectorInitial tethering is generally accomplished by thecells,[10,41,42] which can then target tissue antigens in
selectins expressed on leucocytes and tethering re-the CNS.sults in rolling, thus slowing down the cells. The
3. Adhesion Molecules three selectins, L-selectin on leucocytes, E-selectinand P-selectin on the endothelium, are the mostThe control of T cell migration from blood intoimportant initiators of adhesion.[14-16,20] Of these, thetissues resides in microvessels, the venules. Themost efficient tethering molecules are P-selectin andmicrodynamics of blood flow in venules result inL-selectin, with L-selectin playing a primary role inremarkable shear stresses with the rapid flow ordi-lymphoid tissues and P-selectin in other tissues.narily preventing attachment of intravascular cellsRolling leucocytes are slowed in their progress andto the endothelium. Attachment of the cells requiresare more able to respond to chemoattractants onadhesion receptors, acting as functional anchors, toendothelial cells. Chemoattractants (chemokines)form stable bonds with counter-receptors on theare principally presented on the endothelial surfacevascular wall. These adhesion receptors are not onlywhile others are secreted or diffuse into the vesselmechanical anchors, but also function as tissue-lumen. The chemokines are a family of molecularspecific recognition molecules.[14-17]
signals that direct effector and memory cells toEgress of leucocytes from the intravascular com-peripheral tissues and together interacting with spe-partment and entry into the CNS, as in other tissues,cific adhesions molecules confer organ-specificity.is accomplished by a series of steps: tethering, roll-Chemokines are distinct for different T cell sub-ing, adhesion (binding) and transendothelial migra-groups.[20,25] Although they play a central role in thetion across the BBB.[11,14-17] This is followed by theiregress of specific lymphocyte subgroups into targetsubsequent migration through the extracellular ma-organs, the role of chemokines in MS is outside thetrix in the CNS. Generally, the initial step of tether-scope of this review and thus, will not be discusseding leading to rolling is mediated by the selectinfurther in this article.family of adhesion molecules and their sulfated,
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

The Role of Alpha-4 Integrin in Multiple Sclerosis 913
Despite our knowledge of the role of selectins in of the endothelium results in high levels ofVCAM-1 expression.[13,50,51]inflammatory cascades in other organs, their role in
recruitment of leucocytes into the CNS remains a In addition to delineation of functions in vitro,matter of continuing discussion, partly because of α4β1-integrin has been shown to mediate selectintheir limited expression on cerebral endothelial independent leucocyte rolling in vivo. James et al.[23]
assessed the role of the α4-integrin/VCAM-1 path-cells.[18,22] However, Carrithers et al.[19] obtainedway in the migration of leucocytes through cerebralevidence of P-selectin providing an initial facilita-microvascular endothelial cells in lupus-pronetion of recruitment of activated encephalitogenic TMRL/fas(lpr) mice. They concluded thatcells into the healthy CNS. All selectins bind oligo-α4-integrin/VCAM-1, independent of P-selectin,saccharides related to sialyl-LewisX.[43] Tethering ofmediates leucocyte rolling and adhesion to mousethe leucocyte receptors P-selectin and L-selectincerebral endothelial cells. Such selectin-indepen-have strong affinity for P-selectin glycoproteindent rolling has also been demonstrated in in-ligand I.[44,45] Selectin-mediated bonds generallyterleukin (IL)-1 stimulated venules of the rabbitcannot arrest cells at the endothelial surface on themesentery, IL-4-stimulated venules of the cremastervessel wall, but selectins binding to ligands is anmuscle,[52,53] and in TNFα-stimulated venules ofactivating signal that induces rapid activation ofmice constitutively lacking all three selectins andboth α4 integrins and β2 integrins.ICAM-1[54] This evidence implicates α4β1–integrinThe integrins are a large family of cell surfacetissue ligands in rolling in the CNS, as well as inglycoproteins that mediate cell/cell and cell/matrixother tissues. However, the finding of increasedinteractions and also participate in signal transduc-plasma levels of CD31+ (selectin ligand) endoplas-tion. They are the major adhesion molecules andmic microparticles during MS exacerbations showsintegrins possess high affinity for their ligandsthat selectins are actively involved the immu-ICAM-1 and VCAM-1.[46-48] These cell surface re-nopathology of this human disease as well.[55] How-ceptors exist as non-covalently bound αβ heter-ever, α4β1-integrin is capable of participating inodimers with combinations of different α and βrolling behaviour, as well as adhesion to endotheli-chains. Integrins usually exist in a low affinity state.um and migration through the endothelial barrierUnder inflammatory conditions an activated cell canand movement in the CNS[55] (figure 1).transmit a signal from its cytoplasm that modifies
the molecular conformation of the extracellular do- 4. Role of α4β1-Integrin in Experimentalmains of integrins on the cellular membrane, en- Autoimmune Encephalomyelitishancing the affinity of the integrins for their respec-tive ligands. This activation mechanism is known as The role of α4β1-integrin in the pathogenesis of‘inside out signaling’.[24,49] The integrin heter- EAE has been the subject of a great deal of study.odimers adopt an open molecular conformation and Passive transfer experiments have proven that lym-this switch of integrins to a high affinity state leads phocytes play an essential role in the induction ofto a more efficient and enhanced binding to their EAE.[5,8,10] Macrophages accumulate, secondarily,integrin ligands. As a result, α4 integrins can medi- but become the dominant cell type in the inflam-ate activation-independent rolling interactions as matory lesions and are responsible for loss of thewell as arrest rolling leucocytes and this may be myelin/oligodendrocyte complex. Yednock et al.[13]
more important in the CNS than in other tis- showed that the α4β1-integrin molecule plays a keysues.[18,22] The α4 integrins can mediate tethering, role in the entry of antigen-specific CD4+ T lym-but their role in this is usually less efficient than the phocytes into the CNS in EAE. Monoclonal an-selectins. The primary integrins responsible for leu- tibody to α4β1-integrin prevents migration of CD4+cocyte binding are LFA-1, also referred to as cells into the CNS. In addition, monoclonal antibodyCD11a/CD18 and the two α4 integrins α4β1 and to α4 integrin suppresses and reverses inflammatoryα4β7. In the CNS α4β1 is of primary importance demyelination in EAE.[50] The development of de-because VCAM-1 is constitutively expressed in the myelinating lesions in EAE is primarilyCNS at low levels on endothelium, but stimulation α4β1-integrin dependent.[13,50,51] Recognition of the
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

914 Sheremata et al.
pro-inflammatory cytokine profile toward aTh-2-type cytokine profile.
Accumulated evidence indicates thatα4β1-integrin plays a central role in the pathogene-sis of EAE and in MS because of its role in tran-sendothelial migration of myelin-specific CD4+ Tlymphocytes into the CNS.[15-25,68] The demonstrat-ed role of α4β1-integrin in the adhesion of myelin-specific CD4+ T cells to cerebral microvascularendothelial cells strongly supports this conclu-sion.[19,24] The α4β1-integrin molecule has also beenimplicated in the interactions between myelin basicprotein (MBP)-primed T lymphocytes and microgli-al cells.[69,70] Dasgupta et al.[69] investigated the roleof MBP-primed T lymphocytes in the release ofnitric oxide (NO) and the expression of the inducibleform of NO synthase protein and messenger RNA inmouse BV-2 microglial cells. They reported thatmonoclonal antibody to the α4 chain ofα4β1-integrin blocked expression of α4β1-integrin
Natalizumab(α4β1-integrin
antagonist)
Lymphocyte
VLA-4
VCAM-1
Lymphocyte
VLA-4
VCAM-1
Endothelial cell
Extravasation
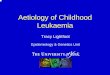
Fig. 1. Diagram representing the mechanism of action of natal-izumab. Binding of the lymphocyte adhesion molecule very lateactivation antigen-4 (VLA-4) with its ligand (counter-receptor) vas-cular adhesion molecule -1 (VCAM-1) expressed on endothelium isshown on the left side of the figure. Transmigration of a cell acrossthe endothelium (i.e. blood-brain barrier [BBB] in the CNS) occur-ring as a result of such binding is shown to the right of the cellsbinding. The mechanism of blocking VLA-4/VCAM-1 binding by amonoclonal antibody to the α4 chain of α4β1-integrin (natalizumab)is shown on the right side of the figure. This blocking of the α chainof the α4β1-integrin molecule is effective in binding and therebyprevents migration of lymphocytes across the BBB. at the surface of the MBP-primed T lymphocytes
and also blocked microglial NO production. Thissignificance of this pioneering work led directly to finding suggests that α4β1-integrin is a regulator ofthe initiation of human studies with a humanised cell-cell contact-mediated induction of induciblemonoclonal antibody, natalizumab, in MS.[56-62] NO synthase (iNOS).
Dasgupta and colleagues[70] also reported thatSeveral small molecules have been shown toMBP-primed T lymphocytes modulate expressionblock integrins LFA-1 and VLA-4 from bindingof pro-inflammatory cytokines in microglial cells.with their respective ligands ICAM-1 and VCAM-1They showed that MBP-primed T lymphocytes ex-both in vitro and in vivo.[63-67] Canella et al.[65]
pressed α4β1-integrin on their surface and again,investigated the effect of a synthetic small molecule,functional blocking of these adhesion molecules bynon-peptide antagonist of α4β1-integrin, TBC 3486,monoclonal antibody to the α4 chain inhibited Tin the treatment of the SJL mouse relapsing EAElymphocyte induction of microglial pro-inflam-
model. TBC 3486 has previously been shown to matory cytokines through CCAAT/enhancer bind-selectively block α4β1-integrin and also inhibit its ing protein β.binding to connecting segment-1 of fibronectin, aswell as to VCAM-1.[66] Clinical benefit of TBC 5. Role of α4β1-Integrin in MS3486 has also been documented in animal models of
The role of α4β1-integrin in MS has been thearthritis and pulmonary inflammation.[67] In EAE,
subject of continuing study since the seminal obser-daily administration of TBC 3486 for 14 days before vations by Yednock et al.[13] in EAE in 1992. Cala-the predicted onset of acute manifestations of EAE bresi et al.[71] reported that in MS interferonβ-1bmarkedly delayed the onset of disease, and delayed (IFNβ-1b) decreased α4β1-integrin expression inrelapse when administered in the chronic phase.[65]
CD3+ lymphocytes in vivo. In another study,There was also a reduction in the clinical severity of Muraro et al. found a link between decreased in-the disease and pathological evidence of demyelin- tegrin expression on lymphocytes and the therapeu-ation in the lesions. Immunocytochemistry and tic benefit from IFNβ-1b in reducing MRI activity inWestern blot assays of CNS tissue from acutely- MS.[72] In this study patients were followed from 2treated animals demonstrated a shift from Th-1 type months prior to treatment with IFNβ-1b to 3 months
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

The Role of Alpha-4 Integrin in Multiple Sclerosis 915
after initiation of treatment with IFNβ-1b.[72] shown to prominently inhibit trafficking of leuco-Monthly contrast enhanced magnetic resonance cytes across the BBB in EAE guinea pigs and toimaging (MRI) correlated closely with the down- rapidly reverse clinical manifestation of EAE inregulation of α4β1-integrin expression on CD4+ primates.[50,51] In early human studies it was found toand CD8+/CD45RO+ ‘memory’ T-lymphocytes. have a good safety profile; it was well tolerated in aExpression of α4β1-integrin was interpreted to dif- phase I, randomised, placebo-controlled, five-levelferentially modulate the proportion of CD4+, CD8+, dose escalation safety and tolerability study in pa-and CD27+ T lymphocytes.[72] The effect of tients who received single intravenous doses ofIFNβ-1b on MRI activity is not unexpected and is natalizumab for MS.[76]
largely attributable to inhibition of metal-7. Natalizumab Clinical Trials in MSloproteinases.[73]
Intravenous methylprednisolone has been report- A pharmacokinetic study of intravenous natal-ed to reduce upregulation of soluble VLA-4, LFA-1, izumab in 28 patients with MS revealed that a de-VCAM-1 and ICAM-1 adhesion molecules in blood tectable serum level of drug with good VLA-4 re-and CSF in relapsing-remitting and secondary pro- ceptor saturation was present 8 weeks after a singlegressive MS.[73] In vitro studies showed that methyl- injection (3 mg/kg dose).[76] This study and fiveprednisolone decreased transmigration of peripheral subsequent trials showed the drug to have a goodblood mononuclear cells through cerebral endotheli- safety profile and was well tolerated in stable MSal cell monolayers.[74,75] Sustained downregulation patients, as well as in relapsing-remitting and secon-of soluble adhesion molecules in vitro and observa- dary progressive MS patients during re-ble clinical benefits from corticosteroid administra- lapse.[56-59,76,77]
tion comparable to that of IFNβ-1b in MS have not Tubridy et al.[56] studied the administration ofbeen reported. two successive monthly intravenous doses of natal-
izumab to determine the effect of treatment on MRI6. Natalizumablesion activity in 72 patients with active, relapsing-
Natalizumab is a humanised monoclonal an- remitting and secondary progressive MS. These pa-tibody derived from a murine monoclonal antibody tients were followed for 24 weeks and were assessed(AN1000226m) to human α4β1-integrin. The mu- using clinical outcome measures as well as MRIrine antibody is humanised by grafting the comple- imaging measures. As might have been predictedmentarity-determining region of the hypervariable from the earlier trial,[76] the treated group exhibitedregion of the gene encoding the murine antibody significantly fewer new active lesions than the pla-onto a human immunoglobulin G4 framework.[13] cebo group (mean 1.8 vs 3.6 lesions per patient) andYednock et al.[13] and Kent et al.[50] reported that new enhancing lesions (mean 1.6 vs 3.3 lesions pertreatment of guinea pig EAE with either natal- patient) over the first 12 weeks when the drug wasizumab or its murine parent AN1000226m results in present in the serum. This benefit was lost in thea striking dose-dependent reversal of both clinical subsequent 12 weeks of the study. The investigatorsmanifestations and CNS leucocyte infiltration. suggested that a rebound in clinical exacerbations
may have occurred after the benefit from drug infu-As discussed, trafficking of specifically sen-sions had ended.[56] However, a 1-year long follow-sitised leucocytes across the BBB requires the inter-up of patients from the pharmacokinetic study[76] didaction of the cell adhesion molecule α4β1-integrinnot reveal any evidence of a clinical rebound effectexpressed on lymphocytes and monocytes with itsfollowing drug administration.[57] On the contrary,ligand VCAM-1. The VCAM-1 molecule is consti-the patients appeared to have fared better than theytutively expressed in low levels on brain and spinalhad prior to treatment.cord endothelial cells and at high levels following
immune activation.[50] Blockade of the molecular Based on the earlier EAE studies, we hy-pair (VLA-4/VCAM-1) binding prevents trafficking pothesised that natalizumab administration givenof leucocytes into the brain and spinal cord and within 36–72 hours of onset of an acute MS relapseresultant lesion formation. Natalizumab has been should accelerate clinical recovery by preventing
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

916 Sheremata et al.
further entry of activated T cells and macrophages analogue scale. In addition, the MRI study[58] suc-ceeded in showing marked inhibition of new T1into existing plaques and prevent the developmentgadolinium-enhancing lesion formation with natal-of new plaques. We predicted a reversal of theizumab over the 14 weeks of observation.evolution and multiplication of acute gadolinium
Miller et al.[59] reported a salutary outcome ofenhancing brain lesions seen in MRI brain studies,natalizumab in a randomised, double-blind, multi-and that more rapid resolution of clinical recoverycentre trial in 213 patients with relapsing-remittingwould logically follow. However, in a randomised,or relapsing secondary progressive MS. One-thirddouble-blind, multicentre study of 180 MS patients,received natalizumab 3 mg/kg (n = 71), one-thirdno difference in clinical recovery between natal-received natalizumab 6 mg/kg (n = 71) and one-thirdizumab and placebo treatment (administered withinreceived placebo (n = 71) every 28 days for 672 hours of exacerbation onset) was found, as mea-months. The primary endpoint was the number ofsured by serial Expanded Disability Status Scale andnew lesions appearing in monthly gadolinium-Scripps neurological rating scores.[58] Patients whoenhanced brain MRI during the 6-month treatmentreceived natalizumab reported a significant im-period. A marked reduction (91%) in the meanprovement in their sense of well-being on a visualnumber of new lesions was seen over 6 months oftreatment in the natalizumab recipients comparedwith placebo. The number of new lesions, over the6-month study duration, was 0.7 lesions per patientin the 3 mg/kg group and 1.1 lesions per patient inthe 6 mg/kg group compared with 9.6 lesions perpatient in the placebo group. Secondary outcomesincluded the number of clinical relapses and self-reported well-being using a visual analogue scale.Importantly, although the study was not powered topredict such a reduction, the patients in the natal-izumab groups experienced a significant (50%) low-er relapse rate and reported an improved sense ofwell-being compared with those who received pla-cebo. No significant difference in the incidence ofadverse events was seen in the active treatmentgroups compared with placebo. Fifteen patients inthe natalizumab groups developed binding antibo-dies, 13 of whom developed them during the treat-ment period and two during the post-treatmentfollow-up. In all of the earlier reported clinical trialsof natalizumab, an 8–10% incidence of binding an-tibodies has been documented.[56,58,59,76] In review-ing the data from these trials, no observable effect ofantibody on treatment outcomes was shown in pa-tients. Treatment emergent signs and symptoms arepresented in table II.
8. Pivotal Trials of Natalizumab in MS
The first year results of two large phase III trialsof natalizumab in MS were accepted as a basis forUS FDA approval in November 2004. A limitedamount of outcome data was released in the package
Table II. The adverse effects of natalizumab[59,77]
Adverse events Patients (%)
natalizumab placebo
General 35 30
headache 30 35
fatigue 24 18
arthralgia 15 11
allergic reaction 7 3
urinary urgency/frequency 7 5
chest discomfort 4 2
local bleeding 3 1
rigors 3 1
syncope 2 1
Infection
urinary tract 18 15
lower respiratory tract 14 14
gastroenteritis 9 5
vaginitis 8 5
tonsillitis 5 3
Psychiatric
depression 17 14
Gastrointestinal
abdominal discomfort 10 9
abnormal liver function test 5 3
Skin
rash 9 7
dermatitis 5 4
pruritus 4 2
Menstrual disorders
irregular menses/dysmenorrhoea 7 2
amenorrhoea 2 0
Neurological
tremor 3 2
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

The Role of Alpha-4 Integrin in Multiple Sclerosis 917
insert.[77] The two trials, the AFFIRM (Antegren® 1 reduced. In addition, the number of new or enlargingsafety and efficacy in relapsing-remitting multiple T2 lesions was substantially and significantly re-sclerosis) and SENTINEL (safety and efficacy of duced with natalizumab (p < 0.0001). There wasnatalizumab in combination with Avonex® also a highly significant impact on the MS Function-[IFNβ-1a] in patients with relapsing-remitting mul- al Composite (MSFC) scale as well as quality of lifetiple sclerosis) trials, have been completed and the measures. The majority of treated patients remainedfull 24-month AFFIRM trial outcomes were relapse free.presented at the American Academy of Neurology The SENTINEL study[78] was a secondheld in Miami Beach, Florida, USA, 9-16 April 120-week, randomised, double-blind, placebo-2005.[60-62,78]
controlled, multi-centre trial of 1171 patients withThe AFFIRM study was a 120-week, randomis- relapsing-remitting MS. The same dosage that was
ed, placebo-controlled, multicentre trial of a fixed- used in the AFFIRM trial was used in this study;dose intravenous natalizumab (300mg) administered intravenous natalizumab 300mg was administeredevery 4 weeks in patients with relapsing-remitting every 4 weeks. Patients who had been treated withMS.[60-62] A total of 942 patients were enrolled into Avonex® who had experienced one or more relapsesthe study, of whom 627 patients received active during treatment, were randomised to receive natal-treatment. On the basis of the achieving the primary izumab or placebo on a 1 : 1 basis. Avonex® wasoutcome in the first year, which was a highly signifi- continued throughout the study for both groups. Thecant reduction (66%) of relapses (p < 0.0001), and a placebo plus Avonex® group consisted of 582 pa-favourable safety and tolerance, the drug was ap- tients and the natalizumab plus Avonex® groupproved by the FDA (November 2004) for the pre-
consisted of 589 patients. These groups were wellvention of relapses in MS. The reduction in relapses
matched for baseline characteristics, including timewas sustained through to the end of the 120-week
on Avonex®. The outcome measures for this secondstudy with a ‘per patient’ reduction of 68% for the
2-year study were the same as those for the AFFIRMentire study (p < 0.0001). The primary outcomestudy. After the first year, natalizumab plusmeasure for the completed 2-year study was theAvonex® reduced the frequency of relapse by 53%impact of treatment on the prevention of sustainedcompared with placebo plus Avonex® (p < 0.0001).disability. Disability was defined as a 12-week sus-Gadolinium-enhancing brain lesions were reducedtained increase in disability by one point on theby 87% in the natalizumab plus Avonex® groupsextended disability status scale (EDSS). However, ifcompared with Avonex® and placebo.patients had no disability measurable at entry, an
The SENTINEL study was terminated prior toincrease of at least 1.5 points was required. The riskthe completion of the second year because two pa-of sustained disability was significantly less fortients receiving natalizumab plus Avonex® werenatalizumab recipients (17%) compared with place-diagnosed with progressive multifocal leukoen-bo-treated patients (29%; p < 0.0002). Interestingly,cephalopathy (PML), one of whom died.[79,80] Thethe risk for disability sustained for 24 weeks – thepatient in this study who died had neuropathologicaltime period used for the Avonex® study – was alsochanges typical of PML, but lesions typical of MSsignificantly less with natalizumab (11%) comparedwere not described at necropsy.[80] Moreover, a thirdwith placebo (23%), a reduction of 52% (p <patient who had Crohn’s disease was diagnosed with0.0001). The risk of progressing to an EDSS of ≥4.0PML after receiving treatment with natalizumab forwas markedly reduced with natalizumab, as was thethis condition.[81] Natalizumab was withdrawn fromrisk of progressing to an EDSS of ≥6.0. The numberthe market by the manufacturer on 28 February,of gadolinium enhancing lesions was reduced by2005 pending a review of the safety data by an92% for both the first and second year (p < 0.0001).independent review board.The volume of these lesions was also significantly
1 Antegren® is the former trade name for natalizumab. The new trade name is Tysabri®. The use of trade names is forproduct identification purposes only and does not imply endorsement.
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

918 Sheremata et al.
9. Why Might Progressive Multifocal Carrithers et al.[19] have demonstrated that activatedLeukoencephalopathy Complicate CD4+ Th1 cells can enter the brain in the absence ofNatalizumab Therapy Combined with an inflammatory focus. The blockade of VLA-4Other Drugs? with a monoclonal antibody analogous to natal-
izumab does not inhibit these nonspecifically acti-vated cells from entering the CNS. NonspecificallyIn the prospective MS drug trials, natalizumabactivated CD4 cells upregulate selectins on the en-monotherapy was shown to be safe and well tolerat-dothelial surface 2 hours after transfer to an experi-ed for >2 years. This record represents >1270 pa-mental animal and are necessary for the egress oftient years of experience.[60-62] However, this obser-these cells. Using a monoclonal antibody to block-vation stands in contrast to the outcome of combinedade P-selectin binding with its ligand (CD31) effec-IFNβ-1a and natalizumab therapy.[78] The occur-tively blocks early entry of activated cells into therence of PML in two patients diagnosed with
MS[79,80] who were treated concomitantly with CNS.[19] Clearly, therefore, early migration is regu-IFNβ-1a, was completely unexpected. PML is an lated by a set of molecules distinct from those usedopportunistic CNS infection caused by the JC virus, once inflammation has been established, that is:a polyomavirus.[79-82] VLA-4/VCAM-1. It is important to note that the
The incidence of antibody to the JC virus in- blockade of VLA-4 does not block early entry ofcreases with age, and rates for antibody positivity activated lymphocytes whose role certainly includesdiffer in different populations, averaging immune surveillance. In contradistinction to natal-50–85%.[81,82] Following the initial infection, the izumab, interferons have a great many differentvirus becomes a latent resident in the kidney and is effects on immune function, which collectively haveassociated with virus shedding in urine of up to 74% a major impact on re-establishing and maintainingof individuals.[81] It is also present in lymphoid the integrity of the BBB.[71,73] Jy et al.[83] havetissue in up to 35% of individuals. Despite the shown that IFNβ-1a (Avonex®) treatment in MSfrequent presence of virus, PML is rare, occurring reduces CD31+ endothelial microparticles in plasmaprimarily in the immunosuppressed patient.[82] The that result from the interaction of activated cellslargest group of patients with PML is in the HIV- with their ligand on the endotheolium. Therefore, itinfected population.[82]
is not so surprising that the combined effect ofThe absence of serious infections complicating natalizumab and IFNβ-1a on blocking the BBB
the use of natalizumab in earlier short-term studies should be so effective. Indeed, Carrithers et al.[19]
and in the pivotal trials was reassuring to investiga- argued that such combined treatment with IFNβ andtors.[56,57,59,61,76] There was a commonly held as- monoclonal antibody to VLA-4 should be explored.sumption, based on previous animal work, that the Unfortunately, the combined effect of these modali-impairment of immune function, attendant to the ties on the immunosurveillance may be excessive.blockade of VLA-4, was limited.[14-19,71,78] It was
Sustained antibody production to natalizumabfurther assumed that the addition of IFNβ was un-was observed in 6% of recipients after ≥3 months oflikely to affect the safety profile, and complicationstreatment.[61] Its presence was associated with a lossof immunosuppression were unlikely.[19,71,78]
of therapeutic benefit. In antibody-positive patientsIn some experimental situations, results havehypersensitivity reactions were commonly seen,been interpreted as suggesting that the adhesionconstituting 1.4% of the natalizumab treatedmolecule LFA-1, an integrin, may be more impor-group.[61] These reactions included urticaria, dizzi-tant in immune function than VLA-4.[14,15,78] Inness, fever, rash, rigors, pruritus, nausea, flushingsome rodent models, the blockade of this moleculehypotension, dyspnea, and chest pain. Severe reac-had a greater impact in experimental disease thantions, including anaphylaxis, occurred in <1% ofthe blockade of VLA-4.[13-19] However, there is yetpatients. Combined treatment with natalizumab andanother dimension of cellular immune function thatAvonex® resulted in a 30% decrease in clearance ofappears to be directly relevant in the unexpectedAvonex®.appearance of PML with natalizumab treatment.[19]
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

The Role of Alpha-4 Integrin in Multiple Sclerosis 919
In view of the relative safety of monotherapy lesions is seen with high dose IFNβ, which is similarwith natalizumab and the absence of new cases with to that with natalizumab.[85,86,88-90] Steinman,[92] incombined natalizumab and Avonex® treatment, it is whose laboratory at Stanford University (Stanford,likely that natalizumab will return to the market, California, USA), the initial development ofwith certain provisos. The possible occurrence of monoclonal antibodies to VLA-4 was carried out,PML in patients will probably require prospective has recently reviewed the subject of immune therapyscreening for the JC virus infection. Screening for for autoimmune diseases including MS.the unlikely event of atypical PML cases resembling
11. ConclusionsMS may become common place. It is probable thatalternative dosage schedules will also be studied. The age of rational therapy for MS arrived withRetesting of patients for the JC virus undergoing the successful targeting and blocking of VLA-4 onnatalizumab therapy, as well as other immunomodu- the surface of CD4+ cells, preventing adhesion oflatory agents, may become mandatory. circulating cells to its endothelial VCAM-1 counter-
receptor. The resulting outcome, the prevention of10. Comparison with Other Treatmentsclinical exacerbations and progression of disability,for MSas well as white matter lesions evidenced by brainMRI, is a scientific success and a potential improve-Beneficial clinical and MRI outcomes leading toment for the management for patients with MS. TheFDA approval have been reported for four drugssafety of natalizumab therapy in the AFFIRM trialcurrently on the market for the treatment of re-and the results from the first year of the SENTINELlapsing MS: IFNβ-1b (Betaseron®), IFNβ-1atrial led to the conclusion that the drug had a good(Avonex® and Rebif®) and glatiramer acetatesafety profile and was well tolerated, although it is(Copaxone®).[84-90] However, the marked reductionimmunogenic, stimulating the production of thein exacerbations within the initial 2 months of natal-blocking antibody. However, the development ofizumab treatment, which is also sustained thereafter,PML in MS patients treated with natalizumab,is in contrast to results reported with IFNβ-1b,[84]
though rare, has led to its withdrawal from theIFNβ-1a,[87-90] and glatiramer acetate[91] in MS pa-market. Although many researchers and clinicianstients. No significant reduction of exacerbations wasremain optimistic, the jury is still out as to whetherevident at 6 months in those pivotal studies.[84-90]
this remarkably effective drug, natalizumab, willAfter 2 years of treatment, exacerbations are re-return to the market, and if so, under what condi-duced by approximately 30% for each of these earli-tions.er approved products. Although subcutaneous
IFNβ-1b (Betaseron®)[84] and IFNβ-1a (Rebif®)[88] New agents that are currently in trials includehave similar reductions in exacerbations at 1 year in 683699 (GlaxoSmithKline [GSK]) a small moleculethe majority of recipients, both are associated with that effectively blocks VLA-4 (presently on hold).injection site reactions as well as significant system- GSK’s web site stated that “In a recent study, oralic ‘flu-like’ reactions.[84-90] Similarly, glatiramer ac- ‘699 [683699] matched the biomarker activity ofetate is associated with injection site reactions, but intravenous Antegren – the latest advance in theonly about half as frequently (about 40%) and a treatment of the disease.”[93] The 683699 trial in MStransient anxiety-like syndrome with chest tightness has temporarily been put on hold pending FDAin a smaller proportion of patients. A ‘flu-like’ syn- decisions on the safety of pharmacological blockadedrome is relatively uncommon in glatiramer acetate- of VLA-4. Several other companies (e.g. Biogentreated patients. Idec, Celltech R&D, Encysive Pharmaceuticals/
Schering-Plough, and Uriach) have very early stageThe clinical outcomes in the phase III trials ofdevelopment research programmes with VLA-4 an-natalizumab greatly surpass those of the other prod-tagonists in the treatment of MS.ucts currently available. The AFFIRM 2-year trial
outcome revealed a remarkable impact of natal- With the results of the AFFIRM trial, natal-izumab in preventing disability. However, in MRI izumab promised to quickly become the new stan-studies, an early reduction in gadolinium enhancing dard for the treatment of MS. The reported success-
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

920 Sheremata et al.
19. Carrithers MD, Visintin I, Kang SJ, et al. Differential adhesionful trial of natalizumab in Crohn’s disease supportsmolecule requirements for immune surveillance and inflam-
the concepts that drove the initiation of natalizumab matory recruitment. Brain 2000; 123: 1092-10120. von Andrian UH, MacKay CR. T-cell function and migration:trials in human diseases and further demonstrates
two sides of the same coin. N Engl J Med 2000; 343: 1020-34the therapeutic potential of this molecule.[94] Hope- 21. Vajkoczy P, Laschinger M, Engelhardt B. Alpha4-integrin-fully, a way to safely use natalizumab and similar VCAM-1 binding mediates G protein-independent capture of
encephalitogenic T cell blasts to CNS white matter microves-products will be found. Perhaps restrictions/moni-sels. J Clin Invest 2001; 108: 557-65
toring inclusions will enable natalizumab to return 22. Kerfoot SM, Kubes P. Overlapping roles of P-selectin and alpha4 integrin to recruit leukocytes to the central nervous system into the market so that patients with MS may haveexperimental autoimmune encephalomyelitis. J Immunolaccess to this effective drug. 2002; 169: 1000-6
23. James WG, Bullard DC, Hickey MJ. Critical role of the alpha 4integrin/VCAM-1 pathway in cerebral leukocyte trafficking inAcknowledgementslupus-prone MRL/fas(lpr) mice. J Immunol 2003; 170: 520-7
24. Hogg N, Laschinger M, Giles K, et al. T-cell integrins: moreNo sources of funding were used to assist in the prepara-than just sticking points. J Cell Sci 2003; 116 (Pt 23):tion of this review. The authors have no conflicts of interest4695-705that are directly relevant to the content of this review.
25. von Adrian UH, Engelhardt B. α4 integrins as therapeutictargets in autoimmune disease. N Engl J Med 2004; 348: 68-72
26. Birner U, Issekutz TB, Walter U, et al. The role of alpha (4) andReferencesLFA-1 integrins in selectin-independent monocyte and neutro-1. Charcot JM. Histologie de la sclerose en plaques. Gaz Hop Parisphil migration to joints of rats with adjuvant arthritis. Int1868; 41: 554-66Immunol 2000; 12: 141-502. Compston A, Ebers G, Lassman H, et al. McAlpine’s Multiple
27. Schwartz S, Mohr A, Knauth M, et al. Acute disseminatedSclerosis. 3rd ed. London: Churchill Livingstone, 1988encephalomyelitis: a follow-up study of 40 adult patients.3. Oppenheimer DR. Demyelinating diseases. In: Blackwood W,Neurology 2001; 56: 1312-8Corsellis JAN, editors. Greenfield’s neuropathology. 3rd ed.
28. Hartung HP, Grossman RI. ADEM. Distinct disease or part ofLondon: Edward Arnold, 1976: 470-499the MS spectrum? Neurology 2001; 56: 1257-604. Noseworthy JH, Lucchinetti C, Rodriguez M, et al. Multiple
29. Murthy JM, Yangala R, Meena AK, et al. Acute disseminatedsclerosis. N Engl J Med 2000; 343: 938-52encephalomyelitis: clinical and MRI study from South India. J5. Patterson PY. Transfer of allergic encephalomyelitis in rats byNeurol Sci 1999; 165: 133-6means of lymph node cells. J Exp Med 1960; 111: 119-36
30. Rocklin RE, Sheremata WA, Feldman RG, et al. The Guillain-6. Bornstein MB, Appel SH. Application of tissue culture to theBarre syndrome and multiple sclerosis: in vitro cellular re-study of experimental allergic encephalomyelitis: 1. Patternssponses. N Engl J Med 1971; 284: 803-8of demyelination. J Neuropathol Exp Neurol 1961; 20: 141-57
31. Sheremata WA, Cosgrove JBR, Eylar EH. Cellular hypersensi-7. Bornstein MB, Raine CS. Multiple sclerosis and experimentaltivity to basic myelin (A1) protein and clinical multiple sclero-allergic encephalomyelitis: specific demyelination of CNS insis. N Engl J Med 1974; 291: 14-7culture. Neuropathol Appl Neurobiol 1977; 3: 359-67
32. Hohlfeld R, Meinl E, Weber F, et al. The role of autoimmune T8. Ben-Nun A, Cohen IR. Genetic control of experimental autoim-lymphocytes in the pathogenesis of multiple sclerosis. Neurol-mune encephalomyelitis at the level of cytotoxic lymphocytesogy 1995; 45 Suppl. 6: S33-8in guinea pigs. Eur J Immunol 1982; 12: 709-13
33. Lassmann H, Vass K. Are current immunological concepts of9. Behan PO, Kies MW, Lisak RP, et al. In vitro studies: mecha-multiple sclerosis reflected by the Immunopathology of itsnisms of demyelination in experimental allergic encephalitis inlesions? Springer Semin Immunopathol 1995; 17: 77-87non-human primates. Arch Neurol 1973; 29: 4-9
34. Lassman H, Raine CS, Antel J, et al. Immunopathology of10. Owens T, Sriram S. The immunology of multiple sclerosis andmultiple sclerosis: report on an international meeting held atits animal model experimental allergic encephalomyelitis.the Institute of Neurology of the University of Vienna. JNeurol Clin 1995; 13 (1): 57-73Neuroimmunol 1998; 86: 213-711. Engelhardt B. Development of the blood-brain barrier. Cell
35. Luccinetti C, Brueck W. Paris J, et al. Heterogeneity of multipleTissue Res 2003; 314: 119-29sclerosis lesions: implications for the pathogenesis of demye-12. Minagar A, Alexander JS. Blood-brain barrier disruption inlination. Ann Neurol 2000; 47: 707-17multiple sclerosis. Mult Scler 2003; 9: 540-9
36. Massacesi L, Genain CP, Lee-Parritz D, et al. Active and13. Yednock TA, Cannon C, Fritz LC, et al. Prevention of experi-passively induced experimental autoimmune encephalomyeli-mental autoimmune encephalomyelitis by antibodies againsttis in common marmosets: as new model for multiple sclerosis.alpha 4 beta 1 integrin. Nature 1992; 356: 63-6Ann Neurol 1995; 37: 519-3014. Carlos TM, Harlan JM. Leukocyte-endothelial adhesion mole-
37. Uccelli A, Giunti D, Capello E, et al. EAE in the commoncules. Blood 1994; 84: 2068-101marmoset Callithrix jacchus. Int MS J 2003; 10: 6-1215. Frenette PS, Wagner DD. Adhesion molecules: Part 1. N Engl J
38. Berger T, Rubner P, Schautzer F, et al. Antimyelin antibodies asMed 1996; 334: 1526-9a predictor of clinically definite multiple sclerosis after a first16. Frenette PS, Wagner DD. Adhesion molecules: Part II: blooddemyelinating event. N Engl J Med 2004; 349: 139-45vessels and blood cells. N Engl J Med 1996; 335: 43-5
39. Bronstein JM, Lallone RL, Seitz RS, et al. A humoral response17. Hickey WF, Hsu BL, Kimura H. T-lymphocyte entry into theto oligodendrocyte-specific protein in MS: a potential molecu-central nervous system. J Neurosci Res 1991; 28: 254-60lar mimic. Neurology 1999; 53: 154-6118. Engelhardt B, Vestweber D, Hallmann R, et al. E- and P-selectin
are not involved in the recruitment of inflammatory cells 40. Vu T, Myers LW, Ellison GW, et al. T-cell responses toacross the blood-brain barrier in experimental autoimmune oligodendrocyte-specific protein in multiple sclerosis. Jencephalomyelitis. Blood 1997; 90: 4459-72 Neurosci Res 2001; 66: 506-9
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

The Role of Alpha-4 Integrin in Multiple Sclerosis 921
41. Lang HLE, Jacobsen JL, Ikemizu S, et al. A functional and resonance imaging (MRI) measures in patients with relapsingstructural basis for TCR cross-reactivity in multiple sclerosis. multiple sclerosis (MS): results from the AFFIRM trial. Neu-Nat Immunol 2002; 3: 940-3 rology 2005; 64 (Suppl.1) 147
63. Lin K, Ateeq HS, Hsiung SH, et al. Selective tight binding42. Wekerle H, Hohlfeld R. Molecular mimicry in multiple sclero-inhibitors of integrin α4β1 that inhibit allergic airway re-sis. N Engl J Med 2003; 349: 185-6sponses. J Med Chem 1999; 42: 920-3443. Etzioni A, Doerschuk CM, Harlan JM. Of man and mouse:
64. Kelly TA, Jeanfavre DD, McNeil DW, et al. Cutting edge: aleukocyte and endothelial adhesion molecule deficiencies.small molecule antagonist of LFA-1 mediated cell adhesion. JBlood 1999; 94: 3281-8Immunol 1999; 163: 5173-744. Vestweber D, Blanks JE. Mechanisms that regulate the function
65. Cannella B, Gaupp S, Tilton RG, et al. Differential efficacy of aof the selectins and their ligands. Physiol Rev 1999; 79:synthetic antagonist of VLA-4 during the course of chronic181-213relapsing experimental autoimmune encephalomyelitis. J45. Clark EA, Brugge JS. Integrins and signal transduction path-Neurosci Res 2003; 71: 407-16ways: the road taken. Science 1995; 268: 233-9
66. You TJ, Maxwell DS, Kogan TP, et al. A 3D structure model of46. Takada Y, Elices MJ, Crouse C, et al. The primary structure ofintegrin alpha 4 beta 1 complex: I. construction of a homologythe alpha 4 subunit of VLA-4: homology to other integrins andmodel of beta 1 and ligand binding analysis. Biophys J 2002;a possible cell-cell adhesion function. EMBO J 1989; 8:82 (Pt 1): 447-571361-8
67. Vanderslice P, Biediger RJ, Woodside DG, et al. Development47. Hynes RO. Integrins: a family of cell surface receptors. Cellof cell adhesion molecule antagonists as therapeutics for asth-1987 Feb 27; 48 (4): 549-54ma and COPD. Pulm Pharmacol Ther 2004; 17: 1-1048. Hynes RO. Integrins: versatility, modulation, and signaling in
68. Elices MJ, Osborn L, Takada Y, et al. VCAM-1 on activatedcell adhesion. Cell 1992; 69: 11-25endothelium interacts with the leukocyte integrin VLA-4 at a49. Ginsberg MH, Du X, Plow EF. Inside-out integrin signaling.site distinct from the VLA-4/fibronectin binding site. CellCurr Opin Cell Biol 1992; 4: 766-711990; 60: 577-84
50. Kent S, Karlik SJ, Cannon C, et al. A monoclonal antibody to α469. Dasgupta S, Jana M, Liu X, et al. Myelin basic protein-primed Tintegrin suppresses and reverses active experimental allergic
cells induce nitric oxide synthase in microglial cells. Implica-encephalomyelitis. J Neuroimmunol 1995; 58: 1-10tions for multiple sclerosis. J Biol Chem 2002; 277 (42):
51. Keszthelyi E, Karlik S, Hyduk S, et al. Evidence for a prolonged 39327-33role of alpha-4 integrin throughout active experimental allergic 70. Dasgupta S, Jana M, Liu X, et al. Role of very-late antigen-4encephalomyelitis. Neurology 1996; 47: 1053-9 (VLA-4) in myelin basic protein-primed T cell contact-in-
52. Hemmerich S, Rosen SD. Carbohydrate sulfotransferases in duced expression of proinflammatory cytokines in microgliallymphocyte homing. Glycobiology 2000; 10: 849-56 cells. J Biol Chem 2003; 278 (25): 22424-31
53. Sperandio M, Forlow SB, Thatte J, et al. Differential require- 71. Calabresi PA, Pelfrey CM, Tranquill LR, et al. VLA-4 expres-ments for core2 glucosaminyltransferase for endothelial L- sion on peripheral blood lymphocytes is downregulated afterselectin ligand function in vivo. J Immunol 2001; 167: treatment of multiple sclerosis with interferon beta. Neurology2268-74 1997; 49: 1111-6
54. Ferrell JC, Lipowsky HH. Leukocyte margination and deforma- 72. Muraro PA, Leist T, Bielekova B, et al. VLA-4/CD49dtion in mesenteric venules of rat. Am J Physiol 1989; 256 (Pt downregulated on primed T lymphocytes during interferon-2): 1667-74 beta therapy in multiple sclerosis. J Neuroimmunol 2000; 111:
55. Minagar A, Jy W, Jimenez JJ, et al. Elevated plasma endothelial 186-94microparticles in multiple sclerosis. Neurology 2001; 56: 73. Stuve O, Dooley NP, Uhm JH, et al. Interferon beta-1b de-1319-24 creases the migration of T lymphocytes in vitro: effect on
56. Tubridy N, Behan PO, Capildo R, et al. The effect of anti-alpha4 matrix metllaoproteinase-9. Ann Neurol 1996; 40: 853-63integrin antibody on brain lesion activity in MS. The UK 74. Elovaara I, Ukkonen M, Leppakynnas M, et al. Adhesion mole-Antegren Study Group. Neurology 1999; 53 (3): 466-72 cules in multiple sclerosis: relation to subtypes of disease and
57. Minagar A, Sheremata WA, Hume A, et al. Reduction of methylprednisolone therapy. Arch Neurol 2000; 47: 546-51relapses in multiple sclerosis after Natalizumab (Antegren) 75. Gelati M, Corsini E, de Rossi M, et al. Methylprednisolone actstreatment. Int MS J (On line) 2000 Mar 15 on peripheral blood mononuclear cells and endothelium in
58. O’Connor PW, Goodman A, Willmer-Hulme AJ, et al., and the inhibiting migration phenomena in patients with multiple scle-Natalizumab Multiple Sclerosis Trial Group. Randomized rosis. Arch Neurol 2002; 59: 774-80multicenter trial of intravenous natalizumab in acute MS re- 76. Sheremata WA, Vollmer TL, Stone LA, et al. A pharmacokinet-lapses: clinical and MRI effects. Neurology 2004; 62: 2038-43 ic study of intravenous natalizumab in patients with multiple
59. Miller MA, Khan OA, Sheremata WA, et al., and the Interna- sclerosis. Neurology 1999; 52: 1072-4tional Natalizumab MS Trial Group. A controlled trial of 77. Elan Pharmaceuticals Inc. Available from URL:natalizumab for relapsing-remitting multiple sclerosis. N Engl www.tysabri.com [Accessed 2004 Nov 26]J Med 2003; 348: 15-23 78. Rudick R, Stuart W, Calabresi P, et al. SENTINEL: A random-
60. Polman C, O’Connor P, Havradova E, et al., for the AFFIRM ized, placebo-controlled, Multicenter trial to determine theInvestigators. Clinical results from AFFIRM, a randomized, efficacy and safety of natalizumab, when added to intramuscu-double-blind, placebo controlled, multicenter trial to determine lar interferon beta-1a, in patients with relapsing multiple scle-the efficacy and safety of natalizumab in patients with re- rosis (MS): one-year clinical and MRI results [abstract]. Neu-lapsing multiple sclerosis (MS) [abstract]. Neurology 2005; 64 rology 2005; 64 Suppl. 1: 277(Suppl.1): 146 79. Langer-Gould A, Atlas SW, Bollen AW, et al. Progressive
61. O’Connor P, Havradova E, Hutchinsdon M, et al., for the multifocal leukoencephalopathy in a patient treated with natal-AFFIRM Investigators. Safety, tolerability and Immunogenic- izumab. N Engl J Med 2005; 353: 375-81ity of natalizumab: results from the AFFIRM Trial [abstract]. 80. Kleinschmidt-DeMasters BK, Tyler KL. Progressive multifocalNeurology 2005; 64 (Suppl. 1): 146 leukoencephalopathy complicating treatment with natal-
62. Miller D, O’Connor P, Havradova E, et al., for the AFFIRM izumab and interferon beta-1a for multiple sclerosis. N Engl JInvestigators. The efficacy of natalizumab on magnetic Med 2005; 353: 369-74
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)

922 Sheremata et al.
81. Van Assche G, Van Ranst J, Sciot R, et al. Progressive multifo- 89. The PRISMS Study Group and the University of British Colum-cal leukoencephalopathy after natalizumab therapy for bia MS/MRI Analysis Group. PRISMS-4: longer term efficacyCrohn’s disease. N Engl J Med 2005; 353: 362-8 of interferon-beta-1a in relapsing MS. Neurology 2001; 56:
82. Berger JR, Koralnik IJ. Editorial. Progressive multifocal 1628-36leukoencephalopathy and natalizumab: unforeseen conse- 90. Panitch H, Goodin DS, Francis G, et al. Randomized, compara-quences. N Engl J Med 2005; 353: 414-6
tive study of interferon β-1a treatment regimens in MS: The83. Jy W, Delgado S, Minagar A, et al. Interferonbeta-1a reduces EVIDENCE Trial. Neurology 2002; 59: 1496-506
plasma CD31+ endotheoial microparticles in MS [abstract].91. Johnson KP, Brooks BR, Cohen JA, et al. Copolymer 1 reducesAnn Neurol 2003; 54 Suppl. 7: S60
relapse rate and improves disability in relapsing-remitting84. The IFNB Multiple Sclerosis Study Group. Interferon beta-1b ismultiple sclerosis: results of a phase III multicenter, double-effective in relapsing-remitting multiple sclerosis: 1. clinicalblind, placebo-controlled trial. Neurology 1995; 45: 1268-76results of a multicenter, randomized, double-blind, placebo-
controlled trial. Neurology 1993; 43: 655-61 92. Steinman L. Immune therapy for autoimmune diseases. Science85. Paty DW, Li KDB, the UBC MS/MRI Group and the IFN 2004; 305: 212-6
Multiple Sclerosis Study Group. Interferon beta-1b is effective93. GlaxoSmithKline reviews novel therapeutics for CNS disordersin relapsing-remitting multiple sclerosis. Neurology 1993; 42:
and confirms strong pipeline momentum [company press re-662-7lease] 2004 Nov 23. Available from URL: www.gsk.com/86. Stone LA, Frank JA, Albert PS, et al. Characterization of MRImedia/archive_04.htm [Accessed 2005 Sep 30]response to treatment with interferon beta-1b: contrast-enhanc-
ing MRI lesion frequency as a primary outcome measure. 94. Ghosh S, Goldin E, Gordon FH, et al., Natalizumab Pan-Euro-Neurology 1997 Sep; 49: 862-9 pean Study Group. Natalizumab for active Crohn’s disease. N
87. Jacobs LD, Cookfair DL, Rudick RA, et al. Intramuscular Engl J Med 2003; 348: 24-32interferon beta-1a for disease progression in relapsing multiplesclerosis. Ann Neurol 1996; 39: 285-94
88. PRISMS (Prevention of Relapses and Disability by Interferon Correspondence and offprints: Dr William A. Sheremata, MSβ-1a subacutaneously in multiple sclerosis) Study Group. Center, University of Miami School of Medicine, 1501 NWRandomised double-blind placebo-controlled study of interfer-
9th Avenue, Miami, FL 33136, USA.on β-1a in relapsing/remitting multiple sclerosis. Lancet 2002;E-mail: [email protected]: 1498-504
© 2005 Adis Data Information BV. All rights reserved. CNS Drugs 2005; 19 (11)