Embed Size (px)
Citation preview

www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9 1
Review
Lancet Psychiatry 2015
Published OnlineOctober 27, 2015http://dx.doi.org/10.1016/S2215-0366(15)00356-9
Department of Psychosomatic Medicine, University of Tübingen, Tübingen, Germany (Prof S Zipfel MD, K E Giel PhD); Centre for Psychosocial Medicine, Department for General Internal Medicine and Psychosomatics, Heidelberg University Hospital, Heidelberg, Germany (K E Giel); University of North Carolina at Chapel Hill, Chapel Hill, NC, USA (Prof C M Bulik PhD), Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden (Prof C M Bulik PhD), School of Medicine and Centre for Health Research Western Sydney University, Penrith, NSW, Australia (Prof P Hay MD); and King’s College London, London, UK (Prof U Schmidt MD)
Correspondence to:Prof Stephan Zipfel, Centre of Excellence for Eating Disorders Tuebingen (KOMET) University of Tübingen, Department of Psychosomatic Medicine and Psychotherapy, Tübingen, 72076 Tübingen, [email protected]
Anorexia nervosa: aetiology, assessment, and treatmentStephan Zipfel, Katrin E Giel, Cynthia M Bulik, Phillipa Hay, Ulrike Schmidt
Anorexia nervosa is an important cause of physical and psychosocial morbidity. Recent years have brought advances in understanding of the underlying psychobiology that contributes to illness onset and maintenance. Genetic factors infl uence risk, psychosocial and interpersonal factors can trigger onset, and changes in neural networks can sustain the illness. Substantial advances in treatment, particularly for adolescent patients with anorexia nervosa, point to the benefi ts of specialised family-based interventions. Adults with anorexia nervosa too have a realistic chance of achieving recovery or at least substantial improvement, but no specifi c approach has shown clear superiority, suggesting a combination of re-nourishment and anorexia nervosa-specifi c psychotherapy is most eff ective. To successfully fi ght this enigmatic illness, we have to enhance understanding of the underlying biological and psychosocial mechanisms, improve strategies for prevention and early intervention, and better target our treatments through improved understanding of specifi c disease mechanisms.
“The want of appetite is, I believe, due to a morbid mental state…I prefer---the more general term [anorexia] ‘nervosa’, since the disease occurs in males as well as females, and is probably rather central than peripheral.”
Sir William Gull, 1874 (Transactions of the Clinical Society of London 7: 22–28)
IntroductionAnorexia nervosa is a highly distinctive serious mental disorder. It can aff ect individuals of all ages, sexes, sexual orientations, races, and ethnic origins; however, adolescent girls and young adult women are particularly at risk. This disorder is characterised by an intense fear of weight gain and a disturbed body image, which motivate severe dietary restriction or other weight loss behaviours such as purging or excessive physical activity.1–3 Additionally, cognitive and emotional functioning are markedly disturbed in people with this disorder. Serious medical morbidity and psychiatric comorbidity are the norm.4,5 Anorexia nervosa in adults and older adolescents commonly has a relapsing or protracted course,6 and levels of disability and mortality are high,7,8 especially without treatment. Even partial syndromes (ie, sub-syndromal anorexia nervosa) are associated with adverse health outcomes.9 Quality of life is poor and the burden placed on individuals, families, and society is high.10
This Review, like the Lancet Seminar published in 2010,4 which included all eating disorders, focuses on factors associated with anorexia nervosa that are of particular relevance to clinicians, such as recent developments in diagnosis, epidemiology, pathogenesis, treatment, and prognosis.
Classifi cation and diagnosisLow bodyweight or low body-mass index (BMI) is the central feature of anorexia nervosa. Tables 1 and 2 give an overview of diagnostic criteria for anorexia nervosa according to DSM2 and ICD11. Restricting and binge-purge subtypes and remission and severity specifi ers exist. Amenorrhoea is no longer required in the new DSM-5 diagnostic criteria and is also expected to be dropped in ICD-11.12 Main reasons for eliminating this criterion are
based on confl icts with inclusion of male individuals, adolescents who have not yet reached menarche, and women who use exogenous hormones into the diagnostic criteria. This change is also based on a large body of accumulated evidence13 showing no meaningful clinical diff erences between women with anorexia who menstruate and those who do not. DSM-5 also classifi es an atypical anorexia nervosa, which includes restrictive behaviours without meeting the low weight criterion.
In DSM-5, severity of anorexia nervosa is classifi ed along four levels by use of the individual’s BMI: extreme (BMI <15 kg/m²), severe (BMI 15–15·99 kg/m²), moderate (BMI 16–16·99 kg/m²), and mild (BMI ≥17 kg/m²). A systematic review from 201514 reported evidence for distinct illness trajectories and neuro cognitive features for eating disorders characterised by severe restriction (eg, infl exibility) or by overeating (eg, impulsivity and risk of substance use disorders) and evidence for eff ective secondary prevention or early treatment. Preliminary evidence also exists for a specifi c shift in focus of treatment to quality of life as primary outcome in patients with long-standing or intractable anorexia nervosa.15
EpidemiologyIn high-income countries, the lifetime prevalence of anorexia nervosa in the general population is reported to be around 1% in women and less than 0·5% in men.9 Accurate point prevalence has been more diffi cult to calculate, with studies often failing to identify any cases of DSM-IV-defi ned anorexia nervosa. If the broader DSM-5 criteria A and C (low weight in the presence of overvaluation of weight or shape) are applied, the point prevalence is about 0·3–0·5%.16 Some studies,17 but not all clinical incidence studies, support an increase in anorexia nervosa in adolescents in the past two to three decades.9 Anorexia nervosa typically begins in early-to-mid-adolescence, although it can emerge at any age.18 The sex ratio in adults is 1:8, with more female individuals affl icted.19 In children, the sex distribution is less skewed.20 Outcomes diff er across age groups, with higher rates of full recovery and lower mortality in adolescents than in adults (mean mortality 2% vs 5%).21

2 www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9
Review
Psychiatric and physical comorbidityNearly three-quarters of patients with anorexia nervosa report a lifetime mood disorder, most commonly major depressive disorder.22 Between 25% and 75% of patients with anorexia nervosa report a lifetime history of at least one anxiety disorder,23 which typically precedes anorexia nervosa and starts in childhood.24 Obsessive-compulsive disorder occurs in 15–29% of individuals with anorexia nervosa,25 with up to 79% experiencing obsessions or compulsions at some point in their lives.26 In population-based studies, the prevalence of alcohol misuse or dependence in individuals with anorexia nervosa is between 9% and 25% for anorexia nervosa and typically lower in those with the restricting subtype.27,28 Register-based studies29 confi rmed aggregation of autism spectrum disorder in probands with anorexia nervosa and in their relatives; however, the relation between anorexia nervosa and autism spectrum disorder seems to be non-specifi c.29
Advances in studies of comorbidity are emerging from the genetic literature with intriguing signifi cant positive genetic correlations emerging between anorexia nervosa and schizophrenia (rg=0·19)30 and between anorexia nervosa and obsessive-compulsive disorder (rg=0·55).31 These methods have taken us one step beyond reporting the frequency with underlying mechanisms of co-occurrence—in this case, by identifying shared genetic factors.
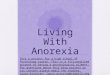
Patients with anorexia nervosa display a broad variety of somatic complications in several organ systems (fi gure) across various stages of illness.32 In the acute state, patients with anorexia nervosa present with many common complaints such as dizziness, fatigue, or even a syncope.33 In patients with a chronic course, almost every organ system can be aff ected because of malnutrition or the presence of binge-eating and purging behaviour.34 Although changes in multiple endocrine axes are mostly adaptive (ie, to optimise energy expenditure),35 up to 21% of patients with anorexia nervosa have osteoporosis and more than 54% have osteopenia of the lumbar spine.36
Patients with anorexia nervosa have an increased life-time prevalence of autoimmune disease, most prominently type 1 diabetes.37 Type 1 diabetes often precedes the onset of anorexia nervosa, is associated with insulin purging, poor glycaemic control, diabetic complications, and very high mortality.38 In children with paediatric acute-onset neuropsychiatric syndrome (PANS) or paediatric autoimmune neuropsychiatric disorder associated with streptococcal infections (PANDAS), food restriction also occurs and has been deemed to be a variant of childhood onset anorexia nervosa.39
PrognosisRegarding the core anorexia nervosa-psychopathology, Steinhausen and colleagues21 analysed 119 studies covering 5590 patients with anorexia nervosa and reported that 59·6% of those patients showed a weight normalisation,
DSM-IV DSM-52
A A refusal to maintain bodyweight at or above a minimally normal weight for age and height (eg, weight loss leading to a maintenance of bodyweight less than 85% of that expected, or failure to make expected weight gain during period of growth, leading to bodyweight less than 85% of that expected).
A Restriction of energy intake relative to requirements, leading to a signifi cantly low bodyweight in the context of age, sex, developmental trajectory, and physical health. Signifi cantly low weight is defi ned as a weight that is less than minimally normal or, for children and adolescents, less than that minimally expected.
B Intense fear of gaining weight or becoming fat, even though underweight.
B Intense fear of gaining weight or of becoming fat, or persistent behaviour that interferes with weight gain, even though at a signifi cantly low weight.
C Disturbance in the way in which one’s bodyweight or shape is experienced, undue infl uence of bodyweight or shape on self-evaluation, or denial of the seriousness of the current low bodyweight.
C Disturbance in the way one’s bodyweight or shape is experienced, undue infl uence of body shape and weight on self-evaluation, or persistent lack of recognition of the seriousness of the current low bodyweight.
D In postmenarcheal females, amenorrhoea—ie, the absence of at least three or more consecutive menstrual cycles. (A woman is considered to have amenorrhoea if her periods occur only following hormone—eg, oestrogen administration).
D ··
DSM criteria were taken from the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental disorders. DSM-IV-TR, Fourth Edition. Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (Copyright ©2013). American Psychiatric Association. All Rights Reserved.
Table 1: Comparison of diagnostic criteria for anorexia nervosa according to DSM-IV versus DSM-5
ICD-1011 ICD-11 (proposed criteria)*
A Weight loss, or in children a lack of weight gain, leading to a bodyweight of at least 15% below the normal or expected weight for age and height.
A Signifi cantly low bodyweight for the individual’s height, age, and developmental stage (BMI less than 18·5 kg/m² in adults and BMI-for-age under fi fth percentile in children and adolescents) that is not due to another health condition or to the unavailability of food.
B The weight loss is self-induced by avoidance of “fattening foods”.
B Low bodyweight is accompanied by a persistent pattern of behaviours to prevent restoration of normal weight, which may include behaviours aimed at reducing energy intake (restricted eating), purging behaviours (eg, self-induced vomiting, misuse of laxatives), and behaviours aimed at increasing energy expenditure (eg, excessive exercise), typically associated with a fear of weight gain.
C A self-perception of being too fat, with an intrusive dread of fatness, which leads to a self-imposed low weight threshold.
C Low bodyweight or shape is central to the person’s self-evaluation or is inaccurately perceived to be normal or even excessive.
D A widespread endocrine disorder involving the hypothalamic-pituitary-gonadal axis, manifest in the female as amenorrhoea, and in the male as a loss of sexual interest and potency (an apparent exception is the persistence of vaginal bleeds in anorexic women who are on replacement hormonal therapy, most commonly taken as a contraceptive pill).
D ··
E Does not meet criteria A and B of bulimia nervosa (F50.2).
E ··
ICD criteria have been taken from the WHO International Statistical Classifi cation of Diseases.11 *Proposed ICD-11 criteria have been taken from ICD-11 Beta Draft. BMI=body-mass index.
Table 2: Comparison of diagnostic criteria for anorexia nervosa according to ICD-10 versus ICD-11 (proposed criteria)

www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9 3
Review
accompanied by a normalisation of menstrual status in 57·0%, and a normalisation of eating behaviour in 46·8% of the whole group of patients with anorexia nervosa. In general, patients with an illness onset before their 17th birthday achieve a better outcome than adult onset, whereas prepubertal onset confers a worse course.40 Long-term follow-up studies8,21 have confi rmed two broad outcome groups with either a good outcome or chronic course with a high risk of premature death. Regarding the time course, several follow-up studies have shown that at least in adult patients with full syndrome anorexia nervosa, time to complete remission is between 5 and 6 years.6
In a meta-analysis41 of excess mortality in the 1990s, anorexia nervosa was associated with the highest rate of mortality among all mental disorders.41 Another meta-analysis7 showed a crude mortality rate (number of deaths within the study population over a specifi ed period) of 5·1 deaths per 1000 person-years and the standardised mortality rate of 5·9 with a mean follow-up period of 14·2 years. Although most deaths due to anorexia nervosa are a direct consequence of starvation-related medical complications, particularly cardiac complications and severe infections, one in fi ve deaths in patients with this disorder results from suicide.9 Data for the course and outcome in male patients with anorexia nervosa are scarce; however, an older age and lower BMI at admission, and a purging subtype of anorexia nervosa led to an increased risk of death in male individuals with anorexia nervosa.42
PathogenesisGenetic factorsAnorexia nervosa is strongly familial43 and heritability estimates range from 28% to 74%.44 Two genome-wide association studies (GWAS),45,46 currently understood to be underpowered in view of the presumed genetic architecture of anorexia nervosa, predictably did not detect genome-wide signifi cant loci. Boraska and colleagues45 conducted sign tests to compare results from the discovery sample with those from the replication sample, and 76% of the results from the replication sample were in the same direction as the discovery sample, a result highly unlikely to be due to chance (p=4 × 10–⁶). This observation strongly suggests that true fi ndings exist and that an increase of the sample size will yield signifi cant results; the fi eld is currently accruing larger samples. A study30 reported a signifi cant negative genetic correlation between anorexia nervosa and BMI and a signifi cant positive genetic correlation between anorexia nervosa and schizophrenia, encouraging a deeper exploration of metabolic factors in anorexia nervosa and a new genetic association between anorexia nervosa and schizophrenia.
Neurobiological factorsMost neurobiological studies have been done in currently ill or recovered patients, thus abnormalities might result from state-related consequences of malnourishment or so-called scarring.
Neurocognition and social cognitionNeurocognitive markers of anorexia nervosa include set shifting diffi culties (ie, diffi culties switching between diff erent tasks or task demands)47 and poor central coherence (ie, a preference for local [detail-focused] over global [bigger picture] processing).48 These impairments have also been noted in unaff ected sisters of people with anorexia nervosa and to some extent persist after recovery.49 Evidence suggests that both illness stage or duration and severity aff ect performance.50 People with anorexia nervosa also have diffi culties in socio-emotional processing, showing attentional biases, impaired emotion recognition, regulation, and expressivity, and poor theory of mind.51 These diffi culties are present both in the ill state and in muted form after recovery. Prospective longitudinal studies of children with a high familial risk of eating disorders suggest that some neuro-cognitive and social cognitive vulnerabilities are present from an early age.52
Structural neuroimagingPatients with acute anorexia nervosa have been reported to have global reductions in grey and white matter, increased cerebrospinal fl uid and regional grey matter decreases in the left hypothalamus, and in reward-related regions of the basal ganglia and the somatosensory cortex.53 Studies in patients who recovered from anorexia nervosa and longitudinal studies (before and after treatment) suggest that brain tissue abnormalities might recover with weight regain.54,55 Many earlier structural studies have methodological limitations (eg, not correcting for age or
Figure: Impaired organ function in anorexia nervosa
Organ systems or organ Pathological findings Leading systems
CNS
Dental system and parotis glands
Endocrine system and reproductive function
Cardiovascular system
Gastrointestinal tract
Haematological and immune system
Renal tract
Bone
Morphological and functional cerebral changes; volumereduction in cerebral greyand white matter
Impaired dental status, dental caries, increased serum amylase
Hypothalamus-pituritary-gonadal-axis, low T3 syndrome, hypercortisol
Hypotension, bradycardia,arrhythmia
Impaired gastric emptying, gastric dilation, gastro-duodenal ulcers
Bone marrow hypoplasia, anaemia with reduced leucocytes and immunoglobulin
Hypokalaemia, hypophosphataemia,hypernatraemia
Reduced bone density (osteopenia)or osteoporosis
Cognitive deficits
Dental caries,enlargement of theparotid glands
Amenorrhoea in women,symptoms of hypothyroidism , depression, elevated stress levels
Syncope
Constipation, ileus, uppergastrointestinal bleeding
Anaemia, (bacterial)infections, compromisedimmune competence
Nephrolithiasis, oedema,syncope
Bone fractures and concomitant pain, spinal compression
oooooonnnnnnnnnnn,
For the ICD-11 Beta Draft see http://apps.who.int/classifi cations/icd11/browse/l-m/en

4 www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9
Review
overall brain volume, not taking anorexia nervosa-subtype or comorbidities into account; results being confounded by eff ects of dehydration or starvation). A series of studies by Frank and colleagues56,57 addressing these limitations reported increased grey matter volume of the medial orbitofrontal cortex gyrus in both adolescents and adults with anorexia nervosa, which persisted into recovery. Similar changes were found in bulimia nervosa, whereas obese adults showed reduced orbito frontal cortex gyrus rectus volume. The orbito frontal cortex assesses quality and value of reward stimuli, such as food, and is implicated in regulating sensory-specifi c satiety. Additionally, participants with anorexia nervosa had increased right insula grey matter compared with controls. The right anterior insula is associated with self-recognition and interoceptive awareness. Longitudinal studies in at-risk populations are needed to fully assess whether these changes are biomarkers of the illness.
Functional neuroimagingStudies using visual food cue models have found diff erences between anorexia nervosa and controls in prefrontal areas and in limbic and paralimbic circuits, associated with salience and reward processes with some inconsistences between studies due to methodological diff erences.58 Findings from studies56,57 using taste stimuli to assess neural processing of food reward show that people who recovered from anorexia nervosa have a reduced functional brain response to predictably given, but an increased response to unpredictably given, sugar solutions with insula, striatum, or orbitofrontal cortex response distinguishing anorexia nervosa from controls. The same authors, contrasted people with anorexia nervosa, bulimia nervosa, or obesity who underwent a dopamine-related conditioning task (unexpected receipt or omission of sweet taste) and found greater activation of the ventral striatum, insula, and frontal cortex in patients with anorexia nervosa than in healthy controls, but lower activation in patients with bulimia nervosa and obesity, suggesting that people with anorexia nervosa are highly sensitive to uncertainty (unpredictable reward).
Neuroimaging studies of body-image disturbance in anorexia nervosa suggest that this is a multidimensional construct, with the posterior parietal network related to a perceptive component and the prefrontal cortex-insula-amygdala network related to an aff ective component of body-image distortion in anorexia nervosa.59
In summary, these symptom provocation models have largely suggested aberrant functioning of subcortical regions promoting so-called bottom-up (stimulus-driven) responses—ie, in parietal somatosensory regions, anxiety-related mesolimbic circuits, and reward-related regions (eg, striatum)—and in so-called top-down (evaluative) prefrontal regions implicated in executive control.60 These fi ndings provide important pointers towards targets for neurobiologically informed treatments.
Neurobiological models of anorexia nervosaBased on these neuroimaging fi ndings, and integrating additional evidence from studies on cerebrospinal fl uid (CSF) measures of metabolites, PET, and SPECT brain imaging studies, Kaye and colleagues61,62 suggest that some childhood temperamental and personality traits, such as anxiety, obsessions, and perfectionism might refl ect neurobiological risk factors for the development of anorexia nervosa. Restrictive eating thus might be a means of reducing negative aff ect caused by imbalance between serotoninergic (aversive or inhibitory) and dopaminergic (reward) systems. Other neurobiologically informed models of anorexia nervosa have highlighted the role of stress, fear, and anxiety,63 the rewarding nature of anorexia nervosa symptoms,64 and the subsequent shift to compulsive or habitual behaviours65,66 as key factors in the persistence of the illness.
Developmental factorsSeveral adverse experiences occurring around universal stages and transitions of development are associated with an increased prevalence of anorexia nervosa. These developmental risk factors include adverse prenatal, perinatal, and neonatal events, such as dysmaturity or prematurity67,68 as well as feeding and sleeping diffi culties in infancy.68 Throughout childhood, emerging personality traits associated with anxiety, depression, perfectionism, and autism spectrum68 have been identifi ed as risk factors for anorexia nervosa. Puberty and adolescence are characterised by profound changes, vulnerabilities, and the transition to adulthood, and they represent the period of fi rst onset of anorexia nervosa. A possible explanation for the crucial role of puberty for the onset of anorexia nervosa might lie in hormonal changes and dysregulations that interact with neurotransmitter functioning, brain maturity, and genetic factors.69
Environmental factorsFemale gender has consistently been shown to be a risk factor for anorexia nervosa.68 The increase of anorexia nervosa in low-income and middle-income countries suggests that cultural transitions associated with industrialisation, urbanisation, and globalisation might be associated with environmental risk constellations for the development of anorexia nervosa.9 These con stellations might include the adoption of the so-called western lifestyle, including nutritional habits and thin ideal internalisation. However, although body dissatis faction has been identifi ed as a risk factor for the development of any eating disorder,70 risk factors associated with thin ideal internalisation and associated sociocultural pressures have not been confi rmed for anorexia nervosa. Appraising the potential infl uence of environmental factors, it has to be taken into account that the incidence of anorexia nervosa is relatively low worldwide despite these pervasive sociocultural pressures to be thin.71 It is possible that these western infl uences could simply increase the number of

www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9 5
Review
individuals who engage in behaviours such as strict dieting or excessive exercise, which can then trigger eating disorders in genetically susceptible individuals.
TreatmentInitial assessment and investigationsInitial assessment of the patient with anorexia nervosa includes an in-depth interview, a physical examination, and investigations to establish severity and nature of eating disorder symptoms and diagnosis, comorbid psychological and physical symptoms, diagnoses and risk, past treatments, current motivation for treatment, and available supports. An early task is to build good rapport with the patient, as they are often highly ambivalent about and fearful of treatment.72 Whenever possible, it is important to involve signifi cant others (family, partners) in assessment and subsequent treatment. Table 3 summarises recommended physical investigations to be done at assessment. We have also formulated indicators of high risk, requiring rapid intensive specialist consultation and intervention (panel 1).
Pathways (levels) of careA Finnish epidemiological study74 reported that about 50% of people with anorexia nervosa in the community do not access treatment. Those who do engage in treatment typically show varying degrees of ambivalence about change.75 However, with treatment, at least 40% of people with anorexia nervosa (and more in younger samples) will make a full recovery.21 Additionally, access to care from a specialist service with expertise in anorexia nervosa might be associated with better outcomes.76
Thus it is important that health-care practitioners at all levels are competent to identify anorexia nervosa and that there is early access to secondary and tertiary levels of care. This early access is particularly important in view of evidence that there is a critical window for eff ective intervention in the early stages of illness (ie,
duration of <3 years) beyond which full recovery becomes much more diffi cult to achieve.77 Despite this critical window, there should not be therapeutic nihilism in those who develop severe and enduring anorexia nervosa and have a very high risk of disability or death. Findings from a randomised trial of outpatient psychotherapy15 supported the effi cacy of modifying psychological approaches in longstanding illness such that the focus shifts from weight regain and recovery to improved quality of life.
Essential Optional
Medical and psychiatric history Full examination Structured diagnostic interview (eg, SCID I and II, EDE)
Physical assessment BMI, heart rate, blood pressure, temperature In case of severe oedema: albumin, total protein, protein electrophoresisIn patients with a long-term course: bone density (DEXA) scanIn case of seizures or diff erential diagnosis: EEG and neuroimaging (CT, MRI)In case of unclear thoracic pain or abdominal symptoms: chest radiograph, abdominal ultrasound, gastroscopy
Blood profi le Full blood count, blood sedimentation rate In severe anaemia: reticulocytes, iron, ferritin, transferring, vitamin B12
Biochemical profi le Sodium, potassium, calcium, magnesium, phosphate, creatinine, urea, liver enzyme profi le, blood glucose
In case of elevated creatinine: creatinine clearanceIn case of low BMI (<12kg/m²) and in the early phase of nutritional rehabilitation: monitoring of sodium, potassium, phosphate (at least weekly)
Cardiovascular assessment ECG In case of cardiovascular abnormalities: Holter ECG, echocardiography
SCID I and II=structured clinical interview for DSM axis I and II disorders. EDE=eating disorder examination interview. BMI=body-mass index. DEXA=dual-energy X-ray absorptiometry. ECG=electrocardiograph.
Table 3: Investigations recommended at initial assessment, on admission, or at regular intervals over the course of refeeding
Panel 1: Indicators of high medical risk and other reasons for considering inpatient treatment
Weight• BMI <14 kg/m² or rapid weight loss (adults) or <75% of
expected bodyweight or rapid weight loss (adolescents)
Medical status• Heart rate <50 bpm• Cardiac arrhythmia• Postural tachycardia (increase >20 bpm)• Blood pressure <80/50 mm Hg• Postural hypotension >20 mm Hg• QTc >450 ms• Temperature <35·5°C• Hypokalaemia <3·0 mmol/L• Neutropenia• Phosphate <0·5 mmol/L
Additional indicators • Severe bingeing and purging (eg, several times daily)• Failure to respond to outpatient or daypatient treatment• Severe psychiatric comorbidity• Suicidality
These indicators are only a guide and do not replace the need for individual clinical judgement (adapted from Hay and colleagues, 2014,73 and Treasure and colleagues, 20104). QTc=corrected QT.

6 www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9
Review
Practice guidelines (eg, from the American Psychiatric Association,2 the German College for Psychosomatic Medicine,78 the National Institute for Health and Care Excellence,79 and the Royal Australian & New Zealand College of Psychiatrist73) agree that most people with anorexia nervosa can be treated as outpatients but that day-patient and inpatient services are needed for those with more severe illness and those who do not improve with outpatient care. Brief inpatient care followed by intensive outpatient care could achieve similar effi cacy to that of longer hospital stays in adolescents,80 but there is a paucity of randomised trials to guide service use.
In a multicentre randomised trial, Herpertz-Dahlmann and colleagues81 reported that a stepped care approach (day-patient treatment after short inpatient care) was equally eff ective and less costly than inpatient treatment in patients with non-chronic adolescent anorexia nervosa at the end of treatment and at 1 year follow-up.
Evidence-based psychological treatment in adolescent and adult patientsBased on comprehensive systematic reviews4,82,83 and complemented by well designed and suffi ciently powered treatment studies, we have reported on the fi rst-line behavioural treatments for adolescent and adult patients with anorexia nervosa separately (table 4) and have supplemented this by interventions for relapse prevention and aftercare as well as specifi c interventions for carers. Additionally, we have added information (panel 2) on the setting, structure, and content of
psychotherapeutic interventions applied in randomised trials since 2010.
First, the overall evidence base for the treatment of adolescent patients with anorexia nervosa is increasing. However, the number of empirically supported psychosocial treatments trials opposed to the number of treatments for adolescent anorexia nervosa remains scarce. In total, 12 randomised trials (n=1060 patients) have compared diff erent psychological treatments in adolescent patients with the disorder (age <19 years). Lock84 concluded in a systematic review on psychological treatments in children and adolescents that there is clear and growing evidence to support the effi cacy of family treatment in adolescent anorexia nervosa compared with individually based approaches, and that there is evidence that supports family-based treatment (FBT) with a focus on eating disorder behaviour and weight gain as opposed to more general family processes.
Second, over the past 30 years, 12 randomised trials (n=1157 patients) comparing diff erent psychological treatments in adult patients with anorexia nervosa (age >18 years) have been done in outpatient settings. Since the 2010 review,4 several well designed and suffi ciently powered treatment studies for adult patients with anorexia nervosa have been published, reporting substantial weight gain and clear improvements of eating disorder and general psychopathology at the end of treatment and at follow-up.15,85–90 The largest of these trials (n=242) compared three diff erent fi rst-line treatments: focal psychodynamic psychotherapy (FPT), enhanced cognitive behaviour therapy (CBT-E), and an optimised treatment as usual, including psychotherapy as well as medical care by the family doctor.87 Weight gain was similar in all three groups. Considering a combined outcome (weight and eating disorder psychopathology), FPT proved advantageous in terms of recovery at 12-month follow-up, whereas CBT-E was more eff ective with respect to speed of weight gain and improvements in eating disorder psychopathology than the other treatments. Results from one trial (n=56)91 showed that by the end of treatment, an intervention that combined supportive therapy with sound clinical management delivered by eating disorder specialists (specialist supportive clinical management, SSCM) was superior to two specifi c psychotherapies (cognitive behavioural therapy [CBT] and interpersonal psychotherapy [IPT]). However, a long-term follow-up of this trial did not support the superiority of any treatment.92 Findings from another randomised trial15 (n=63) showed that patients with anorexia nervosa with severe and enduring course can make meaningful improvements with both CBT or SSCM.15 A novel anorexia nervosa-specifi c outpatient therapy (Maudsley model of anorexia nervosa therapy for adults, MANTRA) has been compared against SSCM in two trials (n=214).85,86 Although overall outcome did not diff er between groups, patients preferred MANTRA to SSCM, and patients with a more severe illness had a greater weight gain in the MANTRA group than in the
Evidence Eff ect (evidence level)
Adolescent anorexia nervosa84
Family-based treatment (FBT) Strong* +++ (1)
Maudsley family therapy (MFT) Strong* +++ (1)
Family system therapy (FST) Moderate* ++ (2)
Adolescent focused therapy (AFT) Moderate* ++ (2)
Cognitive behavioural treatment (broad; CBT-b) Weak/moderate –/+ (4)
Cognitive behavioural treatment (enhanced; CBT-E) Moderate* + (4)
Adult anorexia nervosa4,73,83
Cognitive behavioural therapy (CBT) Weak +
Cognitive behavioural therapy (enhanced; CBT-E) Moderate* ++
Behavioural therapies (BT) Weak –/+
Interpersonal psychotherapy (IPT) Weak +
Psychodynamic therapy (PT) Weak +
Cognitive analytic therapy (CAT) Weak +
Focal psychodynamic psychotherapy Moderate* ++
Maudsley model of anorexia nervosa treatment for adults (MANTRA) Moderate* ++
Specialist supportive clinical management (SSCM) Moderate* + (+)
Evidence grades are weak, moderate, or strong. Eff ect grades are: – for no benefi cial eff ect; -/+ for mixed result or still inconsistent result; + for slight benefi cial eff ect; +(+) for moderate benefi cial eff ect; ++ for moderate and lasting benefi cial eff ect (further improvement shown in follow-up); and +++ for strong benefi cial eff ect (superiority demonstrated in primary outcome of randomised trial). Evidence levels are: 1 for well established, 2 for probably effi cious, and 4 for experimental. *At least one multicentre randomised trial or more than one randomised trial.
Table 4: Behavioural treatments in adolescent and adult patients with anorexia nervosa

www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9 7
Review
Panel 2: Novel and eff ective psychological treatments in anorexia nervosa
Family-based treatment (FBT)Family-based treatment is a three-phase treatment for adolescent patients with anorexia nervosa and their families over 16 1-h sessions and a 9-month period (initially of 10 h during 6 months). In the fi rst phase, therapy is characterised by attempts to absolve the parents from the responsibility of causing the disorder and by complimenting them on the positive aspects of their parenting. Families were encouraged to work out for themselves how best to help restore the weight of their child with anorexia nervosa. In phase 2, parents were helped to transition eating and weight control back to the adolescent in an age-appropriate manner. The third phase focused on establishing a healthy relationship between the adolescent and the parents. 24 1-h sessions were provided over the 1-year period (Lock and colleagues, 2010 and Agras and colleagues 2014; appendix).
Specialist supportive clinical management (SSCM)This treatment should be delivered by therapists specialised in the treatment of eating disorders and should provide a standardised form of usual outpatient treatment. Patients with anorexia nervosa and a BMI of 15 kg/m² or lower receive up to 30 once-weekly individual therapy sessions and four monthly follow-up sessions. In those patients with a BMI >15kg/m² the number of sessions could be reduced to 20. It combines clinical management (ie, giving information, advice, and encouragement) with a supportive therapeutic style designed to build a positive therapeutic relationship and to foster change. Therapy content includes assessment, identifi cation, and regular review of target symptoms; psychoeducation; monitoring of physical status; establishment of a goal weight range; and nutritional education and advice. The aim is to help patients make a link between their clinical symptoms and their abnormal eating behaviour and weight, and to support patients in a gradual return to normal eating behaviour and weight. Additional therapy content is determined by the patient (McIntosh and colleagues 2006, appendix).
Maudsley model of anorexia treatment for adults (MANTRA)This treatment is an empirically based cognitive-interpersonal treatment, which proposes that four broad factors, linked to underlying obsessional and anxious (or avoidant) personality traits, are central to the maintenance of anorexia nervosa. These are (1) a thinking style characterised by infl exibility, excessive attention to detail, and fear of making mistakes; (2) impairments in the socio-emotional domain (eg, avoidance of emotional experience, regulation, and expression); (3) positive beliefs about how anorexia nervosa helps the person in their life; and (4) unhelpful responses of close others (eg, overinvolvement, criticism, accommodation to symptoms). These factors are targeted in treatment with the aim of improving weight, eating disorder and other symptoms, and psychosocial adjustment. The treatment style is motivational. Treatment is centred around a patient-manual. This manual has core (eg, formulation) and optional modules (eg, module on building a so-called non-anorexic identity). Treatment has a clear structure and hierarchy of
therapeutic procedures. Individual tailoring of treatment arises from fl exibility on how modules are combined and how much emphasis they are given. Nutrition and other symptom management or behaviour change, information or advice is given if the patient is motivationally ready for this. Diff erences from other treatments include that the model was developed specifi cally for anorexia nervosa, it is based on biological and psychological research, and is tailored to characteristic temperamental traits in this disorder. It is unique in its use of a patient workbook, developed in co-production with patients and therapists. It is also unique in its involvement of carers in both the model or formulation and the treatment. Separate carer materials based on the model are available (Schmidt and colleagues, 2015, appendix).
Enhanced cognitive behaviour therapy (CBT-E)According to Fairburn and colleagues CBT-E is the abbreviation for “enhanced cognitive therapy”, and it refers to a “transdiagnostic” personalised psychological treatment for eating disorders. It was developed as an outpatient treatment for adults but is an intensive version for day patient and inpatient settings, and a version for younger people. As an outpatient therapy treatment CBT-E has four stages and is available in a short (20 sessions) and longer version (40 sessions). In stage one, the focus is on gaining a mutual understanding of the person’s eating problem and helping him or her modify and stabilise their pattern of eating. In the brief second stage progress is systematically reviewed and plans are made for the main body of treatment. Stage three focused on the processes that are maintaining the person’s eating problem (eg, addressing concerns about shape and eating). In the last stage the emphasis shifts onto the future. There is a focus on dealing with setbacks and maintaining the changes that have been obtained (Fairburn, 2008; appendix).
Focal psychodynamic psychotherapy (FPT)The initial manualised treatment was designed as a 40 h outpatient psychodynamic-oriented psychotherapy for moderately ill patients with anorexia nervosa (BMI >15 kg/m²). At the beginning of focal psychodynamic therapy, the therapist identifi es psychodynamic relevant foci using a standardised operationalised, psychodynamic diagnostic interview (OPD-II). The psychodynamic treatment manual can be divided roughly into three treatment phases. The fi rst phase focuses mainly on therapeutic alliance, pro-anorectic behaviour and ego-syntonic beliefs (attitudes and behaviour viewed as acceptable), and self-esteem. In the second phase of treatment, main focus is placed on relevant relationships and the association between interpersonal relationships and eating (anorectic) behaviour. The pertinent aspects of the fi nal phase are the transfer to everyday life, anticipation of treatment termination, and parting. Before every treatment session the patient’s weight is assessed and documented (Friederich and colleagues, 2014).
This panel describes eff ective psychological treatments applied in randomised trials (table 4, including those treatment approaches shown the highest evidence and eff ectiveness for adolescents and adults and published as randomised trials since the 2010 review by Treasure and colleagues 20104). For references see appendix.
For more on CBT-E see http://www.credo-oxford.com

8 www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9
Review
SSCM group. In summary, although the evidence base for the treatment of adults with anorexia nervosa is advancing, thus far no specifi c approach has shown clear superiority. Across diff erent individual psychotherapies for adults with anorexia nervosa there are common elements. These elements include a psychotherapeutic approach specifi c to and focused on anorexia nervosa in combination with a focus on weight regain and nutritional rehabilitation.73
Third, few studies have focused on relapse prevention and aftercare in anorexia nervosa, and the little available evidence suggests that patients who have a structured intervention for relapse prevention—based on cognitive-behavioural principles—after inpatient treatment have fewer and later episodes of relapse in anorexia nervosa during the fi rst year after inpatient discharge than do patients without a follow-up intervention.93–95
Finally, in view of the burden of anorexia nervosa on families and partners, and evidence suggesting that carers’ distress and behaviours might inadvertently maintain the illness, several randomised trials have also trialled interventions targeting carers of adults with anorexia nervosa. A new couple-based intervention for anorexia nervosa (Uniting Couples in the Treatment of Anorexia Nervosa)96 also focuses on leveraging the support of close others in the treatment of anorexia nervosa. These studies show that carer outcomes (distress and unhelpful behaviours) can be improved and that this improvement in turn might positively aff ect relationships with the patient and patients’ clinical outcomes.97,98
Pharmacological treatmentsSystematic reviews consistently conclude that antidepressants neither improve weight gain99 nor reduce eating disorder or other psychological symptoms in the re-feeding phase.99 The utility of antidepressants for relapse prevention in the post-weight restoration phase remains uncertain.99 This mixed evidence is based on two trials, one smaller positive trial and a second larger trial that tested the effi cacy of adding fl uoxetine to CBT on post-weight restoration and found no added benefi t in preventing relapse at 1 year (for references on single trials see appendix). A pooled meta-analysis of four placebo-controlled randomised trials on antidepressants (two on a tricyclic and two of fl uoxetine) and a relapse prevention trial also failed to fi nd a signifi cant eff ect on weight gain.100 As a consequence, treatment guidelines73 are cautious in recommending use even for comorbid features such as depression until it is established that these features are not due to the starvation state and remit with weight restoration.
The review on eating disorders by Treasure and colleagues4 reported emerging evidence for the use of olanzapine, an atypical antipsychotic in reducing illness preoccupations and anxiety during refeeding. The inconsistent results and inability to achieve signifi cance in pooled meta-analyses of placebo controlled trials for weight gain100–102 have led to a consensus in the medical
literature that more, larger, and consistently positive trials of antipsychotics are needed before their use can be recommended.99,100
There has been little advance in evidence for any other psychotropic medication in anorexia nervosa treatment since the review by Treasure and colleagues.4 Other drugs that are currently under investigation for a putative role in anorexia nervosa treatment are tumour necrosis factor, dronabinol (a cannabinoid receptor agonist), and ghrelin agonists103 to promote appetite or antagonists to reduce hyperactivity (for references on single trials see appendix). These drugs do not have an evidence base for their use at this stage.
Nutritional treatmentsIn moderately ill outpatients with anorexia nervosa, nutritional counselling alone is not an adequate treatment;94 however, dieticians are an important part of a multidisciplinary treatment team. Patients who are substantially underweight and malnourished should be admitted to a specialist inpatient or day-patient eating disorder unit for a combined programme of supervised refeeding and anorexia nervosa-related psychotherapy. First, it is important to accurately assess nutritional and fl uid intake and to document premorbid weight and the course of weight loss. Depending on the duration of weight loss and malnutrition, age of the patient, somatic comorbidity, and the severity of purging behaviour, recommended weight gain rates range from 500 g to 1400 g per week.73,79 Evidence exists that substantial weight gain is best achieved in inpatient settings,104 particularly in patients with increased somatic risk. Refeeding syndrome is a serious and potentially fatal medical complication, particularly during the early stages of refeeding in those patients at the highest risk, who have been malnourished and emaciated for a long time.27,79 Due to a switch from fasting gluconeogenesis to carbohydrate-induced insulin release, there is a rapid intracellular uptake of potassium, phosphate, and magnesium with the consequence of a rapid onset of hypophosphataemia, hypomagnesia, and hypo-kalaemia.105 In accordance with the RANZP protocol (2014),73 adult patients with anorexia nervosa should start with a refeeding of 6000 kJ/day, increased by 2000 kJ/day every 3 days, until an adequate intake to meet the person’s needs for weight restoration is reached. As a consequence, particularly in the early phase of refeeding, electrolytes should be regularly monitored and this diet should be supplemented by phosphate at 500 mg twice daily and thiamine at least 100 mg daily for the fi rst week, and thereafter as clinically indicated for people at high risk of refeeding syndrome (eg, those with BMI <13). Nutritional therapy includes supervised meals and, if necessary, additional high-protein oral liquid supplements. In severely emaciated patients at high medical risk, nasogastric feeding, including professional and supportive supervision, could be indicated. On very
See Online for appendix

www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9 9
Review
rare occasions and after failure of the above nutritional strategies, parenteral nutrition might be indicated. In adolescent patients with a short duration of illness, a more rapid refeeding protocol can be applied. In principle, the least intrusive and most physiological normal method of nutrition should be applied.73
Osteoporosis prevention and treatmentThe most effi cient strategy to improve bone density is to restore weight and, in women, menstrual function. Oestrogen-replacement therapy, primarily via transdermal application, only partially increases bone density in adolescents.35 Oral oestrogen-progesterone combinations are ineff ective in increasing bone mineral density in adolescent and adult anorexia nervosa patients.106 Moreover, neuroendocrine changes can have a direct eff ect on neurocognition and mood as well as on core eating disorder psychopathology.35
Experimental treatments There is widespread agreement that new interventions are needed to improve outcomes, especially in adults with anorexia nervosa. Such interventions should target specifi c disease mechanisms.107,108 We describe some of the more promising experimental treatments.
Psychobiological treatmentsCognitive remediation therapy (CRT) for anorexia nervosa targets neuropsychological ineffi ciencies in executive functioning, chiefl y poor set-shifting and weak central coherence (extreme attention to detail at the expense of the bigger picture). Two systematic reviews109,110 identifi ed four small to medium sized (n=32–82 participants) randomised trials of CRT (for references on single trials see appendix). These studies varied in populations, intensity of CRT (8–30 sessions), comparison treatments (CBT, treatment as usual, exposure treatment, non-specifi c neurocognitive training), and primary outcomes (eating disorder symptoms, test meal consumption, set-shifting, treatment dropout). Therefore no meta-analysis was possible. Two studies found diff erential short-term improvements in neurocognition for CRT versus comparison treatment. One trial of CRT plus treatment as usual versus treatment as usual alone in inpatients with either anorexia nervosa or bulimia nervosa found greater improvement in quality of life at end of treatment and greater improvement on eating disorders symptoms at 6 months follow-up in the group containing CRT than in the TAU alone group. These fi ndings are promising but well designed large-scale studies of CRT are as yet not available.
Abnormalities in fear conditioning have been thought to be causally implicated in anorexia nervosa. In line with this thought, exposure therapy (to food or body stimuli) might be another promising treatment for anorexia nervosa. One systematic review111 identifi ed one
placebo-controlled randomised trial (n=14) of food exposure and D-cycloserine (DCS) in anorexia nervosa, based on evidence that DCS enhances fear extinction during exposure therapy in anxiety disorders (for references on single trials see appendix). DCS compared with placebo had no eff ect in any of the training or test meals. One further randomised trial (n=32) compared food exposure with CRT in weight-restored anorexia nervosa and found greater test-meal consumption at end of treatment in the exposure treatment group.
Other promising psychobiological treatments include cognitive bias modifi cation treatments,112 based on converging evidence suggesting a range of cognitive biases (attention, memory) in relation to illness-relevant and emotional stimuli in anorexia nervosa. However, randomised trials are so far not available.
Neurobiological treatmentsImproved understanding of the neurocircuitry involved in anorexia nervosa113 has given rise to the use of neuromodulation treatments, such as deep brain stimulation (DBS), repetitive transcranial current stimu-lation (rTMS), and transcranial direct current stimulation (tDCS), especially in severe and enduring anorexia nervosa. We identifi ed two systematic reviews114,115 summarising cases studies and three further case studies describing use of these techniques (for references on single trials see appendix). As yet, no randomised trials of therapeutic use of neuromodulation treatments have been published. Several cases studies or series of DBS (nucleus accumbens, ventral capsule or ventral striatum, or subcallosal cingulate cortex) targeting anorexia nervosa symptomatology directly (n=12) or targeting obsessive-compulsive disorder or depression with parallel improvements in anorexia nervosa symptoms (n=2) have been identifi ed. These studies suggest that DBS might have promise in highly selected severe and enduring cases. Likewise, rTMS (DLPFC) or tDCS (anodal, DLPFC) case studies (n=13) have shown promise in enduring anorexia nervosa.
Evidence-based prevention programmesPrevention eff orts can be divided into universal, selective, and indicated, depending on whether they address the general population or populations with increased risk (eg, children of eating disordered mothers; elite athletes) or those exhibiting early signs of a disorder. Eating disorder prevention has focused on either risk factors (eg, body dissatisfaction) or eating disorder pathology or caseness. A systematic review116 of eating disorders prevention programmes for young people between the ages of 12 and 25 years identifi ed six reviews and 46 universal prevention trials, with psychoeducation the most commonly tested intervention (26 trials).116 The review also identifi ed six reviews and 40 trials in at-risk populations, where psychoeducation and cognitive dissonance programmes were equally common (12 each).

10 www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9
Review
Meta-analyses of controlled trials from other reviews were summarised as indicating that “prevention programmes generally produce large eff ects on outcomes related to eating disorder knowledge, and only small net eff ects for other important prevention targets such as reducing exhibited risk factors, changing attitudes, and reducing eating pathology”.116 The review also found that larger eff ect sizes are usually seen for studies of at-risk populations and interactive programmes using multi-session formats.
Other systematic reviews117 have specifi cally examined school-based interventions,118 e-health interventions, and the role of parental involvement119 in eating disorders and body dissatisfaction prevention programmes for children and adolescents, suggesting that these settings and ways of delivery are fruitful avenues to explore in future studies.
ConclusionsThe past 5 years have seen substantial advances in the knowledge of anorexia nervosa. Recent treatment studies suggest that patients with anorexia nervosa have a realistic chance of recovery, especially if treated early, or at least, to achieve substantial improvement. However, there is widespread agreement that several challenges remain in the management of anorexia nervosa (panel 3) and new interventions are needed to improve outcomes, especially in adults with the disorder. Such interventions should target specifi c disease mechanisms. The neuro-psycho logical constructs introduced within the research domain criteria (RDoC) matrix off er a new systematic basis for determining the neural substrates underlying the biological predisposition to anorexia nervosa.120 A clearer understanding of how anorexia nervosa behaviour is encoded in neural circuits would provide a key for developing more eff ective treatments. To conclude, we still need to discover how to provide better, faster, and lasting improvements in the management of this enigmatic disorder.ContributorsAll authors contributed to the search and selection of the medical literature and to the writing of the Review.
Declaration of interestsCB is a grant recipient from Shire Pharmaceuticals and an author for Pearson and Walker. PH receives royalties or honoraria for works on eating disorders from BMJ Publishing House, Hogrefe & Huber, and McGraw Hill.
AcknowledgmentsWe thank the anonymous reviewers for their comments on early drafts of this Review.
References1 Zipfel S, Mack I, Baur LA, et al. Impact of exercise on energy
metabolism in anorexia nervosa. J Eat Disord 2013; 1: 37.2 American Psychiatric Association. Diagnostic and statistical manual
of mental disorders: DSM-5. Washington, DC: American Psychiatric Association; 2013.
3 Gümmer R, Giel KE, Schag K, et al. High levels of physical activity in anorexia nervosa: a systematic review. Eur Eat Disord (in press). DOI:10.1002/erv.2377.
4 Treasure J, Claudino AM, Zucker N. Eating disorders. Lancet 2010; 375: 583–93.
Search strategy and selection criteria
We searched PubMed for articles published between Jan 1, 2010, and Dec 31, 2014, covering the time period since the review by Treasure and colleagues,4 published in The Lancet. We combined the search term “anorexia nervosa” each with “chronicity”, “comorbidity”, ”epidemiology“, “prognosis”, or “mortality”, “risk factor” or “maintaining factor”, “treatment” or “psychotherapy” or “pharmacological”, “prevention”. We narrowed the search to titles and abstracts. We used no language restriction. From the identifi ed 4612 publications, due to space considerations, we mainly cited selected landmark studies, review articles, and meta-analyses. We additionally selected earlier landmark studies we judged as relevant.
Panel 3: Key unmet challenges in the management of anorexia nervosa
Adolescents with anorexia nervosa• Which factors are essential to identify patients at risk and how could we address this
target group with adequate and eff ective prevention programmes?• What are the predictors, moderators, and mediators of outcome in the treatment of
adolescent patients with anorexia nervosa?• What to do when family-based treatment is unsuccessful or inappropriate
(eg, if there is substantial intrafamilial abuse)?
Adults with anorexia nervosa• How can we improve treatment outcomes–ie, what works and for whom and in what
setting?• What is the best fi rst-line outpatient treatment? • What treatments should be used as second-line treatments?• How important is it to involve family members and partners in treatment?• How can we prevent relapse after inpatient or day-patient treatment?
Across the age range• What brain circuits are involved in the onset and maintenance of anorexia nervosa?
• Which structures are implicated for which subtypes of anorexia nervosa? • Are there imaging markers to identify treatment responders and non-responders?
• In view of the typical age of onset of anorexia nervosa, does it make sense to have separate adolescent and adult eating disorder services or should there be seamless services across the ages?
• How should treatment and treatment goals be adjusted for diff erent stages of illness?• What is an adequate course of treatment for anorexia nervosa? • How should treatment resistance and palliative care be defi ned?
• How can we help the subgroup of patients with severe hyperactivity?
Treatment of comorbidities (psychiatric or physical)• How can we reduce mortality and suicide in individuals with anorexia nervosa? • How can we help the subgroup of patients with severe psychiatric comorbidities?
• What is the treatment for patients suff ering from comorbid post-traumatic stress disorder, personality disorder, developmental disorders (eg, autism spectrum disorder), and alcohol or substance misuse?
• How can we help the subgroup of patients with a severe somatic comorbid disorder? • What is the treatment for patients with comorbidities such as diabetes mellitus or
infl ammatory bowel disease?• What is the optimum management of osteop enia and osteoporosis in anorexia
nervosa?• What is the treatment for patients with a comorbidity such as food-related allergy?

www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9 11
Review
5 Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003; 361: 407–16.6 Herzog W, Schellberg D, Deter HC. First recovery in anorexia nervosa
patients in the long-term course: a discrete-time survival analysis. J Consult Clin Psychol 1997; 65: 169–77.
7 Arcelus J, Mitchell AJ, Wales J, Nielsen S. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatry 2011; 68: 724–31.
8 Zipfel S, Löwe B, Reas DL, Deter HC, Herzog W. Long-term prognosis in anorexia nervosa: lessons from a 21-year follow-up study. Lancet 2000; 355: 721–22.
9 Smink FR, van Hoeken D, Hoek HW. Epidemiology of eating disorders: incidence, prevalence and mortality rates. Curr Psychiatry Rep 2012; 14: 406–14.
10 Stuhldreher N, Konnopka A, Wild B, et al. Cost-of-illness studies and cost-eff ectiveness analyses in eating disorders: a systematic review. Int J Eat Disord 2012; 45: 476–91.
11 WHO. International statistical classifi cation of diseases and related health problems (ICD-10). Geneva: World Health Organization, 1992.
12 Al-Adawi S, Bax B, Bryant-Waugh R, et al. Revision of ICD—status update on feeding and eating disorders. Adv Eat Disord 2013; 1: 10–20.
13 Attia E, Roberto CA. Should amenorrhea be a diagnostic criterion for anorexia nervosa? Int J Eat Disord 2009; 42: 581–89.
14 Treasure J, Stein D, Maguire S. Has the time come for a staging model to map the course of eating disorders from high risk to severe enduring illness? An examination of the evidence. Early Interv Psychiatry 2015; 9: 173–84.
15 Touyz S, Le Grange D, Lacey H, et al. Treating severe and enduring anorexia nervosa: a randomized controlled trial. Psychol Med 2013; 43: 2501–11.
16 Hay P, Girosi F, Mond J. Prevalence and sociodemographic correlates of DSM-5 eating disorders in the Australian population. J Eat Disord 2015; 3: 19.
17 Lucas AR, Crowson CS, O’Fallon WM, Melton LJ 3rd. The ups and downs of anorexia nervosa. Int J Eat Disord 1999; 26: 397–405.
18 Herpertz-Dahlmann B. Adolescent eating disorders: defi nitions, symptomatology, epidemiology and comorbidity. Child Adolesc Psychiatr Clin N Am 2009; 18: 31–47.
19 Steinhausen HC, Jensen CM. Time trends in lifetime incidence rates of fi rst-time diagnosed anorexia nervosa and bulimia nervosa across 16 years in a danish nationwide psychiatric registry study. Int J Eat Disord 2015.
20 Nicholls DE, Lynn R, Viner RM. Childhood eating disorders: British national surveillance study. Br J Psychiatry 2011; 198: 295–301.
21 Steinhausen HC. The outcome of anorexia nervosa in the 20th century. Am J Psychiatry 2002; 159: 1284–93.
22 Fernandez-Aranda F, Pinheiro AP, Tozzi F, et al. Symptom profi le of major depressive disorder in women with eating disorders. Aust N Z J Psychiatry 2007; 41: 24–31.
23 Swinbourne JM, Touyz SW. The co-morbidity of eating disorders and anxiety disorders: a review. Eur Eat Disord Rev 2007; 15: 253–74.
24 Raney TJ, Thornton LM, Berrettini W, et al. Infl uence of overanxious disorder of childhood on the expression of anorexia nervosa. Int J Eat Disord 2008; 41: 326–32.
25 Salbach-Andrae H, Lenz K, Simmendinger N, Klinkowski N, Lehmkuhl U, Pfeiff er E. Psychiatric comorbidities among female adolescents with anorexia nervosa. Child Psychiatry Hum Dev 2008; 39: 261–72.
26 Halmi KA, Sunday SR, Klump KL, et al. Obsessions and compulsions in anorexia nervosa subtypes. Int J Eat Disord 2003; 33: 308–19.
27 Bulik CM, Klump KL, Thornton L, et al. Alcohol use disorder comorbidity in eating disorders: a multicenter study. J Clin Psychiatry 2004; 65: 1000–06.
28 Root TL, Pinheiro AP, Thornton L, et al. Substance use disorders in women with anorexia nervosa. Int J Eat Disord 2010; 43: 14–21.
29 Koch SV, Larsen JT, Mouridsen SE, et al. Autism spectrum disorder in individuals with anorexia nervosa and in their fi rst- and second-degree relatives: Danish nationwide register-based cohort-study. Br J Psychiatry 2015; 206: 401–07.
30 Bulik-Sullivan B, Finucane HK, Anttila V, et al. An atlas of genetic correlations across human diseases and traits. Nat Genet 2015; published online Sep 28. doi: 10.1038/ng.3406.
31 Anttila V, Bulik-Sullivan B, Finucane H, Ripke S, Malik R, Pers T. The Brainstorm project; a cross-phenotype analysis of 14 brain disorders by heritability-, constraint- and pathway-based methods, using genome-wide association data from 500,000 samples. American Society of Human Genetics Annual Meeting. San Diego; 2014.
32 Mehler PS, Brown C. Anorexia nervosa - medical complications. J Eat Disord 2015; 3: 11.
33 Mascolo M, Trent S, Colwell C, Mehler PS. What the emergency department needs to know when caring for your patients with eating disorders. Int J Eat Disord 2012; 45: 977–81.
34 Zipfel S, Löwe B, Herzog W. Medical complications. In: Treasure J, Schmidt U, Van Furth EF, eds. Handbook of eating disorders. Chichester: Wiley; 2003.
35 Misra M, Klibanski A. Endocrine consequences of anorexia nervosa. Lancet Diabetes Endocrinol 2014; 2: 581–92.
36 Zipfel S, Seibel MJ, Löwe B, Beumont PJ, Kasperk C, Herzog W. Osteoporosis in eating disorders: a follow-up study of patients with anorexia and bulimia nervosa. J Clin Endocrinol Metab 2001; 86: 5227–33.
37 Raevuori A, Haukka J, Vaarala O, et al. The increased risk for autoimmune diseases in patients with eating disorders. PLoS ONE 2014; 9: e104845.
38 Nielsen S, Emborg C, Mølbak AG. Mortality in concurrent type 1 diabetes and anorexia nervosa. Diabetes Care 2002; 25: 309–12.
39 Toufexis MD, Hommer R, Gerardi DM, et al. Disordered eating and food restrictions in children with PANDAS/PANS. J Child Adolesc Psychopharmacol 2015; 25: 48–56.
40 Herpertz-Dahlmann B. Adolescent eating disorders: update on defi nitions, symptomatology, epidemiology, and comorbidity. Child Adolesc Psychiatr Clin N Am 2015; 24: 177–96.
41 Harris EC, Barraclough B. Excess mortality of mental disorder. Br J Psychiatry 1998; 173: 11–53.
42 Raevuori A, Keski-Rahkonen A, Hoek HW. A review of eating disorders in males. Curr Opin Psychiatry 2014; 27: 426–30.
43 Strober M, Freeman R, Lampert C, Diamond J, Kaye W. Controlled family study of anorexia nervosa and bulimia nervosa: evidence of shared liability and transmission of partial syndromes. Am J Psychiatry 2000; 157: 393–401.
44 Yilmaz Z, Hardaway A, Bulik C. Genetics and epigenetics of eating disorders. Adv Genomics Genet 2015; 5: 131–50.
45 Boraska V, Franklin CS, Floyd JA, et al, and the Wellcome Trust Case Control Consortium 3. A genome-wide association study of anorexia nervosa. Mol Psychiatry 2014; 19: 1085–94.
46 Wang K, Zhang H, Bloss CS, et al, and the Price Foundation Collaborative Group. A genome-wide association study on common SNPs and rare CNVs in anorexia nervosa. Mol Psychiatry 2011; 16: 949–59.
47 Tchanturia K, Davies H, Roberts M, et al. Poor cognitive fl exibility in eating disorders: examining the evidence using the Wisconsin Card Sorting Task. PLoS ONE 2012; 7: e28331.
48 Lang K, Lopez C, Stahl D, Tchanturia K, Treasure J. Central coherence in eating disorders: an updated systematic review and meta-analysis. World J Biol Psychiatry 2014; 15: 586–98.
49 Kanakam N, Treasure J. A review of cognitive neuropsychiatry in the taxonomy of eating disorders: state, trait, or genetic? Cogn Neuropsychiatry 2013; 18: 83–114.
50 Lang K, Stahl D, Espie J, Treasure J, Tchanturia K. Set shifting in children and adolescents with anorexia nervosa: an exploratory systematic review and meta-analysis. Int J Eat Disord 2014; 47: 394–99.
51 Caglar-Nazali HP, Corfi eld F, Cardi V, et al. A systematic review and meta-analysis of ‘Systems for Social Processes’ in eating disorders. Neurosci Biobehav Rev 2014; 42: 55–92.
52 Kothari R, Solmi F, Treasure J, Micali N. The neuropsychological profi le of children at high risk of developing an eating disorder. Psychol Med 2013; 43: 1543–54.
53 Titova OE, Hjorth OC, Schiöth HB, Brooks SJ. Anorexia nervosa is linked to reduced brain structure in reward and somatosensory regions: a meta-analysis of VBM studies. BMC Psychiatry 2013; 13: 110.
54 Van den Eynde F, Suda M, Broadbent H, et al. Structural magnetic resonance imaging in eating disorders: a systematic review of voxel-based morphometry studies. Eur Eat Disord Rev 2012; 20: 94–105.

12 www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9
Review
55 King JA, Geisler D, Ritschel F, et al. Global cortical thinning in acute anorexia nervosa normalizes following long-term weight restoration. Biol Psychiatry 2015; 77: 624–32.
56 Frank GK. Advances from neuroimaging studies in eating disorders. CNS Spectr 2015; 20: 391–400.
57 Frank GK. Recent advances in neuroimaging to model eating disorder neurobiology. Curr Psychiatry Rep 2015; 17: 559.
58 García-García I, Narberhaus A, Marqués-Iturria I, et al. Neural responses to visual food cues: insights from functional magnetic resonance imaging. Eur Eat Disord Rev 2013; 21: 89–98.
59 Gaudio S, Quattrocchi CC. Neural basis of a multidimensional model of body image distortion in anorexia nervosa. Neurosci Biobehav Rev 2012; 36: 1839–47.
60 Zhu Y, Hu X, Wang J, et al. Processing of food, body and emotional stimuli in anorexia nervosa: a systematic review and meta-analysis of functional magnetic resonance imaging studies. Eur Eat Disord Rev 2012; 20: 439–50.
61 Wierenga C, Bischoff -Grethe A, Melrose AJ, et al. Altered BOLD response during inhibitory and error processing in adolescents with anorexia nervosa. PLoS ONE 2014; 9: e92017.
62 Kaye WH, Wierenga CE, Bailer UF, Simmons AN, Bischoff -Grethe A. Nothing tastes as good as skinny feels: the neurobiology of anorexia nervosa. Trends Neurosci 2013; 36: 110–20.
63 Guarda AS, Schreyer CC, Boersma GJ, Tamashiro KL, Moran TH. Anorexia nervosa as a motivated behavior: Relevance of anxiety, stress, fear and learning. Physiol Behav 2015. DOI:10.1016/j.physbeh.2015.04.007. (Epub ahead of print).
64 O’Hara CB, Campbell IC, Schmidt U. A reward-centred model of anorexia nervosa: a focussed narrative review of the neurological and psychophysiological literature. Neurosci Biobehav Rev 2015; 52: 131–52.
65 Walsh BT. The enigmatic persistence of anorexia nervosa. Am J Psychiatry 2013; 170: 477–84.
66 Godier LR, Park RJ. Compulsivity in anorexia nervosa: a transdiagnostic concept. Front Psychol 2014; 5: 778.
67 Tenconi E, Santonastaso P, Monaco F, Favaro A. Obstetric complications and eating disorders: a replication study. Int J Eat Disord 2015; 48: 424–30.
68 Jacobi C, Hayward C, de Zwaan M, Kraemer HC, Agras WS. Coming to terms with risk factors for eating disorders: application of risk terminology and suggestions for a general taxonomy. Psychol Bull 2004; 130: 19–65.
69 Herpertz-Dahlmann B, Seitz J, Konrad K. Aetiology of anorexia nervosa: from a “psychosomatic family model” to a neuropsychiatric disorder? Eur Arch Psychiatry Clin Neurosci 2011; 261 (suppl 2): S177–81.
70 Stice E, Marti CN, Durant S. Risk factors for onset of eating disorders: evidence of multiple risk pathways from an 8-year prospective study. Behav Res Ther 2011; 49: 622–27.
71 Schmidt U. Aetiology of eating disorders in the 21(st) century: new answers to old questions. Eur Child Adolesc Psychiatry 2003; 12 (suppl 1): I30–37.
72 Mander J, Teufel M, Keifenheim K, Zipfel S, Giel KE. Stages of change, treatment outcome and therapeutic alliance in adult inpatients with chronic anorexia nervosa. BMC Psychiatry 2013; 13: 111.
73 Hay P, Chinn D, Forbes D, et al, and the Royal Australian and New Zealand College of Psychiatrists. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders. Aust N Z J Psychiatry 2014; 48: 977–1008.
74 Keski-Rahkonen A, Hoek HW, Susser ES, et al. Epidemiology and course of anorexia nervosa in the community. Am J Psychiatry 2007; 164: 1259–65.
75 Ackard DM, Cronemeyer CL, Richter S, Egan A. Do symptom-specifi c stages of change predict eating disorder treatment outcome? Eat Weight Disord 2015; 20: 49–62.
76 House J, Schmidt U, Craig M, et al. Comparison of specialist and nonspecialist care pathways for adolescents with anorexia nervosa and related eating disorders. Int J Eat Disord 2012; 45: 949–56.
77 Hay PJ, Touyz S, Sud R. Treatment for severe and enduring anorexia nervosa: a review. Aust N Z J Psychiatry 2012; 46: 1136–44.
78 Herpertz S, Herpertz-Dahlmann B, Fichter M, Tuschen-Caffi er B, Zeeck A. S3-Leitlinie Diagnostik und Behandlung der Essstörungen. Berlin: Springer; 2011.
79 National Collaborating Centre for Mental Health. Eating disorders: core interventions in the treatment and management of anorexia nervosa, bulimia nervosa and related eating disorders.: National Institute for Clinical Excellence; 2004.
80 Madden S, Miskovic-Wheatley J, Wallis A, et al. A randomized controlled trial of in-patient treatment for anorexia nervosa in medically unstable adolescents. Psychol Med 2015; 45: 415–27.
81 Herpertz-Dahlmann B, Konrad K, Timmesfeld N, Dempfl e A. Treatment of adolescents with anorexia nervosa--authors’ reply. Lancet 2014; 384: 230–31.
82 Hay P. A systematic review of evidence for psychological treatments in eating disorders: 2005-2012. Int J Eat Disord 2013; 46: 462–69.
83 Watson HJ, Bulik CM. Update on the treatment of anorexia nervosa: review of clinical trials, practice guidelines and emerging interventions. Psychol Med 2013; 43: 2477–500.
84 Lock J. An Update on Evidence-Based Psychosocial Treatments for Eating Disorders in Children and Adolescents. J Clin Child Adolesc Psychol 2015; 44: 707–21.
85 Schmidt U, Magill N, Renwick B, et al. The Maudsley Outpatient Study of Treatments for Anorexia Nervosa and Related Conditions (MOSAIC): Comparison of the Maudsley Model of Anorexia Nervosa Treatment for Adults (MANTRA) with specialist supportive clinical management (SSCM) in outpatients with broadly defi ned anorexia nervosa: A randomized controlled trial. J Consult Clin Psychol 2015; 83: 796–807.
86 Schmidt U, Oldershaw A, Jichi F, et al. Out-patient psychological therapies for adults with anorexia nervosa: randomised controlled trial. Br J Psychiatry 2012; 201: 392–99.
87 Zipfel S, Wild B, Groß G, et al, and the ANTOP study group. Focal psychodynamic therapy, cognitive behaviour therapy, and optimised treatment as usual in outpatients with anorexia nervosa (ANTOP study): randomised controlled trial. Lancet 2014; 383: 127–37.
88 Whitney J, Murphy T, Landau S, et al. A practical comparison of two types of family intervention: an exploratory RCT of family day workshops and individual family work as a supplement to inpatient care for adults with anorexia nervosa. Eur Eat Disord Rev 2012; 20: 142–50.
89 Steinglass JE, Albano AM, Simpson HB, et al. Confronting fear using exposure and response prevention for anorexia nervosa: A randomized controlled pilot study. Int J Eat Disord 2014; 47: 174–80.
90 Juarascio A, Shaw J, Forman E, et al. Acceptance and commitment therapy as a novel treatment for eating disorders: an initial test of effi cacy and mediation. Behav Modif 2013; 37: 459–89.
91 McIntosh VV, Jordan J, Carter FA, et al. Three psychotherapies for anorexia nervosa: a randomized, controlled trial. Am J Psychiatry 2005; 162: 741–47.
92 Carter FA, Jordan J, McIntosh VV, et al. The long-term effi cacy of three psychotherapies for anorexia nervosa: a randomized, controlled trial. Int J Eat Disord 2011; 44: 647–54.
93 Carter JC, McFarlane TL, Bewell C, et al. Maintenance treatment for anorexia nervosa: a comparison of cognitive behavior therapy and treatment as usual. Int J Eat Disord 2009; 42: 202–07.
94 Pike KM, Walsh BT, Vitousek K, Wilson GT, Bauer J. Cognitive behavior therapy in the posthospitalization treatment of anorexia nervosa. Am J Psychiatry 2003; 160: 2046–49.
95 Fichter MM, Quadfl ieg N, Nisslmüller K, et al. Does internet-based prevention reduce the risk of relapse for anorexia nervosa? Behav Res Ther 2012; 50: 180–90.
96 Bulik CM, Baucom DH, Kirby JS, Pisetsky E. Uniting Couples (in the treatment of) Anorexia Nervosa (UCAN). Int J Eat Disord 2011; 44: 19–28.
97 Grover M, Naumann U, Mohammad-Dar L, et al. A randomized controlled trial of an Internet-based cognitive-behavioural skills package for carers of people with anorexia nervosa. Psychol Med 2011; 41: 2581–91.
98 Hoyle D, Slater J, Williams C, Schmidt U, Wade TD. Evaluation of a web-based skills intervention for carers of people with anorexia nervosa: a randomized controlled trial. Int J Eat Disord 2013; 46: 634–38.
99 Aigner M, Treasure J, Kaye W, Kasper S, Disorders WTFOE, and the WFSBP Task Force On Eating Disorders. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of eating disorders. World J Biol Psychiatry 2011; 12: 400–43.

www.thelancet.com/psychiatry Published online October 27, 2015 http://dx.doi.org/10.1016/S2215-0366(15)00356-9 13
Review
100 de Vos J, Houtzager L, Katsaragaki G, van de Berg E, Cuijpers P, Dekker J. Meta analysis on the effi cacy of pharmacotherapy versus placebo on anorexia nervosa. J Eat Disord 2014; 2: 27.
101 Kishi T, Kafantaris V, Sunday S, Sheridan EM, Correll CU. Are antipsychotics eff ective for the treatment of anorexia nervosa? Results from a systematic review and meta-analysis. J Clin Psychiatry 2012; 73: e757–66.
102 Lebow J, Sim LA, Erwin PJ, Murad MH. The eff ect of atypical antipsychotic medications in individuals with anorexia nervosa: a systematic review and meta-analysis. Int J Eat Disord 2013; 46: 332–39.
103 Tortorella A, Brambilla F, Fabrazzo M, et al. Central and peripheral peptides regulating eating behaviour and energy homeostasis in anorexia nervosa and bulimia nervosa: a literature review. Eur Eat Disord Rev 2014; 22: 307–20.
104 Hartmann A, Weber S, Herpertz S, Zeeck A, and the German Treatment Guideline Group for Anorexia Nervosa. Psychological treatment for anorexia nervosa: a meta-analysis of standardized mean change. Psychother Psychosom 2011; 80: 216–26.
105 Kohn MR, Madden S, Clarke SD. Refeeding in anorexia nervosa: increased safety and effi ciency through understanding the pathophysiology of protein calorie malnutrition. Curr Opin Pediatr 2011; 23: 390–94.
106 Misra M, Klibanski A. Anorexia nervosa and bone. J Endocrinol 2014; 221: R163–76.
107 Insel TR, Gogtay N. National Institute of Mental Health clinical trials: new opportunities, new expectations. JAMA Psychiatry 2014; 71: 745–46.
108 Holmes EA, Craske MG, Graybiel AM. Psychological treatments: A call for mental-health science. Nature 2014; 511: 287–89.
109 Lindvall Dahlgren C, Rø O. A systematic review of cognitive remediation therapy for anorexia nervosa—development, current state and implications for future research and clinical practice. J Eat Disord 2014; 2: 26.
110 Tchanturia K, Lounes N, Holttum S. Cognitive remediation in anorexia nervosa and related conditions: a systematic review. Eur Eat Disord Rev 2014; 22: 454–62.
111 Koskina A, Campbell IC, Schmidt U. Exposure therapy in eating disorders revisited. Neurosci Biobehav Rev 2013; 37: 193–208.
112 Renwick B, Campbell IC, Schmidt U. Review of attentional bias modifi cation: a brain-directed treatment for eating disorders. Eur Eat Disord Rev 2013; 21: 464–74.
113 Lipsman N, Woodside DB, Lozano AM. Neurocircuitry of limbic dysfunction in anorexia nervosa. Cortex 2015; 62: 109–18.
114 Lipsman N, Woodside DB, Giacobbe P, Lozano AM. Neurosurgical treatment of anorexia nervosa: review of the literature from leucotomy to deep brain stimulation. Eur Eat Disord Rev 2013; 21: 428–35.
115 McClelland J, Bozhilova N, Campbell I, Schmidt U. A systematic review of the eff ects of neuromodulation on eating and body weight: evidence from human and animal studies. Eur Eat Disord Rev 2013; 21: 436–55.
116 Bailey AP, Parker AG, Colautti LA, Hart LM, Liu P, Hetrick SE. Mapping the evidence for the prevention and treatment of eating disorders in young people. J Eat Disord 2014; 2: 5.
117 Yager Z, Diedrichs PC, Ricciardelli LA, Halliwell E. What works in secondary schools? A systematic review of classroom-based body image programs. Body Image 2013; 10: 271–81.
118 Loucas CE, Fairburn CG, Whittington C, Pennant ME, Stockton S, Kendall T. E-therapy in the treatment and prevention of eating disorders: A systematic review and meta-analysis. Behav Res Ther 2014; 63C: 122–31.
119 Hart LM, Cornell C, Damiano SR, Paxton SJ. Parents and prevention: a systematic review of interventions involving parents that aim to prevent body dissatisfaction or eating disorders. Int J Eat Disord 2015; 48: 157–69.
120 Lutter M, Croghan AE, Cui H. Escaping the Golden Cage: Animal Models of Eating Disorders in the Post-Diagnostic and Statistical Manual Era. Biol Psychiatry 2015; published online Feb 12. DOI:10.1016/j.biopsych.2015.02.006.
![[PPT]Anorexia Nervosa - Mr Sitar's Website - homemrsitarswebsite.wikispaces.com/file/view/Anorexia Nervosa... · Web viewWhat is the definition to this illness? Anorexia nervosa is](https://img.pdfslide.us/doc/110x75/5af162f57f8b9ad0618f592d/pptanorexia-nervosa-mr-sitars-website-nervosaweb-viewwhat-is-the-definition.jpg)