Embed Size (px)
Citation preview
Procedural errors in endodontics;
aetiology, prevention and management
Year 5 DDS – Nov. 2014
Dr. Ahmad El-Ma’aita
BDS, MSc, PhD, MEndo RCSEd
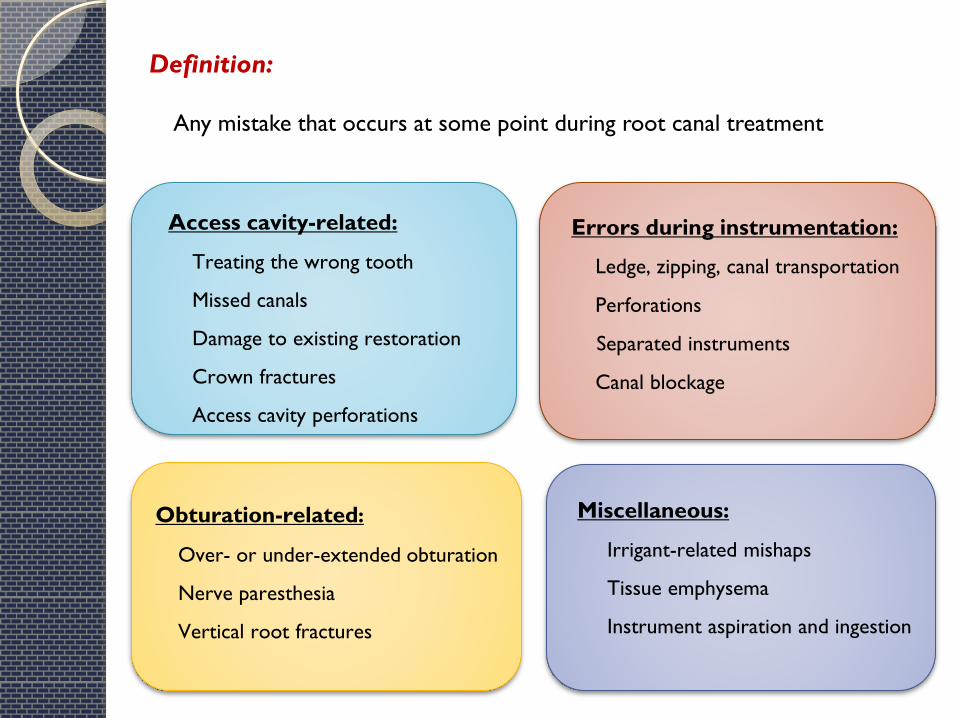
Definition:
Any mistake that occurs at some point during root canal treatment
Miscellaneous:
Irrigant-related mishaps
Tissue emphysema
Instrument aspiration and ingestion
Obturation-related:
Over- or under-extended obturation
Nerve paresthesia
Vertical root fractures
Access cavity-related:
Treating the wrong tooth
Missed canals
Damage to existing restoration
Crown fractures
Access cavity perforations
Errors during instrumentation:
Ledge, zipping, canal transportation
Perforations
Separated instruments
Canal blockage
Treatment of the Wrong Tooth
Aetiology: either misdiagnosis or inattention.
Prevention:
a) Ensure correct diagnosis through detailed history and examination.
b) Mark the tooth which requires treatment (with a pen!).
Management:
a) Complete the treatment of both teeth
b) Inform the patient
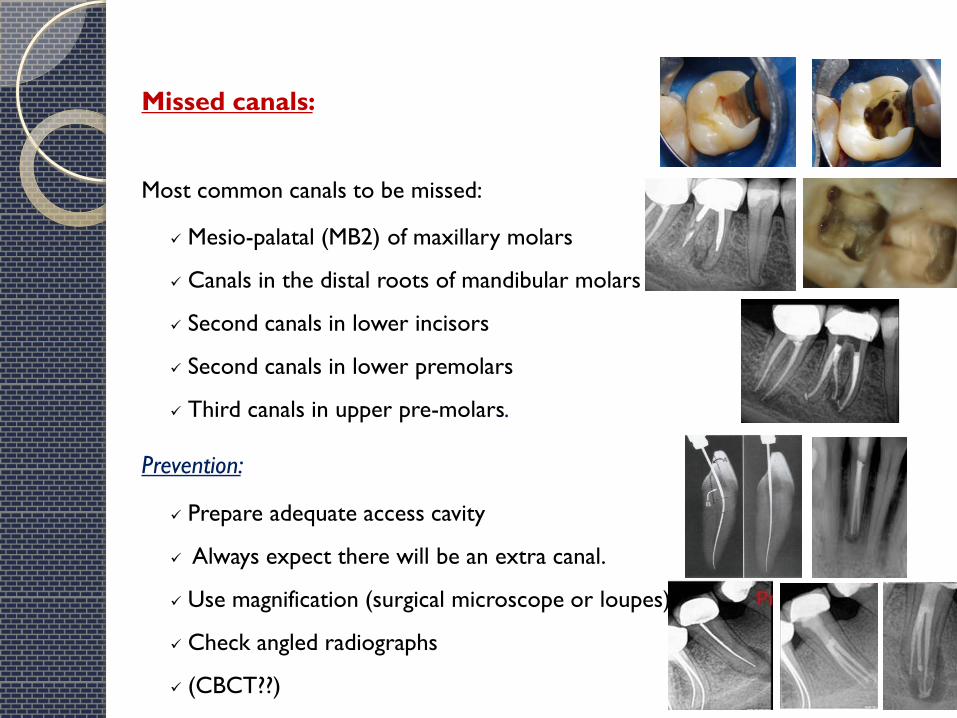
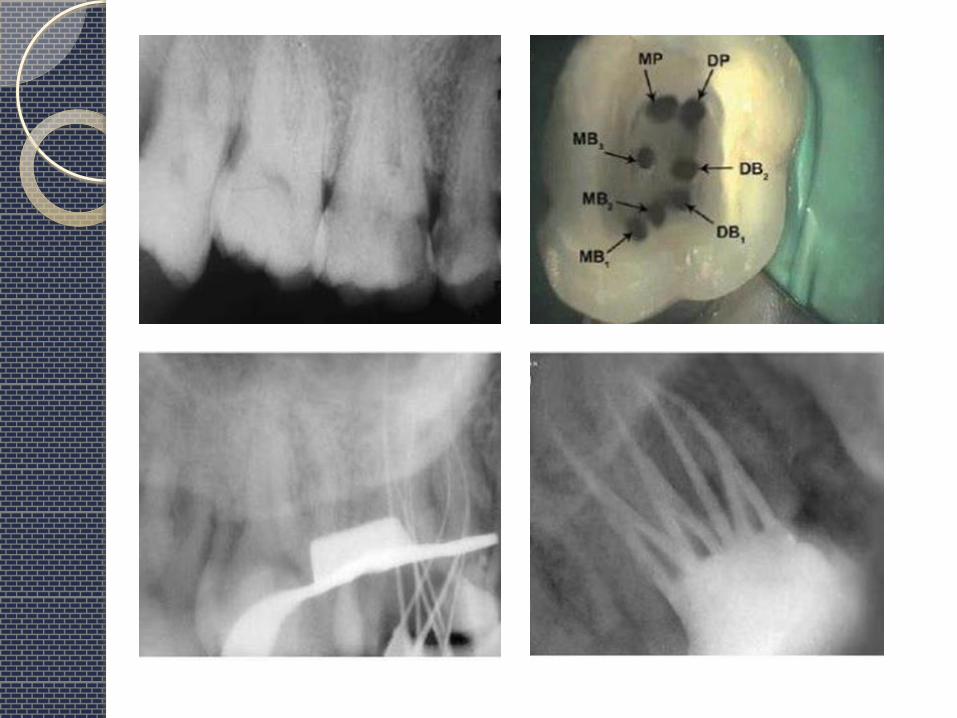
Missed canals:
Most common canals to be missed:
Mesio-palatal (MB2) of maxillary molars
Canals in the distal roots of mandibular molars
Second canals in lower incisors
Second canals in lower premolars
Third canals in upper pre-molars.
Prevention:
Prepare adequate access cavity
Always expect there will be an extra canal.
Use magnification (surgical microscope or loupes)
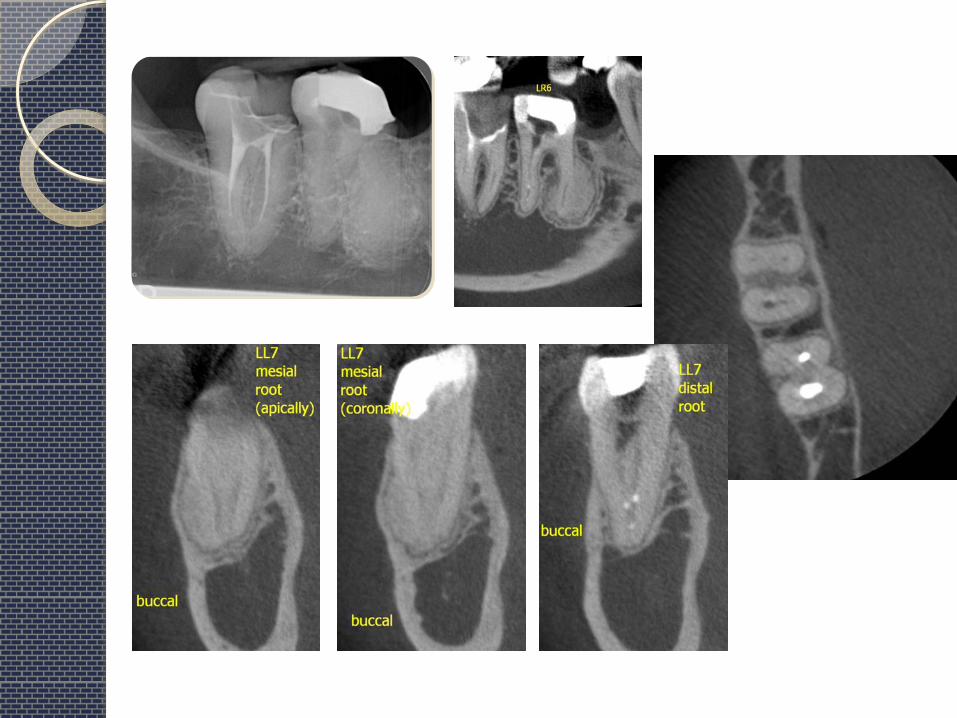
Check angled radiographs
(CBCT??)
Damage to an existing restoration:
Porcelain crowns are the most susceptible to chipping and fracture.
Prevention:
Use a water-cooled, smooth diamond bur
Do not force the bur (let it cut its own way)
Do not place a rubber dam clamp on the gingiva of a
porcelain or porcelain-faced crown.
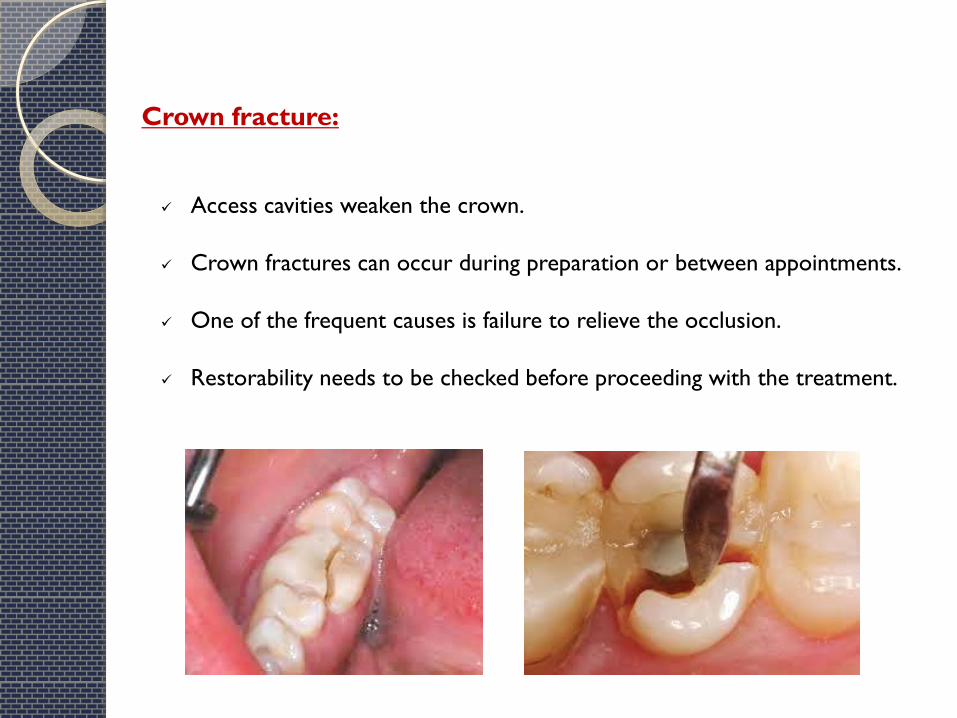
Crown fracture:
Access cavities weaken the crown.
Crown fractures can occur during preparation or between appointments.
One of the frequent causes is failure to relieve the occlusion.
Restorability needs to be checked before proceeding with the treatment.
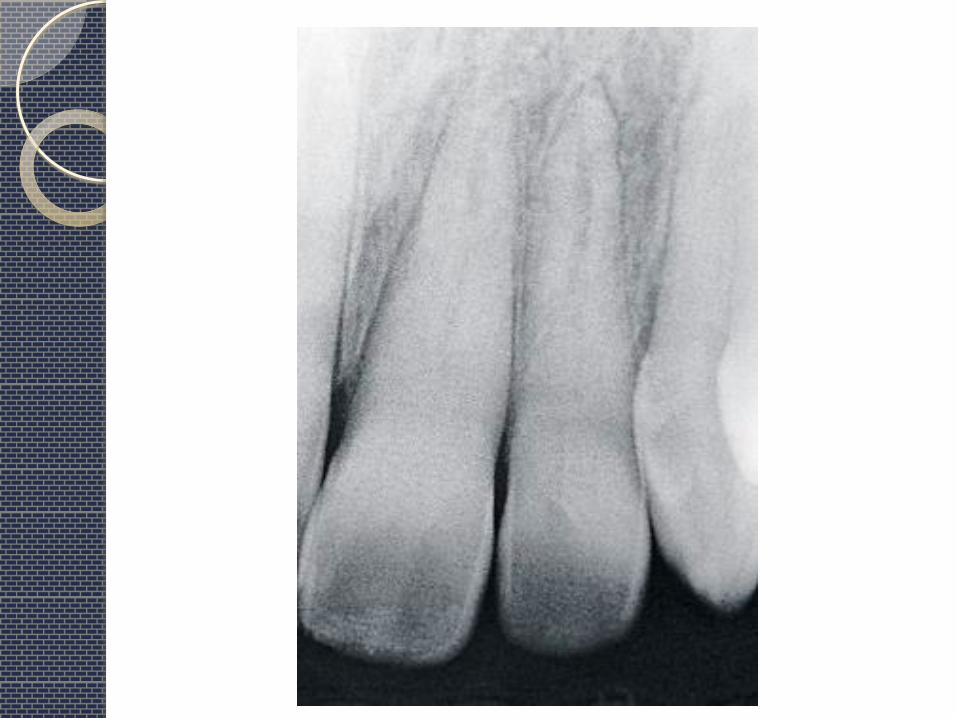
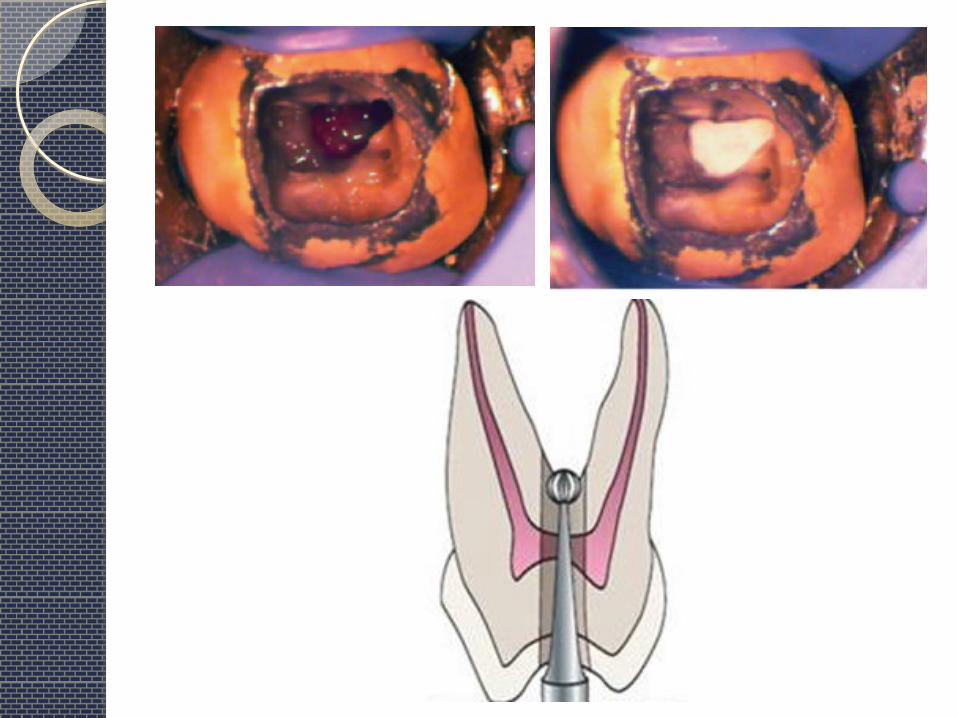
Perforations:
Definition:
Pathologic or iatrogenic communication between the pulp space and the oral or
peri-radicular tissues.
Aetiology:
A- Iatrogenic:
1- Misaligned use of burs during access preparation and search for canal orifices
2- During efforts to negotiate calcified and curved canals
3- Overzealous instrumentation towards a root concavity (Strip perforation)
4- Inappropriate post space preparation
B- Pathological:
1- Caries
2- Root resorption



Bacterial infection emanating either from the root canal or the periodontal
tissues, or both, prevents healing and brings about inflammatory sequels.
This results in pain, suppurations, abscesses, and fistulae.
Down-growth of gingival epithelium to the perforation site can emerge,
especially when accidental perforations occur in the crestal area by lateral
perforation or perforation in furcations of multi-rooted teeth.
Once an infectious process has established itself at the perforation site,
prognosis for treatment is precarious and extraction may be needed.
Whether or not a root perforation can be successfully treated depends on
whether the perforation can be repaired such that bacterial infection of the
perforation site can either be prevented or eliminated
Prognosis depends on:
1) Time
2) Size
3) Location
4) Adequacy of seal
Prognosis of perforations:
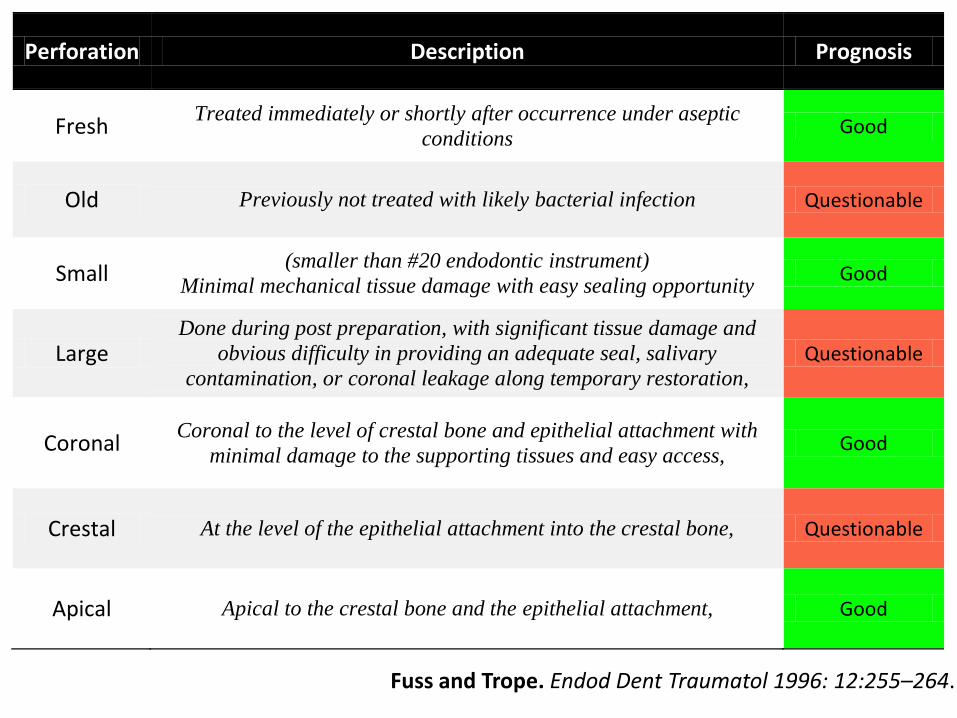
Perforation Description Prognosis
Fresh Treated immediately or shortly after occurrence under aseptic
conditions Good
Old Previously not treated with likely bacterial infection Questionable
Small (smaller than #20 endodontic instrument)
Minimal mechanical tissue damage with easy sealing opportunity Good
Large Done during post preparation, with significant tissue damage and
obvious difficulty in providing an adequate seal, salivary
contamination, or coronal leakage along temporary restoration, Questionable
Coronal Coronal to the level of crestal bone and epithelial attachment with
minimal damage to the supporting tissues and easy access, Good
Crestal At the level of the epithelial attachment into the crestal bone, Questionable
Apical Apical to the crestal bone and the epithelial attachment, Good
Fuss and Trope. Endod Dent Traumatol 1996: 12:255–264.
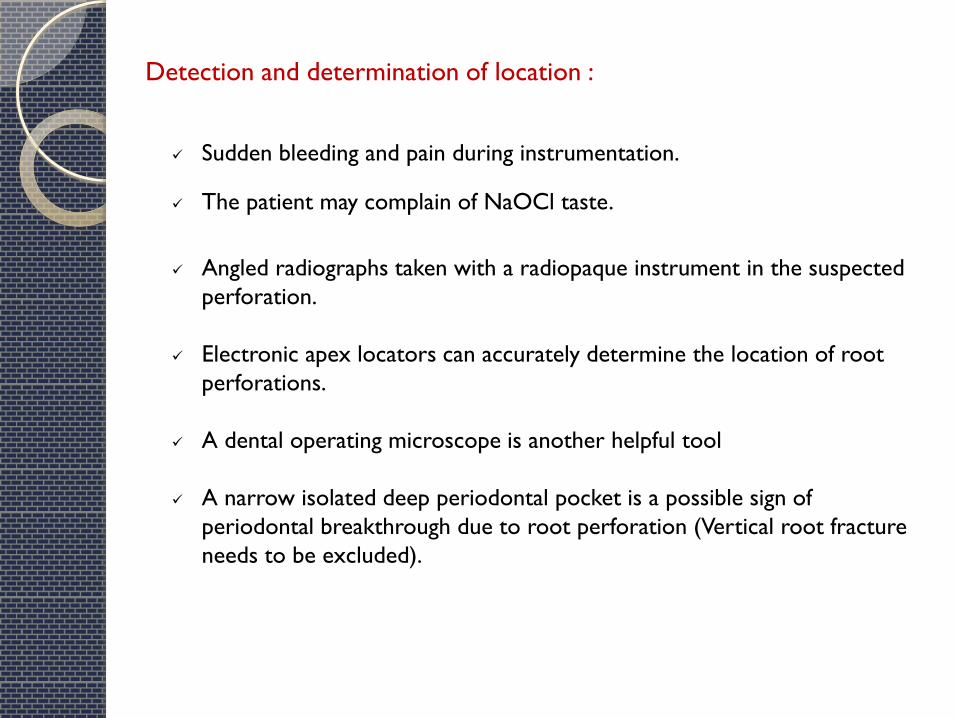
Detection and determination of location :
Sudden bleeding and pain during instrumentation.
The patient may complain of NaOCl taste.
Angled radiographs taken with a radiopaque instrument in the suspected
perforation.
Electronic apex locators can accurately determine the location of root
perforations.
A dental operating microscope is another helpful tool
A narrow isolated deep periodontal pocket is a possible sign of
periodontal breakthrough due to root perforation (Vertical root fracture
needs to be excluded).
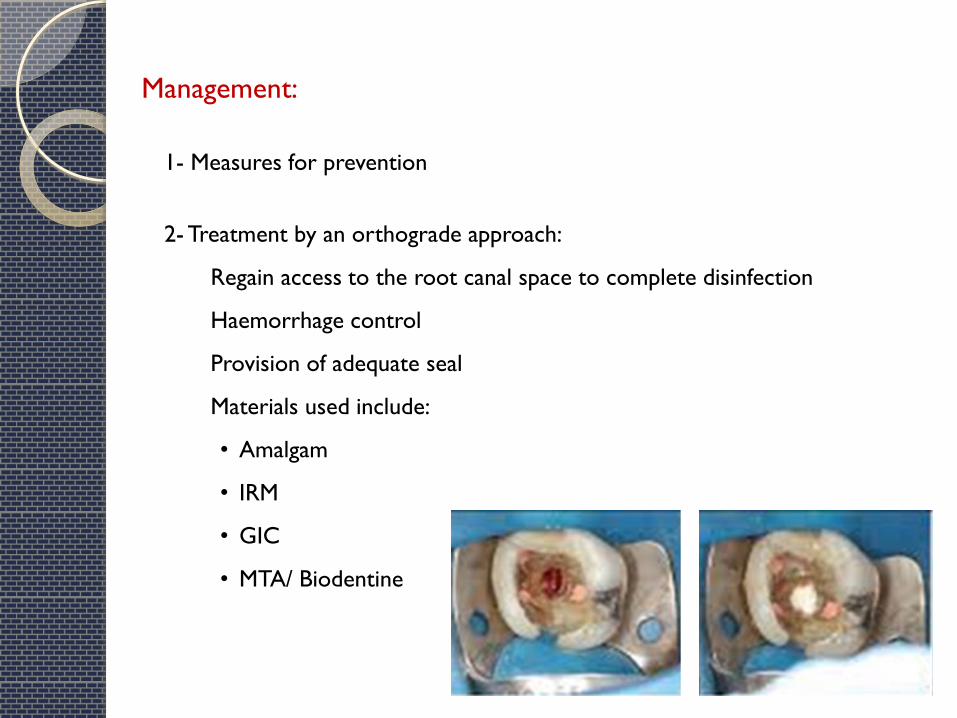
Management:
1- Measures for prevention
2- Treatment by an orthograde approach:
Regain access to the root canal space to complete disinfection
Haemorrhage control
Provision of adequate seal
Materials used include:
• Amalgam
• IRM
• GIC
• MTA/ Biodentine
Management:
3- Treatment by a surgical approach
To surgically expose the perforation site and achieve a fluid-tight seal.
To prevent bacteria and their byproducts in the root canal from entering
the surrounding periodontal tissues
4- Orthodontic extrusion?? (for crestal perforations)
5- Intentional replantation
When orthograde and surgical treatments are not possible, undesirable, or
have already failed
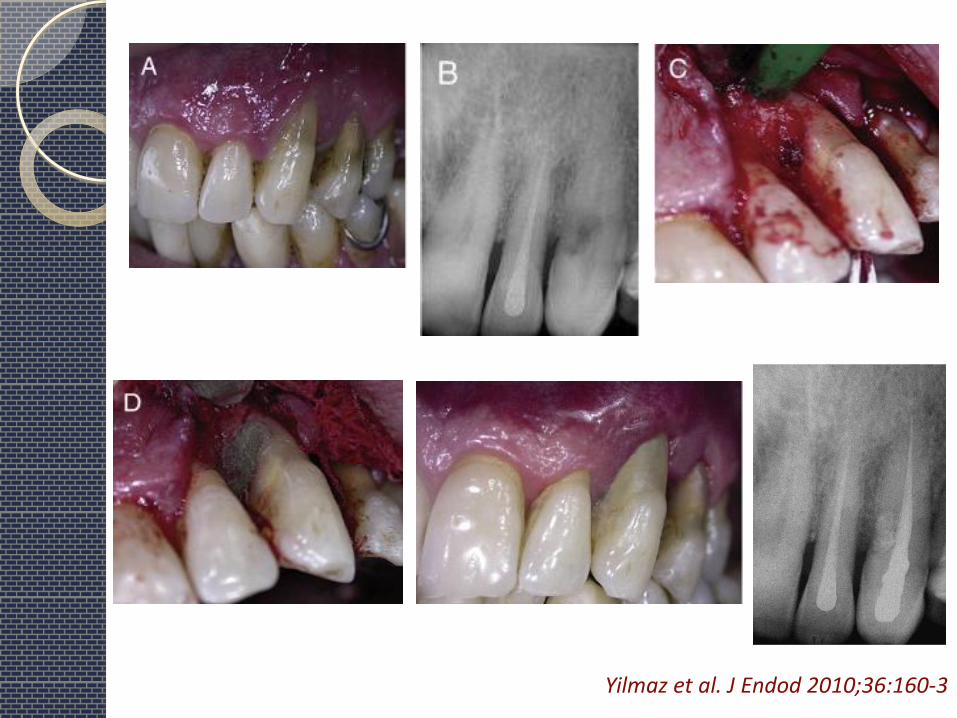
Yilmaz et al. J Endod 2010;36:160-3
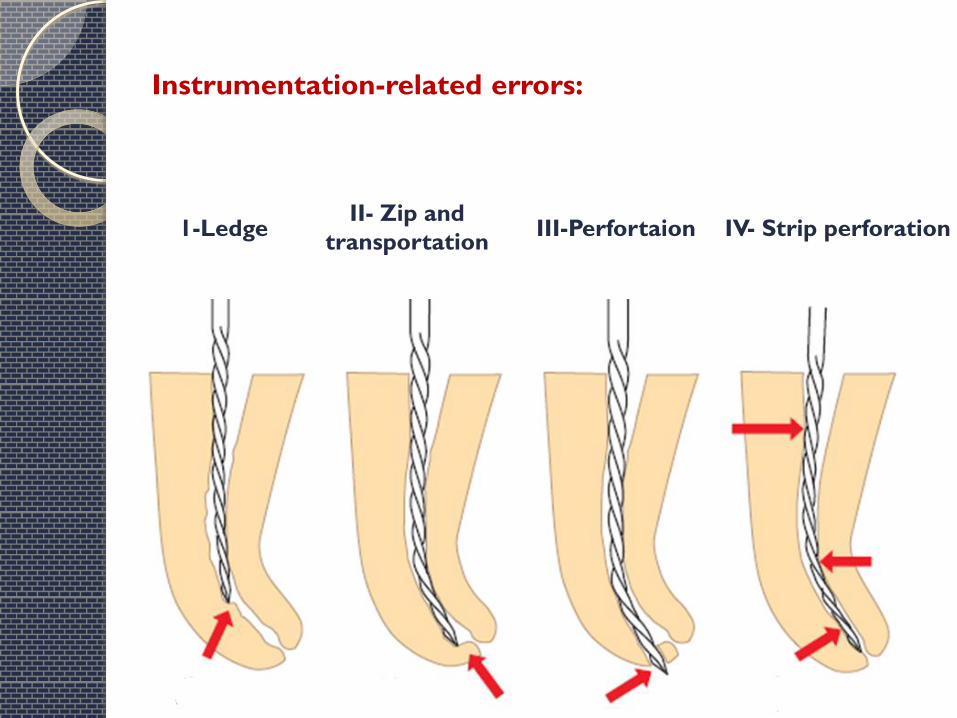
Instrumentation-related errors:
1-Ledge
II- Zip and
transportation
III-Perfortaion IV- Strip perforation
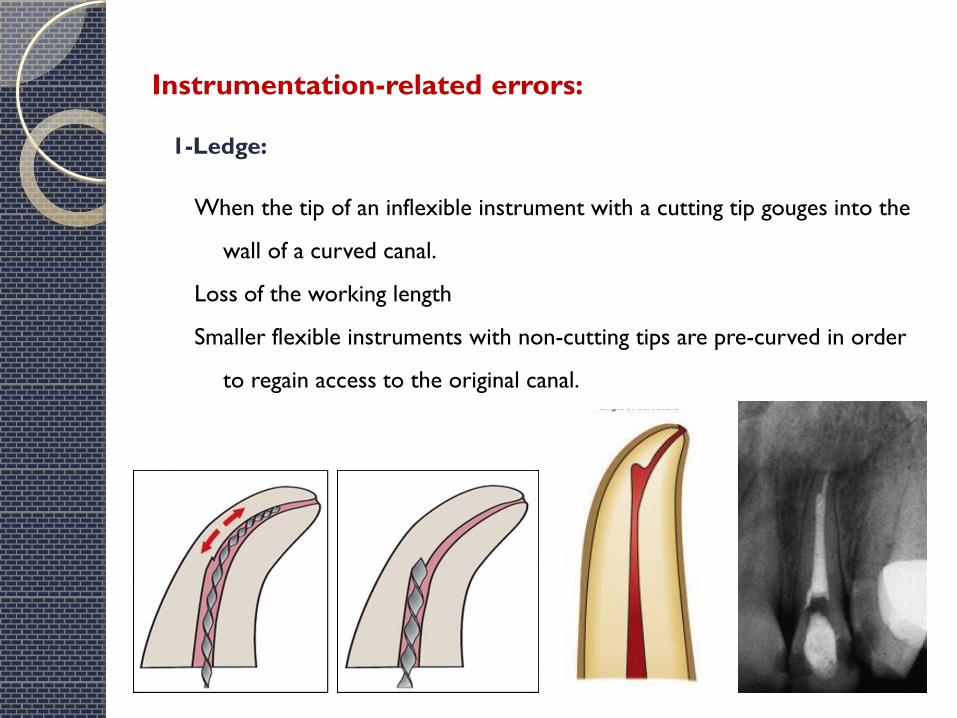
1-Ledge:
Instrumentation-related errors:
When the tip of an inflexible instrument with a cutting tip gouges into the
wall of a curved canal.
Loss of the working length
Smaller flexible instruments with non-cutting tips are pre-curved in order
to regain access to the original canal.
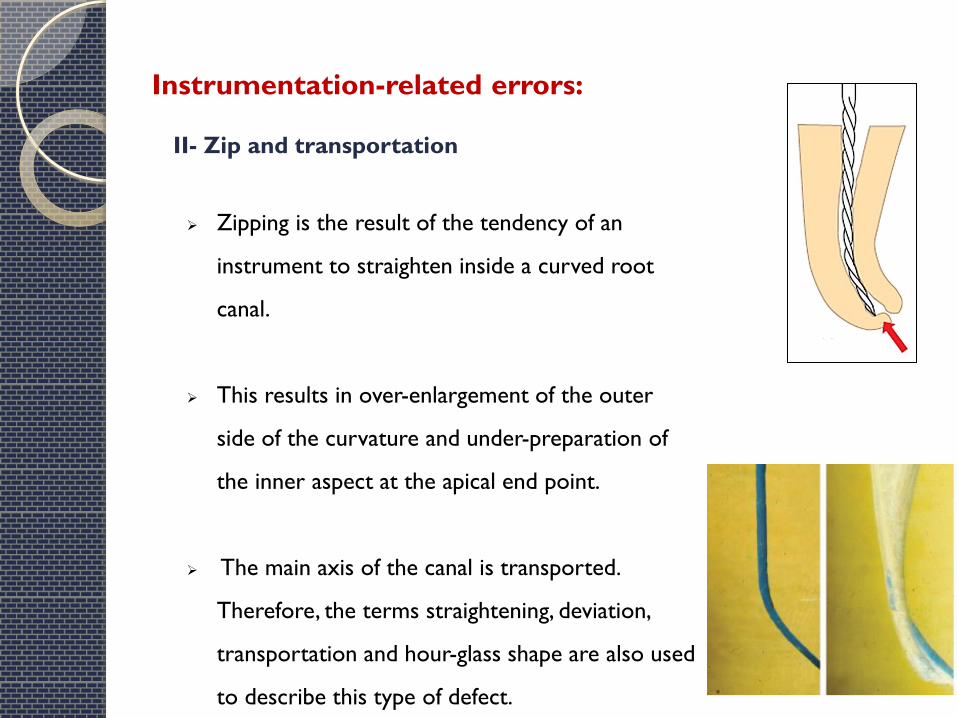
II- Zip and transportation
Instrumentation-related errors:
Zipping is the result of the tendency of an
instrument to straighten inside a curved root
canal.
This results in over-enlargement of the outer
side of the curvature and under-preparation of
the inner aspect at the apical end point.
The main axis of the canal is transported.
Therefore, the terms straightening, deviation,
transportation and hour-glass shape are also used
to describe this type of defect.
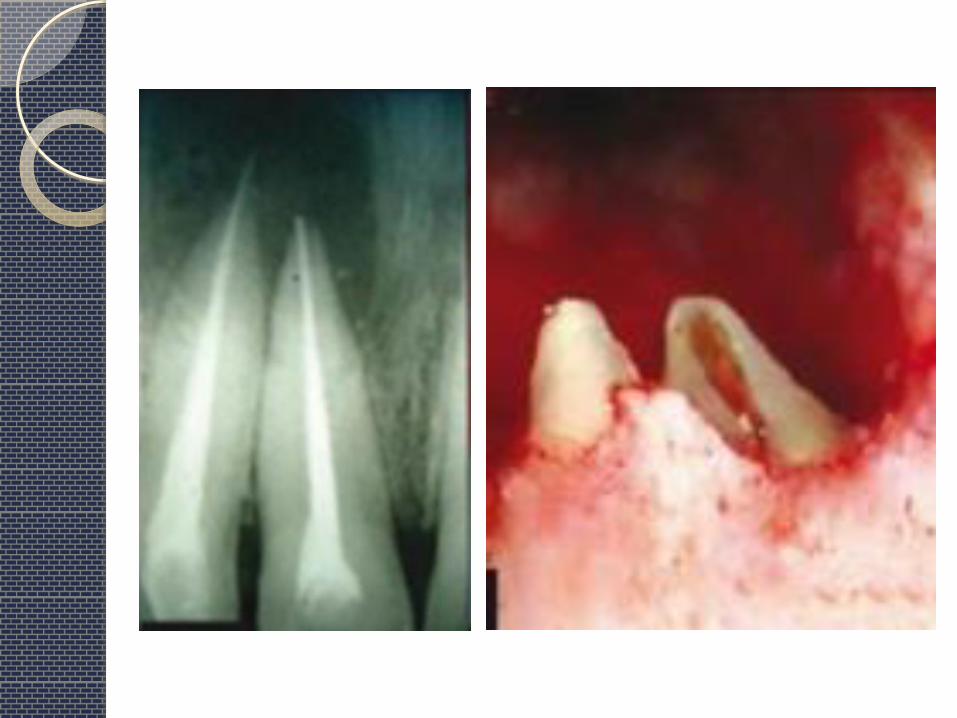
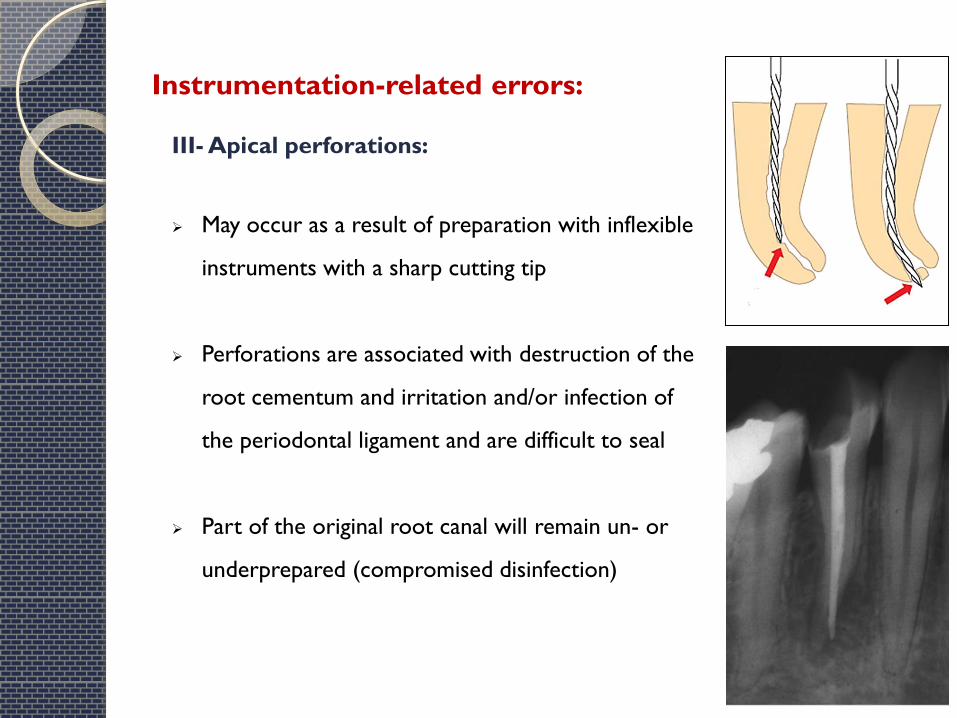
III- Apical perforations:
Instrumentation-related errors:
May occur as a result of preparation with inflexible
instruments with a sharp cutting tip
Perforations are associated with destruction of the
root cementum and irritation and/or infection of
the periodontal ligament and are difficult to seal
Part of the original root canal will remain un- or
underprepared (compromised disinfection)
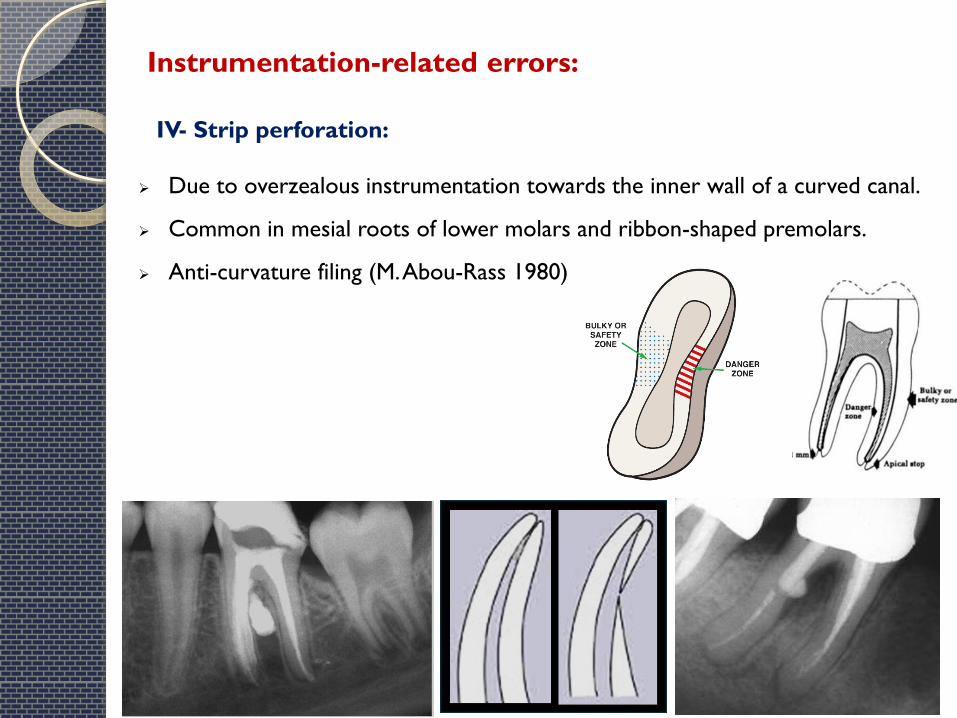
IV- Strip perforation:
Due to overzealous instrumentation towards the inner wall of a curved canal.
Common in mesial roots of lower molars and ribbon-shaped premolars.
Anti-curvature filing (M. Abou-Rass 1980)
Instrumentation-related errors:
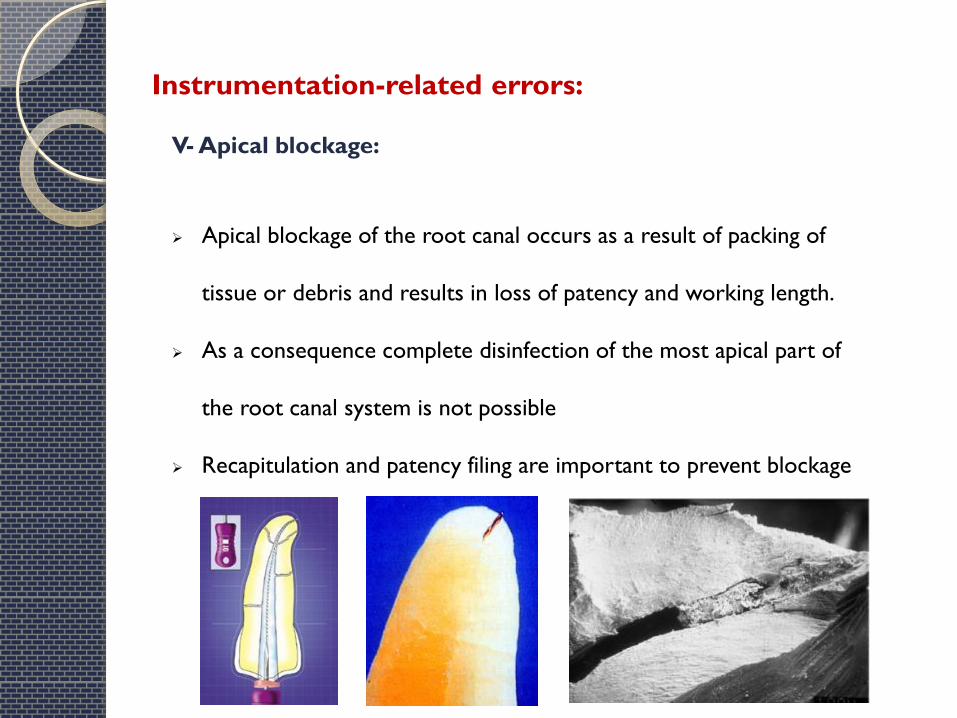
V- Apical blockage:
Instrumentation-related errors:
Apical blockage of the root canal occurs as a result of packing of
tissue or debris and results in loss of patency and working length.
As a consequence complete disinfection of the most apical part of
the root canal system is not possible
Recapitulation and patency filing are important to prevent blockage
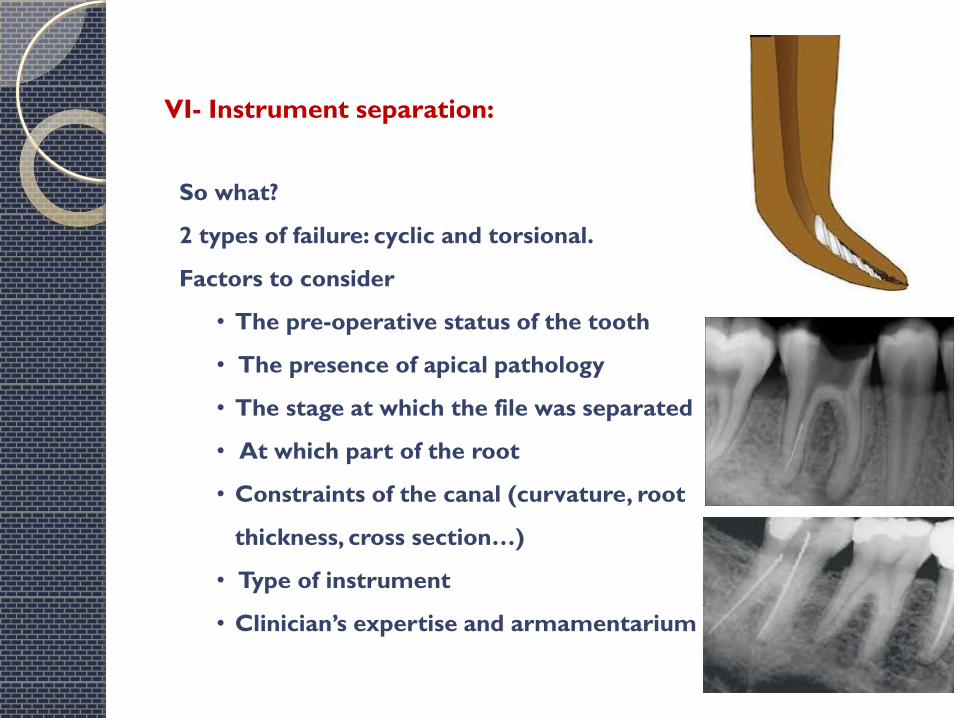
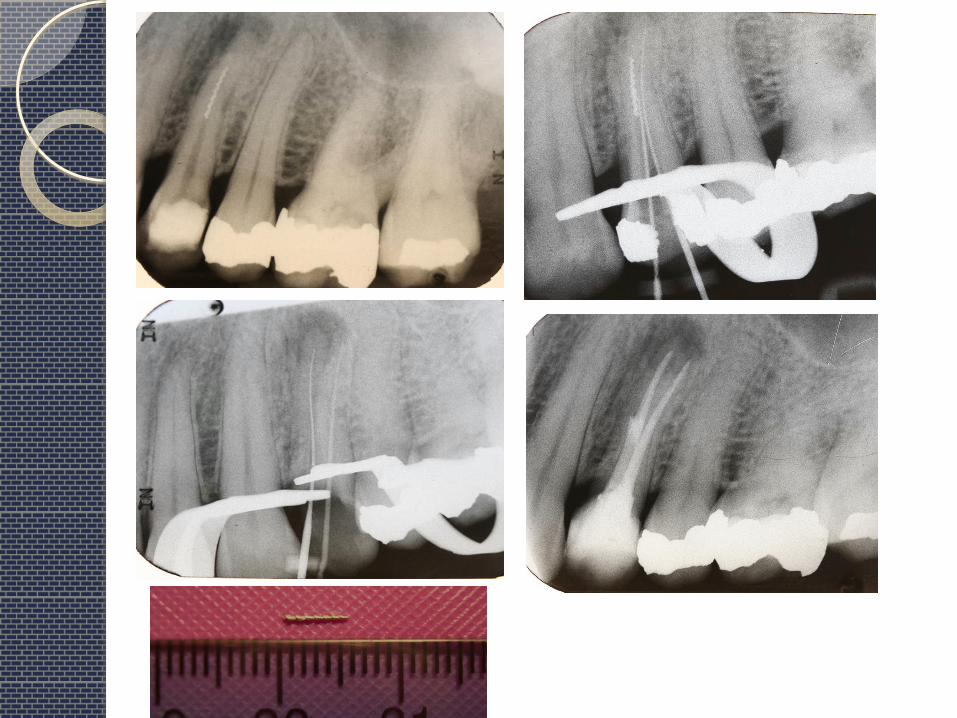
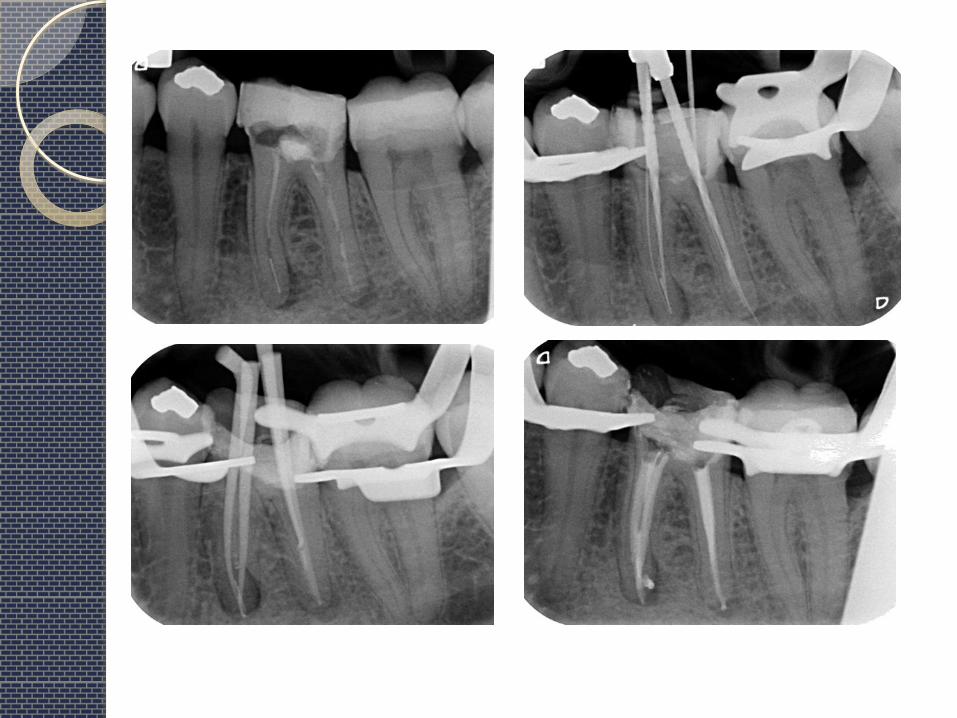
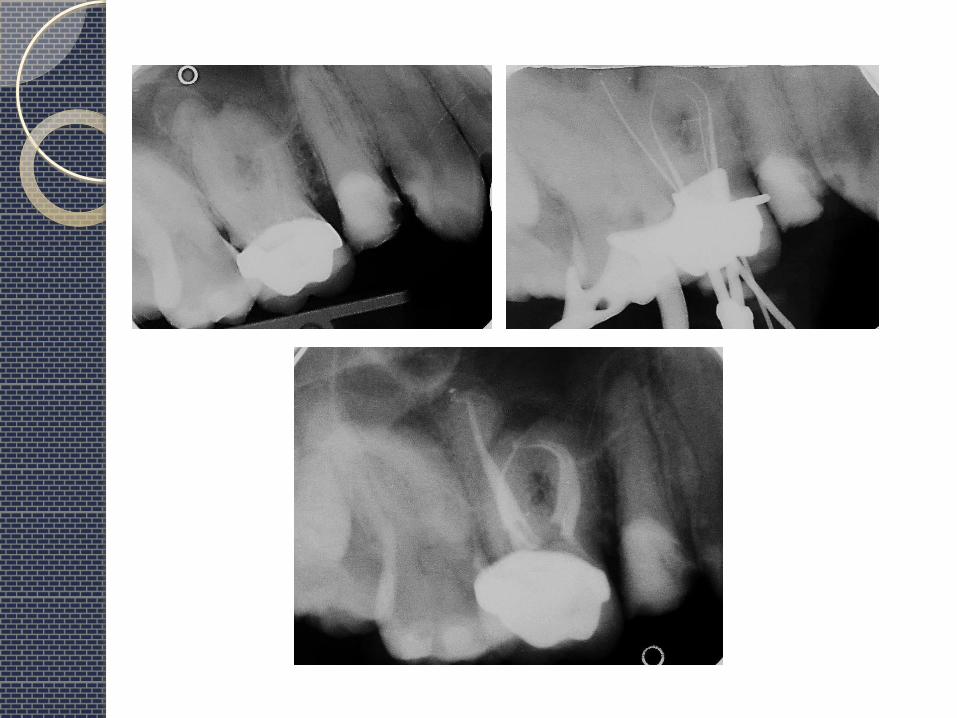
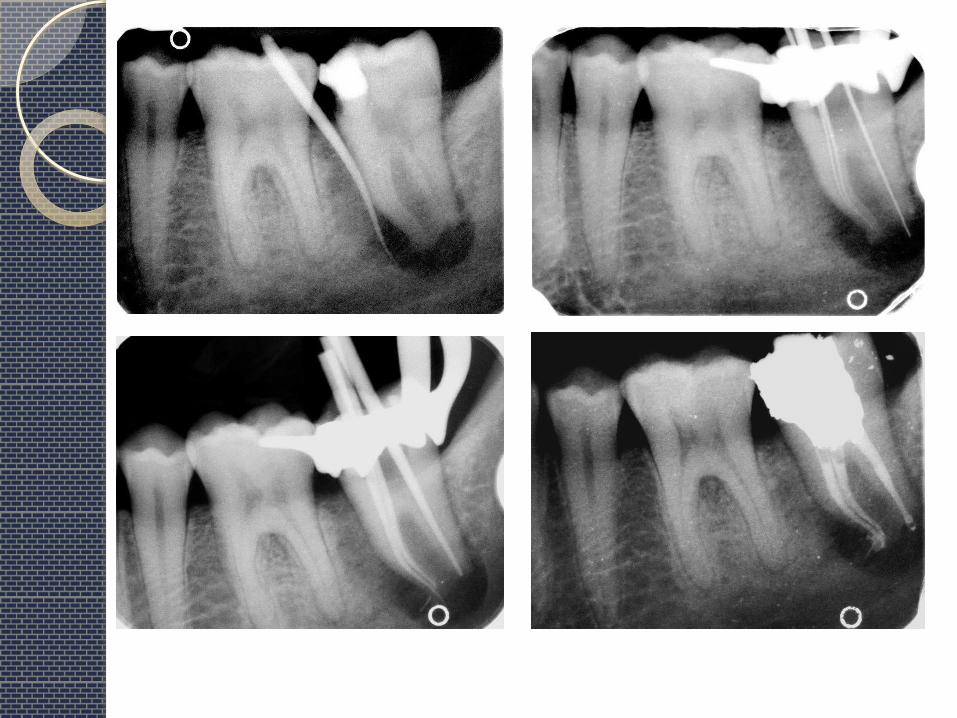
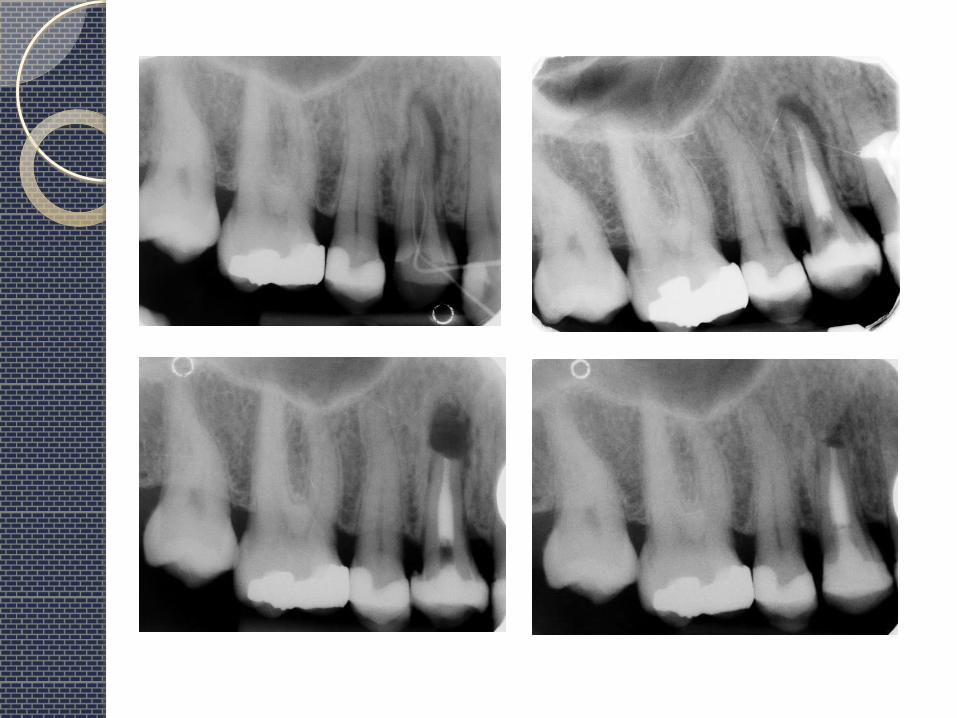
VI- Instrument separation:
So what?
2 types of failure: cyclic and torsional.
Factors to consider
• The pre-operative status of the tooth
• The presence of apical pathology
• The stage at which the file was separated
• At which part of the root
• Constraints of the canal (curvature, root
thickness, cross section…)
• Type of instrument
• Clinician’s expertise and armamentarium
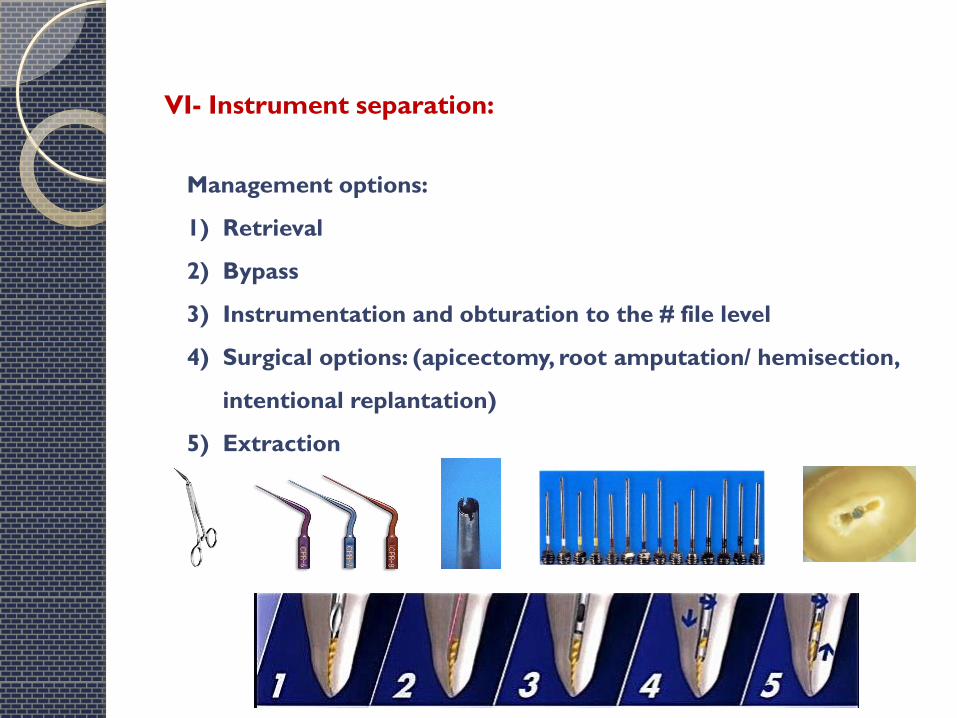
Management options:
1) Retrieval
2) Bypass
3) Instrumentation and obturation to the # file level
4) Surgical options: (apicectomy, root amputation/ hemisection,
intentional replantation)
5) Extraction
VI- Instrument separation:
How to reduce the incidence of instrument separation?
1- Pre-assessment of the case complexity
II- Straight line access
III- Copious irrigation
IV- Preflaring the coronal canal
V- Achieve a glide path
VI- Single use of instruments
VII- Working length radiograph
VIII- Follow manufacturer’s instructions
IX- Anti-curvature filing
X- Avoid apical pressure
XI- Clean the flutes regularly
XII- Patency filing?
Obturation-related mishaps:
I- Over-extended root fillings:
The apical termination point of canal instrumentation and obturtion is the
apical constriction (dentinocemental junction)
Slight extrusion of the root canal filling is called a “puff” or “button”.
Healing against these slight overfills is usually inconsequential.
Loss of apical constriction by perforation is often the cause of
overextension when there is no barrier compact the root filling against.
Gross overextension may deter healing and may even end up in the
maxillary sinus or the mandibular canal.
Nerve paresthesia is a possible result.
For massive overfills, removal by surgery followed by a retrofilling is often
the only solution

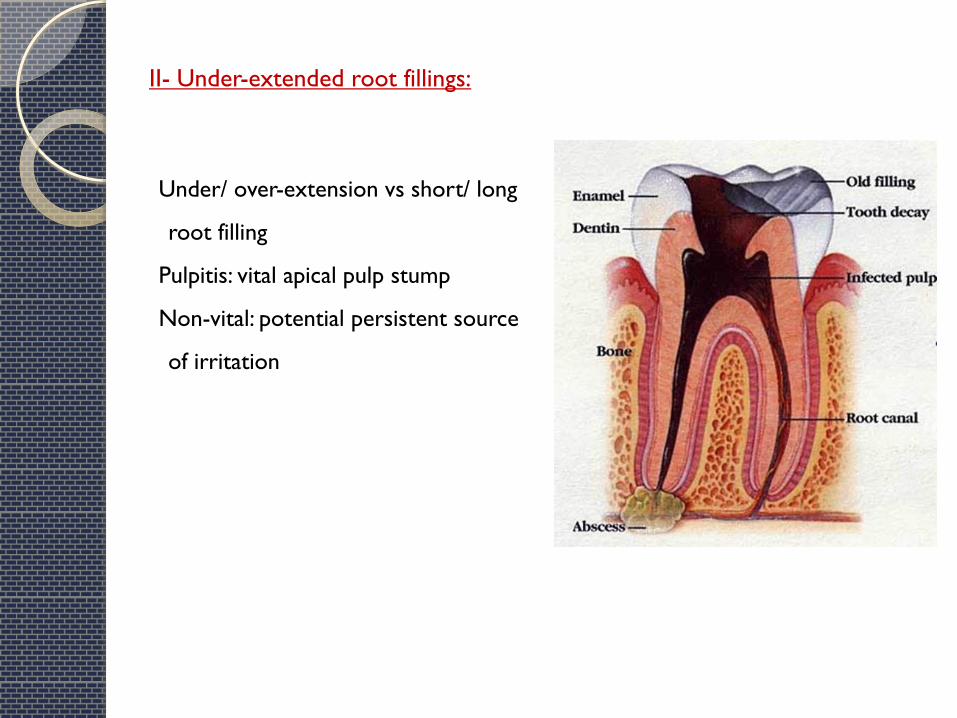
II- Under-extended root fillings:
Under/ over-extension vs short/ long
root filling
Pulpitis: vital apical pulp stump
Non-vital: potential persistent source
of irritation
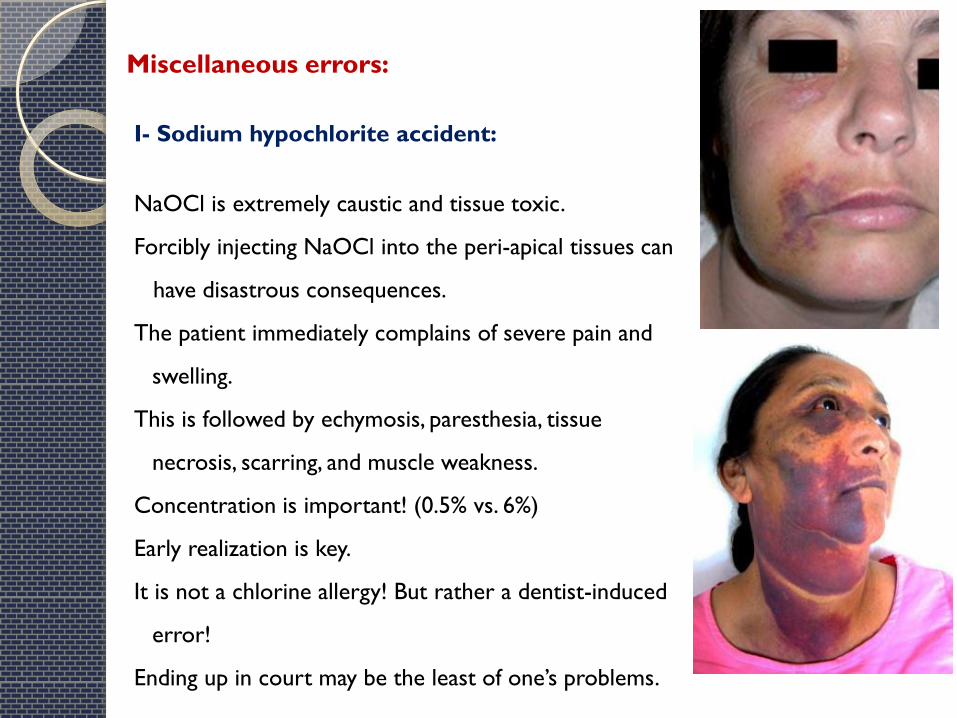
I- Sodium hypochlorite accident:
NaOCl is extremely caustic and tissue toxic.
Forcibly injecting NaOCl into the peri-apical tissues can
have disastrous consequences.
The patient immediately complains of severe pain and
swelling.
This is followed by echymosis, paresthesia, tissue
necrosis, scarring, and muscle weakness.
Concentration is important! (0.5% vs. 6%)
Early realization is key.
It is not a chlorine allergy! But rather a dentist-induced
error!
Ending up in court may be the least of one’s problems.
Miscellaneous errors:
Prevention:
Passive placement of the irrigating needle (no wedging).
Side-vented or notched needles are recommended.
No great force is exerted on the plunger of the syringe (use index finger Prevention:
Passive placement of the irrigating needle (no wedging).
Side-vented or notched needles are recommended.
No great force is exerted on the plunger of the syringe (use index finger
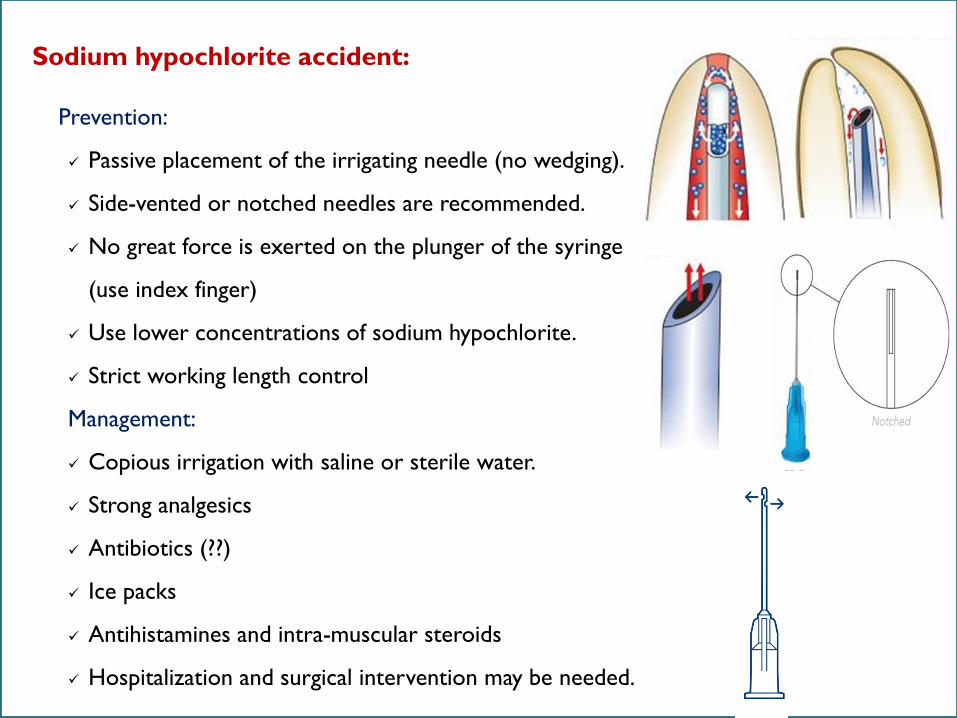
Prevention:
Passive placement of the irrigating needle (no wedging).
Side-vented or notched needles are recommended.
No great force is exerted on the plunger of the syringe
(use index finger)
Use lower concentrations of sodium hypochlorite.
Strict working length control
Management:
Copious irrigation with saline or sterile water.
Strong analgesics
Antibiotics (??)
Ice packs
Antihistamines and intra-muscular steroids
Hospitalization and surgical intervention may be needed.
Sodium hypochlorite accident:
Collection of air (or another gas) below the subcutaneous tissues
Relatively uncommon.
Two actions may cause this to happen:
A blast of air to dry a canal (more likely to happen with youngsters, in
whom the canals in anterior teeth are relatively large)
Exhaust air from a high-speed drill directed toward the tissue.
The usual sequence of events is rapid swelling, erythema, and crepitus.
It is usually a benign condition that resolves over 3–10 days as the gas is
resorbed into the blood stream for eventual excretion via the lungs.
Complications (although rare) include: pneumomediastinum, airway
compromise and death!
Rickls NH, Joshi BA. Death from air embolism during root canal therapy. J. Am.
Dent. Assoc. 1963; 67: 399–404
II- Subcutaneous tissue emphysema:

Prevention:
Use paper points. Do not blow air directly down an open canal.
Employ a handpiece that exhausts the spent air out the back of the
handpiece rather than into the operating field.
Management:
Reassurance
Referral and hospitalization
A course of antibiotics designed to cover normal oral flora (weak evidence)
Subcutaneous tissue emphysema:
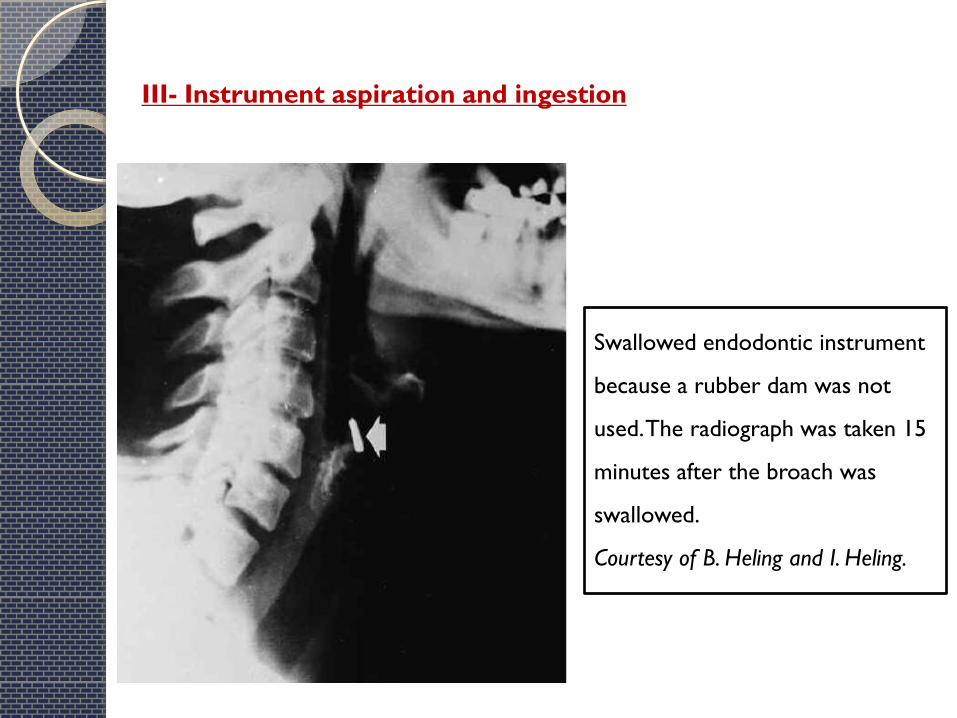
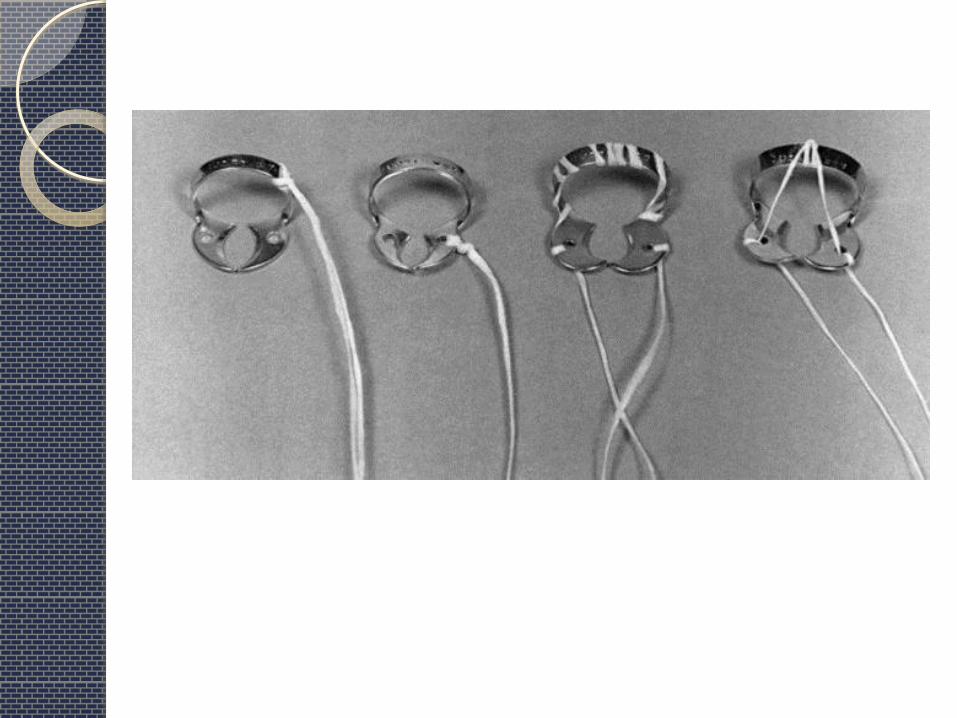
III- Instrument aspiration and ingestion
Swallowed endodontic instrument
because a rubber dam was not
used. The radiograph was taken 15
minutes after the broach was
swallowed.
Courtesy of B. Heling and I. Heling.
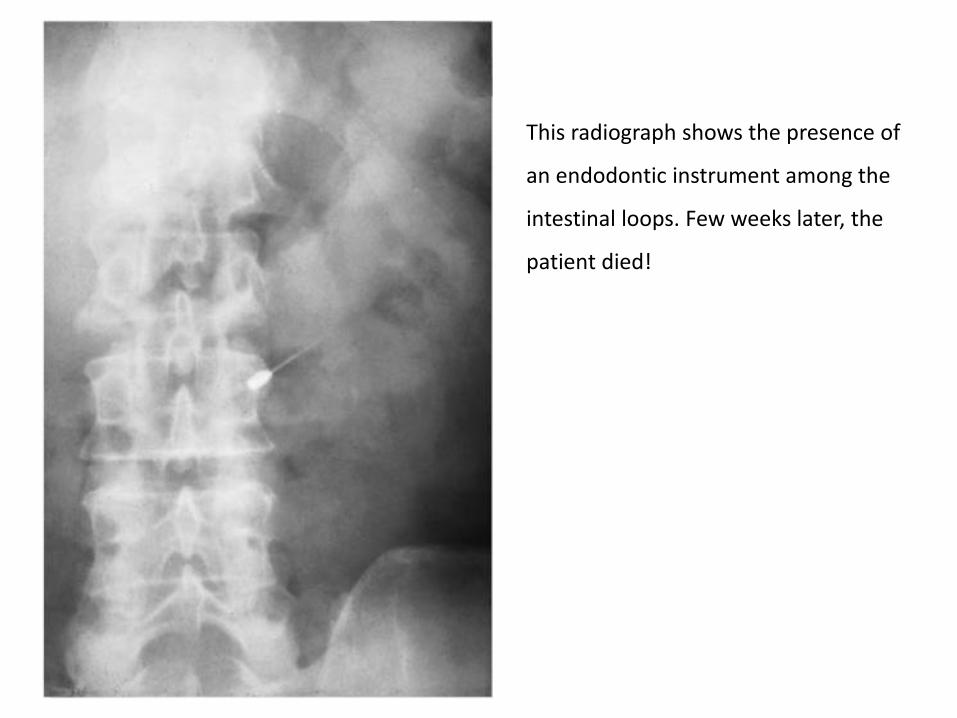
This radiograph shows the presence of
an endodontic instrument among the
intestinal loops. Few weeks later, the
patient died!

Instrument aspiration and ingestion
Always use a rubber dam!
If one insists on placing rubber dam clamps before the dam is placed, the
clamp should be fitted with a long string of dental floss to aid in its
recovery
If instrument aspiration or ingestion is apparent, the patient must be taken
immediately to a medical emergency facility for examination, and the
dentist must accompany the patient.
Radiography of the thorax and abdomen. (It is helpful if the dentist takes a
sample file along so the radiologist has a better idea of what to look for)
Surgical intervention would be the only solution.
Be prepared for a session in court!!
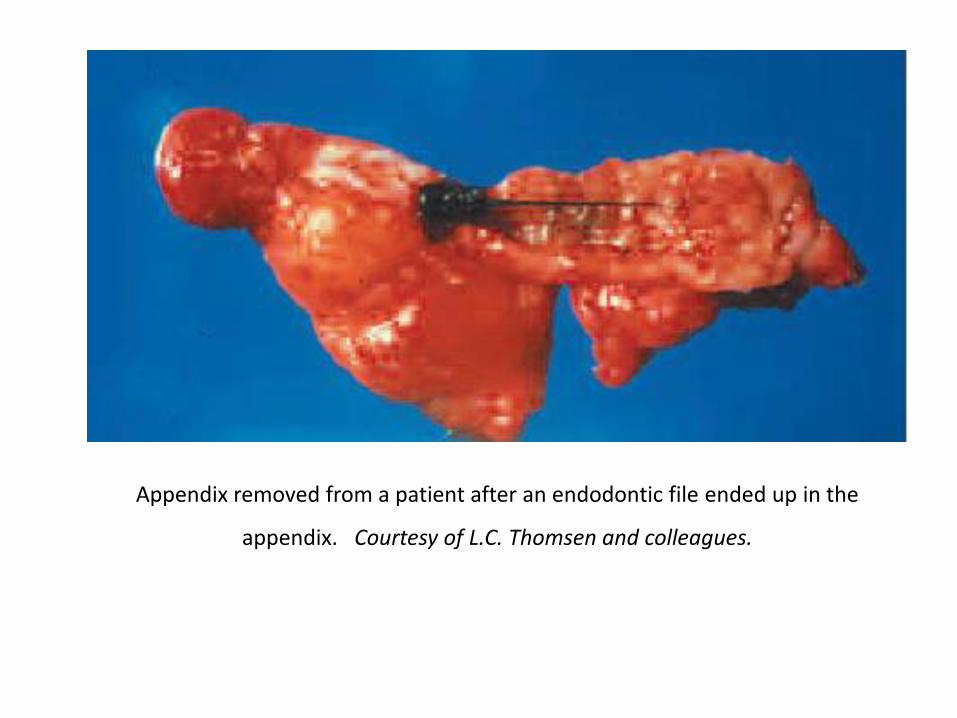
Appendix removed from a patient after an endodontic file ended up in the
appendix. Courtesy of L.C. Thomsen and colleagues.

Thank you