Embed Size (px)
Citation preview

Aetiopathogenesis
Vaibhav ShriyaVII Semester

Aetiologic Agent• family – human retroviriadae• subfamily – lentivirus• 2 types: HIV-1, HIV-2• m/c throughout the world = HIV-1• Both HIV-1, HIV-2 are zoonotic infections• Natural reservoir of HIV-1 = Pan troglodytes troglodytes {Chimps} (most likely source of original human infection)• HIV-2 more close to SIV (Simian Immunodeficiency Virus) than HIV-1 (about 40% resemblance to HIV-1 phylogenetically)

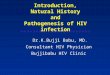
Morphology of HIV

MoTA. Sexual Transmission
• Predominantly STD worldwide• m/c MoT worldwide – heterosexual
transmission (2nd m/c MoT in dvlpd. nations)• HIV demonstrated in semen w/i infected
mononuc. cells (particularly high in epididymitis, urethritis), cell-free material
• Increased risk with (+) of STD’s genital ulcern (HSV, T. pallidum, H. ducreyi); nonulcerative infl. (C. trachomatis, N. gonorrhoeae, T. vaginalis)


• Vaginal intercourse – more MF than FM (?)
• Strong asso. with receptive anal intercourse (?)
• Extremely low asso. with oral intercourse (not 100% safe)
• OCP’s induces cervical mucosal change more chances of viral penetration
• Circumcision lowers risk of inf. in men (?)

B. Blood & Blood prdts.
• i.v, s.c, i.m• Whole blood transfusion, blood prdts. (Packed
RBC’s, WBC’s, platelets, plasma), transplant tissue
• Hyperimmune-gamma globulin, anti-HBV Ig, Rho Ig, plasma-derived HBV vaccine DON’T transmit HIV
• Now HIV tranfer via blood, organ transplant very rare d/t – scan for p24 Ag., viral ss-RNA, anti-HIV Abs., screen for HIV during HBV & HCV inf. test
• In Haemophiliacs clotting factors more safer than FFP d/t elimination of virus by heat t/t of clotting factors concentrate

C. Occupational (Health care workers & settings, Lab)
• Transmission of HIV by sharps = 0.3% (USA)• Transmission of HIV by contact of mucosa or non-
intact skin to HIV containing paraphernalia = 0.09%• Transmission of HIV by intact skin not
documented• Transmission of HIV by human biting other
human at least 4 cases reported• Risk of transmission of HIV by blood > other
bodily fluids (tears, saliva, urine, CSF, serous fluids, sputum, faeces, vomitus, etc.)

D. MTCT• m/c in perinatal pd. (50-60% risk of transmitting HIV)• can be transmitted as early as during I, II trimester• Higher MTCT correlated with closer HLA match
between mother, child• control:-
1. Universal voluntary HIV test, counseling of preg. female
2. HAART with >=1 drugs {lami.(NRTI’s), ZDV(NRTI’s)}
3. Reduce foet. exposure to mat. blood, gemital secretions
4. Avoid breast feeding** In dvlping. nations Nevirapine is cheap alter of
ZDV, lami.

E. Bodily fluids• HIV (+) in LOW titres in saliva no evidence to be
transmitted by kiss• (+) of anti-HIV IgA, M, G in saliva of infected
person• (+) of SLPI in saliva cleaves CD4 receptors• former USSR children infected with HIV (by
transfusion) had bleeding oral sore breast feeding laceration, abrasion around nipple by biting (breast feeding was continued until children were older) mother contracted HIV

Replication Cycle

HIV Provirus Genome

Pathogenesis• Virus enters body by diff. MoT• Undergoes replication cycle (mainly TH; sometimes NK, Macro., mono., glial, B-ly.) damages TH cells
Fig.: Mechanisms of CD4+ T-cell dysfunction & depletion

A. 1o inf., viral dissemination
Fig.: Summary of early events in HIV infection

B. Persistent Viral replication
Fig.: Generation of latently infected, resting CD4+ T-cells in HIV infected individuals

Fig.: Different immunologic effector mechanisms

C. Evasion of immune controlMainly foll. mechs. –
1.Sustained replication with high rate of mutn. & recombi. (RTase, gag encoded prots.) {1:104 bases copied}
2.Exhaustion of CD8+ CTL’s d/t (+) of PD-1 mol. on activated cells
3.Extensive N-linked Glycosylation of envelope (k/a GLYCAN shield)
4.Conformational masking of neutralizing epitopes
5. Sequestration of inftd. Cells in sites like CNS

Fig.: Elements of the immune response to HIV

D. Advanced HIV dz
Fig.: Events that transpire from primary HIV infection

Destruction of immunity by HIV
1. Opportunistic infns.
2. Autoimmunity
3. Neoplasms (esp. KS)• angioprolif. dz, not true sarcoma (at least initially)• excess prolif. of spindle cells of vasc. origin• 4 diff. epidem. forms: 2 are opportunistic infns.• interplay of R/F’s – HIV-1, HHV-8, immune actvn., cytokines• in HIV, % prev. of HHV-8 in KS in M:F = 35:4• HHV-8 is aetio. agent of KS
• mol. mimicry by viral components• Abs. to WBC’s, platelets, s. prots. (albumin, Ig, tgb)• cross-rxn. b/w gp120,41 & MHC-II• dzs like psoriasis, ITP, APAS, Grave’s dz, 1o biliary cirrhosis (+)
• TB (pul./extra-pul.)• P. jiroveci pnuemonia• Recurr. Salmonella septicaemia•CMV retinits• Oral hairy leukoplakia• Candida: oropx. thrush, vulvovaginitis• PID• Periph. neuropathy• HSV-1 infn.• Toxoplasmosis – brain• Cx – dysplasia• HZV (shingles)