Embed Size (px)
DESCRIPTION
teaching bangsal
Citation preview
TEACHING BANGSAL 1
SUSPEK MORBUS HANSEN
NAMA KELOMPOK
1. Dewi Gemala Wahab
2. Widuri wulandari
3. Ine Wahyudi Dean
4. Ratna Nur Aisyah
5. Riffatiyani Arsyad
6. Vany Matasak
7. Sinta
8. Hajratul Aswad Ute

PATIENT IDENTITYName : Yoseph Wenghu
Gender : Male
Age : 41 years old
Admission date : 16/02/2015
Medical record no : 700151
ANAMNESISA male patient came to consult from the Outpatient Unit with dyspneu and chest pain.
The patient has experiencing it since 2 weeks ago. The patient was also experienced a
chipped-red-spots on the face region, does not itch. Initially small in the chin area and
spreads to other areas in the cheeks and eyebrows. Efflorescence: macular
erythematous, scaly (+). The patient is a patient consulted from the Internal
Departement with dyspneu and chest pain. The patient was cosulted to the Dermatology
Departement because of the existence of red spots on the eyebrows, cheeks and chin.
These complains occurred since 2 weeks ago. Pain (-), Fever (-). No history of the same
disease and have never been treated before. Family with history of the same disease (-).
CURRENT STATUSConsciousness : good
General Condition : good
Hygiene : Moderate
Nutrition : Moderate
Vital sign :
BP : 100/70 mmHg
Pulse : 86x/minutes
RR : 28x/minutes
Temperature : 37,2˚C
DERMATO-VENEROLOGY STATUSRegio : Facialis
Efflorescence : Macula erythem, Skuama

REGIO FACIALIS
DIFFERENTIAL DIAGNOSISDermatitis seboroik
Tinea facialis
Psoriasis vulgaris
DIAGNOSISSuspek Morbus Hansen
DERMATITIS SEBOROIKDefinition : Seborrheic dermatitis is a common mild chronic eczema typically confined to skin regions with high sebum production and the large body folds. Although its pathogenesis is not fully elucidated, there is a link to sebum overproduction and the commensal yeast Malassezia.
Clinical Features :
sharply demarcated patches or thin plaques that vary from pink– yellow to dull red to red–brown in color with bran-like to flaky ‘greasy’ scales; vesiculation and crusting may occur but are rare and mostly due to irritation (e.g. overenthusiastic treatment)
limitation to those periods of life when sebaceous glands are active, i.e. the first few months of life and post puberty
a predilection for areas rich in sebaceous glands, e.g. the scalp, face, ears, presternal region and, less often, the intertriginous areas (e.g. the axillae, inguinal and inframammary folds, and umbilicus)
a mild course with little or moderate discomfort
Treatment: topical azoles (e.g. ketoconazole), either as shampoos (scalp) or as creams (body).
Second-line treatment options are zinc pyrithione and tar shampoos. Hydroxypyridone ciclopirox has antifungal and anti-inflammatory activities and has been shown to be effective as a shampoo or cream in double-blind

TINEA FACIALISDefinition : superficial infection of the epidermis caused by dermatophites
Effloresensi: scale, annular configuration, pustules in the border

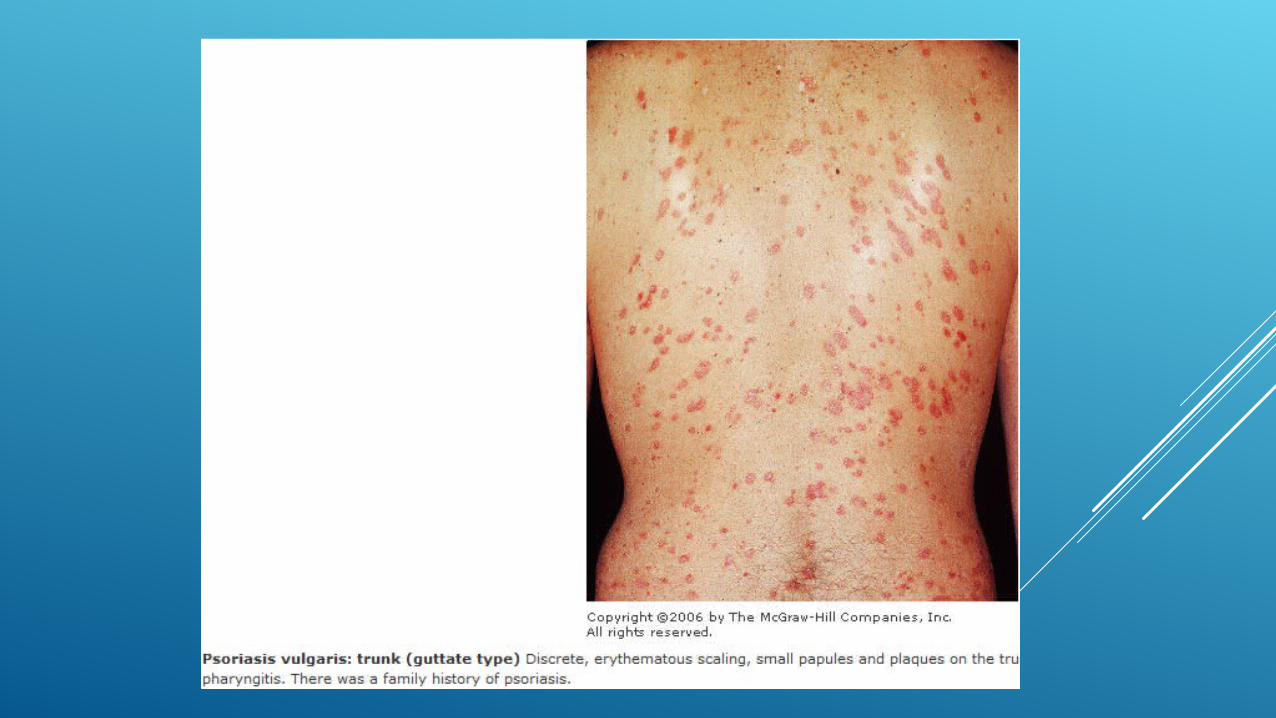
PSORIASIS VULGARISSkin Lesion: The classic lesion of psoriasis is a sharply marginated erythematous papule with a silvery-white scale. Scales are lamellar, loose, and easily removed by scratching. Removal of scale results in the appearanceof minute blood droplets (Auspitz' sign). Papules grow to sharply marginated plaques with lamellar scaling that coalesce to form polycyclic or serpiginous patterns. May occur anywhere on the body but there are classic predilection sites.
•Treatment: topical :corticosteroid, antralin, calcipotriol, derifat vit.D topical and analog vit.A, imunomudulator topical, keratolitik terapi (As.Salisil)
•Sistemik: metotrexat, acitretin, siclosporin,
TREATMENT PLAN
-Plan punch iopsi
-Carmed urea
-hidrokortison
DEFINITION AND ETIOLOGYDefinition:
Morbus Hansen is a chronic granulomatous disease caused by Mycobacterium leprae, principally affecting peripheral nerves and skin.
Etiologi:
Mycobacterium leprae
PATOFISIOLOGI
When the bacteria M. leprae enter the body, then the body will react issued macrophages derived from blood monocytes. mononuclear cells and histiocytes for his phagocytosis. Ability to phagocytosis depends on the immune system Schwann Cells are the target cells for the growth of M. leprae.
When going for the body's immune disorders in Schwann cells, bacteria can migrate and air activation. As a result of nerve regeneration activity is reduced, there is damage to the nerves that progressiv.
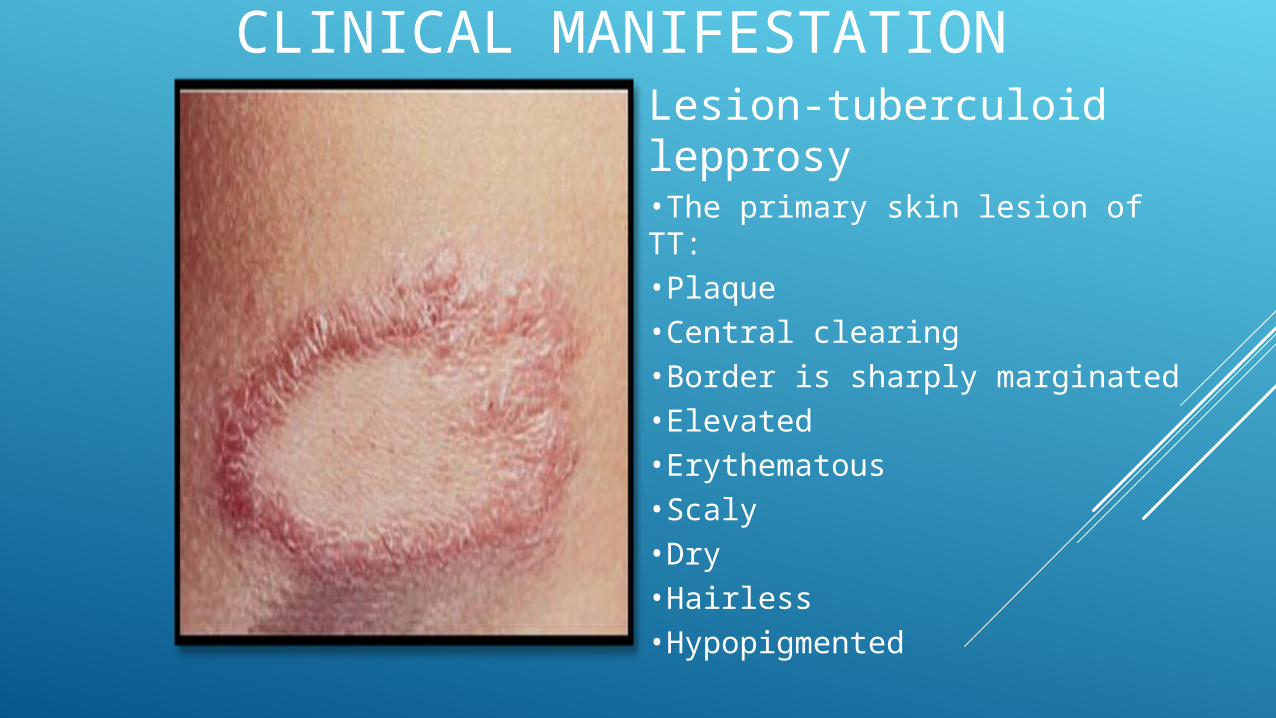
CLINICAL MANIFESTATIONLesion-tuberculoid lepprosy•The primary skin lesion of TT:•Plaque•Central clearing•Border is sharply marginated•Elevated•Erythematous•Scaly•Dry•Hairless•Hypopigmented
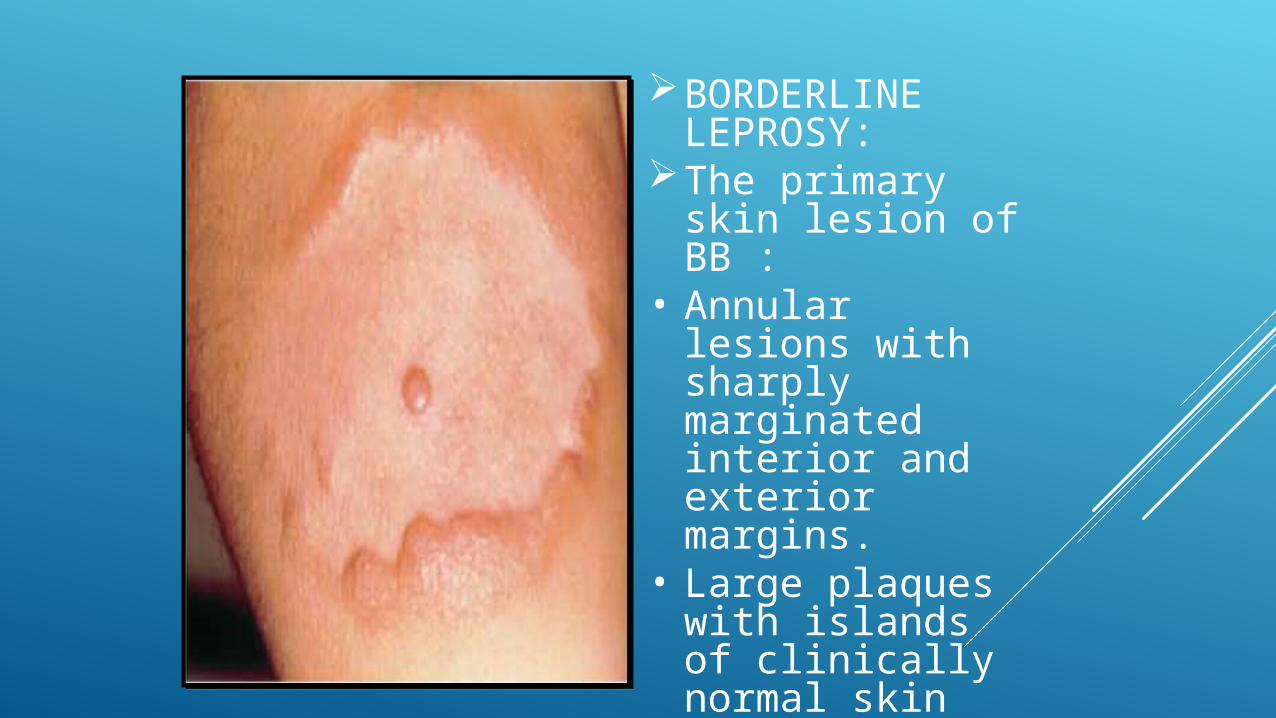
BORDERLINE LEPROSY:
The primary skin lesion of BB :
• Annular lesions with sharply marginated interior and exterior margins.
• Large plaques with islands of clinically normal skin within the plaque.
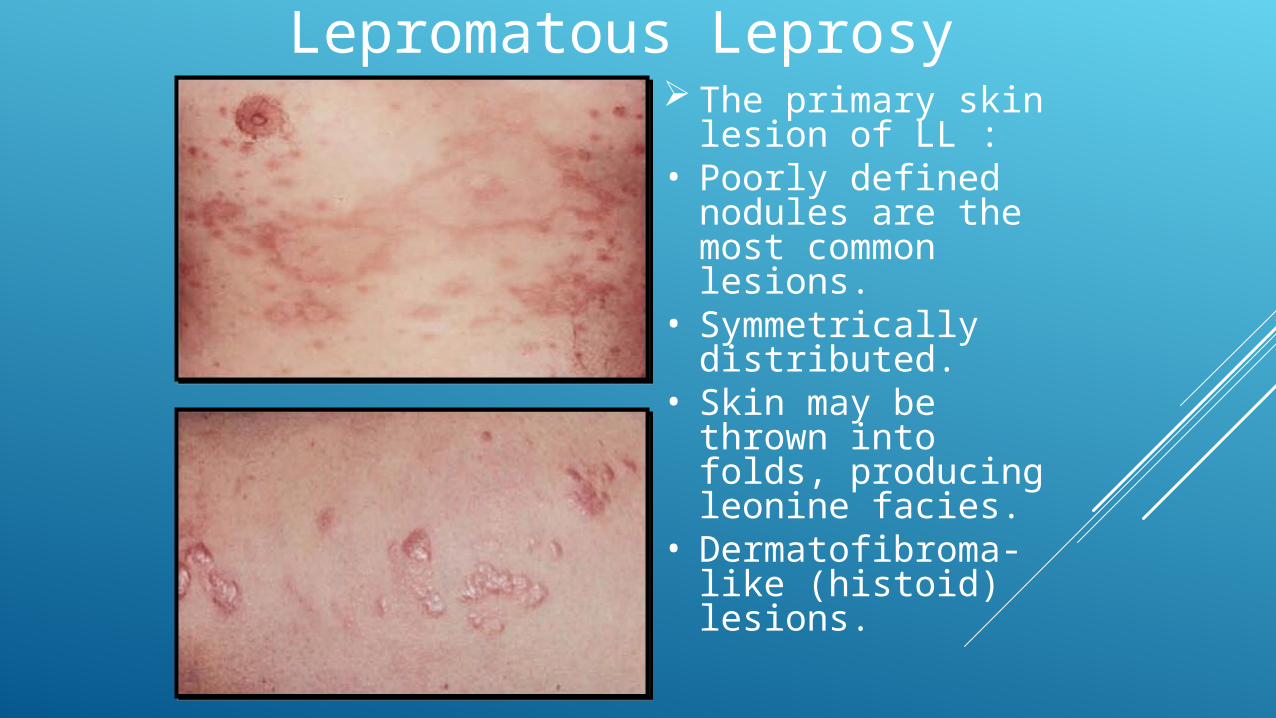
Lepromatous Leprosy The primary skin
lesion of LL :• Poorly defined
nodules are the most common lesions.
• Symmetrically distributed.
• Skin may be thrown into folds, producing leonine facies.
• Dermatofibroma- like (histoid) lesions.
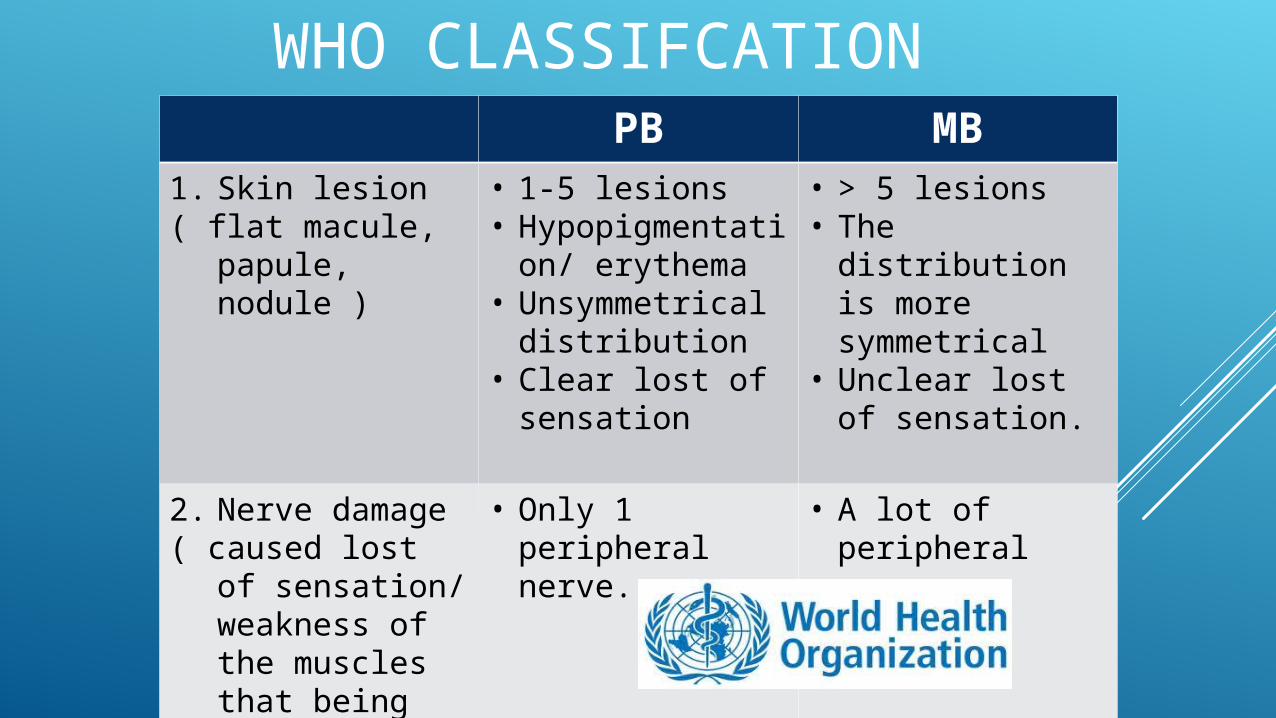
WHO CLASSIFCATIONPB MB
1. Skin lesion ( flat macule,
papule, nodule )
• 1-5 lesions• Hypopigmentati
on/ erythema • Unsymmetrical
distribution• Clear lost of
sensation
• > 5 lesions• The distribution
is more symmetrical
• Unclear lost of sensation.
2. Nerve damage ( caused lost of
sensation/ weakness of the muscles that being innervated by damaged nerves)
• Only 1 peripheral nerve.
• A lot of peripheral nerves
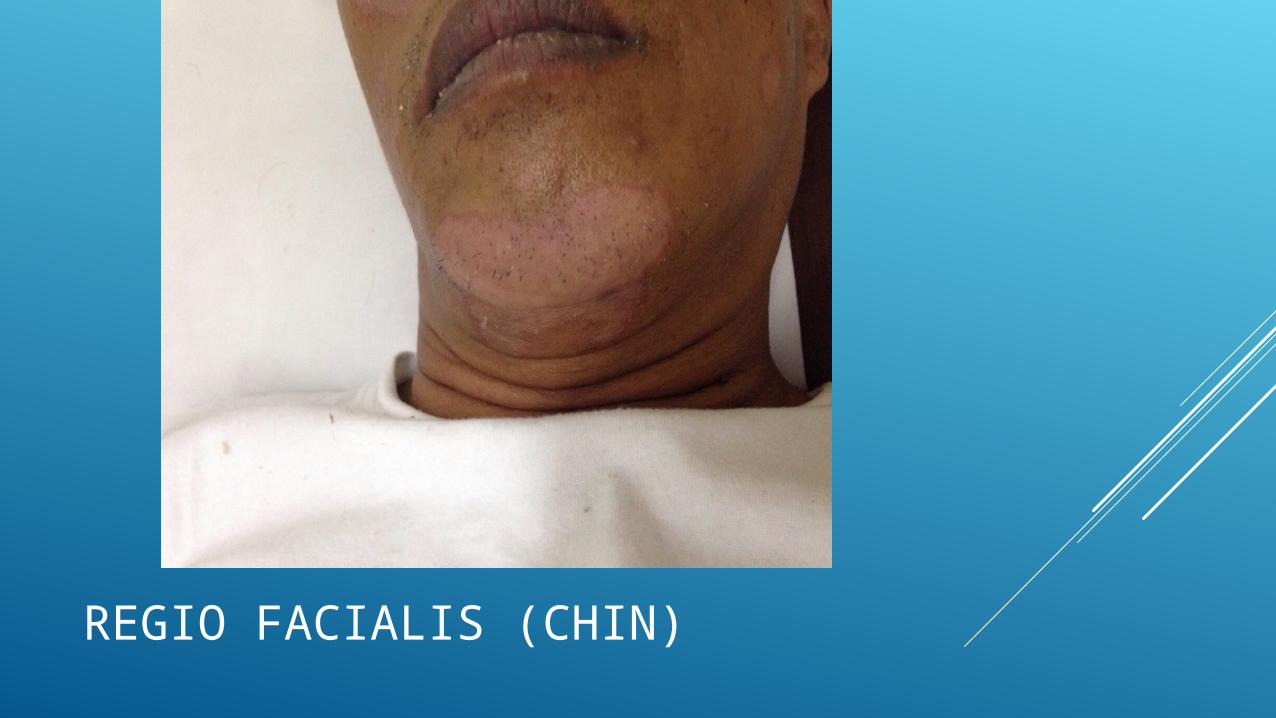
REGIO FACIALIS (CHIN)
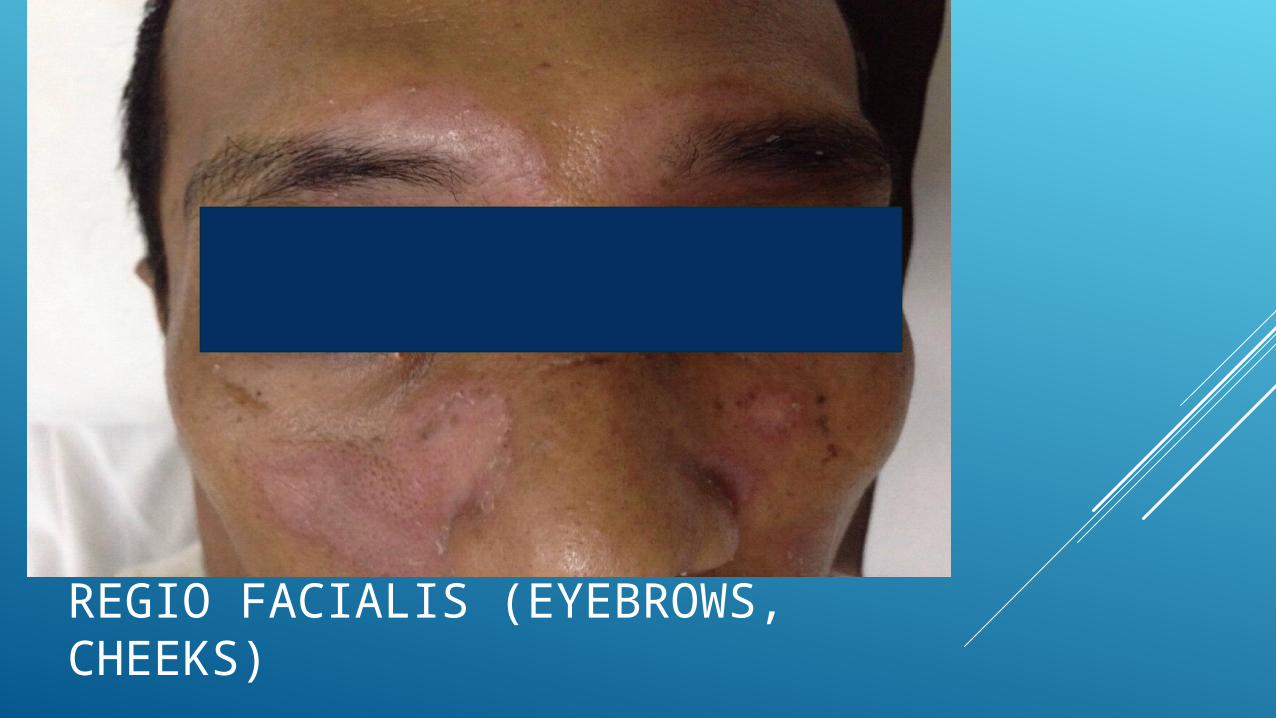
REGIO FACIALIS (EYEBROWS, CHEEKS)
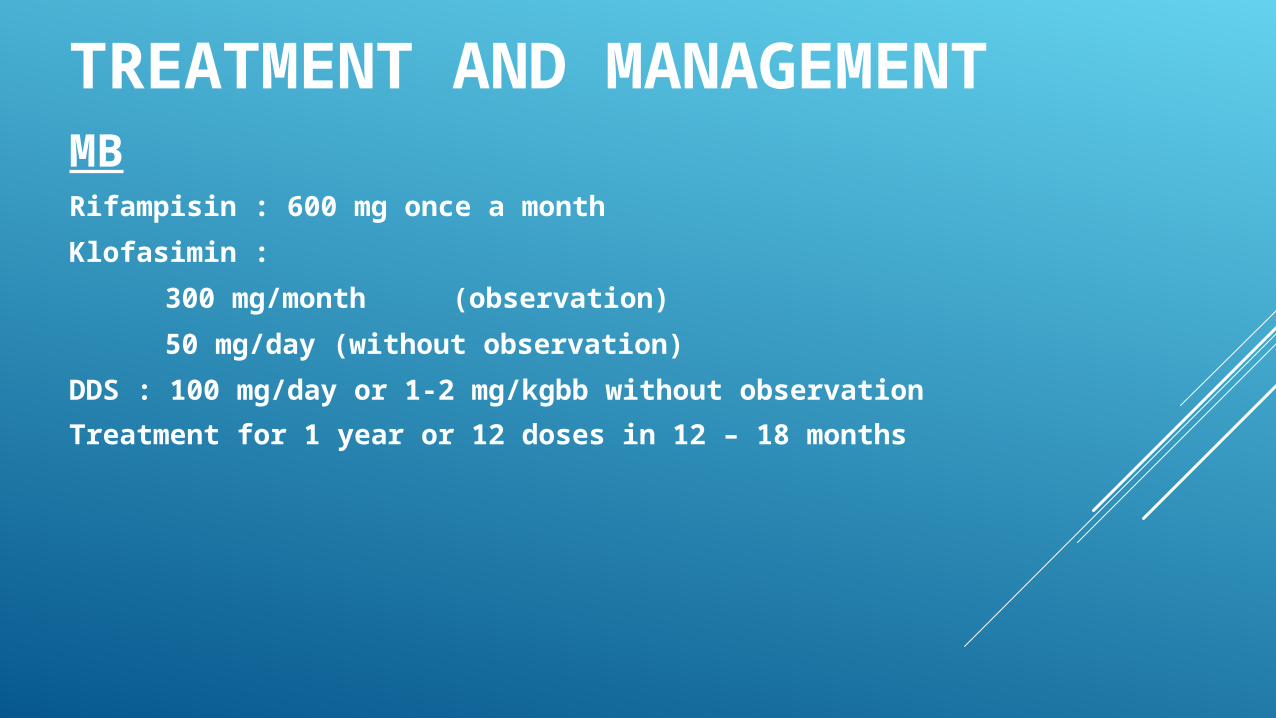
TREATMENT AND MANAGEMENTMBRifampisin : 600 mg once a month
Klofasimin :
300 mg/month (observation)
50 mg/day (without observation)
DDS : 100 mg/day or 1-2 mg/kgbb without observation
Treatment for 1 year or 12 doses in 12 – 18 months
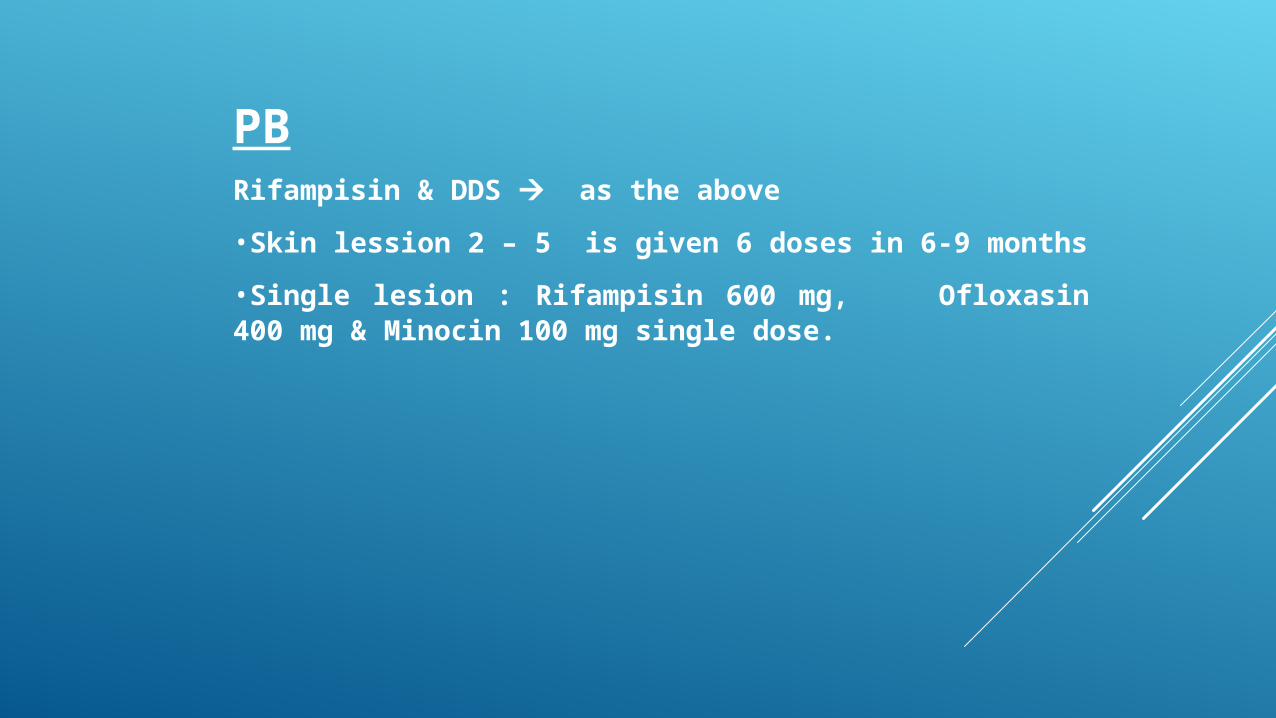
PBRifampisin & DDS as the above
•Skin lession 2 – 5 is given 6 doses in 6-9 months
•Single lesion : Rifampisin 600 mg, Ofloxasin 400 mg & Minocin 100 mg single dose.

POST TREATMENT