-
8/12/2019 (2014) Teaching Bangsal - NET
1/38
TOXIC EPIDERMAL
NECROSISTEACHING BANGSAL
-
8/12/2019 (2014) Teaching Bangsal - NET
2/38
GROUP MEMBERS KHAIRIYAH SURIATMAJAYA NADHIRAH BINTI MOHD. NOH
WANDRYATMO SANTOSA TONAPA JIMMY PATABANG SUDARMAN ARUNG T. ANDI DWI
RAHMAT ARMYN ANDI ALFISYA BAYU
NURIA IFTITAH DEDIKASIH ANDI TENRI ISMI SHANDRA RACHMAT
HIDAYAT
-
8/12/2019 (2014) Teaching Bangsal - NET
3/38
PATIENTS IDENTITY Name: Ms.Sarmina Gender: Female Age: 40 y.o
Marital Status: Married Religion: Islam Address:Jl.Dahlia
batangluku kab.gowa Occupation: Housewife Registered: August, 1st
2014
-
8/12/2019 (2014) Teaching Bangsal - NET
4/38
HISTORY TAKING
Chief complaint:Erotion and scale in whole bodyAnamnesis:
Patient is admitted to RS Wahidin in referralfrom RSUD Syeikh
Yusuf with complaint ofgeneralised erotion and scale of whole body
withoral lesion, red eyes and tearing as well asgenital laceration
since 1.5 month ago. Initially,the patient consumed cefadroxyl
three days
before skin manifestation.
-
8/12/2019 (2014) Teaching Bangsal - NET
5/38
The cefadroxyl was given as a treatment of
the patients ear due to infection witheffusion. There is also
complaint ofdifficulty in swallowing food and difficulty
in defecation and urination for more thanone week.The patient is
also consulted to otherdepartment which are Internal
Medicinedepartment, Opthamology department andENT department.
-
8/12/2019 (2014) Teaching Bangsal - NET
6/38
TREATMENT
Dexamethasone amp 15 mg/8 hrs/IV Kenalog Ora Base Lanolin 10% +
Vaselin 30g Biocream - Face IVFD : RL/NaCl/Dextrose 5% =
1:1:1
-
8/12/2019 (2014) Teaching Bangsal - NET
7/38
Dermatovenerology status
Location : GeneralisedEfflorescence : scale (+), erosion
(+), crust (+), madidans
-
8/12/2019 (2014) Teaching Bangsal - NET
8/38
Additional examination:- Complete Blood Count (CBC)August 1st,
2014WBC : 16,3 10 3uLHB :10,71 g/dLAugust 4th, 2014WBC: 19,29 10
3uLHB: 9,1 g/dL
-
8/12/2019 (2014) Teaching Bangsal - NET
9/38
PRESENT STATUS
General condition : severe illnessConsciousness :
composmentisVital sign :BP : 180/70 mmHgPulse : 100x/minute
RR : 32x/iTemperature : 38,4 C
-
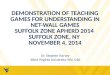
8/12/2019 (2014) Teaching Bangsal - NET
10/38First photo during admission
-
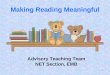
8/12/2019 (2014) Teaching Bangsal - NET
11/38
Sixth day of treatment
-
8/12/2019 (2014) Teaching Bangsal - NET
12/38
Diagnosis and Treatment fromInternal Medicine Department
Subdivision : TropicalInfection
Subdivision : GEH
A/ Sepsis ec SSTI A/ GEH
P/ - O2 3 Ltr via nasal canul- Ceftriaxone 2 g/24 hrs/dripsin
100 cc NaCl 0.9%
- Sistenol 3x1
P/ - Diet hepar- HP Pro 1-1-1- Vip Albumin 3x1- Urdahex 250 mg
0-1-1
Additional Exam::SGOT : 32SGPT : 94Ureum : 213Keratin : 1,07
-
8/12/2019 (2014) Teaching Bangsal - NET
13/38
Diagnosis and Treatment fromOpthamology department
A/ ectropion ODS Tx/ - C. Lyters ODS 6x1 gtt ODS
- C. Polygran 3x1 gtt ODS
-
8/12/2019 (2014) Teaching Bangsal - NET
14/38
A/ - Acute Tonsillopharyngitis- Otitis Media Externa
Profunda
Difus dextra et sinistra
P/ - Oral betadine- Burowi Tampon
Diagnosis and Treatment from ENTDepartment
-
8/12/2019 (2014) Teaching Bangsal - NET
15/38
Toxic Epidermal Necrolysis (TEN)
-
8/12/2019 (2014) Teaching Bangsal - NET
16/38
DEFINITION
Toxic Epidermal Necrolysis (TEN) is anacute life-threatening
mucocutaneus
reaction which characterized by mucousmembrane erosion,
necrolysis, andextensive epidermal detachment.
-
8/12/2019 (2014) Teaching Bangsal - NET
17/38
The difference between SJS and TEN
is the involvement of body surfacearea (BSA)
< 10% BSA : SJS10-30% BSA : overlapping SJS-TEN
> 30% : TEN
-
8/12/2019 (2014) Teaching Bangsal - NET
18/38
EPIDEMIOLOGY SJS and TEN are very rare cases. Cases incidence of
SJS :
1-6 cases per million persons-years Cases incidence of TEN :
0,4-1,2 cases per million persons-years Occurs at any ages
Increasing risk : age after the 4 th decade Women > Men
-
8/12/2019 (2014) Teaching Bangsal - NET
19/38
ETIOLOGY
Primary cause : DRUGS High risk drugs : sulfonamide
antibacterial,
aromatic anticonvulsant, allopurinol, oxicam NSAID, lamotrigine,
and nevirapine.
Other etiologies : Mycoplasma pneuomoniae infection,
vaccination, graft-versus-hostdisease, and radiation.
-
8/12/2019 (2014) Teaching Bangsal - NET
20/38
PATHOGENESIS
I mmunologic pattern of early lesion : cell-mediated cytotoxic
reaction against
keratinocytes massive apoptosis presence of CD8 T-killer
lymphocytes in
dermis and epidermis
CD8 T-killer lymphocyte express - T-cellreceptors and are able
to kill through perforinand ganzyme B
-
8/12/2019 (2014) Teaching Bangsal - NET
21/38
presence of other cytokines, like IL-6, TNF- ,
and Fas-L
I mmunologic pattern of late lesion : >>> monocytes
-
8/12/2019 (2014) Teaching Bangsal - NET
22/38
CLINICAL MANIFESTATION
Prodromal symptoms (1-14 days): fever, sore throat, chills,
headache, malaise
Mucocutaneous lesions : macule that develope into papules,
vesicles,
bullae, urticarial plaques, or confluenterythema targetoid
lesions
-
8/12/2019 (2014) Teaching Bangsal - NET
23/38
MUCOSAL LESIONS
M outh : hemorrhage andcrust on lips
erosions in mouthcovered by necroticwhite
pseudomembrane ulcerativestomatitis
Geni tal : painful erosions
Eyes :
erosiveconjunctivitis corneal ulcer
-
8/12/2019 (2014) Teaching Bangsal - NET
24/38
DIAGNOSIS
1. H istory Taking
- Non-specific symptom (1-3 days) : fever,stinging eyes, pain
upon swallowingheadache, rhinitis, myalgia.- Epidermal necrolysis :
8 weeks after drugsconsumption- Initial lesion : erythema macula
(bodytrunks, then spread to other body sites)
-
8/12/2019 (2014) Teaching Bangsal - NET
25/38
2. Physical Examination Skin :
- irregular-shaped erythema,hyperpigmentations, purpuric
macules- targetoid lesion- confluent necrotic lesions- Nikolsky
sign (+)- lesions evolve into flaccid blisters
-
8/12/2019 (2014) Teaching Bangsal - NET
26/38
Mucous membrane:
- buccal, ocular, genital mucous- painful erythema and erosion-
impaired function (impaired alimentation, photophobia, conjunctival
synechiae,dysuria)
-
8/12/2019 (2014) Teaching Bangsal - NET
27/38
3. Laborator ium Examination Blood Examination
- anemia - lymphopenia-leukocytosis - mild thrombocytopenia
- eosinophilia - neutropenia- blood urea nitrogen - serum urea -
electrolyte imbalance - serum bicarbonate
- hypoalbuminemia - hypoproteinemia
-
8/12/2019 (2014) Teaching Bangsal - NET
28/38
Immunologic Examination- perifer CD4 lymphopenia
4. Dermatopathology Examination
- sparse apoptotic keratinocytes (suprabasallayers) which
rapidly evolve to a full-
thickness EN and sub-epidermal detachment- mononuclear cell
infiltrate
-
8/12/2019 (2014) Teaching Bangsal - NET
29/38
- among T cells : lymphocytes CD8 with phenotypic features of
cytotoxic cells
- eosinophils : less common in patients with
the most severe form of TEN.
-
8/12/2019 (2014) Teaching Bangsal - NET
30/38
SCORTEN (Score of Toxic Epidermal Necrolysis )
Fitzpatricks Dermatology in General Medicine 8th Edition
-
8/12/2019 (2014) Teaching Bangsal - NET
31/38
THERAPY
Early recognition Prompt withdrawal of the offending drugs
1. Symptomatic Treatment Only patients with limited skin
involvement and
SCORTEN score of 0 or 1. Manage replacement of IV fluid and
electrolytes Nutrition support (nasogastric tube)
-
8/12/2019 (2014) Teaching Bangsal - NET
32/38
Environmental temperature : 28C 30C Eyes : - examined daily by
ophtalmologist
- artificial tears, antibiotic or antisepticeyedrops, vitamin A,
mechanicaldisruption of early synechiae
Pruritus : antihistamine
-
8/12/2019 (2014) Teaching Bangsal - NET
33/38
2. Specif ic Treatment High-dosed IV IG : 0,75 mg/kg/day for
4
consecutive days Cyclosporin : 3 mg/kg/day Plasmapharesis or
Hemodialysis : prompt the
removal of the offending drugs, itsmetabolites, or inflammatory
mediators.
-
8/12/2019 (2014) Teaching Bangsal - NET
34/38
Corticosteroid :- controversial- given in early phase-
dexamethasone 40 mg/day
Cyclosporine A- powerful immunosuppressive agent
- activates of T helper 2 cytokines, inhibitionof CD8+ cytotoxic
mechanisms, andantiapoptotic effect
-
8/12/2019 (2014) Teaching Bangsal - NET
35/38
DIFFERENTIALDIAGNOSES
-
8/12/2019 (2014) Teaching Bangsal - NET
36/38
SJS TENERYTHEMA
MULTIFORMS.S.S.S
PEMPHIGUSVULGARIS
Etiology
drugs, infection,vaccination, graft-
versus-host disease,radiation
drugs, infection,vaccination, graft-
versus-hostdisease, radiation
autoimmune,drugs, viral or
bacterial infection
Staphylococcus
aureus
genetic,
autoimmune
ClinicalFeatures
macule, papule, plaque, erosion,ulcer, necrosis,
blistering,conjunctivitis
macule, papule, plaque, erosion,ulcer, necrosis,
blistering,conjunctivitis,
epydermolysis, Nickolsky sign (+)in erithematous
area
erythematousmacule, well-marginated,
edematous papule,iris lesion
desquamation,skin exfoliative in
sheets, lesionsmore superficial
(granular layer), Nickolsky sign(+)
mucous erosionand thin-walled,
flaccid, easilyrupture bullae,
Nickolsky sign(+)
Predilection trunk, palms, soles trunk, palms, soles
dorsal hands
symmetrically,acrally
neck, groin,axillae
mouth, burn orskin injury sites
Age
increasing risk atage > 40 y.o
woman > man
increasing risk atage > 40 y.o
woman > man
adolescence neonates &children
middle age
woman = man
-
8/12/2019 (2014) Teaching Bangsal - NET
37/38
COMPLICATIONS
Acute phase : sepsis is the most commoncomplication
Respiratory system : bronchopneumonia Genitourinary system :
acute tubular necrosis,
renal failure, penile scar, or vaginal stenosis Gastroenterology
system : esophageal stricture Ocular system : corneal ulcer,
anterior uveitis,
panophtalmitis, blindness
-
8/12/2019 (2014) Teaching Bangsal - NET
38/38
PROGNOSIS
SJS TEN : life-threatening diseases Overall hospital mortality
of TEN is 22-25%
Mortality rate of SJS : 5-12% Mortality rate of TEN :
>30%