Embed Size (px)
Citation preview

Surveillance of hepatitis C Infection in France
JC Desenclos,
Département des Maladies Infectieuses
Institut de Veille Sanitaire

Outline• Background• Ongoing Surveillance
– HCV screening activity– newly treated patients in reference centres– blood donors & residual risk– indicators of arm reduction activities– nosocomial HCV infections
• Repeated surveys– HIV-HCV co-infection– prevalence and % of HCV infected screened– HCV associated deaths
• Other projects

HCV national prevention and control plan
• National plan initiated by the Ministry of Health• Planned at the regional level• Secondary and tertiary prevention
– screening of at risk groups (goal : 70% in 2002) – early follow up, management and treatment
• Primary prevention– blood (NAT, 2001) and organ donation safety
– harm reduction policy among IV drug users– control of iatrogenic transmission
• health care related (standard precautions…)• tattooing, piercing…
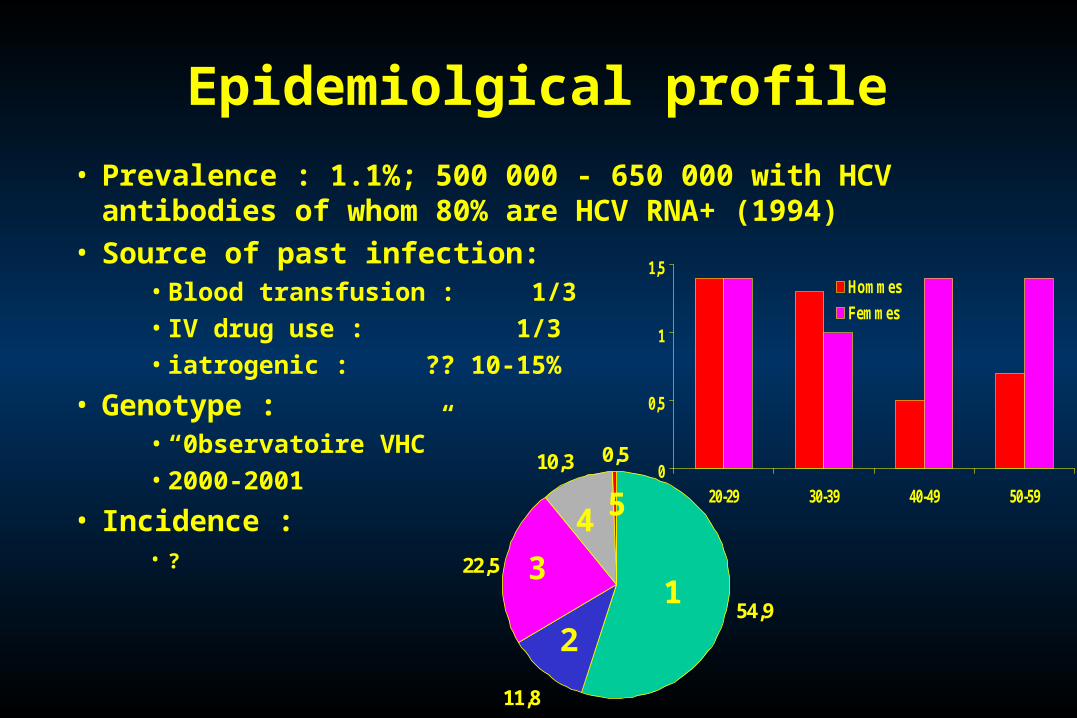
Epidemiolgical profile
• Prevalence : 1.1%; 500 000 - 650 000 with HCV antibodies of whom 80% are HCV RNA+ (1994)
• Source of past infection:• Blood transfusion : 1/3• IV drug use : 1/3• iatrogenic : ?? 10-15%
• Genotype :• “0bservatoire VHC”• 2000-2001
• Incidence : • ?
0
0,5
1
1,5
20-29 30-39 40-49 50-59
Hommes
Femmes
54,9
11,8
22,5
10,3 0,5
1
2
3
4 5

Centre*Centre*0,8 %0,8 %
IdFIdF**0,9 %0,9 %
Lorraine*Lorraine*1,0 %1,0 %
PACA*PACA*1,7 %1,7 %
Lyon : 1,3%
Fécamp : 1,9%
Prevalence of HCV serum antibodies in 4 regions, France, 1994

0
20
40
60
80
1993 1995 1997 2000
IV drug use
Transfusion <91
Others
Total
%
Year
Proportion of HCV positive subjects who knew their status when screened, Social security examination center,
Région Centre, France, 1993-2000
Source : Dubois et al, Concours Médical

Objectives of HCV surveillance• Data for decision making
– burden– trends– risk factors
• Evaluate prevention and control programs– screening activities– blood safety– IVDU harm reduction
• Disease control : outbreak detection, investigation and control
• Link and interaction with public health research

Surveillance of laboratory HCV antibody screening activity
• RENAVHC : network of hospitals and public laboratories nationally distributed (N = 257)
• Initiated in 2000• Activity by quarter
– monitor screening activities– number of serologic tests done and of positive– test confirmation activity– basic characteristics of positive tests
• Analysis by quarter and region (n = 22)

Screening activity by quarter, RENAVHC network (n=257), France 2000
Quater 2000 Number of tests
(ELISA, Immunoblot)
%
Positive
January - March 113 834 5,1
Aprill – June 110 327 5,2
Juilly - September 103 737 4,7
Octobrer- Décember 118 254 5,0
Total 446 152 5

Newly referred patients in hepatitis C reference centers
• 30 reference centers– hepatology or gastro-enterology centers– designated by the ministry of health– coordinate a regional network of clinical care, information,
treatment, prevention, training…
• National surveillance network– reference centers-InVS (23 in 2000; 25 in 2001)– trend overtime in patient characteristics– case definition : newly referred hepatitis C
– data : clinical, epidemiological and virological

Newly referred HCV patients, “pôles de référence, 2000” : mode of discovery of HCV
Mode of discovery
1 modalité de découverte
WomenN = 718n (%)
MenN = 948n (%)
TotalN = 1666
n(%)Systematic check up(blood donation, pre surgery check up…)
248 (34,5) 282 (29,8) 530 (31,8)
Risk factor 175 (24,4) 333 (35,1) 508 (30,5)
Diagnostic procedure following symptoms orbiologic abnomalities(anomalie des tests hépatiques, complication decirrhose, bilan d’un carcinome hépato-cellulaire)
170 (23,7) 186 (19,6) 356 (21,4)
Others 125 (17,4) 147 (15,5) 272 (16,3)

Newly referred HCV patients, “pôles de référence, 2000” : clinical stage
Clinical stage N = 1559n (%)
Normal ALT 317 (20,3)
Chronic hepatitis 1064 (68,3)
Compensated Cirrhosis 129 (8,3)
Decompensated cirrhosis 24 (1,5)
Carcinoma 16 (1,0)
Acute hepatitis 9 (0,6)
9,8 *
* 1991-1993 : 20%; F. Roudot-Thoraval et al. Hepatology 1997 ; 26 : 485-90

Newly referred HCV patients, “pôles de référence, 2000” : source of infection
Suspected source of Women Men
infection n (%) n (%) Transfusion 359 46,2 281 27,1
IV drug use 183 23,2 518 49,5
Nasal drug use 37 5,1 131 4,1
Professional exposure † 35 4,5 20 1,9
Nosocomial exposure ‡ 146 18,4 136 12,9
Other factors ¶ 146 18,7 202 19,4
No risk factors 99 12,3 115 10,7
total >100%, > to more than 1 risk factorr; †health care related ;
‡ dialysis, surgery, endoscopy ; ¶ acupuncture, injections, piercing,
sexual partner HCV+
* : in 1991-2003 : 34 and 25%, respectively
34*
38*HCV-HIV co-infection : 7%

Surveillance of blood safety
• Collaborative surveillance between blood centers & InVS
• HBV, HCV and HIV markers– all donors– repeat donors– denominators– characteristics of positive patients
• Incidence among repeat donors• Estimate of residual risk

Incidence of HIV, HBV, HCV and HTLV among Incidence of HIV, HBV, HCV and HTLV among repeat blood donors, France, 1992-2000repeat blood donors, France, 1992-2000
0,00,0
1,01,0
2,02,0
3,03,0
4,04,0
5,05,0
6,06,0
1992-941992-94 1993-951993-95 1994-961994-96 1995-971995-97 1996-981996-98 1997-991997-99 1998-001998-00
HCVHCVHTLVHTLV
HIVHIVHBVHBV
Source : GATT, InVS, INTSSource : GATT, InVS, INTS
Cases per 100 000 person year
3 years moving period

Residual risk of transmission of blood-borne Residual risk of transmission of blood-borne viruses per million blood donations, 1992-2000viruses per million blood donations, 1992-2000
(Transfusion; 2002, in press(Transfusion; 2002, in press))
Source : GATT, InVS, INTSSource : GATT, InVS, INTS
0,00,0
1,01,0
2,02,0
3,03,0
4,04,0
5,05,0
6,06,0
7,07,0
8,08,0
9,09,0
1992-941992-94 1993-951993-95 1994-961994-96 1995-971995-97 1996-981996-98 1997-991997-99 1998-001998-00
HCVHCV
HTLVHTLVHIVHIV
HBVHBV
3 years moving period
Risk per 1 000 000

Harm reduction activities : SIAMOIS• National data-base, stratified by district• Delivery indicators
– number of syringes sold– number of steribox kit sold– amount of subutex sold– methadone
• Impact indicators– overdose deaths– arrests for drug offense
• National and local monitoring• Sharp drop in 1ml syringe sale in last year

Notification of nosocomial infection events
• Introduced in 2001• Nosocomial sentinel events
– based on criteria; no positive nor negative list– HCV and HBV infection following medical care
• Notification – to local district health offices – inter-regional nosocomial coordination centers– national coordination : RAISIN-InVS

Examples of notification of HCV iatrogenic transmission since July 2001
• Outbreak in an haemodialysis center, 2001– 22 new infections; incidence : 52%person years– 3 genotypes– major breaches in hygiene procedures– case-control study: infection associated with :
• care by a nurse who had just cared for an HCV+ patient• not to dialysis on a machine used previously by an HCV positive patient
• Seroconversions associated with : – endoscopy (1) – inappropriate use of a glucometer (1)

Surveys
• Seroprevalence and behavioral surveys of IV drug users (InVS, INED, ANRS)– multi-city (5 to 6 large urban area)– cluster (multi site) probability sample– blood (finger) taken for HIV, HCV and HBV– questionnaire– pilot done in Marseille (April 2002)
• Prevalence of HIV-HCV co-infection• National seroprevalence survey

HIV-HCV co-infection
• National probability sample of HIV wards – one day survey (June 2001)– in- and out- HIV positive patients– basic epidemiological and clinical characteristics
• Results – N = 1744 – co-infecion : 28% (25-30 000 patients)
• Among HCV patients, HIV infection : 7%
• New survey planned in 2003– hepatitis B markers– include hepatology wards

% HCV infection among HIV patients, France, June 2001
Caractéristiques Catégories
Patients
VIH+ (N)
% séropositifs
pour VHC
RégionPACA 219 43Ile-de-france 836 25Autres régions 691 23
SexeHommes 1175 27Femmes 569 26
AgeMoins de 35 392 1835 à 44 ans 821 3845 ans et plus 521 15
Stade VIHStade A 627 25Stade B 400 31Sida 693 25
TransmissionToxicomanes 394 84Transfusés 64 53Homosexuels 562 6Hétérosexuels 621 9

Population survey• Aim : evaluate HCV prevention plan
– prevalence by age (18-80), gender, region (5 inter-regions) and social status (low vs others)
– % of HCV+ subjects who knew HCV status– % of HCV+ patient that are taken in charge
• Stratified probability cluster sample of social security affiliated– N = 15 000– HCV and HBV– Planned for last quarter of 2002
Mortality associated with hepatitis C
• Vital statistics• Specific viral hepatitis included in 10th ICD• Not available in the 9th ICD:
– chronic hepatitis– cirrhosis– carcinoma
• Survey of death certificates (CépiDC-InVS) – retrospective survey of certifiers and medical records– random sample of certificates with mention of liver conditions and
HIV– done in 1997 and planned in 2003 for (HCV and HBV)

Death associated with chronic hepatitis per 100 000 population, by gender, France,
1979-1998. Source : CépiDC-INSERM
0,0
0,2
0,4
0,6
0,8
1,0
1,2
1,4
Hommes
Femmes
Taux de décès / 100 000

Representative sample of death certificates with mention of liver disease (N = 360),
France, 1997
Cause of death Number Viral hepatitis 140 Other infections 40 Liver tumor 50 Other liver diseases 60 Cirrhosis 70
Total 360
Source : CépiDC

Estimate of the number of deaths associated with HCV in 1997
• By applying sampling fraction• Deaths : 1 837, 95% CI : 1 740 - 1 930• Death per 100 000 : 3,2; 95% CI : 2,9 - 3,3• Initial versus associated cause of death :
– initial : 630– associated cause : 1207
• major role : 564• not major : 643
– Total : 1837
Source : CépiDC

0
5
10
15
20
25
<25 25-44 45-64 >64 Tous âges
HommesFemmes
Total
Age
Death per 100 000
Death rate associated to HCV infection by age and gender, France, 1997
Source : CépiDC

Disease registries
• Cancer registriy (Francim)– all cancers (liver cancer included)– covers 10 districts (12% of population)– certified, coordinated and funded jointly by InVS and
INSERM– being strengthened to monitor long term trends
• Cirrhosis registry– no registry in France– interaction between HCV, HBV and alcohol

Public health research conducted under the auspices of ANRS
• Case control study of HCV seroconversions– plan to include 70 cases and 280 controls– ongoing
• Cohort study of HCV- intravenous drug users– north and east of France– one year follow up– basic incidence rate : ~ 10% person year
• Sociological research : perception, barriers to screening, follow up, treatment; quality of life...
• Cost-efficacy studies...





























