Embed Size (px)
DESCRIPTION
kul bahan
Citation preview
SEPSIS
dr. Donnie Lumban Gaol, SpPD
DAHULU
“Sepsis” the Greek word for putrificationDenoted tissue breakdown that resulted in illness

SEPSIS
EPIDEMIOLOGI MORTALITAS DAN MORBIDITAS ETIOLOGI DEFINISI MANIFESTASI KLINIK PATOGENESIS DIAGNOSIS PENATALAKSANAAN
EPIDEMIOLOGI
1995: 6 million records analyzed from 7 states
750,000 cases of severe sepsis occur annually
( 3/ 1000) Mortality 28.6% or 250,000 deaths Projected increase by 1.5% per year
Angus et al , CCM 2001, 29: 1303-1310
SEPSIS
EPIDEMIOLOGI MORTALITAS DAN MORBIDITAS ETIOLOGI DEFINISI MANIFESTASI KLINIK PATOGENESIS DIAGNOSIS PENATALAKSANAAN
MORTALITAS DAN MORBIDITAS
Angka mortalitas secara keseluruhan sekitar 28.6%, setara dengan 215.000 kematian tiap tahun di Amerika Serikat.
Faktor-faktor yang mempengaruhi pada awal kematian adalah jumlah sistem organ yang terlibat, rendahnya pH darah arteri, dan skor SAPS, MEDS24 atau APACHE yang tidak baik
Angus DC, et al. Crit Care Med 2001
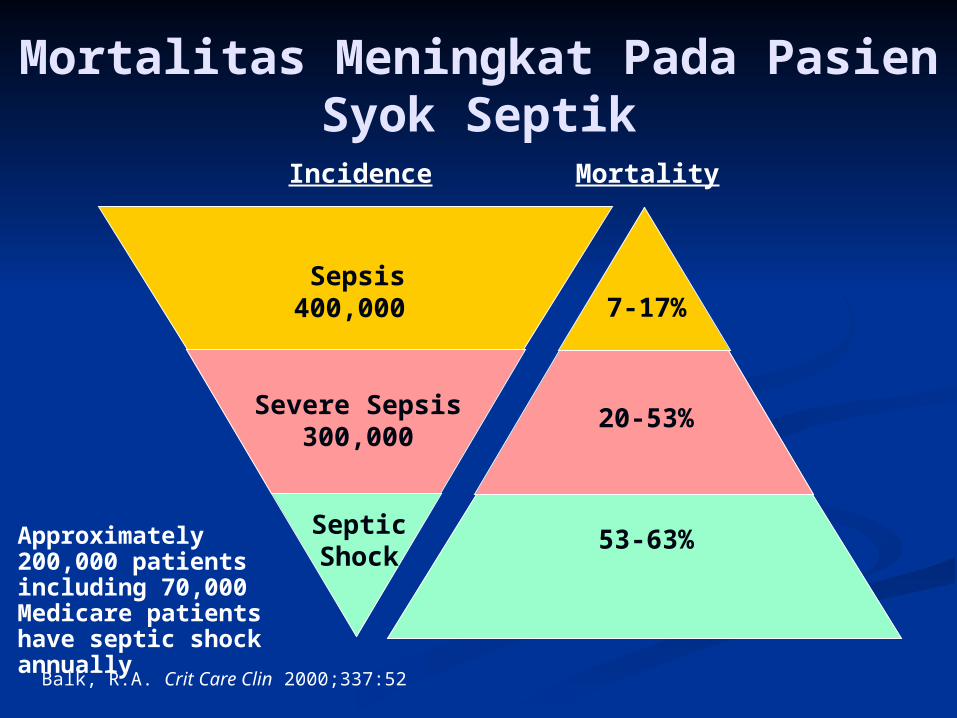
Mortality
Septic Shock
53-63%
20-53%Severe Sepsis300,000
7-17%Sepsis
400,000
Incidence
Balk, R.A. Crit Care Clin 2000;337:52
Mortalitas Meningkat Pada Pasien Syok Septik
Approximately 200,000 patients including 70,000 Medicare patients have septic shock annually
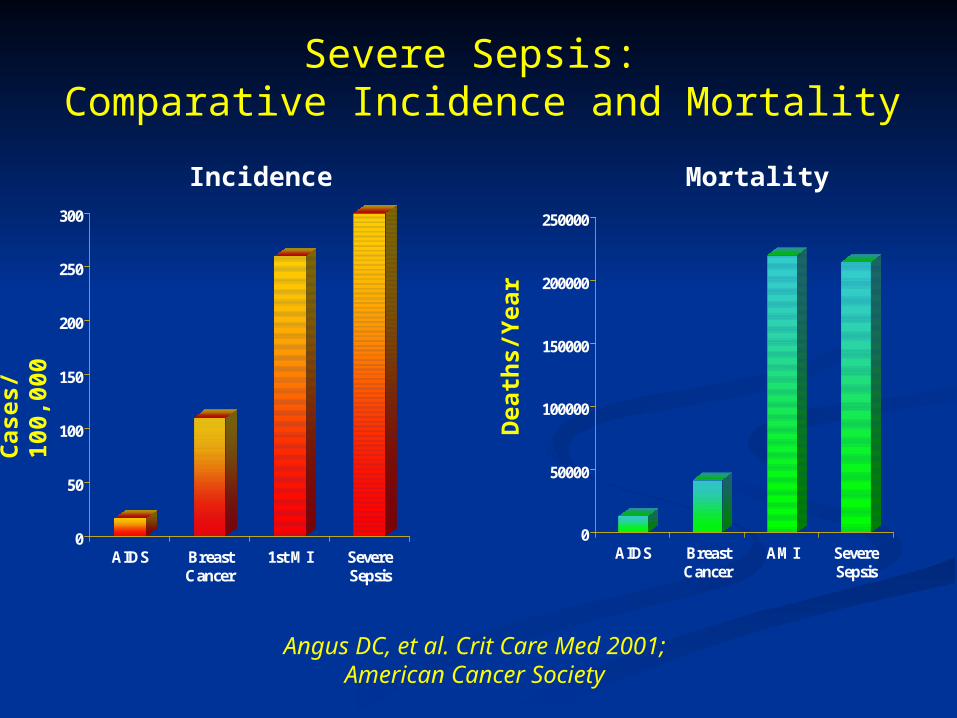
Severe Sepsis: Comparative Incidence and Mortality
Angus DC, et al. Crit Care Med 2001; American Cancer Society
0
50
100
150
200
250
300
AIDS BreastCancer
1st MI SevereSepsis
Incidence
Cas
es/1
00,0
00
0
50000
100000
150000
200000
250000
AIDS BreastCancer
AMI SevereSepsis
Mortality
Dea
ths/
Yea
r
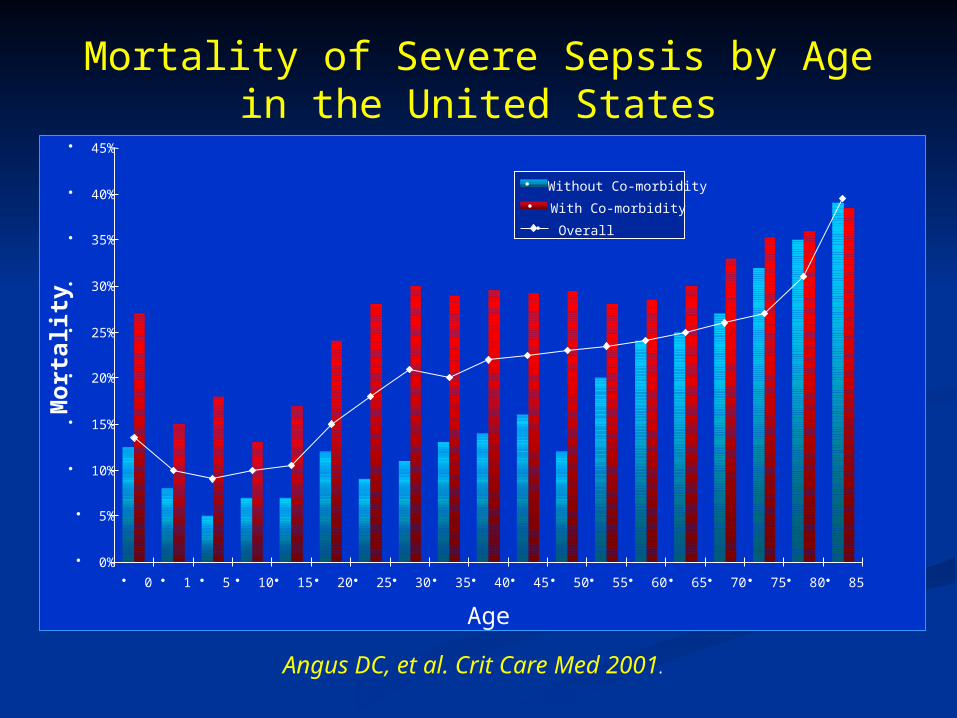
Mortality of Severe Sepsis by Age in the United States
Angus DC, et al. Crit Care Med 2001.
• 0%
• 5%
• 10%
• 15%
• 20%
• 25%
• 30%
• 35%
• 40%
• 45%
• 0 • 1 • 5 • 10 • 15 • 20 • 25 • 30 • 35 • 40 • 45 • 50 • 55 • 60 • 65 • 70 • 75 • 80 • 85
Age
Mo
rtal
ity
• Without Co-morbidity
• With Co-morbidity
• Overall
EPIDEMIOLOGI MORTALITAS DAN MORBIDITAS ETIOLOGI DEFINISI MANIFESTASI KLINIK PATOGENESIS DIAGNOSIS PENATALAKSANAAN
60-70% penyebab sepsis adalah gram negatif
Infeksi gram negatif merupakan hal yang predominan pada sekitar tahun 1960an dan 1970an,
akan tetapi infeksi gram positif telah meningkat dalam 2 dekade terakhir dan sekarang penyebab pada sebagian kasus sepsis berat
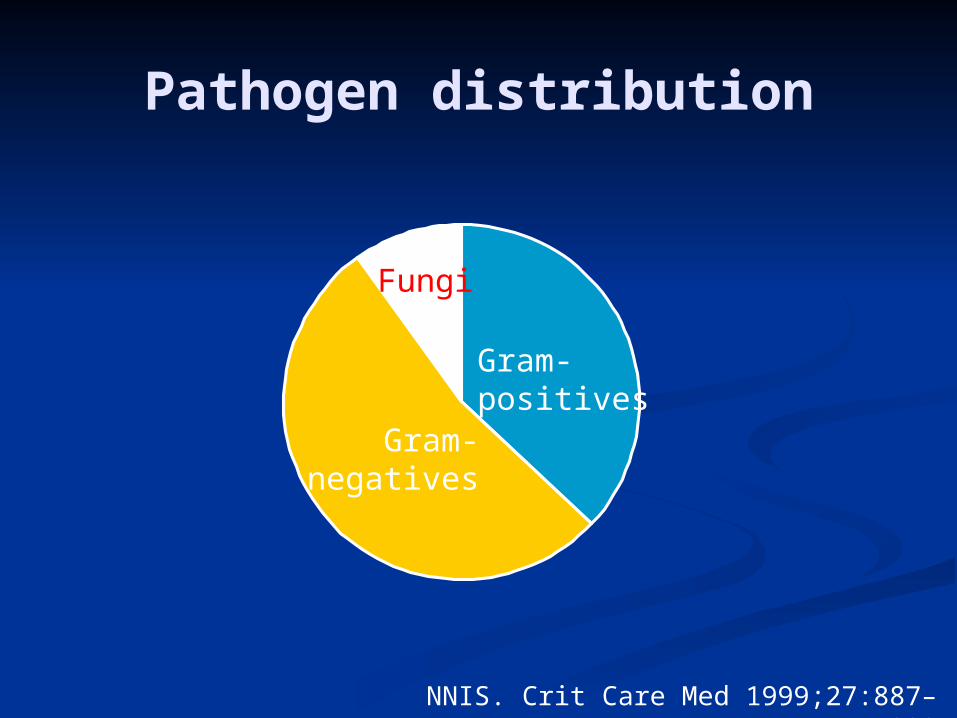
Pathogen distribution
Gram-positives
Gram-negatives
Fungi
NNIS. Crit Care Med 1999;27:887–892
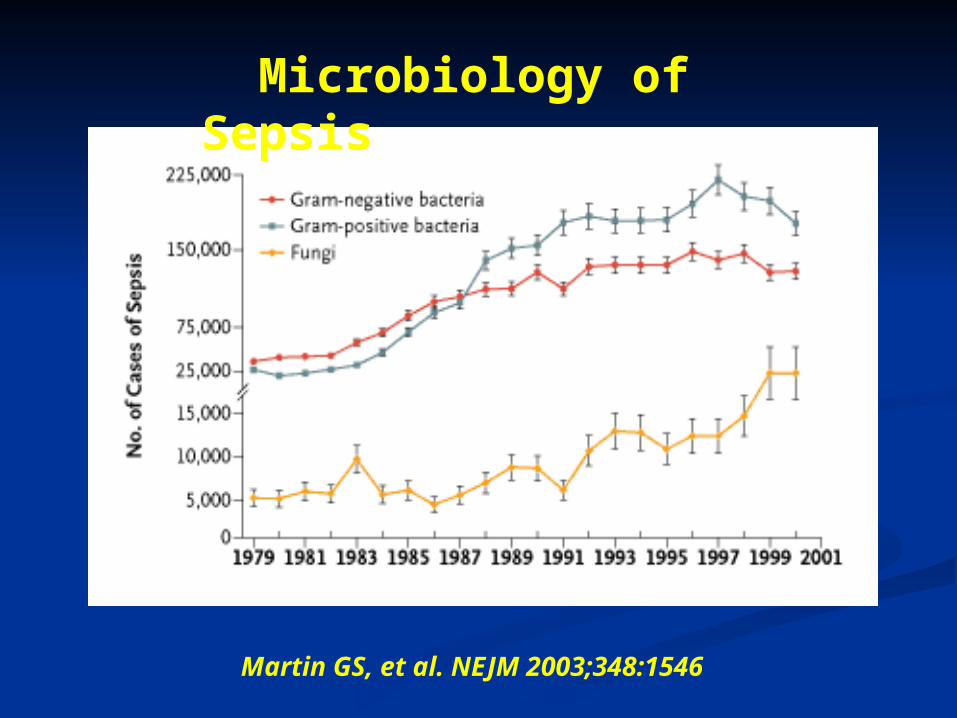
Microbiology of Sepsis
Martin GS, et al. NEJM 2003;348:1546
EPIDEMIOLOGI MORTALITAS DAN MORBIDITAS ETIOLOGI DEFINISI MANIFESTASI KLINIK PATOGENESIS DIAGNOSIS PENATALAKSANAAN
ACCP/ SCCM Consensus Conference 1992
Systemic Inflammatory Response Syndrome
( SIRS) Sepsis Severe Sepsis Septic shock
Bone RC, CHEST 1992: 101(6):1644-55
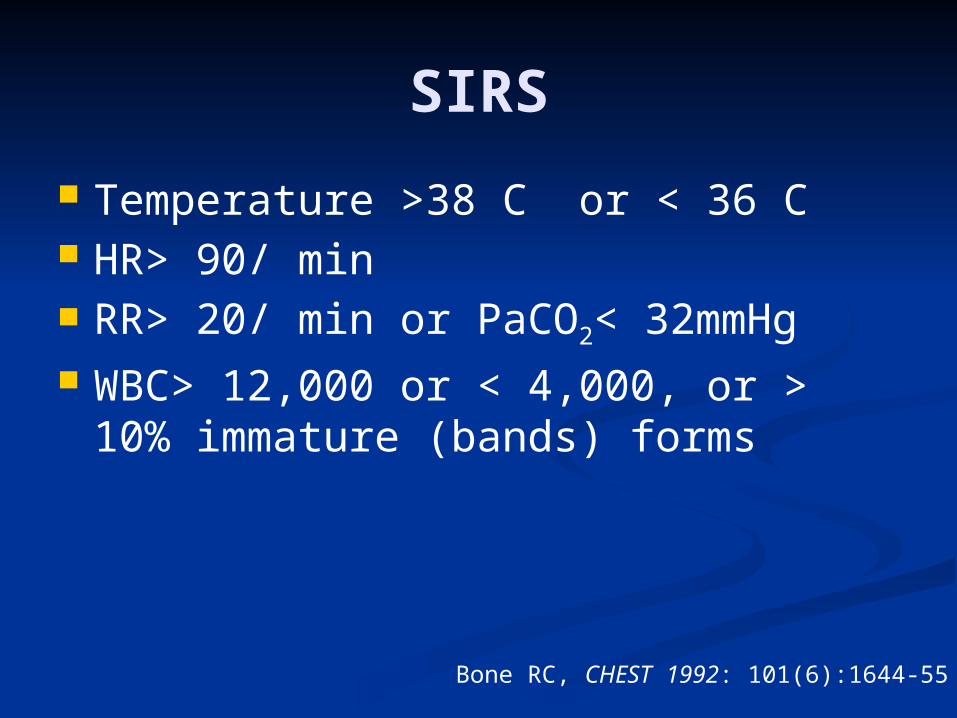
SIRS
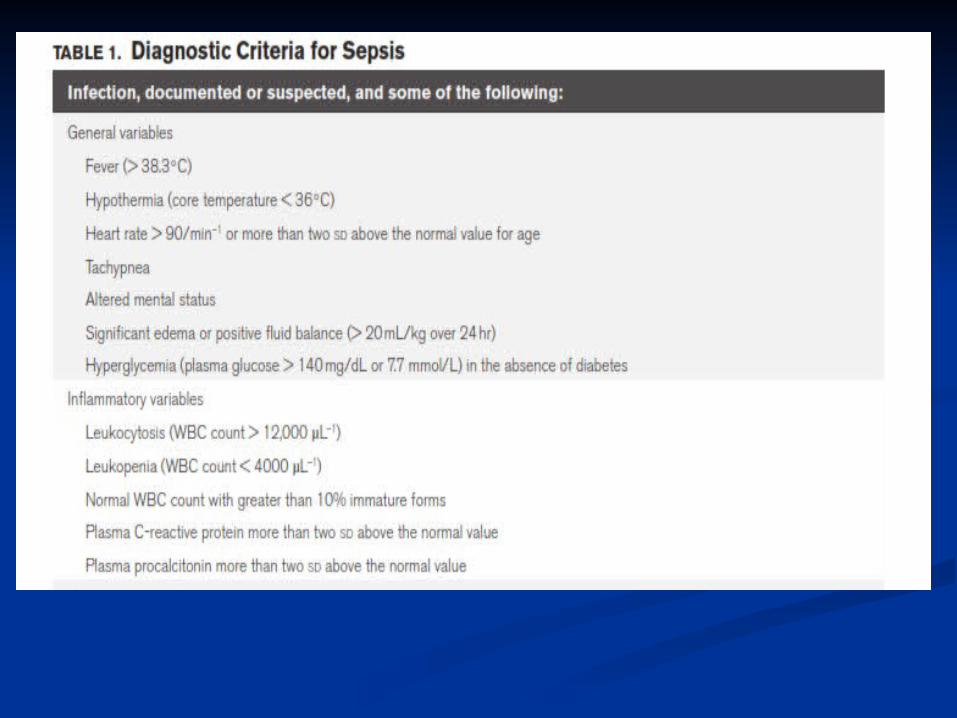
Temperature >38 C or < 36 C HR> 90/ min RR> 20/ min or PaCO2< 32mmHg WBC> 12,000 or < 4,000, or > 10%
immature (bands) forms
Bone RC, CHEST 1992: 101(6):1644-55
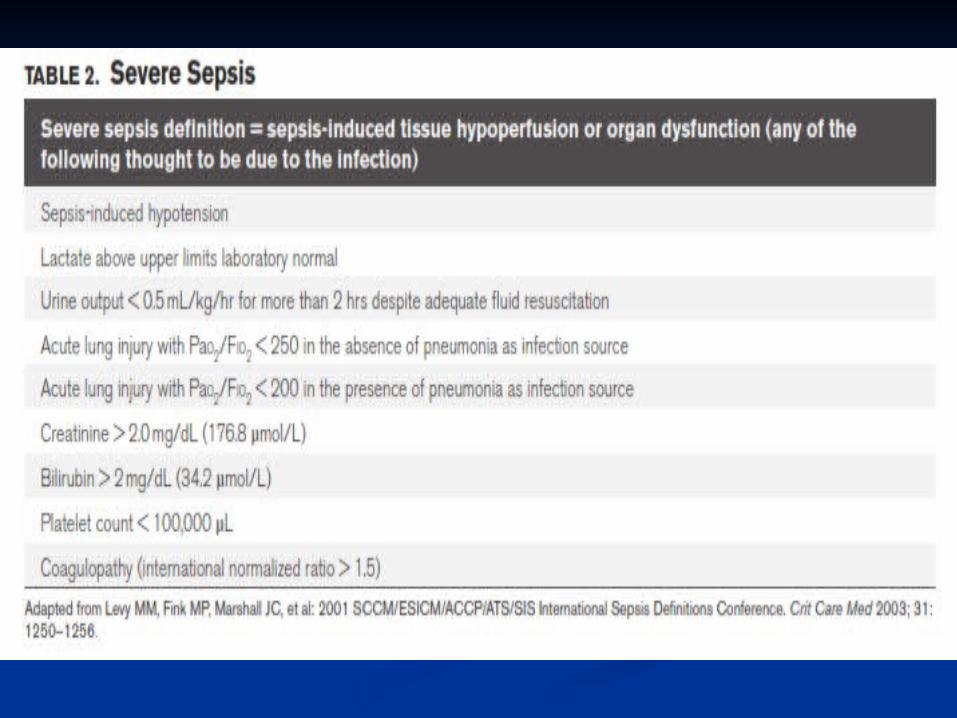
Definitions
Sepsis Systemic inflammatory response to known or suspected infection
Severe Sepsis SIRS associated with organ dysfunction (failure), hypoperfusion, and perfusion abnormalities
Bone, R et al. Chest 1992;101:1644
Definitions Continued
Septic shock A subset of severe sepsis, where patients experience combined decreased systemic vascular resistance and the presence of reduced myocardial performance
Bone, et al. CHEST , 1992;101:1644
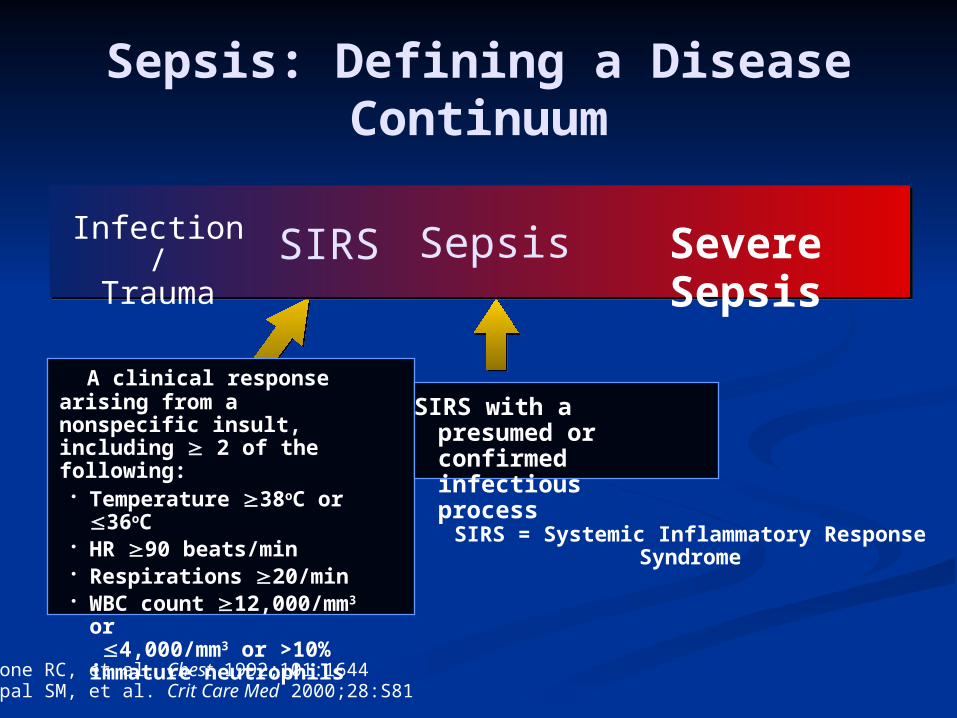
Sepsis: Defining a Disease Continuum
A clinical response arising from a nonspecific insult, including 2 of the following:
• Temperature 38oC or 36oC
• HR 90 beats/min• Respirations 20/min• WBC count
12,000/mm3 or 4,000/mm3 or >10% immature neutrophils
SIRS = Systemic Inflammatory Response Syndrome
SIRS with a presumed or confirmed infectious process
SepsisSIRSInfection/Trauma Severe Sepsis
Bone RC, et al. Chest 1992;101:1644Opal SM, et al. Crit Care Med 2000;28:S81
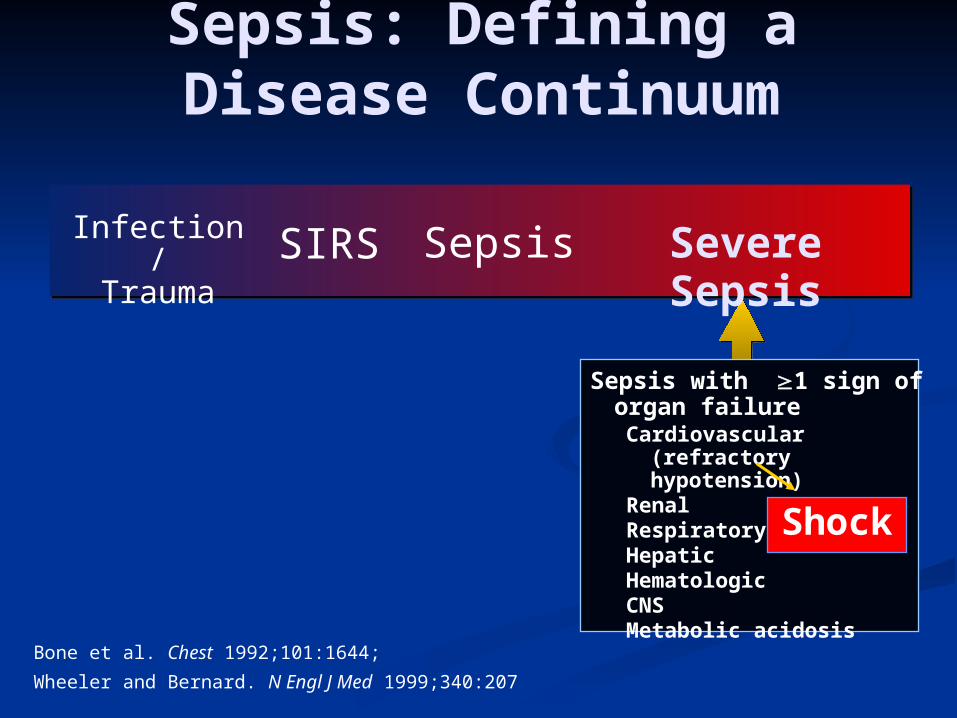
Sepsis: Defining a Disease Continuum
Bone et al. Chest 1992;101:1644;
Wheeler and Bernard. N Engl J Med 1999;340:207
SepsisSIRSInfection/Trauma Severe Sepsis
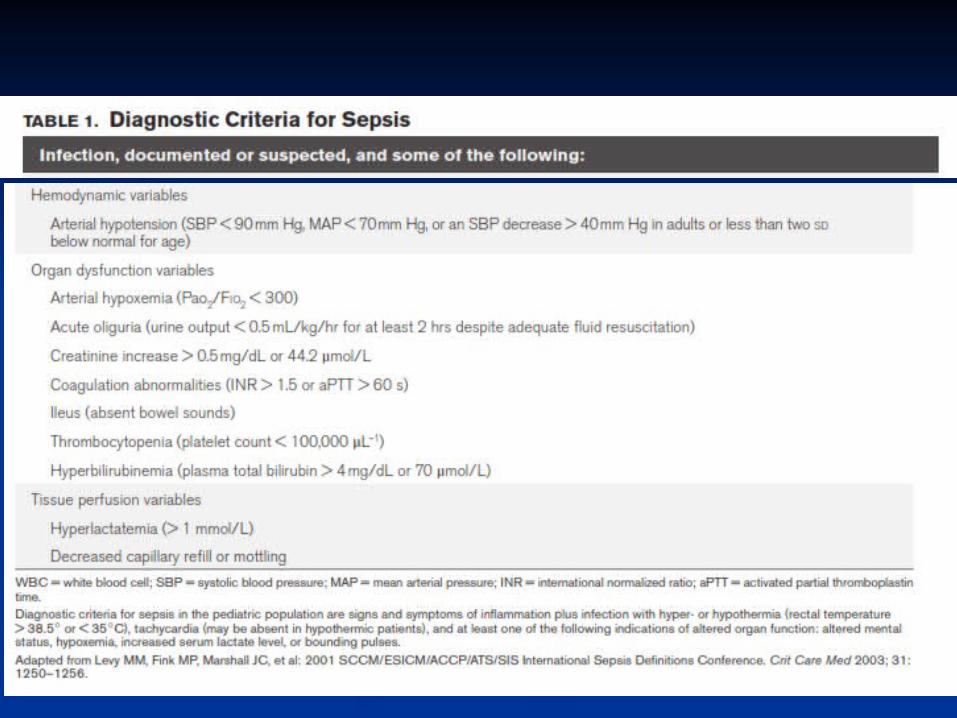
Sepsis with 1 sign of organ failure
Cardiovascular (refractory hypotension)
RenalRespiratoryHepaticHematologicCNSMetabolic acidosis
Shock
Bone et al. Chest 1992;101:1644
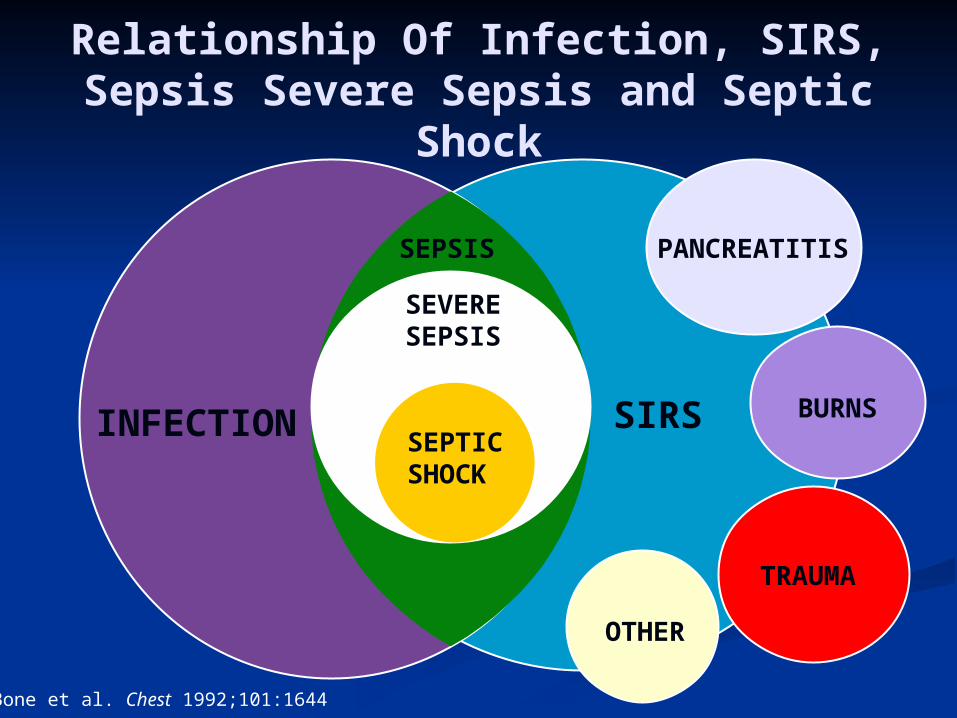
Relationship Of Infection, SIRS, Sepsis Severe Sepsis and Septic
Shock
SIRSINFECTION
PANCREATITIS
BURNS
TRAUMA
OTHER
SEPSIS
SEVERESEPSIS
SEPTICSHOCK
EPIDEMIOLOGI MORTALITAS DAN MORBIDITAS ETIOLOGI DEFINISI MANIFESTASI KLINIK PATOGENESIS DIAGNOSIS PENATALAKSANAAN
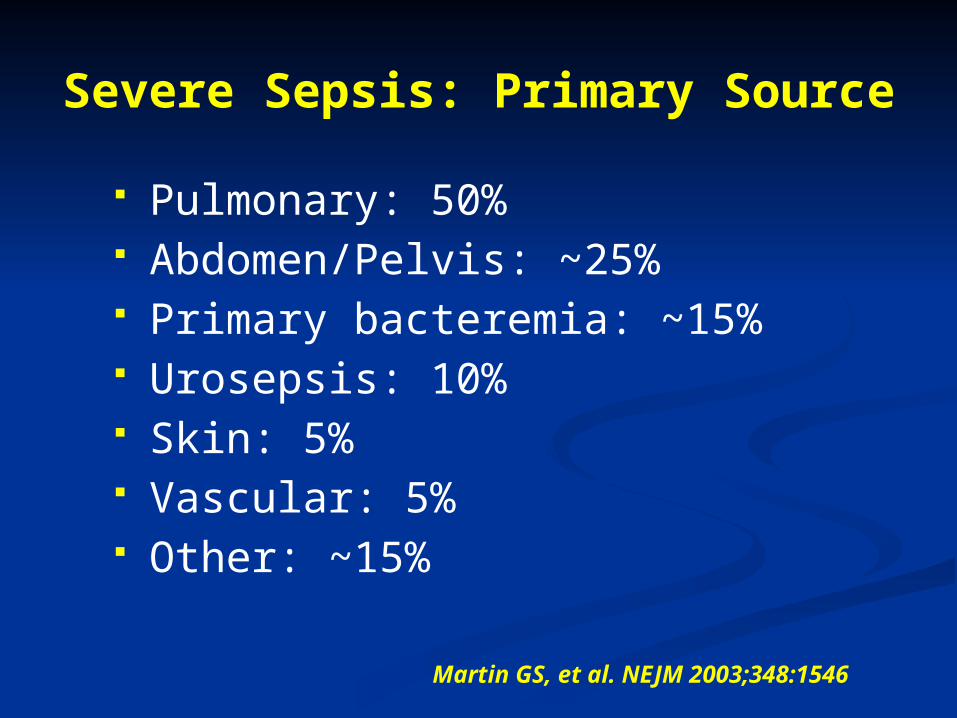
Severe Sepsis: Primary Source
Pulmonary: 50% Abdomen/Pelvis: ~25% Primary bacteremia: ~15% Urosepsis: 10% Skin: 5% Vascular: 5% Other: ~15%
Martin GS, et al. NEJM 2003;348:1546
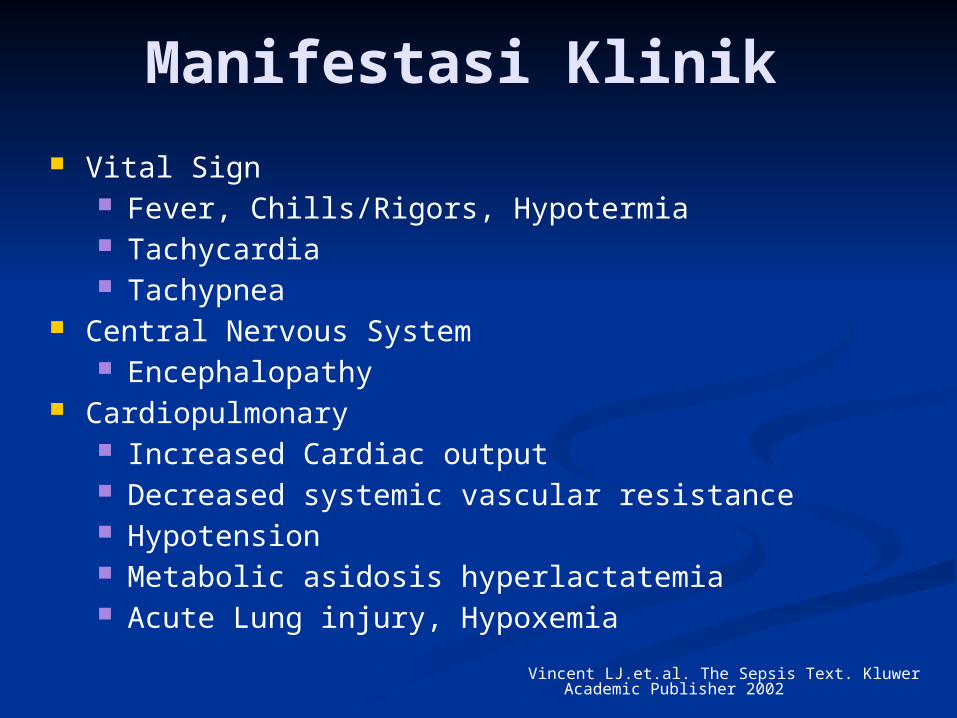
Manifestasi Klinik
Vital Sign Fever, Chills/Rigors, Hypotermia Tachycardia Tachypnea
Central Nervous System Encephalopathy
Cardiopulmonary Increased Cardiac output Decreased systemic vascular resistance Hypotension Metabolic asidosis hyperlactatemia Acute Lung injury, Hypoxemia
Vincent LJ.et.al. The Sepsis Text. Kluwer Academic Publisher 2002
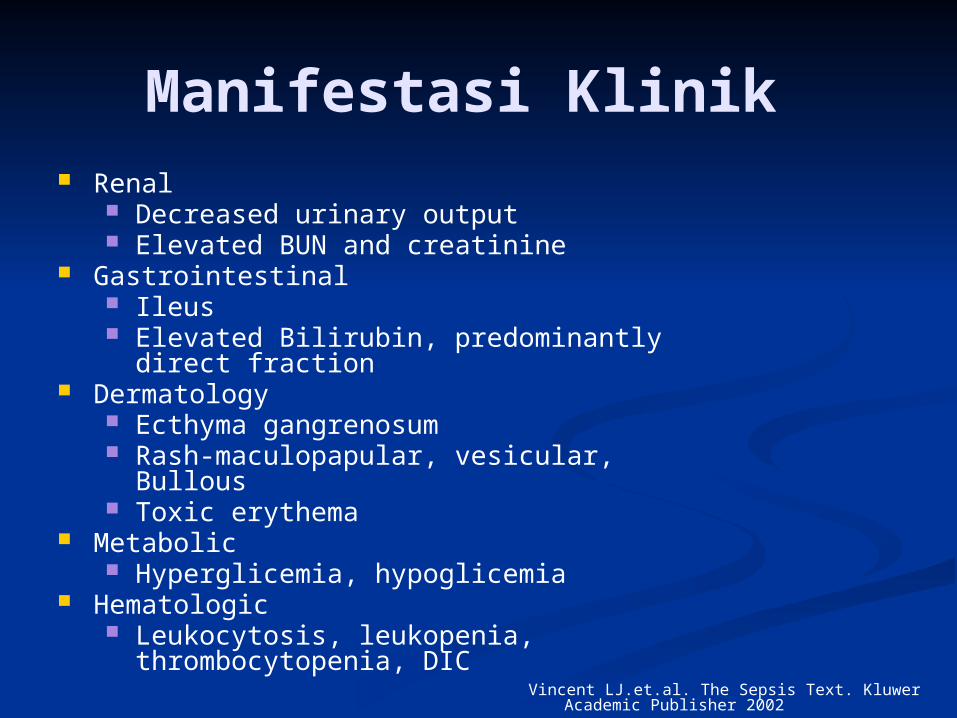
Manifestasi Klinik Renal
Decreased urinary output Elevated BUN and creatinine
Gastrointestinal Ileus Elevated Bilirubin, predominantly direct
fraction Dermatology
Ecthyma gangrenosum Rash-maculopapular, vesicular, Bullous Toxic erythema
Metabolic Hyperglicemia, hypoglicemia
Hematologic Leukocytosis, leukopenia,
thrombocytopenia, DIC
Vincent LJ.et.al. The Sepsis Text. Kluwer Academic Publisher 2002
EPIDEMIOLOGI MORTALITAS DAN MORBIDITAS ETIOLOGI DEFINISI MANIFESTASI KLINIK PATOGENESIS DIAGNOSIS PENATALAKSANAAN
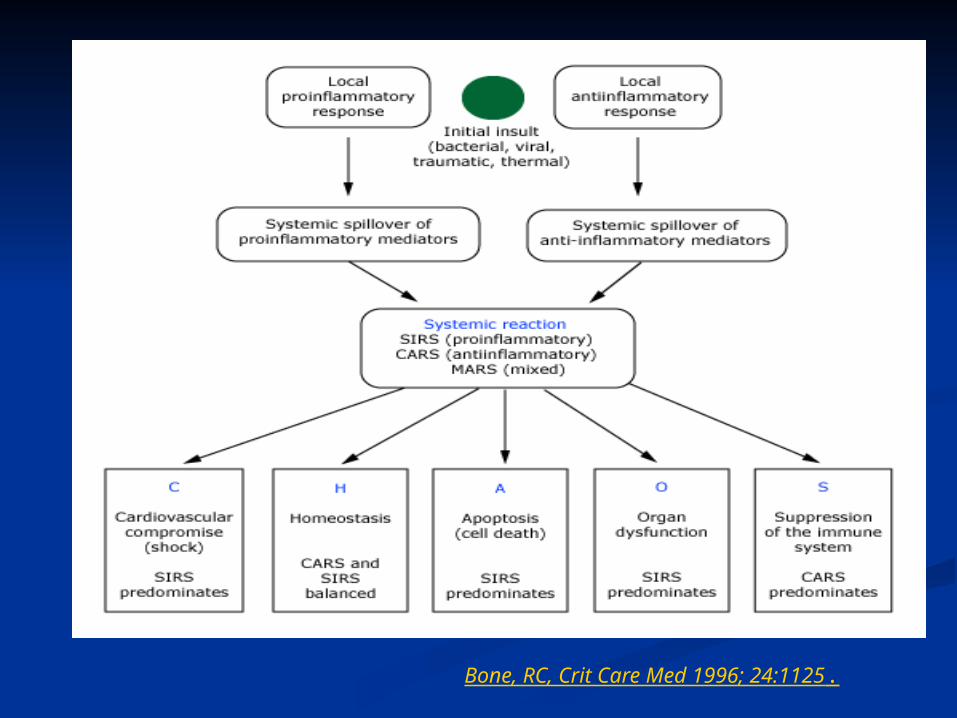
Bone, RC, Crit Care Med 1996; 24:1125.

Sepsis Battlefield: Cells and Mediators
Hotchkiss RS, Karl IE, NEJM 2003;348:138
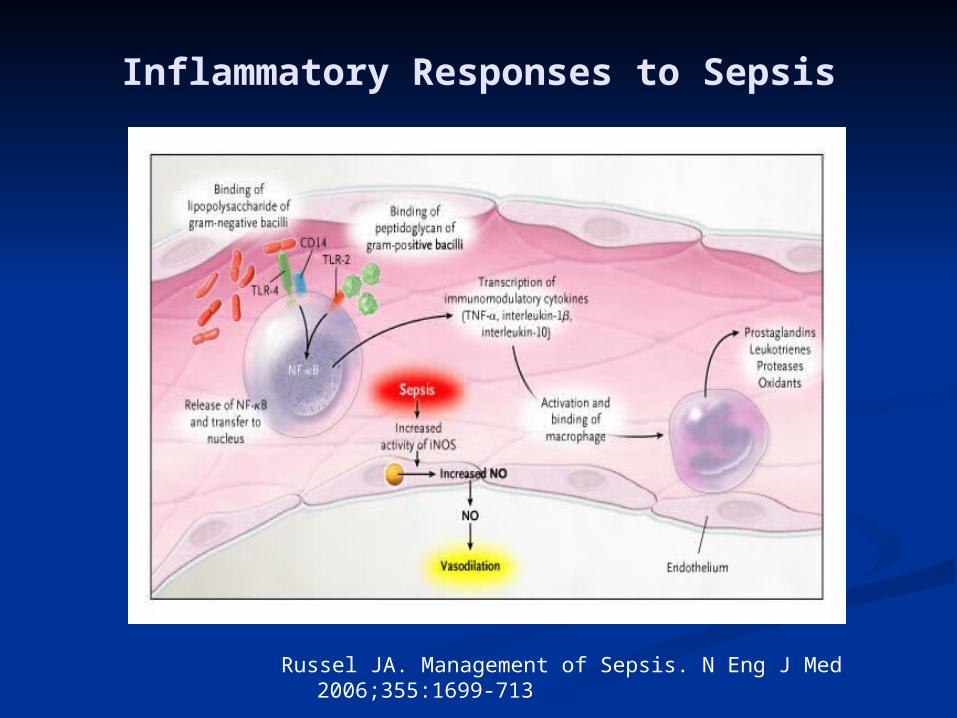
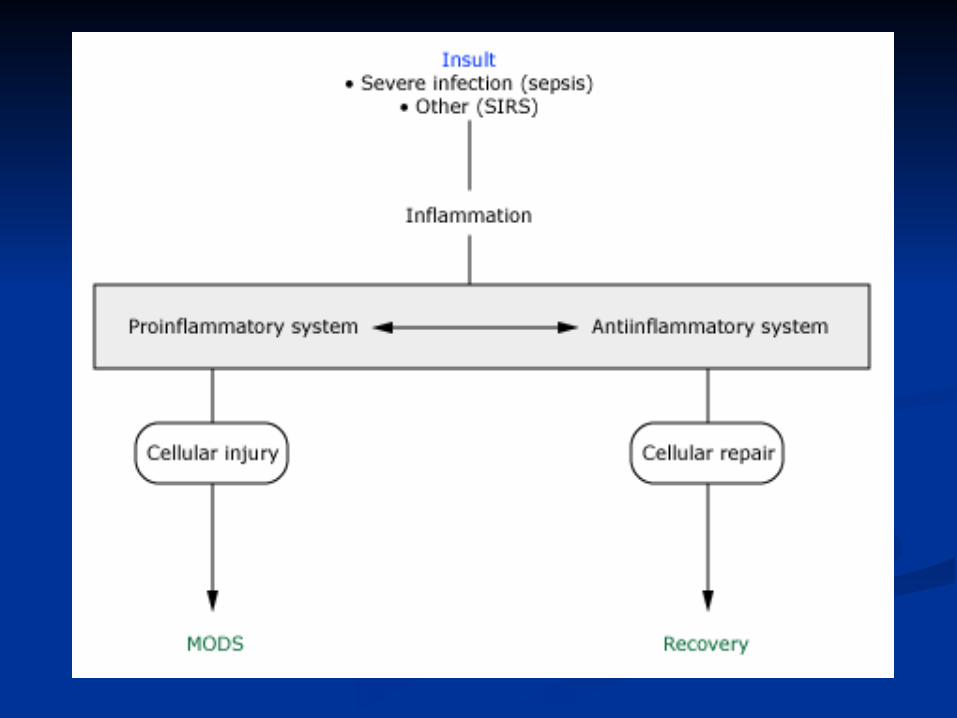
Inflammatory Responses to Sepsis
Russel JA. Management of Sepsis. N Eng J Med 2006;355:1699-713
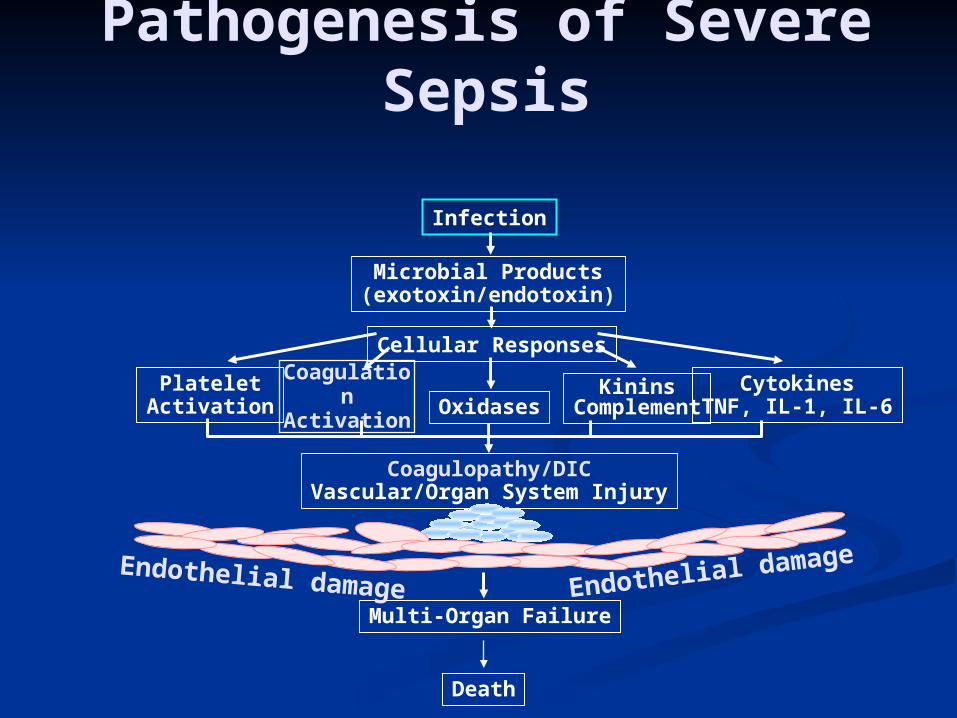
Pathogenesis of Severe Sepsis
Infection
Microbial Products(exotoxin/endotoxin)
Cellular Responses
OxidasesPlatelet
ActivationKinins
Complement
Coagulopathy/DICVascular/Organ System Injury
Multi-Organ Failure
Death
Endothelial damage Endothelial damage
CoagulationActivation
CytokinesTNF, IL-1, IL-6
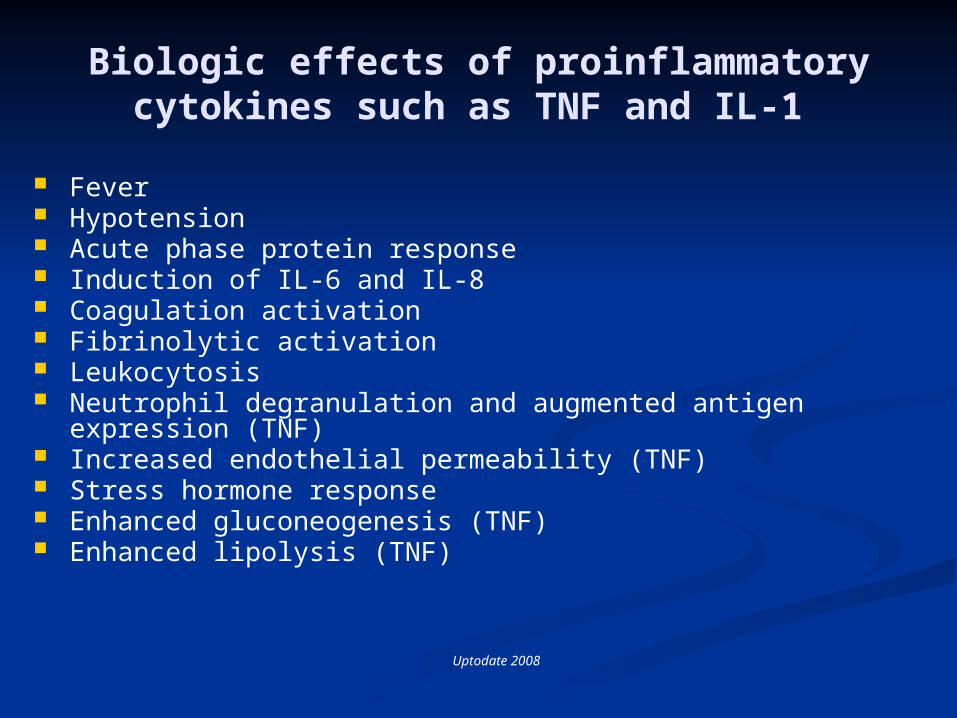
Biologic effects of proinflammatory cytokines such as TNF and IL-1
Fever Hypotension Acute phase protein response Induction of IL-6 and IL-8 Coagulation activation Fibrinolytic activation Leukocytosis Neutrophil degranulation and augmented antigen expression
(TNF) Increased endothelial permeability (TNF) Stress hormone response Enhanced gluconeogenesis (TNF) Enhanced lipolysis (TNF)
Uptodate 2008
EPIDEMIOLOGI MORTALITAS DAN MORBIDITAS ETIOLOGI DEFINISI MANIFESTASI KLINIK PATOGENESIS DIAGNOSIS PENATALAKSANAAN
Severe Sepsis:Initial Resuscitation (1st 6
hours) Should begin as soon as the
syndrome is recognized and should not be delayed pending ICU admission.
Elevated serum lactate concentration identifies tissue hypoperfusion in patients at risk who are not hypotensive.
Resuscitation Goals
Goals in the first 6 hours: CVP: 8-12 mm Hg MAP > 65 mm Hg Urine output > 0.5 ml/kg/hr Central venous (SVC) or mixed
venous oxygen (SvO2) saturation > 70%
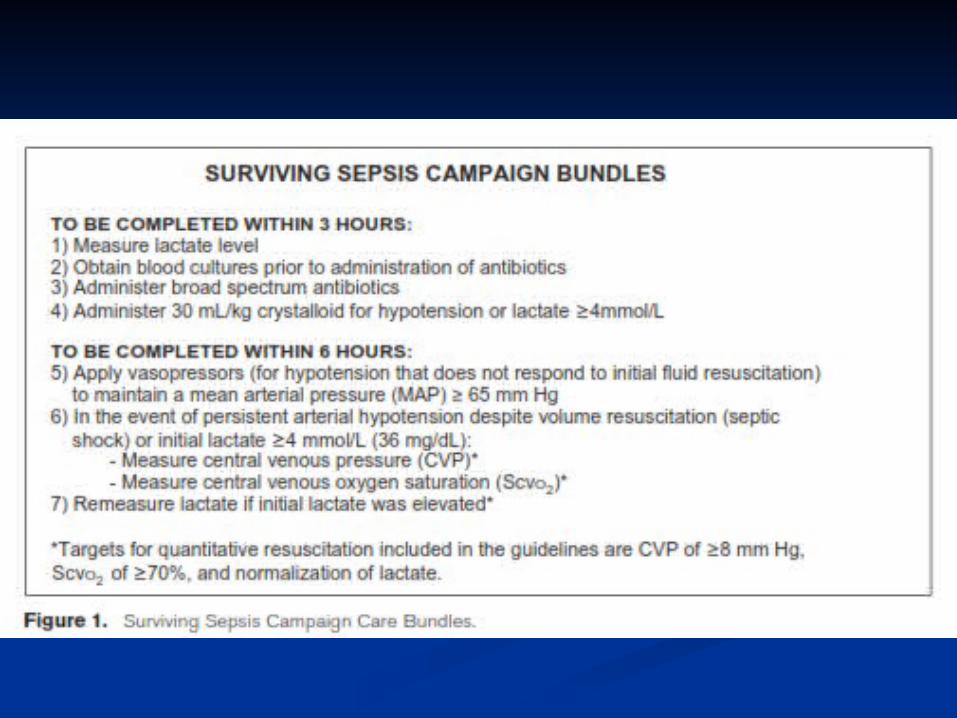
6 Hour Resuscitation Bundle
Early Identification Early Antibiotics
and Cultures Early Goal
Directed Therapy
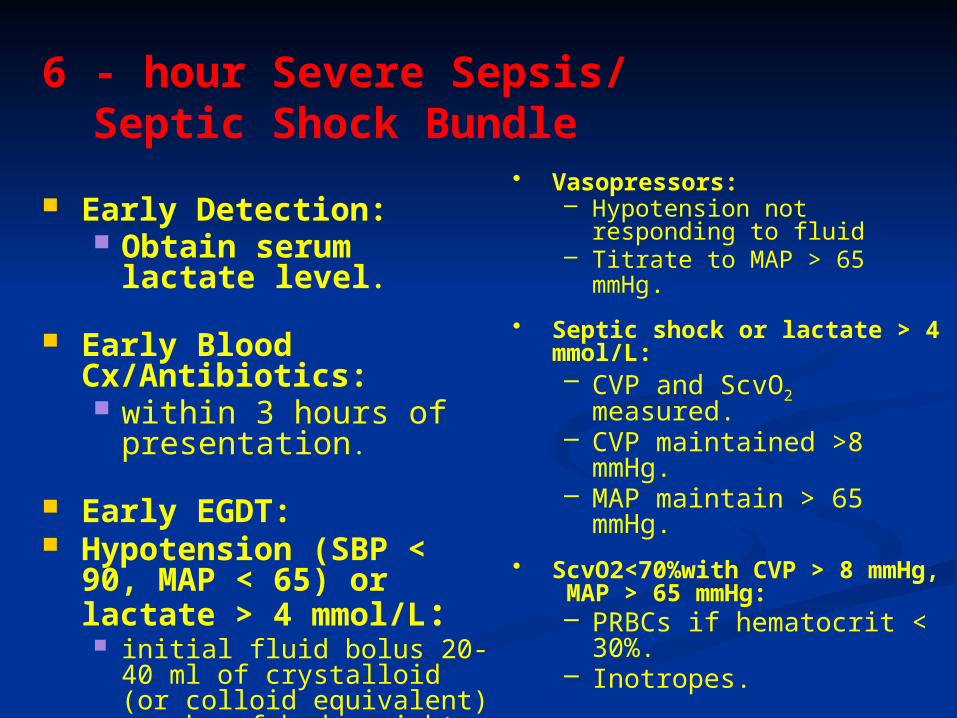
6 - hour Severe Sepsis/Septic Shock Bundle
Early Detection: Obtain serum lactate
level.
Early Blood Cx/Antibiotics: within 3 hours of
presentation.
Early EGDT: Hypotension (SBP <
90, MAP < 65) or lactate > 4 mmol/L: initial fluid bolus 20-40 ml
of crystalloid (or colloid equivalent) per kg of body weight.
• Vasopressors:– Hypotension not responding
to fluid– Titrate to MAP > 65 mmHg.
• Septic shock or lactate > 4 mmol/L:– CVP and ScvO2
measured.– CVP maintained >8
mmHg.– MAP maintain > 65
mmHg.
• ScvO2<70%with CVP > 8 mmHg, MAP > 65 mmHg:– PRBCs if hematocrit <
30%. – Inotropes.

Early Goal Directed Therapy
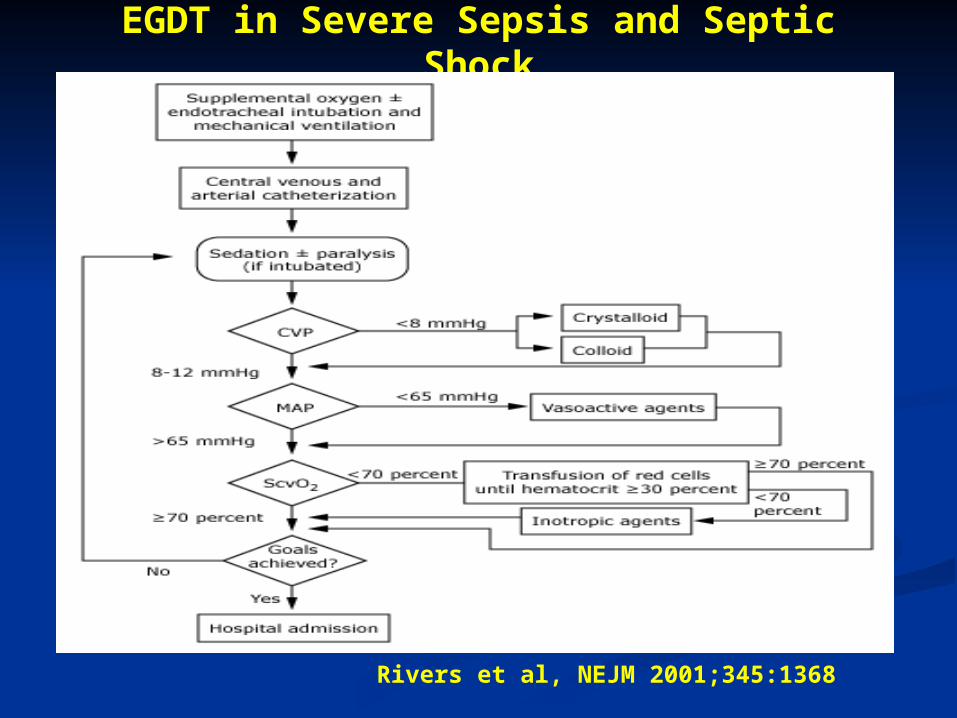
EGDT in Severe Sepsis and Septic Shock
Rivers et al, NEJM 2001;345:1368
Terima Kasih





























