Embed Size (px)
Citation preview
Makalah Oral Biologi
Disusun oleh :
NAMA :Rama Dia Dara
NIM :04101004015
Program Studi :Kedokteran gigi
Fakultas :Kedokteran
Dosen Pembimbing :drg.Shanty chairany
DINAS PENDIDIKAN NASIONAL
UNIVERSITAS SRIWIJAYA
An overview of orthodontic material degradation in oral cavity
TP Chaturvedi1, SN Upadhayay2
1 Department of Orthodontics, Faculty of Dental Sciences, Institute of Medical Sciences, Varanasi, UP, India2 Department of Chemical Engineering, IT, Banaras Hindu University, Varanasi, UP, India
Click here for correspondence address and email
Date of Submission 27-Apr-2009
Date of Decision 07-Nov-2009
Date of Acceptance 06-Feb-2010
Date of Web Publication 22-Jul-2010
Abstract
Various types of metallic orthodontic appliances are used in the management of malocclusion. These appliances are placed in oral environnent under many stresses and variations such as masticatory forces, appliance loading, temperature fluctuations, varieties of ingested food and saliva. These metals undergo electrochemical reactions with the oral environment resulting in dissolution or formation of chemical compounds. Various microorganisms and many aggressive ions containing oral environment can cause material degradation (corrosion) and its associated problems during long time exposure. Orthodontic alloys must have excellent corrosion resistance to the oral environment, which is highly important for biocompatibility as well as for orthodontic appliance durability. This article reviews various aspects of corrosion (surface degradation) of orthodontic alloys. It explores the emerging research strategies for probing the biocompatibility of materials. During orthodontic treatment, use of nickel free, better corrosion resistance alloys and less use of fluoride containing toothpaste or gel is expected.
Keywords: Biocompatibility, corrosion, dental alloys, material degradation, nickel allergy, orthodontic alloys, orthodontic wires, surface degradation
How to cite this article:Chaturvedi TP, Upadhayay SN. An overview of orthodontic material degradation in oral cavity. Indian J Dent Res 2010;21:275-84
How to cite this URL:Chaturvedi TP, Upadhayay SN. An overview of orthodontic material degradation in oral cavity. Indian J
Dent Res [serial online] 2010 [cited 2011 Nov 3];21:275-84. Available from: http://www.ijdr.in/text.asp?2010/21/2/275/66648
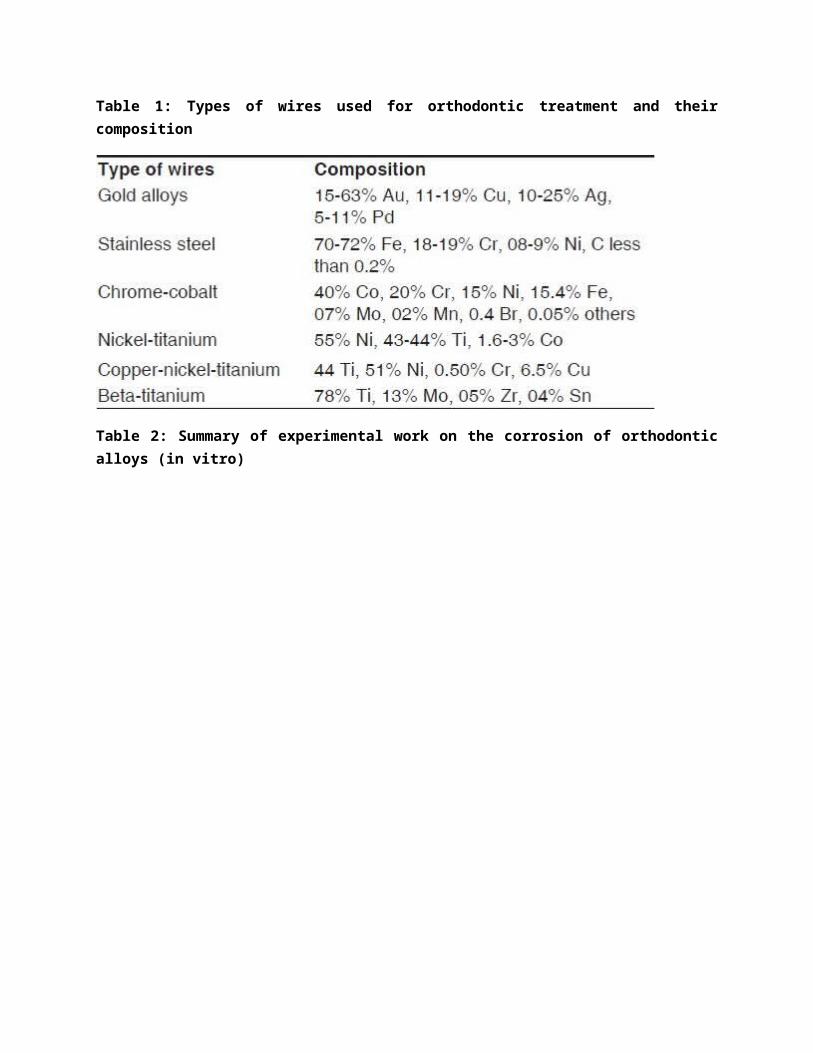
Biocompatibility of dental material is now a fundamental requirement of successful clinical behavior in oral cavity. It draws on knowledge from biology, patient risk factors, clinical experience and engineering. There are two key factors that appear to be important in determining biocompatibility of any dental material - some involve various types of corrosion or material degradation and others include surface characteristics. Dental materials within the mouth interact continually with physiological fluids. Saliva is a hypotonic solution containing bioactonate, chloride, potassium, sodium, nitrogenous compounds and proteins. [1] Corrosion, the graded degradation of materials by electrochemical attack, is of concern particularly when orthodontic appliances are placed in the hostile electrolytic environment provided by the human mouth. [2],[3] Various types of wires and brackets are used in the treatment of malocclusion e.g. stainless steel, cobalt-chromium-nickel alloys, nickel-titanium alloys, β-titanium alloys, etc [Table 1]. A ductile wire can be formed into various shapes. As a manufacturing process, the industry uses brazing alloys to join the base and wing components of brackets. Silver based brazing alloys form a galvanic couple that can lead to ionic release mainly copper and zinc. Solder joints of removable appliances and face bows, and brazed joints of some stainless steel brackets may affect the mechanical properties. [4]
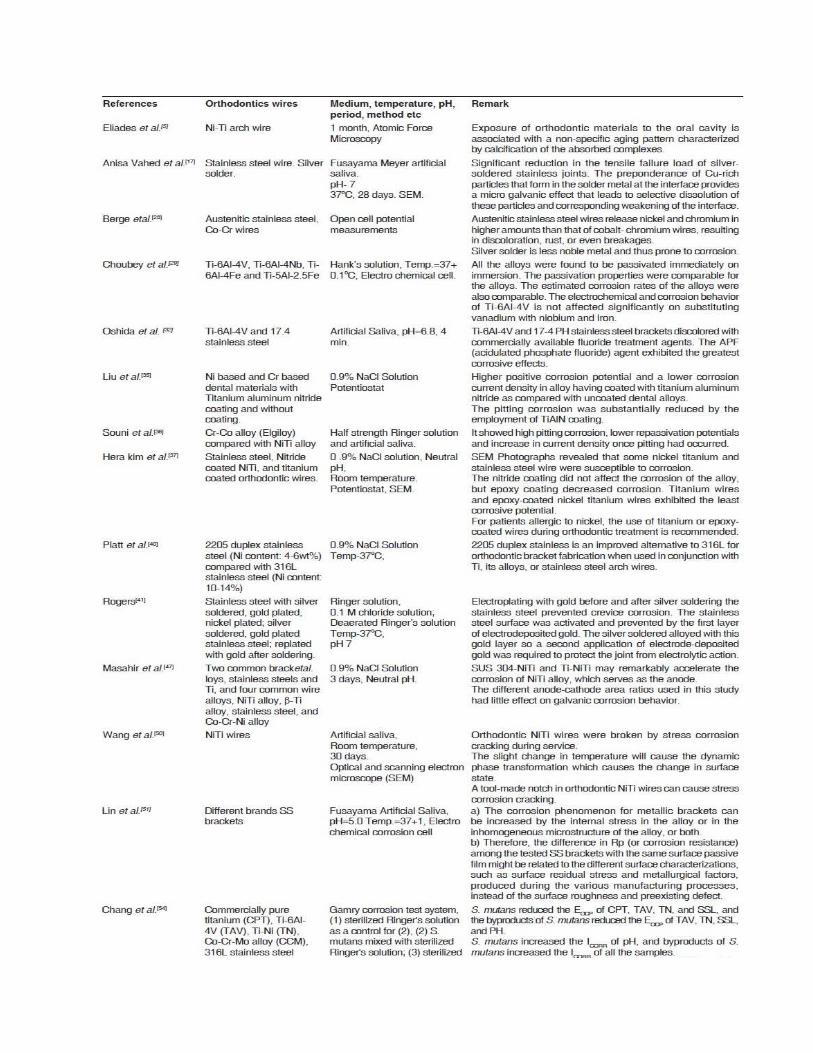
The objective of the present article is to review briefly the corrosion aspects (material degradation) and its effect on orthodontic wires and brackets in oral environment, effect of fluoride gel/toothpaste on orthodontic appliances and nickel sensitivity. A Summary of the few experimental works on the corrosion of orthodontic alloys (in vitro) are given in [Table 2], which can explore the future research strategies for properties of orthodontic materials.
Table 1: Types of wires used for orthodontic treatment and their composition

Table 2: Summary of experimental work on the corrosion of orthodontic alloys (in vitro)

Weakening of Appliances
Stainless steel becomes susceptible to intergranular corrosion, which may ultimately weaken the alloy. Tensile strength of the orthodontic silver-soldered stainless steel joints will be affected by corrosion process. [12],[13] Despite the good corrosion resistance of stressed NiTi, breakage of orthodontic wires has frequently been found in clinical studies and subjected to degradation caused by corrosion in the oral environment. [14],[15] According to Zinelis et al.[16] Ag-based soldering alloys introduce a galvanic couple with stainless steel alloys, inducing release of metallic ions like Cu ++ and Zn ++ , the elements mostly leached out from silver solder alloys. Vahed A et al.[17] report that prolonged exposure in stimulated saliva leads to significant reduction in the tensile failure load of silver-soldered stainless joints. The reduction in tensile properties is brought about by a weakness induced by localized corrosion of the solder metal at the solder/wire interface. The preponderance of Cu-rich particles that forms in the solder metal at the interface provides a micro galvanic effect that leads to selective dissolution of these particles and corresponding weakening of the interface. Corrosion is the main cause of the progressive dissolution of brazing filler metal, leading to detachment of the wing from the bracket base during orthodontic therapy or at debonding stage. [18]
Sliding friction
Friction is a phenomenon that generally affects the clinical efficacy of orthodontic appliances. The frictional forces that oppose the tooth movement during sliding are effects of different arch wire bracket combinations (e.g. material, size, shape and angulations), influence of ligation e.g. material and contact force and interaction of appliances with surrounding environment e.g. (interbracket distances and oral fluids). Corrosion increases orthodontic friction force between the arch wire/bracket interfaces due to an increase in the surface roughness. [17],[18],[19]
Local pain/swelling
Corrosion products have been implicated in causing local pain or swelling in the region of the orthodontic appliances in the absence of infection, which can lead to secondary infection. [20],[21]
Cytotoxic responses
Iron, nickel and chromium are major corrosive products of stainless steel. Nickel and chromium induce Type-IV hypersensitivity reaction in the body. [22] These metals cause several cytotoxic responses including decrease in some enzyme activities, interference with biochemical pathways, carcinogenicity, and mutagenicity. [23],[24] Titanium wires containing nickel may cause localized tissue irritation in some patients. Manganese from the alloy is also consumed with saliva which produces toxicity leading to nervous, skeletal disorders, etc. It has been suggested that long term exposure to nickel containing dental materials affect both human monocytes and oral mucosal cells. [25],[26]
Decalcification of teeth
Various acids are formed during the microbial attack on metallic orthodontic appliances in oral environment. Biofilm for med on the tooth surface with the help of food debris and metabolic products of microbes. Acids cause reduction of pH and influence the decalcification of teeth and corrosion of metallic appliances. [27]
Effect of Corrosion On Orthodontic Wires
Corrosion of stainless steel
Orthodontic stainless steel wires are generally made of austenitic stainless steel containing approximately 18% chromium and 8% nickel. In general, these wires have good biocompatibility and high corrosion resistance in oral environment. It owes its corrosion resistance property to chromium, a highly reactive base metal. The corrosion resistance of alloy depends on the passive film, which spontaneously forms (passivation) and reforms (repassivation) in air and under most wet conditions. Oxygen is necessary to form and maintain the film, whereas acidity and chloride ions can be particularly detrimental to it. [28] The presence of soldered joints increase corrosion susceptibility since they have a tendency to emit electrogalvanic currents with saliva and consequently release metal ions. Austenitic stainless steel may lose its resistance to corrosion if it is heated between approximately 400 o C and 900 o C. Such temperatures are within the range used by the orthodontist for soldering and welding. The decrease in corrosion resistance is caused by the precipitation of chromium-iron carbide at the grain boundaries at these high temperatures. [29] Precipitation does not occur below these temperatures and chances of corrosion are less. Corrosion of stainless steel may result due to galvanic cell forming in one or more of the following ways:
Surface roughness of stainless steel of wires may cause localized corrosion attack. Any cut or abrasion of stainless steel by carbon steel pliers/carbon steel bur may act as galvanic
cell, and Brazed or soldered joints in orthodontic appliances can also form galvanic couples in vivo.
Titanium and its Alloys (nickel-titanium alloys, β-titanium alloys, titanium- aluminum-vanadium alloy)
Titanium is highly corrosion resistant as a result of the passivating effect afforded by a thin layer of titanium oxide that is formed on its surface. When the stable oxide layer is broken down or removed and is unable to reform on parts of the surface, titanium and its alloy can be as corrosive as many other base metals. The surface roughness of titanium containing alloy is more as compared to stainless steel wires, which may act as galvanic cell in the mouth. [30],[31],[32]

Types of Corrosion in Orthodontic Wires
The features that determine how and why dental materials corrode are oxidation and reduction reactions as well as passivation or the formation of a metal oxide passive film on a metal surface. [33]
Various forms of corrosion are shown in [Figure 1] and described as follows.
Uniform corrosion
A uniform corrosion is any chemical or electrochemical reaction that proceeds uniformly over the entire exposed surface or over a large area. It is the most common type of corrosion, occurring with all metals at different rates. The process arises from the interaction of metals with the environment and the subsequent formation of hydroxides or organometallic compounds. For uniform corrosion, the corrosive environment must have the same access to all parts of the surface, and metal itself must be metallurgically and compositionally uniform. Uniform attack may not be detectable before large amounts of metal are dissolved.
Pitting corrosion
Pitting is a form of extreme attack that results in holes on metal surface. It usually occurs on base metals, which are protected by a naturally forming thin film of an oxide. It has been identified in brackets and wires. In the presence of chloride in the environment, the film locally breaks down and rapid dissolution of the underlying metal occurs in the form of pits. Surfaces of stainless steel and NiTi wire may exhibit crevices and pores which may give rise to attack since they represent sites susceptible to corrosion. Potentiodynamic polarization experiments and scanning electron microscopic observations of archwires composed of stainless steel, CoCr, NiCr, NiTi and Beta-Ti exposed to electrochemical corrosion in artificial saliva have shown evidence of pitting corrosion formed on the wire surfaces. [34] Liu [35] studied mechanical characteristics and corrosion behavior of titanium aluminum nitride coating on dental alloys, especially in nickel- and chromium-based dental materials. They tested corrosion behaviors in 0.9% NaCl solution and observed a higher positive corrosion potential and a lower corrosion current density in alloys having coated with titanium aluminum nitride as compared with uncoated dental alloys. In addition, the pitting corrosion was substantially reduced by the employment of TiAlN coating. Es Souni et al.[36] found that Cr-Co alloy (Elgiloy) showed high pitting corrosion compared with NiTi alloy, lower repassivation potentials and increase in current density once pitting had occurred. Kim et al.[37] showed that nickel titanium and stainless steel wires were susceptible to pitting and localized corrosion.
Crevice corrosion
Crevice corrosion occurs between two close surfaces or in constricted places where oxygen exchange is
not available. It often occurs through the application of nonmetallic parts of metal (i.e., elastomeric ligatures on a bracket). The reduction in pH and increase in the concentration of chloride ions are two essential factors in the initiation and propagation of the crevice corrosion phenomenon. When the acidity of the medium increases with time the passive layer of the alloy dissolves and it accelerates local corrosion process. Crevice corrosion of stainless steels in aerated salt solutions is widely known. Corrosion products of Fe, Cr, and Ni, the main components of stainless steel, accumulate in the crevice and form highly acidic chloride solutions in which corrosion rates are very high. [38],[39] Platt et al.[40] report that 2205 duplex stainless steel is an improved alternative to 316L for orthodontic bracket fabrication when used in conjunction with Ti, its alloys, or stainless steel arch wires. Rogers [41] showed that by electroplating with gold before and after silver soldering, the stainless steel prevented crevice corrosion. Recycling orthodontic wires and brackets was once common in many countries, but it is not recommended in many countries now. Recycling can comprise heat chemical and mechanical process which could lead to accelerated crevice corrosion of brazed joints.
Fretting and erosion-corrosion
Erosion-corrosion is increase in rate of deterioration or attack on material because of relative movement between corrosive fluid and material surface. The stagnant or slow-flowing fluids will cause a low or modest corrosion rate, but rapid movement of the corrosive fluid physically erodes and removes the protective corrosion product film, exposes the reactive alloy beneath and accelerates corrosion. Fretting corrosion (type of erosion-corrosion) is responsible for most of the metal released into tissues. [42],[43]
Conjoint action of chemical and mechanical attack results in fretting corrosion. It occurs in contact areas of materials under load and finds its analogue in the slot-arch wire interface of the bracket.
Intergranular corrosion
Due to more reactive nature of grain boundaries, intergranular corrosion occurs adjacent to grain boundaries with little corrosion of grains. Stainless steel brackets subjected to a range of temperatures, known as sensitization temperatures, undergo an alteration in their microstructure. The phenomenon is due to a precipitation of carbide at the boundaries of the grains. [44] Berge et al.[28] reported that austenitic stainless steel wires release nickel and chromium in higher amounts than cobalt- chromium wires, resulting in discoloration, rust, or even breakages.
Galvanic corrosion
This type of corrosion occurs due to galvanic coupling of dissimilar metals involved in which less corrosion resistant metals become an anode and usually corrode. In a clinical situation, two dissimilar alloys having different corrosion potentials are often placed in contact such as in orthodontic brackets and arch wires. This can cause galvanic corrosion that leads to preferential release of metal ions from the anodic metal or alloy. Surface area ratio of the two dissimilar alloys is a very important factor because it affects the galvanic corrosion behavior. An unfavorable area ratio, which consists of a large cathode and a small anode, might lead to greater corrosion rate from the anodic alloy. Reed and

Willman [45] demonstrated the presence of galvanic currents in the oral cavity probably first time in detail. Approximate values for magnitude were established. Burse [46] described an experimental protocol for in vivo tarnish evaluation and showed the importance of proper elemental ratio in gold alloys. Masahir et al.[47] showed the NiTi alloy coupled with SUS 304 or Ti exhibited a relatively large galvanic current density even after 72 hours. It is suggested that coupling SUS 304-NiTi and Ti-NiTi may remarkably accelerate the corrosion of NiTi alloy, which serves as the anode. The different anode-cathode area ratios used in this study had little effect on galvanic corrosion behavior. Tufekci et al.[48] described highly sensitive analytical technique which showed the release of individual elements over a month period which appeared to be correlated with micro structural phases in the alloys. Several forms of electrochemical corrosion are based on the mechanism that produces inhomogeneous areas. Failures could be minimized in orthodontic solder joints by employing material couples that minimize galvanic and micro galvanic effects.
Stress corrosion
Stress corrosion cracking refers to cracking caused by the simultaneous presence of tensile stress in corrosive medium. This process can dangerously impair mechanical integrity of orthodontic wires. When arch wire engaged to brackets are bonded to crowded teeth, the reactivity status of the alloy increases. The increased reactivity results from the generation of tensile and compressive stresses developed locally because of the multiaxial, three dimensional loading of wire. Thus, an electrochemical potential difference occurs with specific sites acting as anodes and other surfaces acting as cathodes. NiTi orthodontic wires remain in the oral environment for several months and suffer a large number of small loads during mastication. Despite good corrosion resistance of stressed NiTi, the breakage of NiTi orthodontic wires has frequently been found in clinical studies. [49],[50] Wang et al.[51] studied stress corrosion cracking of NiTi in artificial saliva and demonstrated that the orthodontic NiTi wires were broken by stress corrosion cracking during service. The slight change in temperature causes the dynamic phase transformation, which causes the change in surface state.
Hydrogen damage
Under certain circumstances, orthodontic wires can absorb hydrogen under cathodic condition. The presence of absorbed hydrogen decreases ductility of metals. It can embrittle reactive metals such as titanium, vanadium, niobium etc. [1],[6]
Effect of Oral Environment
In the oral environment, fluoride-containing commercial mouthwashes, toothpastes and prophylactic gels are widely used to prevent dental caries or relieve dental sensitivity or for proper oral cleaning after application of normal brushes with tooth paste. [52],[53] The detrimental effect of fluoride ions on the corrosion resistance of Ti or Ti alloys has been extensively reported. Fluoride ions are very aggressive on

the protective TiO 2 film formed on Ti and Ti alloys. Since outermost surface of NiTi arch wire contains mainly TiO 2 film with trace amount of NiO, fluoride enhanced corrosion of the NiTi arch wires in fluoride containing environment has been considered. [54],[55] Fluoride-containing environments can penetrate into the narrow crevices between the orthodontic arch wire and bracket in the mouth which is not cleaned out thoroughly. Topical high fluoride concentrations will stay in place and attack the arch wire/bracket interface depending on the fluoride concentration. This may increase friction force between arch wire and bracket. Using topical fluoride agents with NiTi wire could decrease the functional unloading mechanical properties of wires and contribute to prolonged orthodontic treatment. [56],[57] Orthodontic patients are required to maintain a high level of oral hygiene, which include regular tooth brushing. In vitro studies [58],[59] on effects of tooth brushing showed significant increase in elemental release from nickel alloys when toothpaste was used, however, without toothpaste there is no significant increase in elemental release. There is also evidence to suggest that some mouth rinses may also increase ionic release from silver soldered joints in orthodontic appliances. Schiff et al.[60] studied corrosion resistance of three types of brackets (cobalt-chromium, iron chromium-nickel and titanium based brackets) in three fluoride mouthwashes. The results showed that the bracket materials could be divided into two groups: Ti and FeCrNi in one and CoCr, which has properties close to those of Pt. Many studies have shown that fluoride ions can destroy the protectiveness of the surface TiO 2
passive film on Ti or Ti alloy, leading to attacked corrosion morphology, decreased polarization resistance and an increased anodic current density or metal ion release. [61]
Further, the corrosion resistance of NiTi decreases on increasing NaF concentration in the artificial saliva. Schiff et al.[62] studied the corrosion resistance of orthodontic wires in three different commercial mouthwashes and found that the NiTi wires were subject to severe corrosion in Na 2 FPO 4
containing mouthwashes. Huang [63] studied surface topography variations of different nickel-titanium orthodontic arch wires in different commercial fluoride containing environments. Four tested NiTi arch wires had different surface topography variations, depending on the fluoride ion concentration. The arch wire manufacturer and emersion environment had a statistically significant influence on surface roughness variation. The increase in surface roughness of NiTi orthodontic arch wires in the commercial fluoride containing environments should be taken into account when considering the effectiveness of orthodontic appliances.
Nickel Containing Orthodontic Wires
Nickel containing alloys find extensive application in orthodontics, including metallic brackets, arch wires, bands, springs and ligature wires. For most materials, a rough surface promotes corrosion. Doubts remain about biocompatibility of Ni-based alloys when used in dentistry. The use of nickel is of particular concern since it is the most allergenic of all metallic materials. Not all nickel- allergic individuals will react to intraoral nickel, and it is currently not possible to predict which individuals will react. Because the frequency of nickel allergy is high, it is possible that individuals will become sensitized after placement of nickel containing alloys in the mouth. Nickel is a known allergen. [64] In a study of
Finnish adolescents, the prevalence of nickel allergy was found to be 30% in girls and 3% in boys. [65],[66]
This was thought to be related to sensitization to nickel by ear piercing as the prevalence in adolescents, with ear piercing it was found to be 31% and only 2% otherwise. Allergic responses are mediated through the immune system. The majority of dental allergies, including responses to nickel containing dental alloys, comprise type IV hypersensitivity reactions, cell mediated by T-lymphocytes. Nickel containing dental alloys can undergo corrosion with release of metal ions. [67],[68] High content nickel-titanium wires should be avoided in nickel sensitive patients, nickel free alternatives being available for use in such cases. [69] Bishara et al.[70] studied biodegradation of orthodontic appliances in vitro and showed that nickel ions released from orthodontic appliances of nickel- titanium and stainless steel increased over the first week then diminished over time. Gjerdt et al.[71] studied metal release from heat treated orthodontic wires and demonstrated that heat treatment of the alloys under laboratory conditions increased the release of metal ions-15-60 times. They showed significant initial increase in the concentration and mass of nickel in saliva sample of patient with fixed orthodontic appliances as compared to sampled saliva of patients without orthodontic appliances. Other studies have shown that the release of nickel ions is not proportional to the nickel content of orthodontic wires, but to the nature of the alloys and the method of construction of the appliance. Kerosuo et al.[72] studied the in vitro release of nickel and chromium ions from different types of simulated orthodontic appliances. Metal appliances immersed in 0.9% sodium chloride solution showed significantly higher cumulative release of nickel under dynamic (simulated function) compared to static condition. It should be noted that nickel ions released from metallic restorations and intraoral appliances will normally be swallowed and will not accumulate in the oral environment furthermore. The amount of nickel released from dental alloys is significantly less than that consumed orally as part of the dietary intake, although the ingested ions will obviously add to the overall burden of previously nickel sensitized patients. Kim et al.[37] opine that for patients allergic to nickel, the use of titanium or epoxy-coated wires during orthodontic treatment is recommended.
Clinical signs and symptoms seen in allergic reactions to nickel include oral edema, perioral stomatitis, gingivitis, and extra oral manifestations such as eczematous rashes. [73],[74],[75] The mechanisms of high allergy frequency to nickel are not known, but there is probably genetic component. [76],[77] In addition, the tendency of nickel containing alloys to release relatively large amount of nickel ions probably contributes to their allerginicity. Nickel ions are a documented mutagen in humans, but there is no evidence that nickel ions cause any carcinogenesis intraorally. [78] Galvanic Current or release of ions could account for many types of dyscrasias, such as lichenoid lesions, ulcers, leukoplakia, cancer and kidney disorder, although research has failed to find any correlation between dissimilar metals and tissue irritation. Future steps would be to find correlation between the problems observed in the mouth due to corrosion products and the results of corrosion tests in vitro. [78], According to Cioffi et al. thin layer activation (TLA) method in the biomedical field appears to be a suitable technique to monitor in real time the corrosion behavior of medical devices.

Protective Measure from Corrosion
To reduce corrosion, patient should avoid eating too much salty food. Salt provides chlorides ions which combines with hydrogen and produces acid which may cause corrosion. Chloride ion is detrimental for formation of passive layer on metal surface. Elastics should be clean or should be change frequently. Empty pockets at the bracket/adhesive interface should be prevented to avoid acceleration of corrosion process. Clinician should follow proper storage, maintenance and sterilization procedures and avoid intermetal contacts. Selection of attachment should be made that are less susceptible to corrosion. Indiscriminate use of heat or disinfection as well as thermal recycling should be avoided. Orthodontic arch wires and brackets can be coated with either titanium nitride or an epoxy resin. The former is used to improve hardness and reduce friction, the latter improves esthetics. Epoxy coating improves corrosion resistance by preventing attack by corrosive fluid. [37] Another method of reducing corrosion of metals is to add a corrosion inhibitor to a solution into which the material is placed but it very difficult to follow in oral cavity.
Summary
A primary requisite of any alloy metal used in the mouth is that it must not produce corrosion products that will be harmful to body. In spite of recent innovative metallurgical and technological advances and remarkable progress related to orthodontic materials, failures do occur. One of the reasons for these failures could be corrosion (material degradation) of orthodontic appliances. It causes severe and catastrophic disintegration of the metal body. Corrosion (material degradation) attack may be extremely localized and causes rapid mechanical failure of a structure, even though the actual volume loss of material is quite small. Surface roughening and deposit build up may have adverse effects on the efficiency of relative wire/bracket function in orthodontic treatment. Application of fluoride containing gel/toothpaste may affect efficiency of orthodontic appliances. In future nickel free materials should be expected in use. Future research is needed regarding material composition influencing corrosion, manufacturing of metallic brackets, influence of various diet pattern as well as diet substance on corrosion, use of topical fluoride treatment during orthodontic treatment for oral hygiene maintenance.
Sebuah gambaran dari degradasi material ortodontik pada rongga mulut
Chaturvedi1 TP, SN Upadhayay21 Departemen Ortodonti, Fakultas Ilmu Gigi, Institute of Medical Sciences, Varanasi, UP, India2 Departemen Teknik Kimia, TI, Banaras Hindu University di Varanasi, UP, India
ABSTRAK
Berbagai jenis peralatan ortodontik logam yang digunakan dalam pengelolaan maloklusi. Peralatan ini ditempatkan di bawah tekanan lingkungan mulut dan variasi seperti gaya pengunyahan, ‘loading alat’, fluktuasi suhu, jenis makanan dan air liur yang ditelan. Logam ini mengalami reaksi elektrokimia dengan lingkungan mulut mengakibatkan peleburan atau pembentukan senyawa kimia. Berbagai mikroorganisme dan ion agresif banyak dikandung lingkungan mulut dapat menyebabkan degradasi material (korosi) dan masalah lain yang sudah lama. Paduan ortodontik harus memiliki ketahanan korosi yang sangat baik untuk lingkungan mulut, yang sangat penting bagi biokompatibilitas serta untuk daya tahan alat ortodontik. Artikel ini meninjau berbagai aspek korosi (degradasi permukaan) paduan ortodontik. Ini mengeksplorasi strategi penelitian untuk menyelidiki biokompatibilitas bahan. Selama perawatan ortodontik, penggunaan nikel bebas, paduan lebih tahan korosi dan kurangnya penggunaan dari pasta gigi berfluoride yang mengandung atau gel yang diharapkan.
Keywords: Biokompatibilitas, korosi, paduan gigi, bahan degradasi, alergi nikel, paduan ortodontik, kawat ortodontik, degradasi permukaanBagaimana untuk mengutip artikel ini:Chaturvedi TP, Upadhayay SN. Sebuah gambaran dari degradasi material ortodontik pada rongga mulut. India J Dent Res 2010; 21:275-84
Bagaimana untuk mengutip URL ini:Chaturvedi TP, Upadhayay SN. Sebuah gambaran dari degradasi material ortodontik pada rongga mulut. India J Dent Res [online urut] 2010 [dikutip 2011 November 3]; 21:275-84. Tersedia dari: http://www.ijdr.in/text.asp?2010/21/2/275/66648
Bagaimana untuk mengutip URL ini:Chaturvedi TP, Upadhayay SN. Sebuah gambaran dari degradasi material ortodontik pada rongga mulut. India J Dent Res [online urut] 2010 [dikutip 2011 November 3]; 21:275-84. Tersedia dari: http://www.ijdr.in/text.asp?2010/21/2/275/66648
Biokompatibilitas bahan gigi sekarang menjadi kebutuhan mendasar dari perilaku klinis yang sukses di rongga mulut. Hal ini mengacu pada pengetahuan dari biologi, faktor resiko pasien, pengalaman klinis dan rekayasa. Ada dua faktor utama yang tampaknya menjadi penting dalam menentukan biokompatibilitas bahan gigi - beberapa melibatkan berbagai jenis degradasi korosi atau material dan lain-lain meliputi karakteristik permukaan. Bahan gigi dalam mulut berinteraksi terus menerus dengan cairan fisiologis. Air liur yang mengandung larutan hipotonik bioactonate, klorida, kalium, natrium, senyawa nitrogen dan protein. [1] Korosi, degradasi dinilai bahan dengan elektrokimia serangan, menjadi perhatian khususnya ketika peralatan ortodontik ditempatkan dalam lingkungan elektrolitik bermusuhan disediakan oleh mulut manusia. [2], [3] Berbagai jenis kawat dan lingkar digunakan dalam pengobatan misalnya maloklusi stainless steel, kobalt-kromium-nikel paduan, paduan nikel-titanium, β-titanium paduan, dll [Tabel 1]. Sebuah kawat ulet dapat dibentuk menjadi berbagai bentuk. Sebagai proses manufaktur, industri menggunakan paduan mematri untuk bergabung dengan komponen dasar dan sayap lingkar. Paduan perak mematri berbasis membentuk pasangan galvanik yang dapat menyebabkan terutama untuk

melepaskan ion tembaga dan seng. Solder sendi peralatan dilepas dan busur wajah, dan sendi dibrazing beberapa lengkung stainless steel dapat mempengaruhi sifat mekanik. [4] Tujuan dari artikel ini adalah untuk meninjau secara singkat aspek korosi (degradasi material) dan efeknya pada kabel ortodontik dan lingkar di lingkungan mulut, efek gel fluoride / pasta gigi pada peralatan ortodontik dan kepekaan nikel. Sebuah Ringkasan dari karya-karya eksperimental sedikit pada korosi paduan ortodontik (in vitro) diberikan dalam [Tabel 2], yang dapat mengeksplorasi strategi penelitian masa depan untuk sifat bahan ortodontik.
Table 1: Types of wires used for orthodontic treatment and their composition
Table 2: Summary of experimental work on the corrosion of orthodontic alloys (in vitro)
Melemahnya Tangga
Stainless steel menjadi rentan terhadap korosi intergranular, yang pada akhirnya dapat melemahkan paduan. Kekuatan tarik dari perak-disolder sendi stainless steel ortodontik akan terpengaruh oleh proses korosi. [12], [13] Meskipun ketahanan korosi yang baik dari Niti menekankan, kerusakan kabel ortodontik sering ditemukan dalam studi klinis dan mengalami degradasi yang disebabkan oleh korosi dalam lingkungan mulut. [14], [15] Menurut Zinelis dkk [16] Ag berbasis paduan solder memperkenalkan pasangan galvanis dengan paduan stainless steel, merangsang pelepasan ion logam seperti Cu. + + Dan Zn + +, sebagian besar elemen tercuci keluar dari solder perak paduan. Sebuah Vahed dkk [17] melaporkan. Bahwa kontak yang terlalu lama dalam air liur dirangsang menyebabkan pengurangan yang signifikan pada beban kegagalan tarik perak-disolder sendi stainless. Penurunan sifat tarik dibawa oleh kelemahan yang disebabkan oleh korosi lokal dari logam solder pada antarmuka solder / kawat. Dominasi Cu kaya partikel yang terbentuk di solder logam pada antarmuka memberikan efek galvanis mikro yang mengarah pada pembubaran selektif partikel-partikel ini dan melemahnya sesuai antarmuka. Korosi adalah penyebab utama pembubaran progresif mematri logam pengisi, menyebabkan detasemen sayap dari dasar braket selama terapi ortodontik atau pada debonding panggung. [18]
Sliding gesekan
Gesekan adalah fenomena yang umumnya mempengaruhi kemanjuran klinis dari peralatan ortodontik. Gaya gesek yang melawan gerakan gigi selama geser efek yang berbeda kombinasi lengkungan kawat braket (misalnya bahan, ukuran, bentuk dan angulasi), pengaruh misalnya ligasi material dan gaya kontak dan interaksi peralatan dengan misalnya lingkungan sekitarnya (Interbracket jarak dan cairan oral). Korosi meningkatkan gaya gesekan antara kawat ortodontik / braket interface lengkungan karena peningkatan kekasaran permukaan. [17], [18], [19]
Lokal nyeri / bengkak
Produk korosi telah terlibat dalam menyebabkan nyeri lokal atau pembengkakan di daerah peralatan ortodontik pada tidak adanya infeksi, yang dapat menyebabkan infeksi sekunder. [20], [21]Sitotoksik tanggapanBesi, nikel dan kromium adalah produk korosif utama dari stainless steel. Nikel dan kromium menginduksi Tipe-IV reaksi hipersensitivitas di dalam tubuh. [22] Logam ini menyebabkan respon beberapa sitotoksik termasuk penurunan dalam beberapa aktivitas enzim, gangguan jalur biokimia, karsinogenisitas, dan Mutagenisitas. [23], [24] Titanium kabel mengandung nikel dapat menyebabkan iritasi jaringan lokal pada beberapa pasien. Mangan dari alloy juga dikonsumsi dengan air liur yang menghasilkan toksisitas yang mengarah ke saraf, gangguan tulang, dll telah menyarankan bahwa paparan jangka panjang terhadap nikel yang mengandung bahan gigi mempengaruhi monosit manusia dan mukosa mulut sel. [25], [26]
Dekalsifikasi gigi
Berbagai asam terbentuk selama serangan mikroba pada peralatan ortodontik logam di lingkungan mulut. Biofilm untuk med pada permukaan gigi dengan bantuan sisa-sisa makanan dan produk metabolisme mikroba. Asam menyebabkan reduksi pH dan mempengaruhi dekalsifikasi gigi dan korosi peralatan logam. [27]
Pengaruh Korosi Pada Kabel Ortodontik
Korosi baja stainless
kawat baja orthodontic stainless yang umumnya terbuat dari baja tahan karat austenit yang mengandung sekitar 18% kromium dan nikel 8%. Secara umum, kabel ini memiliki biokompatibilitas yang baik dan ketahanan korosi yang tinggi dalam lingkungan mulut. Ini ‘owes’ ketahanan korosi properti untuk kromium, logam dasar yang sangat reaktif. Ketahanan korosi paduan tergantung pada film pasif, yang secara spontan bentuk (pasif) dan reformasi (repassivation) di udara dan di bawah kondisi basah paling. Oksigen diperlukan untuk membentuk dan memelihara film, sedangkan ion klorida keasaman dan dapat sangat merugikan untuk itu. [28] Keberadaan titik solder meningkatkan kerentanan korosi karena mereka memiliki kecenderungan untuk memancarkan arus electrogalvanic dengan air liur dan akibatnya melepaskan ion logam. Austenitic stainless steel mungkin kehilangan ketahanan terhadap korosi jika dipanaskan antara sekitar 400 o C dan 900 o C. Suhu tersebut berada dalam kisaran yang digunakan oleh dokter gigi untuk solder dan las. Penurunan ketahanan korosi disebabkan oleh presipitasi karbida kromium-besi di batas butir pada temperatur tinggi. [29] Air hujan tidak terjadi di bawah suhu ini dan kemungkinan korosi kurang. Korosi dari stainless steel dapat mengakibatkan sel galvanik karena terbentuk di satu atau lebih cara berikut:• Permukaan kekasaran dari stainless steel kawat dapat menyebabkan serangan korosi lokal.• Setiap dipotong atau abrasi dari stainless steel dengan tang baja karbon / bur baja karbon dapat bertindak sebagai sel galvanik, dan• sendi Brazed atau disolder dalam peralatan ortodontik juga dapat membentuk pasangan galvanik in vivo.Titanium dan Paduan nya (nikel-titanium paduan, β-titanium paduan, titanium paduan aluminium-vanadium)
Titanium sangat tahan korosi akibat efek pasivator diberikan oleh lapisan tipis titanium oksida yang terbentuk pada permukaannya. Ketika lapisan oksida yang stabil dipecah atau larut dan tidak mampu untuk reformasi di bagian permukaan, dan paduan titanium yang ada sebagai bahan korosif karena banyak logam dasar lainnya. Kekasaran permukaan paduan mengandung titanium lebih dibandingkan dengan kawat stainless steel, yang dapat bertindak sebagai sel galvanik dalam mulut. [30], [31], [32]
Jenis Korosi di Wires Ortodonti
Fitur yang menentukan bagaimana dan mengapa bahan gigi menimbulkan korosi adalah reaksi oksidasi dan reduksi serta passivasi atau pembentukan film oksida logam pasif pada permukaan logam. [33]

Berbagai bentuk korosi ditunjukkan pada [Gambar 1] dan digambarkan sebagai berikut.
Korosi seragam
Sebuah korosi seragam adalah setiap reaksi kimia atau elektrokimia yang keluar seragam pada permukaan terkena seluruh atau atas area yang luas. Ini adalah jenis yang paling umum dari korosi, yang terjadi dengan semua logam pada tingkat yang berbeda. Proses ini timbul dari interaksi logam dengan lingkungan dan pembentukan selanjutnya dari hidroksida atau senyawa organologam. Untuk korosi seragam, lingkungan korosif harus memiliki akses yang sama ke seluruh bagian permukaan, dan logam itu sendiri harus bersifat metalurgi dan komposisinya seragam. Serangan Seragam mungkin tidak terdeteksi sebelum sejumlah besar logam yang terlarut.
Pitting korosi
Pitting adalah bentuk serangan ekstrim yang menghasilkan lubang pada permukaan logam. Ini biasanya terjadi pada logam dasar, yang dilindungi oleh film tipis secara alami membentuk suatu oksida. Ini telah diidentifikasi dalam kurung dan kawat. Dengan adanya klorida di lingkungan, film lokal rusak dan pembubaran cepat dari logam yang mendasari terjadi dalam bentuk lubang. Permukaan dari kawat baja dan Niti steel mungkin menunjukkan celah-celah dan pori-pori yang dapat menimbulkan serangan karena mereka mewakili situs rentan terhadap korosi. Eksperimen polarisasi Potentiodynamic dan pemindaian pengamatan mikroskopis elektron dari archwires terdiri dari stainless steel, CoCr, NiCr, Niti dan Beta-Ti terkena korosi elektrokimia pada saliva buatan telah menunjukkan bukti dari korosi pitting yang terbentuk pada permukaan kawat. [34] Liu [35] mempelajari karakteristik mekanik dan perilaku korosi lapisan aluminium nitrida paduan titanium pada gigi, terutama dalam nikel-dan kromium berbasis bahan gigi. Mereka diuji perilaku korosi dalam larutan NaCl 0,9% dan mengamati potensi yang lebih tinggi korosi positif dan kerapatan yang lebih rendah arus korosi pada paduan memiliki dilapisi dengan titanium nitrida aluminium dibandingkan dengan paduan gigi dilapisi. Selain itu, korosi pitting secara substansial dikurangi oleh kerja TiAlN pelapisan. Es Souni dkk [36] menemukan bahwa paduan Cr-Co (Elgiloy) menunjukkan korosi pitting tinggi dibandingkan dengan paduan Niti, potensi repassivation lebih rendah dan peningkatan densitas arus sekali pitting telah terjadi.. Kim et al [37]. Menunjukkan bahwa nikel titanium dan kawat stainless steel yang rentan terhadap korosi pitting dan lokal.
Korosi celah
Korosi celah terjadi antara dua permukaan yang terdekat atau di tempat-tempat terbatas di mana pertukaran oksigen tidak tersedia. Hal ini sering terjadi melalui penerapan bagian-bagian non-logam dari logam (yaitu, elastomer ligatures pada bracket). Penurunan pH dan peningkatan konsentrasi ion klorida adalah dua faktor penting dalam inisiasi dan propagasi dari fenomena korosi celah. Ketika keasaman media meningkat seiring dengan waktu lapisan pasif paduan larut dan mempercepat proses korosi lokal. Korosi celah baja tahan karat dalam larutan garam soda secara luas dikenal. Produk korosi Fe, Cr, dan Ni, komponen utama dari stainless steel, menumpuk di celah dan membentuk larutan yang sangat asam klorida dimana tingkat korosi sangat tinggi. [38], [39] Platt et al [40] melaporkan bahwa baja tahan karat dupleks 2205 merupakan alternatif ditingkatkan untuk 316L untuk fabrikasi braket ortodontik bila digunakan dalam hubungannya dengan Ti, paduan, atau kawat stainless steel arch.. Rogers [41]
menunjukkan bahwa dengan elektroplating dengan emas sebelum dan sesudah solder perak, stainless steel mencegah korosi celah. Daur ulang dan kurung kawat ortodontik pernah umum di banyak negara, tetapi tidak dianjurkan di banyak negara sekarang. Daur ulang dapat terdiri dari bahan kimia panas dan proses mekanis yang dapat menyebabkan korosi celah sendi dibrazing dipercepat.
Kelelahan dan erosi-korosi
Erosi-korosi adalah peningkatan laju kemerosotan atau serangan pada materi karena gerakan relatif antara fluida korosif dan permukaan material. Cairan diam atau lambat-mengalir akan menyebabkan laju korosi rendah atau sederhana, tetapi gerakan yang cepat dari cairan korosif fisik mengikis dan menghilangkan film produk pelindung korosi, memperlihatkan paduan reaktif bawah dan mempercepat korosi. Korosi resah (jenis korosi erosi) bertanggung jawab untuk sebagian besar logam yang dilepaskan ke jaringan. [42], [43] conjoint aksi serangan kimia dan hasil mekanik di korosi mengeluh. Ini terjadi pada area kontak bahan di bawah beban dan menemukan analog dalam antarmuka kawat slot-lengkungan braket.
Korosi intergranular
Karena sifat yang lebih reaktif dari batas butir, korosi intergranular terjadi berdekatan dengan batas butir dengan sedikit korosi biji-bijian. Lengkungan stainless steel mengalami berbagai suhu, yang dikenal sebagai temperatur sensitisasi, menjalani perubahan dalam mikro mereka. Fenomena ini disebabkan oleh presipitasi karbida pada batas butir. [44] Berge dkk [28] melaporkan bahwa kawat baja austenitik stainless nikel dan kromium rilis dalam jumlah yang lebih tinggi dari kobalt-kromium kabel, mengakibatkan perubahan warna, karat, atau bahkan pecah..
Korosi Galvanik
Jenis korosi terjadi karena kopling galvanik logam berbeda yang terlibat dalam logam yang kurang logam tahan korosi menjadi anoda dan biasanya menimbulkan korosi. Dalam situasi klinis, dua paduan yang berbeda memiliki potensi korosi yang berbeda sering ditempatkan dalam kontak seperti dalam kurung dan kawat ortodontik lengkungan. Hal ini dapat menyebabkan korosi galvanik yang mengarah untuk melepaskan preferensial ion logam dari logam anodik atau paduan. Rasio luas permukaan dari dua paduan yang berbeda merupakan faktor yang sangat penting karena mempengaruhi perilaku korosi galvanik. Rasio wilayah yang tidak menguntungkan, yang terdiri dari katoda anoda besar dan kecil, mungkin menyebabkan laju korosi lebih besar dari paduan anodik. Reed dan Willman [45] menunjukkan adanya arus galvanik dalam rongga mulut mungkin pertama kalinya secara rinci. Perkiraan nilai untuk besarnya didirikan. Burse [46] menggambarkan sebuah protokol eksperimental untuk in vivo menodai evaluasi dan menunjukkan pentingnya rasio unsur yang tepat dalam paduan emas. Masahir dkk [47]. Menunjukkan paduan Niti ditambah dengan SUS 304 atau Ti dipamerkan kepadatan arus galvanik yang relatif besar bahkan setelah 72 jam. Disarankan bahwa kopling SUS 304-Niti dan Ti-Niti sangat dapat mempercepat korosi paduan Niti, yang berfungsi sebagai anoda. Rasio area yang berbeda anoda-katoda yang digunakan dalam penelitian ini memiliki pengaruh yang kecil terhadap perilaku korosi galvanik. Tufekci dkk [48] menjelaskan teknik analisis yang sangat sensitif yang menunjukkan pelepasan unsur-unsur individu selama periode bulan yang tampaknya berkorelasi dengan fase struktural mikro dalam paduan.. Beberapa
bentuk korosi elektrokimia didasarkan pada mekanisme yang menghasilkan daerah homogen. Kegagalan bisa diminimalkan dalam sambungan solder ortodontik dengan menggunakan pasangan bahan yang meminimalkan efek galvanik galvanik dan mikro.
Stres korosi
Stres retak korosi mengacu pada retak yang disebabkan oleh adanya tegangan tarik simultan dalam medium korosif. Proses ini berbahaya dapat mengganggu integritas mekanik kawat ortodontik. Ketika lengkung kawat berikatan dengan lengkung adalah terikat pada banyak gigi, status reaktivitas dari paduan yang mengalami. Hasil reaktivitas meningkat dari generasi tegangan tarik dan tekan dikembangkan secara lokal karena kawat, multiaksial tiga memuat dimensi. Jadi, perbedaan potensial elektrokimia terjadi dengan situs tertentu bertindak sebagai anoda dan permukaan lain yang bertindak sebagai katoda. Kabel ortodontik niti tetap dalam lingkungan mulut selama beberapa bulan dan mengalami sejumlah besar beban kecil selama pengunyahan. Meskipun ketahanan korosi yang baik dari Niti saat menekankan, rusaknya kabel Niti ortodontik telah sering ditemukan dalam studi klinis. [49], [50] Wang et al [51]. Korosi retak stres mempelajari Niti pada saliva buatan dan menunjukkan bahwa kawat ortodontik Niti patah oleh korosi retak stres selama layanan. Perubahan sedikit dalam suhu menyebabkan transformasi fase dinamis, yang menyebabkan perubahan dalam keadaan permukaan.
Kerusakan Hidrogen
Dalam keadaan tertentu, kawat ortodontik dapat menyerap hidrogen dalam kondisi katodik. Kehadiran hidrogen diserap menurunkan daktilitas dari logam. Hal ini dapat logam reaktif embrittle seperti titanium, vanadium, niobium, dll [1], [6]
Pengaruh Lingkungan Oral Dalam lingkungan mulut, obat kumur yang mengandung fluoride komersial, pasta gigi dan gel profilaktik secara luas digunakan untuk mencegah karies gigi atau menghilangkan sensitivitas gigi atau untuk membersihkan mulut yang tepat setelah aplikasi sikat normal dengan pasta gigi. [52], [53] Efek merugikan dari ion fluoride pada ketahanan korosi Ti atau Ti paduan telah banyak dilaporkan. Ion fluorida sangat agresif pada film TiO 2 pelindung terbentuk pada paduan Ti dan Ti. Karena permukaan terluar dari kawat lengkung Niti mengandung terutama TiO 2 film dengan jumlah jejak NiO, korosi fluorida yang disempurnakan kabel lengkungan Niti di lingkungan yang mengandung fluoride telah dipertimbangkan. [54], [55] Fluorida yang mengandung lingkungan dapat menembus ke celah-celah sempit di antara lengkungan kawat ortodontik dan braket di mulut yang tidak dibersihkan secara menyeluruh. Konsentrasi fluoride topikal tinggi akan tinggal di tempat dan menyerang antarmuka kawat / braket lengkungan tergantung pada konsentrasi fluoride. Hal ini dapat meningkatkan gaya gesekan antara kawat lengkung dan braket. Menggunakan agen topikal fluoride dengan kawat Niti dapat menurunkan sifat fungsional mekanik bongkar kabel dan berkontribusi untuk perawatan ortodontik berkepanjangan. [56], [57] pasien ortodontik yang diperlukan untuk mempertahankan tingkat tinggi kebersihan mulut, yang meliputi menyikat gigi secara teratur. Penelitian in vitro [58], [59] pada efek menyikat gigi menunjukkan peningkatan yang signifikan dalam rilis unsur dari paduan nikel saat pasta gigi digunakan, bagaimanapun, tanpa pasta gigi tidak ada peningkatan yang signifikan dalam rilis unsur. Ada juga bukti yang menunjukkan bahwa beberapa larutan kumur juga dapat meningkatkan pelepasan ion dari titik
solder perak di peralatan ortodontik. Schiff dkk [60]. Mempelajari ketahanan korosi dari tiga jenis kurung (kobalt-kromium, besi kromium-nikel dan titanium berbasis kurung) dalam tiga pencuci mulut fluoride. Hasil menunjukkan bahwa bahan-bahan braket dapat dibagi menjadi dua kelompok: Ti dan FeCrNi dalam satu dan CoCr, yang memiliki sifat dekat dengan orang-orang dari Pt. Banyak penelitian telah menunjukkan bahwa ion fluorida dapat menghancurkan protektif dari film TiO 2 permukaan pasif pada Ti atau paduan Ti, yang menyebabkan korosi morfologi menyerang, penurunan resistensi polarisasi dan kepadatan arus meningkat anodik atau pelepasan ion logam. [61]
Selanjutnya, ketahanan korosi Niti menurun pada peningkatan konsentrasi NaF dalam saliva buatan. Schiff dkk [62] mempelajari ketahanan korosi kawat ortodontik pada tiga obat kumur komersial yang berbeda dan menemukan bahwa kabel Niti dikenakan korosi yang parah dalam Na 2 4 obat kumur yang mengandung FPO.. Huang [63] mempelajari variasi topografi permukaan yang berbeda nikel-titanium kabel lengkungan ortodontik pada berbagai lingkungan komersial yang mengandung fluoride. Empat diuji Niti lengkungan kabel memiliki variasi topografi permukaan yang berbeda, tergantung pada konsentrasi ion fluorida. Kawat lengkung kemunculan produsen dan lingkungan memiliki pengaruh yang signifikan secara statistik pada variasi kekasaran permukaan. Peningkatan kekasaran permukaan kawat ortodontik Niti lengkungan di lingkungan komersial yang mengandung fluoride harus diperhitungkan ketika mempertimbangkan efektivitas peralatan ortodontik.
Kabel Orthodonti Mengandung Nikel
Paduan yang mengandung nikel menemukan aplikasi luas dalam orthodonsi, termasuk kurung logam, kabel lengkungan, band, mata air dan kawat pengikat. Untuk bahan yang paling, permukaan kasar mempromosikan korosi. Keraguan tetap tentang biokompatibilitas Ni berbasis paduan bila digunakan dalam kedokteran gigi. Penggunaan nikel menjadi perhatian khusus karena ini adalah yang paling alergi dari semua bahan logam. Tidak semua individu yang alergi nikelyang akan bereaksi terhadap nikel intraoral, dan saat ini tidak mungkin untuk memprediksi yang individu akan bereaksi. Karena frekuensi alergi nikel tinggi, adalah mungkin bahwa individu akan menjadi peka setelah penempatan mengandung nikel paduan dalam mulut. Nikel adalah alergen yang diketahui. [64] Dalam sebuah studi tentang remaja Finlandia, prevalensi alergi nikel ditemukan menjadi 30% pada anak perempuan dan 3% pada anak laki-laki. [65], [66] Hal ini diduga terkait dengan sensitisasi terhadap nikel dengan tindik telinga sebagai prevalensi pada remaja, dengan tindik telinga itu ditemukan menjadi 31% dan hanya 2% jika tidak. Respon alergi dimediasi melalui sistem kekebalan tubuh. Mayoritas alergi gigi, termasuk tanggapan terhadap nikel yang mengandung paduan gigi, terdiri dari tipe IV reaksi hipersensitivitas, sel dimediasi oleh T-limfosit. Mengandung nikel paduan gigi dapat mengalami korosi dengan pelepasan ion logam. [67], [68] kandungan nikel –titaniumyang tinggi harus dihindari pada pasien yang sensitif nikel,kabel nikel adalah alternative yang tersedia untuk digunakan dalam kasus tersebut. [69] Bishara dkk [70] mempelajari biodegradasi peralatan ortodontik in vitro dan menunjukkan bahwa ion nikel dilepaskan dari peralatan ortodontik nikel-titanium dan stainless steel meningkat selama minggu pertama kemudian berkurang dari waktu ke waktu.. Gjerdt dkk [71] mempelajari pelepasan logam dari panas dirawat kabel ortodontik dan menunjukkan bahwa perlakuan panas paduan dalam kondisi laboratorium meningkatkan pelepasan ion logam-15-60 kali.. Mereka menunjukkan peningkatan awal yang signifikan dalam konsentrasi dan massa nikel dalam sampel air liur pasien dengan alat ortodontik tetap sebagai sampel dibandingkan dengan air liur pasien tanpa peralatan ortodontik. Penelitian lain menunjukkan bahwa

pelepasan ion nikel tidak sebanding dengan kandungan nikel kawat ortodontik, tetapi sifat paduan dan metode konstruksi alat. Kerosuo dkk [72] mempelajari dalam rilis vitro ion kromium nikel dan dari berbagai jenis peralatan ortodontik simulasi.. Peralatan logam direndam dalam larutan natrium klorida 0,9% menunjukkan rilis kumulatif secara signifikan lebih tinggi dari nikel dibawah dinamis (fungsi simulasi) dibandingkan dengan kondisi statis. Perlu dicatat bahwa nikel ion dilepaskan dari restorasi logam dan peralatan intraoral biasanya akan tertelan dan tidak akan terakumulasi dalam lingkungan mulut selanjutnya. Jumlah nikel dilepaskan dari alloy gigi secara signifikan kurang dari itu dikonsumsi secara oral sebagai bagian dari asupan makanan, meskipun ion tertelan jelas akan menambah beban keseluruhan dari pasien peka sebelumnya nikel. Kim et al [37]. Berpendapat bahwa untuk pasien alergi terhadap nikel, penggunaan titanium atau epoksi-dilapisi kabel selama perawatan ortodontik dianjurkan.
Tanda dan gejala klinis terlihat pada reaksi alergi terhadap nikel termasuk edema lisan, perioral stomatitis, radang gusi, dan manifestasi oral tambahan seperti ruam eczematous. [73], [74], [75] Mekanisme alergi frekuensi tinggi untuk nikel tidak diketahui, tetapi mungkin ada komponen genetik. [76], [77] Selain itu, kecenderungan paduan mengandung nikel untuk melepaskan jumlah yang relatif besar ion nikel mungkin memberikan kontribusi untuk allerginicity mereka. Ion nikel adalah mutagen didokumentasikan pada manusia, tetapi tidak ada bukti bahwa ion nikel menyebabkan karsinogenesis intraorally. [78] Sekarang galvanic atau pelepasan ion bisa menjelaskan berbagai jenis diskrasia, seperti lesi lichenoid, borok, leukoplakia, kanker dan gangguan ginjal, meskipun penelitian telah gagal untuk menemukan korelasi antara logam berbeda dan iritasi jaringan. Langkah ke depan akan menemukan korelasi antara masalah diamati dalam mulut karena produk korosi dan hasil tes korosi dalam in vitro. [78], Menurut Cioffi et al. aktivasi lapisan tipis (TLA) metode di bidang biomedis tampaknya menjadi teknik yang sesuai untuk memantau secara real time perilaku korosi peralatan medis.
Ukuran pelindung dari korosi
Untuk mengurangi korosi, pasien harus menghindari makan terlalu banyak makanan asin. Garam menyediakan ion klorida yang akan bergabung dengan hidrogen dan menghasilkan asam yang dapat menyebabkan korosi. Ion klorida merugikan bagi pembentukan lapisan pasif pada permukaan logam. Elastis harus bersih atau harus seringdiganti.Celah kosong di antarmuka braket / perekatnya harus dicegah untuk menghindari percepatan proses korosi. Klinisi harus mengikuti prosedur yang tepat penyimpanan, pemeliharaan dan sterilisasi dan menghindari kontak intermetal. Pemilihan harus dibuat lampiran yang kurang rentan terhadap korosi. Sembarangan penggunaan panas atau disinfeksi serta daur ulang termal harus dihindari. Lengkungan kawat ortodontik dan kurung dapat dilapisi dengan titanium nitrida baik atau resin epoksi. Yang pertama digunakan untuk meningkatkan kekerasan dan mengurangi gesekan, yang terakhir meningkatkan estetika. Pelapisan epoksi meningkatkan ketahanan korosi dengan mencegah serangan oleh cairan korosif. [37] Metode lain untuk mengurangi korosi logam adalah dengan menambahkan inhibitor korosi untuk solusi di mana materi ditempatkan tetapi sangat sulit untuk mengikuti rongga mulut.
Ringkasan
Sebuah syarat utama dari setiap logam paduan yang digunakan dalam mulut adalah bahwa ia tidak harus
menghasilkan produk korosi yang akan berbahaya bagi tubuh. Meskipun baru-baru ini kemajuan teknologi metalurgi dan inovatif dan kemajuan luar biasa yang berhubungan dengan bahan ortodontik, kegagalan tidak terjadi. Salah satu alasan kegagalan tersebut bisa korosi (degradasi material) dari peralatan ortodontik. Hal ini menyebabkan disintegrasi parah dan bencana tubuh logam. Korosi (degradasi material) serangan mungkin sangat lokal dan menyebabkan kegagalan mekanis cepat struktur, meskipun kehilangan volume aktual bahan yang cukup kecil. Permukaan roughening dan deposito membangun mungkin memiliki efek buruk pada efisiensi relatif kawat / braket fungsi dalam perawatan ortodontik. Aplikasi fluorida yang mengandung gel / pasta gigi dapat mempengaruhi efisiensi peralatan ortodontik. Dalam nikel masa depan bahan-bahan gratis harus diharapkan digunakan. Penelitian di masa depan diperlukan tentang komposisi bahan yang mempengaruhi korosi, pembuatan kurung logam, pengaruh berbagai pola diet serta substansi diet pada korosi, penggunaan fluoride topikal pengobatan selama perawatan ortodontik untuk pemeliharaan kebersihan mulut.
RINGKASAN
Artikel ini meninjau berbagai aspek korosi (degradasi permukaan) paduan ortodontik dan tujuan dari artikel ini adalah untuk meninjau secara singkat aspek korosi (degradasi material) dan efeknya pada kabel ortodontik dan lingkar di lingkungan mulut, efek gel fluoride / pasta gigi pada peralatan ortodontik dan kepekaan nikel.Ini mengeksplorasi strategi penelitian yang menyelidiki biokompatibilitas bahan. Selama perawatan ortodontik, penggunaan nikel bebas, paduan lebih tahan korosi dan kurangnya pengggunaan dari pasta gigi berfluoride yang mengandung gel yang diharapkan sangat berpengaruh untuk kesehatan gigi dan mulut serta keberhasilan dari perawatan orthodonti.
Sebuah syarat utama dari setiap logam paduan yang digunakan dalam mulut adalah bahwa bahan harus tidak menghasilkan produk korosi yang akan berbahaya bagi tubuh. Meskipun baru-baru ini kemajuan teknologi metalurgi dan inovatif dan kemajuan luar biasa yang berhubungan dengan bahan ortodontik, Salah satu alasan kegagalan tersebut bisa korosi (degradasi material) dari peralatan ortodontik. Hal ini menyebabkan disintegrasi parah dan bahaya logam bagi tubuh.Serangan korosi (degradasi material) mungkin sangat lokal dan menyebabkan kegagalan mekanis struktur tubuh, meskipun kehilangan volume bahan yang cukup kecil. Permukaan roughening mungkin memiliki efek buruk pada efisiensi relatif kawat / braket yang berfungsi dalam perawatan ortodontik. Aplikasi fluorida yang mengandung gel / pasta gigi dapat mempengaruhi efisiensi peralatan ortodontik.Penelitian di masa depan diperlukan tentang komposisi bahan yang mempengaruhi korosi, pembuatan kurung logam, pengaruh berbagai pola diet serta substansi diet pada korosi, penggunaan fluoride topikal pengobatan selama perawatan ortodontik untuk pemeliharaan kebersihan mulut.
Berbagai jenis peralatan ortodontik logam yang digunakan dalam pengelolaan maloklusi. Peralatan ini ditempatkan di bawah tekanan lingkungan mulut dan variasi seperti gaya pengunyahan, ‘loading alat’, fluktuasi suhu, jenis makanan dan air liur yang ditelan. Logam ini mengalami reaksi elektrokimia dengan lingkungan mulut mengakibatkan peleburan atau pembentukan senyawa kimia. Berbagai mikroorganisme dan ion agresif banyak dikandung lingkungan mulut dapat menyebabkan degradasi material (korosi). Paduan ortodontik harus memiliki ketahanan korosi yang sangat baik untuk lingkungan mulut, yang sangat penting bagi biokompatibilitas serta untuk daya tahan alat ortodontik.
Bahan orthoodonti Stainless steel menjadi rentan terhadap korosi intergranular,yang pada akhirnya dapat melemahkan paduan. Kekuatan tarik dari perak-disolder sendi stainless steel ortodontik akan terpengaruh oleh proses korosi bahwa kontak yang terlalu lama dalam air liur menyebabkan pengurangan yang signifikan pada beban kegagalan tarik perak-disolder sendi stainless. Penurunan sifat tarik dibawa oleh kelemahan yang disebabkan oleh korosi lokal dari logam.Sliding gesekan adalah fenomena yang umumnya mempengaruhi kemanjuran klinis dari peralatan ortodontik. Gaya gesek yang melawan gerakan gigi selama geser efek yang berbeda kombinasi lengkungan kawat braket (misalnya bahan, ukuran, bentuk dan angulasi), pengaruh misalnya ligasi material dan gaya kontak dan interaksi peralatan dengan lingkungan sekitarnya (Interbracket jarak dan cairan oral). Korosi meningkatkan gaya gesekan antara kawat ortodontik / braket interface lengkungan karena peningkatan kekasaran permukaan. [17], [18],[19] Titanium kabel mengandung nikel dapat menyebabkan iritasi jaringan lokal pada beberapa pasien. Mangan dari alloy juga dikonsumsi dengan air liur yang menghasilkan toksisitas yang mengarah ke saraf, gangguan tulang, dll telah disarankan bahwa penggunan jangka panjang terhadap nikel yang mengandung bahan gigi mempengaruhi monosit manusia dan sel mukosa mulut. [25], [26] kawat baja orthodontic stainless yang umumnya terbuat dari baja tahan karat austenit yang mengandung sekitar 18% kromium dan nikel 8%. Secara umum, kabel ini memiliki biokompatibilitas yang baik dan ketahanan korosi yang tinggi dalam lingkungan mulut
Erosi-korosi adalah peningkatan laju kemerosotan atau serangan pada materi karena gerakan relatif antara fluida korosif dan permukaan material. Cairan diam atau lambat-mengalir akan

menyebabkan laju korosi rendah atau sederhana, tetapi gerakan yang cepat dari cairan korosif fisik mengikis dan menghilangkan film produk pelindung korosi, memperlihatkan paduan reaktif bawah dan mempercepat,jadi sangat penting memperhatikan bahan yang digunakan untuk perawatan orthodonti seperti ada tidaknya efek toksisitas bagi tubuh,tahan serta ketahanan bahan yang gunakan terhadap korosi karena jika tidak awal dari ketidak cocokan seseorang dengan bahan orthodonsi yang digunakannya akan timbul tanda dan gejala klinis misalnya terlihat reaksi alergi terhadap nikel edema pada lingkungan mulut,perioral stomatitis,radang gusi dan manifestasi oral, Pelapisan epoksi meningkatkan ketahanan korosi dengan mencegah serangan oleh cairan korosif. [37]
Referensi
1. Chaturvedi TP. An overview of the corrosion aspect of dental implants (titanium and its alloys).
Indian J Dental Res 2009;20:91-8.
2. Maijer R, Smith DC. Corrosion of orthodontic bracket bases. Am J Orthod Dentofac Orthop
1982;81:43-8.
3. Maijer R, Smith DC. Biodegradation of the orthodontic bracket system. Am J Orthod Dentofac
Orthop 1986;90:195-8.
4. House K, Sernetz F, Dymock D, Sandy JR, Ireland AJ. Corrosion of orthodontic appliances: Should we
care? Am J Orthod Dentofacial Orthop 2008;133:584-92.
5. Eliades T, Athanasiou AE. In vivo aging of orthodontic alloys: Implications for corrosion potential,
nickel release, and biocompatibility. Angle Orthod 2002;72:222-37.
6. Brantley WA, Eliades T, editors. Orthodontic materials: Scientific and clinical aspects. Stuttgart:
Thieme; 2001. p. 77-103.
7. Chaturvedi TP, Bansal R. Biocompatibility of dental implant materials: An overview. J Indian Dent
Assoc 2008;2:335-7.
8. Jia W, Beatty MW, Reinhardt RA, Petro TM, Cohen DM, Maze CR, et al. Nickel release from orthodontic arch wires and cellular immune response to various nickel concentrations. J Biomed
Mater Res 1999;48:488-95.
9. Dunlap CL, Vincent SK, Barker BF. Allergic reaction to orthodontic wire: Report of case. J Am Dent
Assoc 1989;118:449-500.
10. Greppi AL, Smith DC, Woodside DG. Nickel hypersensitivity reactions in orthodontic patients. Univ
Tor Dent J 1989;J3:11-4.
11. Kerosuo H, Moe G, Kleven E. In vitro release of nickel and chromium from different types of
simulated orthodontic appliances. Angle Orthod 1995;65:2111-6.
12. Iijima M, Endo K, Ohno H, Yonekura Y, Mizoguchi I. Corrosion behavior and surface structure of
orthodontic Ni-Ti alloy wires. Dent Mater J 2001;20:1103-13.
13. Hunt NP, Cunningham SJ, Golden CG, Sheriff M. An investigation into the effect of polishing on surface hardness and corrosion of orthodontic arch wires. Angle Orthod 1999;69:5433-40.
14. Yonekura Y, Endo K, Iijima M, Ohno H, Mizoguchi I. In vitro corrosion characteristics of
commercially available orthodontic wires. Dent Mater J 2004;23:2197-202.
15. Platt JA, Guzman A, Zuccari A, Thornburg DW, Rhodes BF, Oshida Y, et al. Corrosion behavior of 2205 duplex stainless steel. Am J Orthod Dentofac Orthop 1997;112:69-79. Zinelis S, Annouski O, Eliades T, Makou M. Elemental composition of brazing alloys in metallic orthodontic brackets.
Angle Orthod 2004;74:394-9.
16. Vahed A, Lachman N, Robert D. Failure investigation of soldered stainless steel orthodontic
appliances exposed to artificial saliva. Dent Mater 2007;23:855-61.
17. Eliades T. Orthodontic materials research and applications: Part 2. Current status and projected future developments in materials and biocompatibility. Am J Orthod Dentofac Orthop
2007;131:253-64.
18. Matasa CG. Orthodontic attachment corrosion susceptibilities. J Clin Orthod 1995;29:16-
20.
19.Matasa CG. Attachment corrosion and its testing. J Clin Orthod 1995;24:16-23.
20. Maruthamuthu S. Electrochemical behavior of microbes on orthodontic wires. Curr Sci
2005;89:988-1005.
21. Pereira ML, Silva A, Tracana R, Carvalho GS. Toxic effects caused by stainless steel corrosion
products on mouse seminiferous cells. Cytobios 1994;77:73-80.
22. Veien NK, Bochhorst E, Hattel T, Laurberg G. Stomatitis or systemically-induced contact-dermatitis.
Contact Dermatitis 1994;30:210-213.
23. Waheidi EM. Allergic reaction to nickel orthodontic wire: A case report. Quintessence Int
1995;26:385-387.
24. Dunlap CL, Kirk Vincent S, Barker BF. Allergic reaction to orthodontic wire: Report of a case. J Am
Dent Assoc 1989;118:449-50.
25. Christopher M, Brett A, Ioanitescu I, Trandafir F. Influence of the biological fluid on the corrosion of
the biological fluid on the corrosion of dental amalgam. Corros Sci 2004;46:2803-16.
26. Merritt K, Brown SA. Release of hexavalent chromium from corrosion of stainless steel and cobalt-
chromium alloys. J Biomed Mater Res 1995;29:627-33.
27. Berge M, Gjerdet NR, Erichsen ES. Corrosion of silver soldered orthodontic wires. Acta Odont Scand
1982;40:75-92.
28. Choubey A, Balasubramaniam R, Basu B. Effect of replacement of V by Nb and Fe on the electrochemical and corrosion behavior of Ti-6Al-4V in simulated physiological environment. J
Alloys Comp 2004;381:288-94.
29. Sarkar NK, Redmond W, Schwaninger B, Goldberg AJ. The chloride corrosion behaviour of four
orthodontic wires. J Oral Rehabil 1983;10:121-8.
30. Grimsdottir MR, Gjerdet NR, Hensten-Pettersen A. Composition and in vitro corrosion of
orthodontic appliances. Am J Orthod Dentofac Orthop 1992;101:525-32.
31. Oshida Y, Sachdeva RC, Miyazaki S. Microanalytical characterization and surface modification of
TiNi orthodontic arch wires. Bio-Med Mat Engg 1992;2:51-69.
32. Jacobs JJ, Gilbert JL, Urbani RM. Corrosion of metal orhopaedic implants. J Bone Joint Surg Am
1988;80:268-82.
33. Barret RD, Bishara SE, Quinn JK. Biodegradation of orthodontic appliances, Part I: Biodegradation of

nickel and chromium in vitro. Am J Orthod Dentofac Orthop 1993;103:8-14.
34. Liu GT, Duh JG, Chung K, Wang J. Mechanical characteristics and corrosion behavior of (Ti, Al) N
coatings on dental alloys. Surface Coating Technol 2005;20:2100-5.
35. Es-Souni M, Fisher-Brandies H. On theproperties of two binary NiTi shape memory alloys: Effect of surface finish on the corrosion behavior and in vitro biocompatibility. Biomaterials 2002;23:2887-
94.
36. Kim H, Johnson JW. Corrosion of stainless steel, nickel-titanium, coated nickel-titanium, and
titanium orthodontic wires. Angle Orthod 1999;69:39-44.
37. Matasa CG. Characterization of used orthodontic brackets. In: Eliades G, Eliades T, Brantley WA, Watts DC, editors. In vivo-aging of dental biomaterials. Chicago, Ill: Quintessence. In press. Olefjord
I, Wegrelius L. Surface analysis of passive state. Corros Sci 1990;31:89-98.
38. Platt JA, Guzman A, Zuccary A, Moor BK. Corrosion behavior of 2205 douplex stainless steel. Am J
Orthod Dentofac Orthop 1997;112:69-79.
39. Rogers OW. A study in the control crevice corrosion of silver soldered stainless joints. Br Dent J
1977;143:397-403.
40. Eliades T, Eliades G, Athanasiou AE, Bradley TG. Surface characterization of retrieved NiTi
orthodontic arch wires. Eur J Orthod 2000;22:317-26.
41. Eliades T, Eliades G, Watts DC. Intraoral aging of the inner headgear component: A potential
biocompatibility concern? Am J Orthod Dentofac Orthop 2001;119:300-6.
42. Sutow E, Jones DW, Milne EL. The corrosion behavior of implants materials. J Dent Res
1985;64:842-7.
43.Reed GJ, Willman W. Galvinism in the oral cavity. J Am Dent Assoc 1940;27:1471.
44. Burse AB. Comparison of the in vitro and in vivo tarnish of three gold alloys. J Biomed Mat Res

1972;6:267-77.
45. Iijima M, Endo K, Yuasa K. Ohno H, Hayashi K. Kakizaki M. Galvanic corrosion behavior of
orthodontic arch wire alloys coupled to bracketal.loys. Angle Orthod 2005;76:705-11.
46. Tufekci E, Mitchell JC, Olesik JW, Brantley WA, Papazoglou E, Monaghan P. Inductively coupled plasma mass spectroscopy measurements of elemental release from 2 high palladium dental
casting alloys into a corrosion testing medium. J Prosthet Dent 2002;87:80-5.
47. Rashmi M, Chaturvedi TP. An overview of biocompatibility of orthodontic materials. J Indian
Orthod Soc 2008;3:27-32.
48. Wang J, Nianxing Li, Rao G, Han W. Stress corrosion cracking of NiTi in artificial saliva. Dent Mater
2007;23:133-7.
49. Lin M, Lin S, Lee T, Huang H. Surface analysis and corrosion resistance of different stainless steel
orthodontic brackets in artificial saliva. Angle Orthod 2006;76:23-7.
50. Matasa CG. Microbial attack of orthodontic adhesives. Am J Orthod Dentofac Orthop
1995;108:132-41.
51. Chaturvedi TP, Dubey RS, Upadhayay SN. Effect of Indian plant sticks on oral health. J Indian Dent
Assoc 2009;3:77-9.
52. Chang J, Oshida Y, Richard L, Carl J, Thomas M, David T. Electrochemical study on microbiology-
related corrosion of metallic dental materials Bio-Med Mat Engg 2003;13:281-95.
53. Maruthamuthu S, Rajasekar A, Sathiyanarayanan S, Muthukukumar N, Palaniswamy N.
Electrochemical behavior of microbes on orthodontic wires. Curr Sci 2005;89:988-96.
54. Huang HH. Effects of fluoride concentration and elastic tensile strain on the corrosion resistance of
commercially pure titanium. Biomaterials 2002;23:59-63.
55. Huang HH, Lee TH. Electrochemical impedence spectroscopy study of Ti-6Al-4V alloy in artificial

saliva with fluoride and /or albumin. Dent Mater 2005;21:749-55.
56. Oshida Y, Cory B, Sellers, Mirza K, Nia F. Corrosion of dental metallic materials by dental treatment
agents. J Mat Sci Engg 2005;25:343-8.
57. Mary P. Richard J, Katherene S. Effect of fluoride prophylactic agents on the mechanical properties of nickel-titanium-based orthodontic wires. Am J Orthod Dentofac Orthop 2005;127:662-
9.
58. Schiff N, Dalard F, Lissac M, Morgon L, Grosgogeat B. Corrosion resistance of three orthodontic brackets: A comparative study of three flouride mouthwashes. Eur J Orthod 2005;27:541-
9.
59. Huang HH. Effect of fluoride and albumin concentration on the corrosion behaviour of Ti-6Al-4V
alloy. Biomaterials 2003;24:275-82.
60. Nicolas S, Francis D, Michele L, Brigitte G. Influence of fluoridated mouthwashes on corrosion
resistance of orthodontics wires. Biomaterials 2004;25:4535-42.
61. Huang HH. Variation in surface topography of different NiTi orthodontic arch wires in various
commercial fluoride-containing environments. Dent Mater 2007;23:24-33.
62. Bass JK, Fine HF, Cisneros GJ. Nickel hypersensitivity in the orthodontic patient. Am J Orthod
Dentofac Orthop 1993;103:280-285.
63. Kerosuo H, Kullaa A, Kerosuo E, Kanerva L, Hensten-Pettersen A. Nickel allergy in adolescents in relation to orthodontic treatment and piercing of ears. Am J Orthod Dentofac Orthop
1996;109:148-54.
64. Park HY, Shearer TR. In vitro release of nickel and chromium from simulated orthodontic
appliances. Am J Orthod 1983;84:156-69.
65. Staffolini N, Damiani F, Lilli C, Guerra M, Staffolini NJ, Belcastro S, et al. Ion release from
orthodontic appliances. J Dent 1999;27:49-54.
66. Gjerdet NR, Erichsen ES, Remlo HE, Evjen G. Nickel and iron in saliva of patients with fixed

orthodontic appliances. Acta Odontol Scand 1991;49:73-8.
67.Rahilly G, Price N. Nickel allergy and orthodontics. J Orthod 2003;30:171-4.
68. Bishara SE, Barrett RD, Selim MI. Biodegradation of orthodontic appliances, Part II: Changes in the
blood level of nickel. Am J Orthod Dentofac Orthop 1993;103:115-9.
69. Gjerdet NR, Hero H. Metal release from heat treated orthjodontic wires. Actaodontol Scan
1987;45:409-14.
70. Kerosuo H, Moe G, Hensten-Pettersen A. Salivary nickel and chromium in subjects with different
types of fixed orthodontic appliances. Am J Orthod Dentofac Orthop 1997;111:595-8.
71. Hensten-Pettersen A. Nickel allergy and dental treatment procedures. In: Maibach HI, Menne T, editors. Nickel and the skin: Immunology and toxicology. Boca Raton, Fla: CRC Press; 1989. p. 195-205. van Hoogstraten IM, Andersen KE, Von Blomberg BM, Boden D, Bruynzeel DP, Burrows D, et al. Reduced frequency of nickel allergy upon oral nickel contact at an early age. Clin Exp Immunol
1991;85:441-5.
72. Lσpez-Alνas JF, Martinez-Gomis J, Anglada JM, Peraire M. Ion release from dental casting alloys as assessed by a continuous flow system: Nutritional and toxicology implications. Dent Mater
2006;22:832-7.
73. Lindsten R, Kurol J. Orthodontic appliances in relation to nickel hypersensitivity: A review. J Orofac
Orthop 1997;58:100-8.
74. Lee YW, Broday L, Costa M. Effects of nickel on DNA methyltransferase activity and genomic DNA
methylation levels. Mutat Res 1998;415:213-8.
75. Lee YW, Klein CB, Kargacin B, Salnikow K, Kitahara J, Dowjat K, et al. Carcinogenic nickel silences gene expression by chromatin condensation and DNA methylation: A new model for epigenetic
carcinogens. Mol Cell Biol 1995;15:2547-57.
76. Manaranche C, Hornberger H. A proposal for the classification of dental alloys according to their
resistance of corrosion. Dent Mater 2007;23:1428-37.
77. Cioffi M, Gilliland D, Ceccone G, Chiesa R, Cigada A. Electrochemical release testing of nickel-titanium orthodontic wires in artificial saliva using thin layer activation. Acta Biomater 2005;1:717-
24.
78. Yukyo T, Keisuke N, Kohei K, Osamu O. Corrosion behavior of the stainless steel composing dental
magnetic attachments. Int Congr Series 2005;1284:314-5.
Correspondence Address:T P ChaturvediDepartment of Orthodontics, Faculty of Dental Sciences, Institute of Medical Sciences, Varanasi, UP India
DOI: 10.4103/0970-9290.66648
PMID: 20657101





























