Embed Size (px)
Citation preview
Pulmonary Pulmonary Thromboembolic DiseaseThromboembolic Disease
ByBy
Ahmed Mansour, MSc, PhDAhmed Mansour, MSc, PhD
Definition
• PE is a clinically significant PE is a clinically significant obstruction of part or all of the obstruction of part or all of the pulmonary vascular tree (usually pulmonary vascular tree (usually caused by migrating thrombus from caused by migrating thrombus from a distant site;DVT).a distant site;DVT).
• VTE = PE + DVT VTE = PE + DVT
Natural History
• Death within 1 h 11%.Death within 1 h 11%.
• Survival > 1 h 89%Survival > 1 h 89%- Diagnosis made & ttt started 29%Diagnosis made & ttt started 29%
• Survive 92%Survive 92%
• Death 8%Death 8%
- Diagnosis not made 71%Diagnosis not made 71%• Survive 70%Survive 70%
• Death 30%Death 30%
Source of EmboliSource of Emboli
• Lower extremit (80-95%) especially if Lower extremit (80-95%) especially if popliteal or above.popliteal or above.
• Pelvic veins in cases of...Pelvic veins in cases of...
• Upper extremity...Upper extremity...
• Right ventricle, more hemodynamic Right ventricle, more hemodynamic instability and increased mortality.instability and increased mortality.
• Other materials...Other materials...
Presisposing FactorsPresisposing Factors
• Wirchow’s triad.Wirchow’s triad.
• Acquired risk factorsAcquired risk factors
• Inherited thrombophiliasInherited thrombophilias1- Factor V Leiden mutation (APC resistance)1- Factor V Leiden mutation (APC resistance)
2- Prothrombin gene mutation 2- Prothrombin gene mutation
3- Deficienecy of antithrombin III, protein C, protein S.3- Deficienecy of antithrombin III, protein C, protein S.
Major:Major:
1- Surgery1- Surgery
2- Obstetrics2- Obstetrics
3- Malignancy3- Malignancy
4- LL problems4- LL problems
5- Immobility5- Immobility
6- Previous VTE6- Previous VTE
Minor:Minor:
1- Cardiovascular1- Cardiovascular
2- HRT, contraceptives2- HRT, contraceptives
3- Others: obesity, nephrotic 3- Others: obesity, nephrotic syndrome,…syndrome,…
PathophysiologyPathophysiology
• Factors determining the outcome:Factors determining the outcome:1- Size and location of emboli1- Size and location of emboli
2- Coexisiting cardiopulmonary diseases2- Coexisiting cardiopulmonary diseases
3- Secondary humoral mediator release 3- Secondary humoral mediator release and vascular hypoxic responsesand vascular hypoxic responses
4- Resolution rate of emboli 4- Resolution rate of emboli
Haemodynamic consequences Haemodynamic consequences of acute PEof acute PE
1- PAP rises.1- PAP rises.2- RV after-load increases.2- RV after-load increases.3- RV failure if > 50% of pulmonary 3- RV failure if > 50% of pulmonary
vascular bed is obstructedvascular bed is obstructed4- LV filling is reduced…hypotension.4- LV filling is reduced…hypotension.5- Increased RA pressure may lead to 5- Increased RA pressure may lead to
intraccardiac shunt through a patent intraccardiac shunt through a patent foramen ovale.foramen ovale.
Gas-Exchange Gas-Exchange AbnormalitiesAbnormalities
• HypoxemiaHypoxemia::1- Re-direction of blood flow to other parts 1- Re-direction of blood flow to other parts
of pulmonary vascular bed (V/Q of pulmonary vascular bed (V/Q mismatch)mismatch)
2- Increased alveolar dead space due to 2- Increased alveolar dead space due to atelectasis and bronchiolar constriction.atelectasis and bronchiolar constriction.
• HypocapneaHypocapnea due to hyperventilation due to hyperventilation
Clinical features of acute Clinical features of acute PEPE
1- Pulmonary infarction and hemoptysis 1- Pulmonary infarction and hemoptysis ± pleuritic pain (60%):± pleuritic pain (60%):- Acute pleuretic chest pain and hemoptysis Acute pleuretic chest pain and hemoptysis - O/E: local signs e.g. pleura;l rubO/E: local signs e.g. pleura;l rub- ABGs and ECG are usually normalABGs and ECG are usually normal
2- Isolated dyspnea (25%):2- Isolated dyspnea (25%):- Acute SOB in presence of a risk facto for VTEAcute SOB in presence of a risk facto for VTE- O/E: patient is hemodynamically stableO/E: patient is hemodynamically stable- ABGs show hypoxemia, CTPA: central thrombusABGs show hypoxemia, CTPA: central thrombus
3- Circulatory collapse, poor reserve (10%):3- Circulatory collapse, poor reserve (10%):- Usually in elderly patients with cardiopulmonary diseases Usually in elderly patients with cardiopulmonary diseases - Rapid decompensation even with small PERapid decompensation even with small PE- O/E: features of the underlying diseases. O/E: features of the underlying diseases.
4- Circulatory collapse in a previously well patient (1%):4- Circulatory collapse in a previously well patient (1%):- Acute chest pain (RV angina), hemodynamic instability due to massive Acute chest pain (RV angina), hemodynamic instability due to massive
PEPE- O/E: RV failure...O/E: RV failure...- ECG changes, echocardiography shows RV failureECG changes, echocardiography shows RV failure
Clinical features of chronic Clinical features of chronic PEPE
• Insidious onsetInsidious onset over weeks to months due over weeks to months due to recurrent showers of small emboli.to recurrent showers of small emboli.
• Dyspnea and tachypneaDyspnea and tachypnea are the are the commonest features (90%).commonest features (90%).
• Should be considered in the DD of:Should be considered in the DD of:- Unexplained SOBUnexplained SOB- RVFRVF- New AFNew AF- Pleural effusionPleural effusion- CollapseCollapse

ExaminationExamination
1- May be normal1- May be normal2- Vital signs:2- Vital signs:
tachypnea, tachycardia (may be AF), low grade fever. tachypnea, tachycardia (may be AF), low grade fever. 3- Heart:3- Heart:
Signs of pulmonary hypertension (loud splitted S2)Signs of pulmonary hypertension (loud splitted S2)Signs of RV failure (raised JVP, low COP with systemic hypotension, Signs of RV failure (raised JVP, low COP with systemic hypotension,
tricuspid gallop)tricuspid gallop)4- Chest; 4- Chest; the affected side may showthe affected side may show::
Inspection: reduced movementInspection: reduced movementPalpation: diminished expansionPalpation: diminished expansionPercussion: dullness in case of pleural effusionPercussion: dullness in case of pleural effusionAuscultation: pleural rub (Pulmonary infarction ) or diminished intensity of Auscultation: pleural rub (Pulmonary infarction ) or diminished intensity of
breath sounds (pleural effusion)breath sounds (pleural effusion)5- Lower limbs:5- Lower limbs:
Signs of DVT.Signs of DVT.
Diagnosis of Acute PEDiagnosis of Acute PE
• Pre-test clinical probability scoring:Pre-test clinical probability scoring:
- e.g. BTS scoring system:e.g. BTS scoring system:a- Clinical features consistent with PEa- Clinical features consistent with PE
1- Absence of other reasonable clinical explanation1- Absence of other reasonable clinical explanation
2- Presence of a major risk factor2- Presence of a major risk factor
High probability: a+1+2High probability: a+1+2
Intermediate probability: a+ either 1 or 2Intermediate probability: a+ either 1 or 2
Low probability: a onlyLow probability: a only
Diagnosis of Acute PEDiagnosis of Acute PE
• D-dimer:D-dimer:- A fibrinolysis productA fibrinolysis product generated in many clinical situations generated in many clinical situations
e.g...e.g...- Indicated in:Indicated in:
1- Low/intermediate clinical probability1- Low/intermediate clinical probability2- Acute cases only2- Acute cases only3- Outpatient cases only3- Outpatient cases only
- SensitiveSensitive (small no. Of false negatives) but (small no. Of false negatives) but not specificnot specific (large no. Of false positives).(large no. Of false positives).
- Interpretation of the results:Interpretation of the results:* Normal level = negative test, elevated level = positive test* Normal level = negative test, elevated level = positive test* A negative test is valid to exclude PE in cases with * A negative test is valid to exclude PE in cases with
low/intermediate clinical probability. A positive test does not low/intermediate clinical probability. A positive test does not cofirm PE but rather further imaging is requiredcofirm PE but rather further imaging is required
InvestigationsInvestigations
1- ECG1- ECG
2- CXR2- CXR
3- ABGs3- ABGs
4- D-dimer4- D-dimer
5- Troponin and natriuretic peptides5- Troponin and natriuretic peptides
5- CTPA5- CTPA
6- Ventilation/perfusion lung scan6- Ventilation/perfusion lung scan
7- Others7- Others
ECGECG
• Sinus tachycardiaSinus tachycardia
• AF AF
• RBBBRBBB
• RV starinRV starin
• Less commonly; S1Q3T3Less commonly; S1Q3T3
CXRCXR
• Small pleural effusionSmall pleural effusion
• Raised hemi-diaphragmRaised hemi-diaphragm
• CollapseCollapse
• InfiltrateInfiltrate
ABGsABGs
• May be normalMay be normal
• Hypoxemia and hypocapneaHypoxemia and hypocapnea
• Increased A-a oxygen gradientIncreased A-a oxygen gradient
Troponin and natriuretic Troponin and natriuretic peptidespeptides
• Indicate RVDIndicate RVD
• Raised troponin predicts poor Raised troponin predicts poor prognosisprognosis
CTPACTPA
• The gold standard investigationThe gold standard investigation• Highly sensitive (multi-detector scanners)Highly sensitive (multi-detector scanners)• More sensitive for central emboliMore sensitive for central emboli• More helpful for patients with abnormal More helpful for patients with abnormal
CXRCXR• Negative CTPA:Negative CTPA:
- In those with low/intermediate clinical In those with low/intermediate clinical probability: PE is unlikely.probability: PE is unlikely.
- In those with high clinical probablity: further In those with high clinical probablity: further investigations are required.investigations are required.
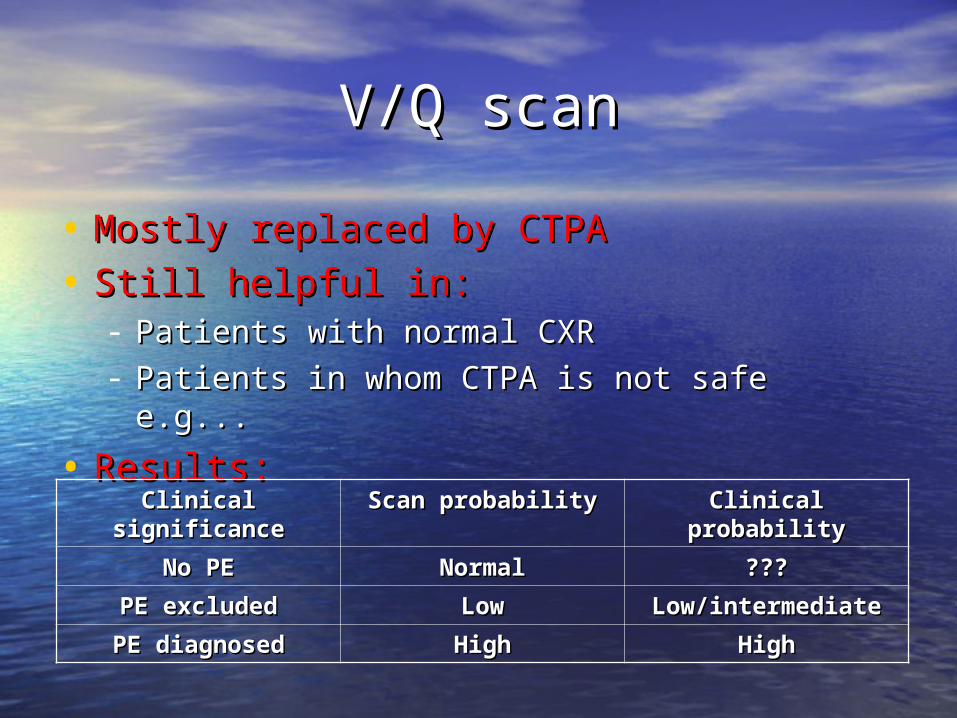
V/Q scanV/Q scan
• Mostly replaced by CTPAMostly replaced by CTPA
• Still helpful in:Still helpful in:- Patients with normal CXRPatients with normal CXR- Patients in whom CTPA is not safe e.g...Patients in whom CTPA is not safe e.g...
• Results:Results:
Clinical probabilityClinical probabilityScan probabilityScan probabilityClinical Clinical significancesignificance
??????NormalNormalNo PENo PE
Low/intermediateLow/intermediateLowLowPE excludedPE excluded
HighHighHighHighPE diagnosedPE diagnosed
Other imaging techniquesOther imaging techniques
• EchocardiographyEchocardiography
• Leg U/SLeg U/S
• CT venographyCT venography
• Transthoracic U/STransthoracic U/S
• Conventional pulmonary angiographyConventional pulmonary angiography
Management of acute massive Management of acute massive PEPE1- 1- 100% O100% O22
2- IV access, baseline clotting screen, ECG2- IV access, baseline clotting screen, ECG3- Analgesia3- Analgesia4- Management of cardiogenic shock4- Management of cardiogenic shock5- IV heparin: 5- IV heparin:
– Unfractionated vs LMWHUnfractionated vs LMWH– Loading, maintenanceLoading, maintenance– APTTAPTT
6- 6- Investigations to confirm PE? Investigations to confirm PE? 7- Thrombolysis 7- Thrombolysis for massive PE causing hemodynamic instablityfor massive PE causing hemodynamic instablity8- Embolectomy 8- Embolectomy in patients with a contraindication for anticoagulants or thrombolyticsin patients with a contraindication for anticoagulants or thrombolytics 9- Oral anticoagulants9- Oral anticoagulants
- OutpatientOutpatient- INRINR- For how long?For how long?
10- 10- IVC filter IVC filter for patients withfor patients with:: - A contraindication for anticoagulantsA contraindication for anticoagulants- Massive PE after survivalMassive PE after survival- Reccurrent VTE despite adequate anticoagulation Reccurrent VTE despite adequate anticoagulation
Thank you