Embed Size (px)
Citation preview

IDtht3tamtis3
ipddpdaVdnpbmbcptg
C0d
8
Thromboembolic Diseases
ncidence, Risk Factors, and Categorieseep venous thrombosis (DVT) and pulmonary embolism (PE),
ogether called venous thromboembolism (VTE), remain a seriousealth care problem. Together it has been estimated that there are morehan 900,000 cases per year in this country alone.1 Approximately00,000 individuals die of PE every year and deaths from PE are 5imes more common than deaths from breast cancer, motor vehicleccidents, and AIDS combined. Venous thromboembolism is the thirdost common vascular disease after heart disease and stroke. Addi-
ionally, patients with post-thrombotic syndrome (pain and leg swell-ng after thrombosis) suffer poor quality of life due to chronicymptoms. The incidence of post-thrombotic syndrome is as high as0% over 8 years.2
Acquired risk factors include age, malignancy, surgery and trauma,mmobilization, oral contraceptive use, hormone replacement therapy,regnancy and the puerperium, obesity, neurological disease, cardiacisease, and antiphospholipid antibodies.3 Genetic causes includeeficiencies of antithrombin, proteins C and S, factor V Leiden,rothrombin 20210A, blood group non-O, hyperhomocystinemia,ysfibrinogenemia, dysplasminogenemia, reduced heparin cofactor IIctivity, elevated levels of clotting factors such as factors XI, IX, VII,III, X, and II, and plasminogen activator inhibitor-1.4 Hematologiciseases associated with an increased risk of DVT include dissemi-ated intravascular coagulation (DIC), heparin-induced thrombocyto-enia (HIT), antiphospholipid antibody syndrome, thrombotic throm-ocytopenic purpura (TTP), hemolytic uremic syndrome (HUS), andyeloproliferative disorders (polycythemia vera and essential throm-
ocythemia).5 For venous thrombosis, indications for screening in-lude venous thrombosis in unusual locations (ie, mesenteric venous,ortal venous, etc), idiopathic venous thrombosis, recurrent venoushrombosis, thrombosis on oral contraceptives, and episodes of ag-
ressive superficial thrombophlebitis.urr Probl Surg 2008;45:844-899.011-3840/2008/$34.00 � 0oi:10.1067/j.cpsurg.2008.08.002
44 Curr Probl Surg, December 2008

V
eispbTnrbkgtpaAtb
V
D
t
Ftt(
C
enous Thrombosis PathogenesisThrombosis in the venous circulation involves a combination of stasis,
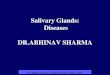
ndothelial perturbations, and hypercoagulabilities. The inciting eventnvolves thrombus formation from local procoagulant events, such asmall endothelial disruptions at venous confluences, saccules, and valveockets. Neutrophils and platelets then adhere to this thrombus andecome activated, generating inflammatory and procoagulant mediators.hrombus is thus amplified.6 With progression, leukocytes (initiallyeutrophils and later monocytes) extravasate into the vein wall ultimatelyesulting in vein wall inflammation (Fig 1). It appears that a balanceetween proinflammatory and anti-inflammatory cytokines and chemo-ines determine the ultimate vein wall response.7 The earliest elevatedlycoprotein present on endothelial cells and platelets, P-selectin appearso play an important role in thrombogenesis along with the generation ofrocoagulant microparticles.8,9 These microparticles are tissue factor richnd are released from activated leukocytes, platelets, and endothelium.dditionally, tissue factor released from the vein wall also contributes to
hrombosis when direct vein wall injury occurs or when tissue factorecomes exposed to the flowing blood.10
enous Disease Diagnosis
eep Venous ThrombosisThe diagnosis of DVT must be made with confirmatory laboratory
IG 1. Immediately after endothelial cell injury, endothelial cells and platelets are activated promotinghe expression of cell adhesion molecules. This vascular response promotes leukocytes rolling andethering onto the endothelium that initiates an inflammatory event which can lead to thrombosis.Reprinted with permission from Wakefield et al,7 © 2008 Lippincott Williams & Wilkins.)
esting, as patients will be asymptomatic at presentation in up to 50% of
urr Probl Surg, December 2008 845

caestaltbsaid
scavTViggpamt
itaafistMptwtd
8
ases with DVT. When symptoms are present, patients complain of a dullche or pain in the calf or leg. The most common physical finding isdema, although Wells and colleagues have classified patients into acoring system that emphasizes the physical presentation of patients. Inheir criteria, characteristics that score points include the presence ofctive cancer, paralysis or paresis, recent plaster immobilization of theower extremity, being recently bedridden for 3 days or more, localizedenderness along the distribution of the deep venous system, the entire legeing swollen, calf swelling that is at least 3 cm larger on the involvedide compared with the noninvolved side, pitting edema in the symptom-tic leg, and a history of a previous DVT.11 With extensive proximal DVTn the iliofemoral system, there may be significant swelling, cyanosis, andilated superficial collateral veins.Massive iliofemoral DVT may cause phlegmasia alba dolens (white
wollen leg) or phlegmasia cerulean dolens (blue swollen leg). When theapillaries occlude, venous gangrene may occur. This occurs as therterial inflow becomes obstructed due to the effects of high levels ofenous hypertension. Alternatively, arterial emboli or spasm may occur.he skin blisters and the toes on the involved limb may turn black.enous gangrene must be differentiated from gangrene caused by arterial
nsufficiency. Such differentiation includes the fact that with arterialangrene the limb is pale and cold without significant swelling. Venousangrene is often associated with an underlying malignancy and is alwaysreceded by phlegmasia cerulea dolens. Associated with venous gangrenere amputation rates of 20% to 50%, PE rates of 12% to 40%, andortality rates of 20% to 40% due to the underlying medical conditions
hat have been described.12
Tests for establishing the diagnosis of DVT of historical interest includendirect flow examinations. Duplex ultrasound imaging has replaced theseests and also contrast phlebography due to its high sensitivity, specificity,nd reproducibility. Duplex ultrasound imaging includes a B-mode imagend Doppler flow pattern. Duplex imaging carries sensitivity and speci-city rates greater than 95%.13 According to the grade criteria for thetrength of medical evidence, duplex ultrasound as the test of choice forhe diagnosis of DVT is given a 2C level of evidence13-15 (Table 1).
agnetic resonance imaging (MRI) may be helpful to diagnose centralelvic vein and inferior vena cava (IVC) thrombosis, and spiral computedomography (CT) scanning is also being used more frequently, especiallyhen combined with chest imaging during examination for PE.16 Even at
he calf level, a level in which duplex imaging is felt to be less accurate,
uplex imaging is an acceptable technique in symptomatic patients. Other46 Curr Probl Surg, December 2008

acaac
tcwbhikiAraiabbc
mlp
Tb
DSLCAUNC
Dmh
C
dvantages of duplex imaging include that it is painless, requires noontrast, can be repeated serially, and is safe during pregnancy. This testlso identifies other potential causes of a patient’s symptoms.14 In thesymptomatic patient, screening venous duplex imaging has been asso-iated with varying levels of sensitivity and specificity.Combining clinical characteristics with a D-dimer assay may decrease
he number of negative duplex scans performed.11 Importantly, a singleomplete technically adequate negative duplex scan is accurate enough toithhold anticoagulation with minimal long-term adverse thromboem-olic complications.17 However, this means that all segments of the legave been imaged and evaluated successfully. If the duplex scan isndeterminate, treatment may be based on other factors such as biomar-ers, with the duplex scan repeated in 24 to 72 hours. Also, repeatmaging may be necessary if the patient’s symptoms change or worsen.lthough the use of clinical characteristics and D-dimer levels is useful to
ule out thrombosis, the converse is not true. A positive D-dimerssociation with a positive risk assessment is associated with thrombosisn only approximately 70% of cases, and is not felt good enough to basenticoagulant therapy on.18 We are attempting to establish a panel ofiomarkers that may be used to establish a positive diagnosis of DVTased on the inflammatory response to the thrombotic process and theross-talk between systems.19
Other conditions may be confused with DVT including lymphedema,uscle strain, and contusion. Iliac vein obstruction in the retroperitoneum
eads to unilateral massive leg edema (May-Thurner syndrome), while the
ABLE 1. Evidence-based recommendations for the diagnosis and treatment of venous thromboem-olism15
Test or interventionLevel of evidence(grade criteria)
uplex imaging for DVT diagnosis 2Cpiral CT imaging for PE diagnosis 1AMWH for initial treatment of VTE 1Ariteria for stopping anticoagulation 1Alternative agents for treatment of HIT 1C/2Cse of IVC filters 2Conpharmacological treatment for DVT 1Aombined pharmacological and mechanical VTE prophylaxis 2A
VT, deep vein thrombosis; CT, computed tomography; PE, pulmonary embolism; LMWH, lowolecular weight heparin; VTE, venous thromboembolism; IVC, inferior vena cava; HIT,eparin-induced thrombocytopenia.
resence of a cyst behind the knee may produce unilateral leg pain and
urr Probl Surg, December 2008 847

ep
P
parishd8rVHaidpqmt
laaiccatscaci1fr
8
dema. Other causes of leg swelling (usually bilateral) include systemicroblems such as cardiac, renal, or hepatic abnormalities.
ulmonary EmbolismThe diagnosis of PE involves ventilation-perfusion (V/Q) scanning orulmonary angiography; newer techniques include spiral CT scanningnd MRI. The sensitivity of V/Q scanning is described in a largeandomized multicenter study (PIOPED I) to be 98%, but the specificitys low, at 10%.20 By combining clinical risk factors with V/Q scan,ensitivity and specificity greater than 95% was achieved. With aigh-probability V/Q scan and 2 risk factors for PE, the sensitivity for PEiagnosis was 97%; with 1 risk factor, 84%; and with no risk factors,2%. Similarly, with a normal V/Q scan, the chance of PE was zero,egardless of the risk factor status.21 These results suggest that a normal/Q scan or a high-probability scan provide good diagnostic information.owever, only a small portion of V/Q scans are in 1 of these 2 categories,
nd thus the majority of patients need further testing. Such further testingncludes lower extremity venous duplex ultrasound imaging (venousuplex imaging is positive in approximately 10% of cases in theseatients) and spiral CT scanning. Pulmonary angiography is used infre-uently today. Indications for pulmonary arteriography include acuteassive PE, IVC interruption, and the planning of pulmonary interven-
ional therapy, such as thrombolysis or pulmonary embolectomy.Spiral CT scanning has demonstrated excellent specificity but relatively
ow sensitivity (50% to 65%), despite promising initial results. However,s the technology has improved, the sensitivity and specificity havelso improved, and now emboli at the subsegmental level can bedentified.22 A recent study reported that the sensitivity for isolatedhest CT imaging was 83%, but increased to more than 90% whenlinical analysis was added. Additionally, sensitivity improved whendding a lower extremity imaging study (either CT or ultrasound) tohe chest CT scan.16 Results from this study (PIOPED II) stronglyuggest that if the clinical presentation and spiral CT scan areoncordant, therapies can be recommended safely. However, if resultsre discordant between clinical presentation and spiral CT, then otheronfirmatory tests are necessary. For the diagnosis of PE, spiral CTmaging is given a 1A level of evidence based on PIOPED II (Table). Magnetic resonance imaging has demonstrated excellent promiseor PE diagnosis and is currently being investigated in a multicenter
andomized study (PIOPED III).48 Curr Probl Surg, December 2008

A
atdosatacsaadc
wmpiaape
S
rti6Afpp
bvn
C
xillary/Subclavian Vein ThrombosisThrombosis of the axillary/subclavian vein accounts for less than 5% of
ll cases of acute DVT. However, it is associated with PE in up to 10%o 15% of cases and additionally can be the source of significantisability.23 Primary axillary/subclavian vein thrombosis results frombstruction of the vein in the thoracic outlet, the Paget Schrotteryndrome, especially prominent in healthy muscular individuals. It maylso occur in patients with hypercoagulable states who have a tendency tohrombosis. Secondary axillary/subclavian vein thrombosis results usu-lly from indwelling catheters or pacemaker wires. Other less commonauses include mediastinal tumors, malignancy, and medical conditionsuch as congestive heart failure and nephrotic syndrome. Patients withxillary-subclavian venous thrombosis often present with pain, edema,nd cyanosis of the arm. Due to the venous obstruction, superficial venousistension may be apparent over the arm, forearm, shoulder, and anteriorhest wall.Upper extremity venous duplex ultrasound is used for those patientsith suspected axillary-subclavian vein thrombosis. Treatment for docu-ented thrombotic episodes includes anticoagulation. Thrombolysis and
hlebography should be considered. If phlebography is performed, it ismportant that the patient undergo positional phlebography, abducting therm 120 degrees to confirm extrinsic compression of the subclavian veint the thoracic outlet. Venous compromise is further evidenced byrominent collateral veins. A chest radiograph should be obtained toxclude the presence of a cervical rib.
tandard Therapy for VTEThe primary treatment of VTE is systemic anticoagulation, which
educes the risk of PE, extension of thrombosis, and recurrence ofhrombosis. Immediate systemic anticoagulation should be undertaken, ast has been shown that the recurrence rate for VTE is approximately 4- to-fold higher if anticoagulation is not therapeutic in the first 24 hours.24
dequate anticoagulation has been shown to prevent the development ofatal PE both during the initial treatment and after treatment is com-lete.25 However, recurrent DVT may still occur in up to one third ofatients over an 8-year period after adequate appropriate therapy.26
Traditionally, systemic intravenous unfractionated heparin (UFH) haseen undertaken for 5 days, during which time oral anticoagulation withitamin K antagonists (usually warfarin) is instituted. International
ormalized ratios (INRs) therapeutic for 2 consecutive days are usuallyurr Probl Surg, December 2008 849

ritbhhaibwrTuacwmmosmLTs1
ptocfbattylVpml
8
ecommended before stopping heparin.27 However, due to the need forntravenous administration, the need for frequent monitoring, as well ashe bleeding risks of UFH, low molecular weight heparin (LMWH) haseen advanced as primary therapy for VTE. Low molecular weighteparins are derived from the lower molecular weight range of standardeparin. They demonstrate less direct thrombin inhibition and morentifactor Xa inhibition. Low molecular weight heparins have significantmprovement in bioavailability and less endothelial cell and proteininding compared with standard unfractionated heparin. Low moleculareight heparins are at least equivalent to UFH if not slightly superior
egarding thrombus recurrence, with a lower risk for major hemorrhage.28
he list of potential advantages of LMWHs compared with standardnfractionated heparin include a lower risk of bleeding, less antiplateletctivity, a lower incidence of HIT, less interference with protein C andomplement activation, and a lower risk of osteoporosis. Low moleculareight heparins may be administered subcutaneously weight based, anday be administered in the outpatient setting. They do not requireonitoring except in certain circumstances such as renal failure, morbid
besity, and during pregnancy.29 However, the use in the outpatientettings usually requires a team approach and a coordinated effort ofultiple health care providers. There is also mounting evidence thatMWH may decrease the incidence of post-thrombotic syndrome.30
aking all of the evidence together, LMWH is now preferred overtandard UFH for the initial treatment of VTE with a level of evidenceA31 (Table 1).Warfarin should be started only after heparinization is therapeutic torevent warfarin-induced skin necrosis, usually on the first day ofherapy. This condition occurs due to transient hypercoagulability thatccurs for the first few days after warfarin is administered. Warfarinauses inhibition of protein C and protein S before most coagulationactors are inhibited by warfarin. The goal for warfarin dosing is an INRetween 2.0 and 3.0. The recommended duration of anticoagulation afterfirst episode of VTE is 3 to 6 months.32 Calf level thrombi may be
reated with 6 to 12 weeks of warfarin. After a second episode of VTE,he usual recommendation is prolonged warfarin unless the patient is veryoung at the time of presentation or there are other mitigating factors. Theength of time of warfarin usage in other situations is controversial.enous thromboembolism recurrence is increased significantly in theresence of homozygous factor V Leiden and prothrombin 20210Autation, protein C/S deficiency, antithrombin deficiency, antiphospho-
ipid antibodies, and cancer until resolved.3 In these conditions, most
50 Curr Probl Surg, December 2008

ampc
acccbbacl
iafprw(aitacT
UWbPbhua
ttd
C
gree with long-term warfarin therapy especially in circumstances withultiple hypercoagulable states. However, heterozygous factor V Leiden/
rothrombin 20210A does not carry the same risk as their homozygousounterparts, and the length of oral anticoagulation is shortened.Recently, 2 additional criteria have been used to determine the length of
nticoagulation. One involves the amount of scar tissue inside the venousirculation leading to stasis. The second and perhaps better validatedriterion involves D-dimer testing obtained 1 month after warfarin isompleted. If the D-dimer level is elevated above normal, warfarin shoulde continued, as this result suggests that the patient is still prothrom-otic.33-35 One recent study has demonstrated a statistically significantdvantage to resuming coumadin if the D-dimer assay is positiveompared with remaining off coumadin over an average 1.4-year fol-ow-up period (odds ratio [OR] 4.26, P � 0.02).36
Idiopathic DVT is an interesting problem. Most believe that truediopathic thrombosis requires more than 6 months of warfarin, but thectual length is not known. A recent multicenter trial has suggested thator idiopathic DVT, low dose warfarin (INR 1.5-2.0) is superior tolacebo over a 4-year follow-up period with a 64% risk reduction forecurrent DVT after the completion of an initial 6 months of standardarfarin therapy.37 A second study has suggested that full-dose warfarin
INR 2-3) is superior to low-dose warfarin in these same patients withoutdifference in bleeding.38 Thus, the data together suggest that for
diopathic thrombosis, long-term treatment is desirable and an INR of 2.0o 3.0 should be achieved. In aggregate, criteria for discontinuation of oralnticoagulation include thrombosis risk, residual thrombus burden, andoagulation system activation (as suggested by D-dimer measurements).hese criteria are given a level of evidence of 1A33-35,37,38 (Table 1).The most common complication of anticoagulation is bleeding. WithFH, bleeding occurs in approximately 10% of cases over the first 5 days.ith the addition of warfarin at an INR of 2 to 3, the incidence of major
leeding is approximately 6% per year. In treating patients for DVT andE, major bleeding has been reported in 0% to 7% of patients, with fatalleeding in 0% to 2% of patients.39 A meta-analysis showed a rate ofemorrhagic complications estimated at 9.1% for anticoagulation contin-ed beyond 3 months. To decrease bleeding, dose adjustments and use ofnticoagulation clinics are emphasized.Another complication of heparin is HIT. Heparin-induced thrombocy-
openia occurs in 0.6% to 30% of patients in whom heparin is adminis-ered. While historically morbidity and mortality have been high, early
iagnosis and appropriate treatment have decreased the rates.40 Heparin-urr Probl Surg, December 2008 851

ibipBwt(secttdstEtatrsinba
SH
oacApwhpi
b
8
nduced thrombocytopenia usually begins 3 to 14 days after heparin isegun (earlier if the patient has been exposed to heparin in the past) ands caused by a heparin-dependent antibody immunoglobulin that binds tolatelets, activates them, and leads to an increase in thrombocytopenia.41
oth bovine and porcine UFH as well as LMWH have been associatedith HIT, although the incidence with LMWH is less. Arterial and venous
hromboses have been reported, and even small exposures to heparinheparin coating on indwelling catheters) has been known to cause theyndrome. The diagnosis should be suspected in a patient who experi-nces a 50% or more drop in platelet count, when there is a fall in plateletount below 100,000/�L during heparin therapy, or in the presence ofhrombosis during heparin administration.42 The test of choice for makinghis diagnosis is an enzyme-linked immunosorbent assay (ELISA) thatetects the antiheparin antibody in the patient’s plasma. This test is highlyensitive but poorly specific. The serotonin release assay is another testhat can be used, but this test is more specific but less sensitive than theLISA test.43 Cessation of heparin is the most important step in
reatment. Warfarin is contraindicated in this condition until an adequatelternative anticoagulant has been established, to prevent paradoxicalhrombosis. Low molecular weight heparins demonstrate high cross-eactivity with standard heparin antibodies and therefore cannot beubstituted for standard heparin in patients with HIT. The direct thrombinnhibitors hirudin (Lepirudin/Refludan) and argatroban are the treatmentsow approved by FDA, although other agents such as fondaparinux haveeen found to treat this syndrome as well.44,45 The use of these alternativegents is given a 2C and 1C level of evidence42,44,45 (Table 1).
pecial Features of Low Molecular WeighteparinThe safety of LMWH compared with warfarin has led to a considerationf the long-term use of LMWH as a replacement for oral vitamin Kntagonists. Rates of recanalization have been reported to be higher inertain venous segments using LMWH versus traditional oral agents.dditionally the use of LMWH has been found to be improved in canceratients compared with standard heparin or LMWH/warfarin therapyhen used for 6 months without differences in major bleeding.46 Theyave also been found to provide better DVT prophylaxis compared withlacebo for extended 4-week prophylaxis in patients undergoing abdom-nal/pelvic cancer surgery.47
The use of once daily compared with twice daily LMWH dosing has
een assessed in a meta-analysis. Considering more than 1500 patients52 Curr Probl Surg, December 2008

wrmst
A
diwtwdtpem
tIh(
T
TRPBT
HF
D
RSA
R
C
ith VTE, there was a nonsignificant difference in the incidence ofecurrent thromboembolism, thrombosis size, hemorrhagic events, andortality.48 However, there may be instances when twice daily dosing is
till more appropriate. These include patients with marked obesity andhose with cancer.49
lternative/Future Medical Treatments for DVT/PETwo new classes of agents for venous thrombosis treatment includeirect thrombin inhibitors and specific factor Xa inhibitors. Ximelagatrans a direct thrombin inhibitor and showed great promise to replacearfarin. However, ximelagatran caused an elevation in liver function
ests in up to 6% of patients administered the drug and because of this itas not approved in either the United States or Europe. A relative of thisrug, dabigatran etexilate, is currently undergoing phase III studies in thereatment of VTE, and has met a noninflammatory target to enaxoparin inrophylaxis for orthopedic procedures without any elevation in livernzymes or acute coronary events50 (Table 2). Other drugs with similarechanisms of action are currently being evaluated.Fondaparinux and its relative idraparinux are most like LMWH. They
arget factor Xa without inhibiting thrombin by potentiating antithrombinII. These drugs are administered subcutaneously and demonstrate aalf-life of 17 hours for fondaparinux and 80 to 130 hours for idraparinux
ABLE 2. Comparison of properties of rivaroxaban, apixaban, and dabigatran etexilate
Property Rivaroxaban ApixabanDabigatranetexilate
arget Factor Xa Factor Xa Thrombinoute of administration Oral Oral Oralrodrug No No Yesioavailability, % �80 �50 6ime to peak druglevel, h
3 3 2
alf-life, h 9 9-14 14-17requency ofadministration
Once daily Twice daily Once or twice daily
rug interactions Potent CYP3A4 andP-glycoproteininhibitors
Potent CYP3A4 andP-glycoproteininhibitors
Proton pumpinhibitors
enal excretion, % 66 25 80afe in pregnancy No No Nontidote No No No
eprinted with permission from Gross and Weitz,50 © 2008 Lippincott Williams & Wilkins.
compared with 4 hours for LMWH). These agents exhibit no endothelial
urr Probl Surg, December 2008 853

ottmf1cithispmctthprtaaiac
aRribD
oasibaa
8
r protein binding. However, no antidote is readily available. Neither ofhese drugs produces thrombocytopenia. Fondaparinux has been tested forhe prophylaxis of major orthopedic surgery. In a meta-analysis involvingore than 7000 patients, there was greater than 50% risk reduction using
ondaparinux begun 6 hours after surgery compared with LMWH begun2 to 24 hours after surgery.51 Although major bleeding was increased,ritical bleeding was not different. Fondaparinux has also been effectiven prophylaxis of general medical patients,52 abdominal surgery pa-ients,53 and for extended prophylaxis after hip fracture.54 Fondaparinuxas also been evaluated in the treatment of both DVT and PE. For DVTt was found equal to LMWH,55 while for PE it was found equal totandard UFH.56 This drug is administered based on body weight: 5 mger body weight �50 kg, 7.5 mg per body weight 50 to 100 kg, and 10g per body weight �100 kg. Treatment at least for 5 days with
oncurrent administration of oral anticoagulation is recommended, untilhe INR is therapeutic at a level of 2 to 3. It has been approved for thereatment of DVT/PE, thrombosis prophylaxis in total hip, total knee, andip fracture patients, and in the extended prophylaxis of hip fractureatients. Idraparinux with the longer half-life in an open label, noninfe-iority trial of 2904 DVT patients and 2215 PE patients was found to meethe noninferiority requirement of DVT, but not for PE.57 Additionally, instudy of long-term treatment in DVT/PE patients, major bleeding wassignificant problem with 3 intracranial bleeding episodes noted.57 Thus
draparinux development has been halted. However, in an attempt to developn antidote, idraparinux is being biotinylated (reversal with avidin) in a drugalled SSR 126517. Phase III trials are currently under way.58
New oral antifactor Xa agents are being developed. Rivaroxaban andpixaban are the 2 agents furthest along in development (Table 2).ivaroxaban has 66% renal excretion, whereas apixaban has only 25%
enal excretion.50,59 Rivaroxaban is in phase II trials showing good resultsn the treatment of DVT regarding symptomatic recurrences and throm-us burden,59 while apixoban is in phase II trials of patients with proximalVT and also phase III trials.50,59
Other antithrombotic agents are being evaluated including oral heparins,ther direct thrombin inhibitors such as lepirudin, bivalirudin, andrgatroban; difibrinating agents such as ancrod; anti-inflammatory agentsuch as P-selectin inhibitors; factor VIIa inhibitors; tissue factor pathwaynhibitor; and activated protein C.60,61 Lepirudin and argatroban haveeen approved for patients with HIT. The use of P-selectin inhibitors is anrea of ongoing research in our laboratory. Such an anti-inflammatory
pproach uses an antithrombotic agent that does not cause direct antico-54 Curr Probl Surg, December 2008

ap
I
tatpiwfio(i
acipnmhireoifte
N
aAPsts
C
gulant activities and thus the possibility of an agent without bleedingotential.
VC FiltersThe primary indications for the use of IVC filters includes a complica-
ion of anticoagulation, a contraindication to the use of anticoagulation,nd/or failure of that anticoagulation. Protection from PE has been greaterhan 95% using cone-shaped wire-based permanent IVC filters over theast 30 years.62 The success achieved with filters has expanded thendications. These include a free-floating thrombus longer than 5 cm,63
hen anticoagulation risk is excessive (ie, older patient with DVT orollowing major trauma),64 when the risk of PE is felt to be very high (asn certain bone and gastric bypass operations),65 and to allow for the usef perioperative epidural anesthesia. Filters can be permanent or optionalretrievable). If a retrievable filter is left in to become a permanent filter,ts long-term fate has not yet been defined.Filters are usually placed in an infrarenal location. However, filters may
lso be placed in either the suprarenal location or in the superior venaava in special circumstances. Indications for suprarenal placementnclude high-lying clot, pregnancy, or in a women of childbearingotential, or a previous device that has filled with clot or failed. Sepsis isot a contraindication to the use of wire-based filters since the trappedaterial can be sterilized with antibiotics. Although traditionally filters
ave been placed under x-ray guidance, percutaneous techniques for filternsertion using bedside external ultrasound or intravascular ultrasound toeduce exposure to x-rays are now being recommended. Transabdominalxternal ultrasound is ineffective in the face of morbid obesity, if there isverlying bowel gas, or if there are open abdominal wounds. In thesenstances, intravascular ultrasound has been found to be more success-ul.66 Other than 1 randomized prospective study on the use of filters asreatment of DVT (which is not how filters are traditionally used), thevidence for the use of filters is given a 2C level of evidence67 (Table 1).
onpharmacological TreatmentsPain and swelling after an above-the-knee DVT can be decreased by
pproximately 50% by the use of strong compression stockings.68
dditionally walking with good compression does not increase the risk ofE, while significantly decreasing the incidence and severity of pain andwelling after DVT.69,70 It is recommended that once patients areherapeutic on anticoagulants they ambulate while wearing compression
tockings. The use of strong compression and early ambulation after DVTurr Probl Surg, December 2008 855

tpe
aNiboslr
T
I
pmdhhettpt
aha
3cmamstwo
8
reatment is initiated can significantly reduce the long-term morbidity ofain and swelling resulting from the DVT and carries a 1A level ofvidence68,69 (Table 1).In addition to the long-term problems related to DVT and PE, there is
n increased rate of death. In a study involving 665,248 patients from theationwide Inpatient Sample, VTE (DVT or PE) was associated with an
ncreased death rate and unfavorable discharge rate (discharge to reha-ilitation facility, nursing home, or another hospital) in those patientsriginally admitted for myocardial infarction, heart failure, pneumonia, ortroke.71 Venous thromboembolism was also associated with increasedength of stay and increased cost. Thus, VTE appears to confer a significantisk of death in addition to its adverse effects on the legs and lungs.
hrombosis Prophylaxis
ntroduction and Magnitude of the ProblemVenous thromboembolism is an enormous and poorly recognizedroblem that affects thousands of people every year and is associated withore deaths annually than breast cancer, AIDS, and accidental
eaths.72,73 More than 12 million patients, which represents 31% of USospital discharges in 2003, were at risk of VTE.74 Heit and colleaguesave estimated that 296,000 patients die yearly from fatal pulmonarymboli (PE) and one third of these individuals die in a community ratherhan hospital setting. It is noteworthy that this analysis estimated that onehird of the fatal PE events manifested as sudden death, denying anyhysician-related treatment opportunities.75 Venous thromboembolism ishe number one preventable cause of death in hospitalized patients.76
It has been estimated that 200,000 nonfatal PE events occur annuallynd 4% of those patients can be expected to develop chronic pulmonaryypertension.77 This problem may pose quality-of-life issues for thoseffected and is a long-term permanent disability.Nonfatal DVT represents a serious health issue affecting approximately75,000 patients per year.75 These patients require anticoagulants, whichan cause spontaneous bleeding and require frequent blood tests. Patientsay need to limit the intake of certain foods and drink while taking the
nticoagulants, and avoid contact sports or similar activities where injuryay result in excessive bleeding. Many of these patients will require
upport stockings to control symptoms or leg swelling and to help preventhe post-thrombotic syndrome.78 Borow and Goldson studied 500 patientsho underwent surgical procedures lasting 1 hour or more, who were
ver the age of 40 years, and who underwent postoperative fibrinogen56 Curr Probl Surg, December 2008

sppmtt
sotapot
oobs
tpssr
T
P
C
canning confirmed with contrast venography. They reported that 66% ofatients who had a history of venous thrombosis developed thrombosisostoperatively. They observed that 50% of the patients with a significantedical history, including previous abdominal or leg surgery, trauma to
he lower abdomen, or leg fracture, developed postoperative venoushrombosis.79,80
One of every 3 patients following a DVT will develop post-thromboticequelae within 2 years; these sequelae are severe in approximately 20%f cases and produce considerable socioeconomic consequences.81 Symp-oms include aching, pain, or leg swelling that progresses during the daynd improves overnight with bedrest. The more severe manifestations ofost-thrombotic syndrome in the legs include skin pigmentation, rashes,r open ulcers.82 This represents a permanent disability and necessitateshe wearing of life-long compression stockings or bandages.83,84
Another important complication of DVT is a paradoxical embolus thatccurs when a clot travels to the right heart, traverses a patent foramenvale, and travels to the brain resulting in a nonhemorrhagic stroke. It haseen documented that 50% of patients presenting with a cryptogenictroke have a patent foramen ovale.85
The focus of thrombosis prophylaxis should be directed toward preven-ion of the many faces of VTE seen in Table 3. Too often clinicians focusurely on preventing clinical and fatal events rather than the entirepectrum of the disease. To evaluate all of the complications of VTE,tudies must be conducted over extended periods of time to see the full
ABLE 3. The many faces of venous thromboembolism
● Prevent fatal pulmonary emboli1% to 5% incidence in patients with �4 risk factors16.7% mortality at 3 months33% of those with pulmonary emboli present as sudden death
● Prevent chronic pulmonary hypertension4% of patients suffering PE
● Prevent clinical venous thromboembolismMorbidity, drugs, tests, hose, changes in lifestyle
● Prevent silent venous thromboembolismRisk of subsequent event doubles that of control population
● Prevent embolic stroke (20% to 30% PFO rate)50% disabled; 20% die; 30% recover
● Prevent the post-thrombotic syndrome33% incidence following DVT and 7% severeMay not be evident for 2 to 5 years
E, pulmonary embolism; PFO, patent foramen ovale; DVT, deep venous thrombosis.
amifications of the disease.86
urr Probl Surg, December 2008 857

R
ttethntVolsghth(Vai1tcbaassVhensrpfoi
8
isk AssessmentRisk assessment as a guide to thrombosis prophylaxis is necessary since
here is not only a variety of risk factors but the relative risk of each ofhese factors is not the same.87 Heit and colleagues calculated riskstimates for individual factors in a large observational study and foundhe following results: malignant neoplasm 18%, trauma 12%, congestiveeart failure 10%, central venous catheter or pacemaker placement 9%,eurological disease with extremity paresis 7%, and superficial veinhrombosis 5%. Together, 8 risk factors accounted for 74% of all cases ofTE in their study.88 Borow and Goldson have shown that the incidencef VTE increases dramatically to more than 60% with age, or with theength of surgical procedures.79,80 Sugerman and colleagues have ob-erved increasing VTE rates in patients with a body mass index (BMI)reater than 55 and the venous stasis syndrome.89 Kroger and colleaguesave identified risk factors in the cancer patient that are associated withhe development of VTE. Hospitalization, past history of VTE, familyistory of VTE, fever, chemotherapy, and elevated C-reactive proteinCRP) were identified. In the absence of all these factors the predictedTE risk was 2.3%, increasing to 72% if all were present.90 Anderson
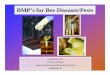
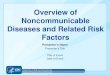
nd Spencer have reported that those with 4 risk factors had a 50%ncidence of VTE in their population-based studies, and the incidence was00% in individuals with 5 documented risk factors.91 We have observedhat evidence-based guidelines are applicable only for patients who fit theriteria of the clinical trials. The unique risk pattern of an individual maye such that the prophylaxis appropriate for a particular group may not beppropriate for an individual. A recent Chest consensus document haslso expressed this opinion.92 Kucher and colleagues developed a risktratification schema that identified a high incidence of imaging-provenymptomatic VTE (8.2%) in patients 90 days after hospital discharge. TheTE incidence was reduced to 4.9% using an electronic alert duringospitalization reminding the physician to consider prophylaxis.93 Wemploy a comprehensive risk assessment schema inquiring about a largeumber of risk factors that have been associated with VTE.87 A relativecore for each of these factors has been calculated based on the results ofandomized clinical trials. To simplify the process and maximize com-liance, we ask the patient to complete a straightforward medical historyorm (Fig 2). This is given to the admitting physician, physician assistant,r nurse, and the full risk assessment completed and scored (Fig 3). This
nformation is used to provide a guide to the onset, type, intensity, and58 Curr Probl Surg, December 2008

dtrtf
ta
F
C
uration of prophylaxis. The document includes an algorithm for selec-ion of prophylaxis for individual patients. We are in the process ofefining and validating this document. Zakai and colleagues have shownhis system to be valuable in identifying medical patients who are at riskor developing VTE.94
Despite these tools the utilization of prophylaxis is poor, and some feelhat until prophylaxis is mandated the percentage of patients that receive
IG 2. Patient intake risk assessment form.
ppropriate protection will remain suboptimal.
urr Probl Surg, December 2008 859

P
apri1rD90bmrpsos
Pprachiphfiitie
ti1lr
8
harmacologic Methods of VTE ProphylaxisLow-dose unfractionated heparin (UFH) was the first pharmacological
gent to be widely investigated for the primary prevention of VTE inatients undergoing surgery. Kakkar demonstrated that LDH significantlyeduced the risk for both DVT and PE in general surgical patients,ncluding fatal PE.95 Thirteen years later another meta-analysis including6,000 patients has compared UFH versus no prophylaxis in surgery. Theesults of this review show that UFH significantly reduced the risk ofVT by 56% compared with no prophylaxis (relative risk [RR] � 0.44;5% confidence interval [CI] 0.37-0.52) and the risk of PE by 30% (RR �.70; 95% CI 0.53-0.93) without significantly increasing the risk ofleeding complications.96 Although no direct comparisons have beenade, in general, UFH should be administered twice daily in moderate-
isk patients, and 3 times daily in high-risk patients according to evidenceresented in the American College of Chest Physicians (ACCP) consen-us document that was just released.97 There is evidence that an increasef wound hematomas from 3.8% to 6.2% could be minimized by avoidingubcutaneous injection of heparin near to the surgical wounds.Unfractionated heparin is very effective for the prevention of DVT andE in general surgery, gynecology, and urology, but suffers from oneotentially serious complication, namely HIT in up to 5% of patientseceiving heparin. This disorder is characterized by the development ofntiplatelet antibodies and characterized by a dramatic drop in the plateletount, usually below 100,000/mm3.98 In 20% of patients suffering fromeparin-related thrombocytopenia there is thrombosis that may lead toschemic complications. One should remember that a 50% drop in thelatelet count is presumptive evidence that HIT is present. The shortalf-life of UFH (0.5-2 hours) is another limitation because it makes morerequent dosing necessary. Yet, this short half-life is an asset when theres a high risk of bleeding complications or in patients with renalmpairment. This drug can be measured with the activated partialhromboplastin time (APTT) and neutralized with protamine sulfate. UFHs widely used for cardiac and vascular surgical procedures and mostvery physician understands the drug and its clinical applications.Low molecular weight heparins (LMWHs) have been developed over
he past 25 years by chemical or enzymatic degradation of UFH resultingn an average molecular weight between 4000 and 8000 D compared with5,000 D for UFH. These LMWHs have improved bioavailability andonger half-life than UFH, and have a more predictable anticoagulant
esponse than UFH. They have become the standard for prophylaxis and60 Curr Probl Surg, December 2008

tisoTbagscswisLrhp
spVt
imhosm
adc
P
aa
a
C
reatment in a wide variety of clinical settings. As a result once dailynjections can be used for prophylaxis including their use in the outpatientetting. The high and consistent bioavailability coupled with an absencef heparin resistance permit using this drug without routine monitoring.he efficacy of LMWHs for the prevention of postoperative VTE haseen demonstrated in several randomized controlled trials and meta-nalyses comparing LMWHs with placebo and UFH in general sur-ery.99-101 The comparison between the 2 compounds has revealedimilar efficacy, and LMWHs, at appropriate doses, may reduce bleedingomplications in general abdominal surgery. A very large study in 23,078urgical patients demonstrated that either LMWH or UFH was associatedith a 0.15% incidence of fatal PE with a bleeding rate of less than 1.5%
n either group.102 This study coupled with the Kakkar and Collinstudies, which total 20,000 patients, demonstrate the value of UFH orMWH in nearly eliminating fatal PE in surgical patients. We would
ecommend using one of these drugs in most situations including for veryigh-risk patients that do not fit the clinical trial criteria but needrotection.Patients having abdominal operations for cancer have been studied in
everal trials employing 30 days of LMWH compared with 7 days ofrophylaxis. The results indicate a statistically significant reduction inTE in the prolonged prophylaxis groups compared with those receiving
he short course of anticoagulants.47,103
Fondaparinux is a synthetic, injectable pentasaccharide that selectivelynhibits factor Xa producing a conformational change in the antithrombinolecule. This drug has a high bioavailability and long half-life (17
ours). Only 1 case of HIT has been associated with this drug, andsteoporosis has not been observed. This drug is renally excreted andhould not be used in patients with a creatinine clearance of less than 30L/min.104
Fondaparinux has been evaluated in high-risk patients undergoingbdominal surgery and showed equivalent efficacy as the LMWHalteparin with no statistically significant differences in bleeding compli-ations.53
hysical Methods of VTE ProphylaxisPhysical and mechanical methods include graduated elastic stockings
nd intermittent pneumatic compression (IPC) of the calf alone, or calfnd thigh and impulse foot.Elastic compression stockings of the legs reduce the cross-sectional
rea of the veins and, as a result, increase the velocity of blood flow
urr Probl Surg, December 2008 861

is3ucu
F
8
n the limb. It has been demonstrated that graduated compressiontockings (GCS) significantly increased the blood velocity around0% at the femoral vein during recumbence as detected by Dopplerltrasound.105 The optimal pressure profile according to these authorsonsisted of 18 mm Hg at the ankle, decreasing to 8 mm Hg in thepper thigh.
IG 3. Venous thrombosis risk factor assessment form.
It has been shown that endothelial cracking is associated with venous
62 Curr Probl Surg, December 2008

domab
F
C
ilation and can be the beginning of a thrombus.106 Venous dilation oftenccurs due to the loss of calf muscle tone with the administration of auscle relaxant during the induction of general anesthesia.107 If the leg is
lso in a dependent position, this aggravates the stasis and can initiate the
IG 3. Continued
eginning of the thrombotic process. It has been shown that GCS can
urr Probl Surg, December 2008 863

pc
m16s
oer0oto
scG
ls8d
iuicbh
tecppdific
8
revent venous distension that occurs in deep veins of the leg during theourse of operation.108
The efficacy of GCS for VTE prevention has been studied in aeta-analysis involving 11 studies investigating the efficacy of GCS in
800 moderate-risk surgery patients. The results showed a significant8% reduction in the incidence of postoperative DVT in patients withtockings (OR 0.28; 95% CI 0.23-0.48; P � 0.0001).109
Seven additional randomized controlled trials in general, gynecological,rthopedic, and neurosurgical patients revealed the incidence of postop-rative DVT detected by objective diagnostic methods to be significantlyeduced from 29% in the control group to 15% in the GCS group (OR.33; CI 0.26-0.49; P � 0.0001).110 Finally in another systematic reviewf the literature in more than 2400 patients, there was a 66% reduction inhe incidence of DVT, from 21% (133 of 677) in the controls to 8.6% (57f 665) in the GCS group (P � 0.001).111
Although GCS are as effective for DVT prevention in moderate-riskurgical patients, there is a lack of data in high-risk patients includingancer or orthopedic surgery patients. There is no evidence to suggest thatCS prevents pulmonary emboli.There is no conclusive evidence regarding the use of thigh versus calf
ength stockings. Two trials comparing thigh-length and knee-lengthtockings revealed that the incidence of DVT was 8.7% (9 of 104) and.3% (9 of 108), respectively. These results are considered inconclusiveue to the small number of patients and the low DVT rate.112,113
The main limitations of GCS include the lack of international standard-zation of their pressure profiles and the difficulty to fit patients withnusual leg sizes or shapes. Patient compliance may be another limitingssue, especially with thigh-length stockings. Common reasons for non-ompliance included that stockings were not reapplied after cleaning orathing, or were removed because patients complained of itching oreat.112
Intermittent pneumatic compression is the most extensively studied ofhe mechanical methods of prophylaxis and is considered the mostffective of the mechanical methods. These devices may be singlehamber or multiple chamber, and provide uniform or sequential com-ression. One of the available devices indirectly estimates the leg venousressure and adjusts the compression cycle to these changes. Theseevices can compress the leg up to 3 times per minute.114 Anothermportant effect of IPC for VTE prevention is the stimulation ofbrinolysis and coagulation physiological inhibitors by a variety of
hanges in specific fibrinolytic parameters.115-11864 Curr Probl Surg, December 2008

rRpfteutipelp
acif
C
dmpt
CA
tswcPcrtCf
C
The results of IPC have been variable, but most studies show that IPCeduces the incidence of DVT in a variety of surgical procedures.oderick and colleagues identified 19 trials assessing IPC in 2255atients and showed that IPC significantly reduced the incidence of DVTrom 23.4% (268 of 1147) in the control group to 10.1% (112 of 1108) inhe IPC group, a 66% odds reduction (P � 0.0001).111 There was novidence that sequential compression devices were more protective thanniform compression machines, as their odds reductions were 65% (6rials) and 66% (12 trials), respectively. Another report of 15 trialsnvolving 2200 patients also demonstrated the efficacy of IPC for VTErophylaxis.119 The issue of whether above-knee IPC devices are moreffective than calf-length devices remains unclear in the absence ofarge-scale trials. The choice between both alternatives should be made onractical grounds, depending on their availability and cost.As with GCS, another important issue regarding IPC is compliance and
dequate implementation. Comerota and colleagues have recorded a poorompliance record for these devices and highlighted an urgent need tomprove patient and nursing staff education on the appropriate use of IPCor VTE prophylaxis to optimize implementation.120
ombination of Physical and Pharmacologic MethodsEver since the first description of the factors leading to theevelopment of a venous thrombosis, we have been searching forethods to prevent venous thromboembolism. The combination of
hysical and pharmacologic methods appears ideal as a method ofhrombosis prophylaxis.
ombination of Mechanical Methods andnticoagulantsThere are multiple randomized controlled trials that demonstrate that
he combination of GCS in addition to another prophylactic method wasignificantly more effective than GCS alone. Deep venous thrombosisas encountered in only 2% of the patients in the combined group
ompared with 15% in the control group.110 The Pulmonary Embolismrevention Trial involved a large multinational study that showed that theombination of GCS stockings plus aspirin was effective in lowering theate of fatal PE in hip fracture patients, whereas aspirin alone did not havehe same effect.121 The combination of heparin and GCS in anotherochrane analysis demonstrated superiority compared with heparin alone
ollowing colorectal surgery.122
Most studies using combined modalities involve the use of IPC in
urr Probl Surg, December 2008 865

ctctg
rTgtpvcigaap21ippruL(0rtccnuwgest1
8
onjunction with various anticoagulants. Borow and Goldson showedhat using the combination of aspirin, heparin, or coumadin inonjunction with IPC resulted in a 1.5% incidence of DVT in thereated population compared with a 26.8% incidence in the controlroup.123
In one study patients undergoing total hip replacement (THR) wereandomized to IPC alone, IPC plus aspirin, or IPC plus low-dose warfarin.he incidence of ultrasound-detected VTE was 10% in each of theroups.124 Woolsen and Watt showed that the combination was not betterhan IPC although the ultrasonic endpoint and small size of the study (196atients) make it difficult to conclude that combination prophylaxis is notaluable. The effectiveness of the plantar venous plexus foot pumpombined with unfractionated heparin in patients having THR was shownn a study that revealed a 6.6% venographic DVT rate in the combinationroup compared with 27% in the nonpumped group (P � 0.025). Theuthors conclude that chemical prophylaxis plus the use of GCS stockingsnd foot pump reduces the incidence of DVT more than chemicalrophylaxis alone.125 Ramos and colleagues performed a study involving551 patients having coronary artery bypass surgery (CABG) over a0-year period. Patients received either 5000 units of UFH twice daily orn combination with long-leg sequential IPC. The incidence of imaging-roven PE was 4.0% in the heparin group and 1.5% in the combinationrophylaxis group (P � 0.001).126 A study in patients having total jointeplacement involving LMWH in combination with IPC showed 0%ltrasound-detected thrombosis compared with the group receivingMWH and compression stockings where the DVT incidence was 28.6%
40% after total knee replacement [TKR], 14% after THR) (P �.0001).127 A large orthopedic study was done in which patients wereandomized prospectively to receive either LMWH alone or in combina-ion with IPC. In the LMWH group, 15 patients (1.7%) had a DVT,ompared with 4 patients (0.4%) who had a DVT (P � 0.007) in theombined group.128 Low molecular weight heparin or aspirin in combi-ation a foot pump was studied in 275 TKR patients and the incidence ofltrasound DVT was 14.1% using LMWH and the foot pump, and 17.8%ith the aspirin and the foot pump.129 Recently a very large series ofeneral surgical patients was reported that were randomized to receiveither a placebo saline injection daily or 2.5 mg of Fondaparinux, aelective inhibitor of factor Xa, daily for 7 days. Bilateral venography onhe seventh day revealed a 5.3% DVT incidence in the saline group and
.7% in the Fondaparinux group.130 All of this evidence supports the66 Curr Probl Surg, December 2008

cc
C
cca
fpa3Ilboa
T
atamprdl1Updogmspesp
C
oncept that combined modalities provide superior DVT preventionompared with any single thrombosis prophylaxis modality.
urrent Recommendations for Combined ProphylaxisThe newly released 8th ACCP recommends IPC as an option in
onjunction with heparin or LMWH in patients in the highest riskategory for VTE. The combination of mechanical methods and thesenticoagulants is listed as a grade 2A suggestion97 (Table 1).Recently Amin and colleagues performed a database review of data
rom 227 hospitals over a 3.5-year period involving nearly 200,000atients looking at thrombosis prophylaxis rates in US hospitals. Theseuthors found the thrombosis prophylaxis rate was 66.8%, and only3.9% received appropriate prophylaxis according to Chest guidelines.131
t was observed that 26.8% of the patients received mechanical prophy-axis alone in cases in which there was no contraindication because ofleeding. Inappropriate prophylaxis postdischarge was noted in two thirdsf the patients, including 4.7% who received mechanical prophylaxislone.
hrombosis Prophylaxis in the Real WorldSixteen years ago we surveyed 3500 North American general surgeons
nd noted that some form of thromboprophylaxis was used 86% of theime. The most frequently used modalities were IPC, low-dose heparin,nd elastic stockings. A combination of physical and pharmacologicethods was used by one fourth of respondents, and only 50% started
harmacologic prophylaxis before the surgical procedure. The thrombosisisk factors that are most frequently considered by surgeons wheneciding about using prophylaxis are history of VTE, immobility, andength of operation.132 Seven years later a follow-up survey was sent to0,000 general surgeons and 1145 responses were received. ConventionalFH at fixed doses remains the preferred pharmacological agent for VTErevention (74%), followed by 2 LMWHs: enoxaparin (34%) andalteparin (16%). Overall, 52% of surgeons preferred physical methodsver pharmacological methods when used separately and 26% of sur-eons utilize combined physical-pharmacological modalities. A largeultinational cross-sectional study in more than 68,000 patients repre-
enting 352 hospitals in 32 countries was recently published. Theercentage of patients that received appropriate prophylaxis according tovidence-based guidelines was 40% in medical patients and 59% inurgical patients (Table 4).133 The Global Orthopedic Registry recently
ublished by Warwick and colleagues shows more encouraging results.urr Probl Surg, December 2008 867

TrmSwomrli3ivsg
A
tdaetm(
satD
vN
T
V
8
here were 15,000 patients in the registry and 95% of these individualseceived anticoagulant or mechanical prophylaxis following joint replace-ent procedures. LMWH prophylaxis was popular outside of the Unitedtates and combined with IPC 11% to 17% of the time. This combinationas used in nearly 25% of American patients. Warfarin use was rareutside the United States; however, it was combined with IPC approxi-ately 33% of the time in the United States.134 Amin and colleagues have
eported a database review from 227 hospitals involving 200,000 patientsooking at thrombosis rates in American hospitals.131 Overall thesenvestigators found the thrombosis prophylaxis rate was 66.8%, with only3.9% conforming to Chest guidelines. This study highlights two remain-ng serious problems regarding thrombosis prophylaxis. There are stillery substantial numbers of patients not being protected and even whenome form of prophylaxis is used, it does not conform to evidence-baseduidelines.
ggressive Therapies for Acute DVT and PEThe term “aggressive treatment” gives the connotation that it is out of
he ordinary or unusual. For the purpose of this discussion, aggressive isefined as adopting a strategy of thrombus removal before long-termnticoagulation, rather than accepting the existing venous thrombosis ormbolic pulmonary occlusion and treating the patient with anticoagula-ion alone, thereby accepting all of the post-thrombotic or embolicorbidity that accompanies iliofemoral DVT and pulmonary embolism
PE).Studies have shown that patients with post-thrombotic syndrome have a
ignificant reduction in their quality of life.135,136 The severity of thecute venous thrombotic event is predictive of the degree of post-hrombotic morbidity. This is especially true in patients with iliofemoralVT.Iliofemoral DVT is a clinically relevant subset of patients with acuteenous thrombosis who suffer severe post-thrombotic morbidity.137-139
ABLE 4. ENDORSE Registry133
Medical Surgical
No. of patients 37,356 30,827At risk for VTE 42% 64%Receiving ACCP Tx 40% 59%
TE, venous thromboembolism; ACCP, American College of Chest Physicians; Tx, treatment.
inety percent of iliofemoral DVT patients who are treated with
68 Curr Probl Surg, December 2008

aisvdto
dphchtshr
hlhittdTtlm
E
rmbwhamtp
C
nticoagulation alone will have ambulatory venous hypertension, result-ng in severe chronic venous insufficiency. Up to 40% will haveymptoms of venous claudication, and within 5 years, 15% developenous ulceration. The adverse impact on quality of life is evident. Thisiscussion reviews the body of evidence demonstrating that a strategy ofhrombus removal is the preferred management for patients with iliofem-ral DVT and offers the best long-term outcome.140,141
In general, avoiding pathophysiology or minimizing pathophysiologicisturbances offers patients the best chance of a favorable outcome. Theathophysiology of post-thrombotic venous disease is ambulatory venousypertension, defined as an elevated venous pressure during exer-ise.142,143 Nicolaides and colleagues143 and Welkie and colleagues144
ave demonstrated that ambulatory venous pressure is directly linked tohe clinical manifestations observed with chronic venous disease, such aswelling, pigmentation, and lipodermatosclerosis. Long-standing venousypertension has a significant effect on the microcirculation, which canesult in dermal breakdown.Two pathologic anatomic components contribute to ambulatory venousypertension: venous valvular incompetence and obstruction of the veinumen. The most severe post-thrombotic morbidity is associated with theighest venous pressures, which occur in patients with combined valvularncompetence and luminal obstruction.142,143,145 It is intuitive that ifhrombus is removed and patency restored, obstruction cannot be part ofhe underlying pathophysiology. Long-term studies of acute DVT haveemonstrated that early thrombus resolution preserves valve function.146
herefore, early thrombus removal in patients with extensive venoushrombosis eventually eliminates the underlying pathologic conditionseading to ambulatory venous hypertension and has the potential ofaintaining normal venous physiology.
vidence Supporting an “Aggressive” ApproachThere is a spectrum of evidence supporting a strategy of thrombus
emoval in patients with acute DVT. Although small segmental thrombiay be well tolerated in many patients without significant post-throm-
otic morbidity, typically in the femoral vein of the mid thigh, patientsith extensive DVT, especially those with iliofemoral thrombosis, willave severe post-thrombotic morbidity if treated with anticoagulationlone. Data are available from experimental observations in animalodels,147,148 long-term follow-up studies in patients with acute DVT
reated with anticoagulation alone,146,149,150 clinical reports of large
atient series,151-153 and randomized trials.154-157 The aggregate dataurr Probl Surg, December 2008 869

ovbot
S
mgofld
ct
ott
T
DCiifiaoAotp
ptttr
8
verwhelmingly demonstrate that patency can be restored, vein wall andalvular function can be maintained, and post-thrombotic morbidity cane reduced if thrombus is successfully eliminated, intrinsic vein pathol-gy (stenosis) corrected, and long-term therapeutic anticoagulation main-ained to avoid rethrombosis.
trategies of Thrombus RemovalStrategies of thrombus removal have not been widely accepted by theedical community. In large part, this is the result of international
uidelines recommending against catheter-directed thrombolysis andperative venous thrombectomy.158 Unfortunately, authors of these in-uential guidelines focused on outdated information published manyecades earlier and overlooked contemporary randomized trials.Treatment approaches that have adopted venous thrombectomy and
atheter-based thrombolytic therapy have demonstrated significantly bet-er outcomes compared with patients treated with anticoagulation alone.The underlying principles are similar whether one employs an operativer percutaneous approach. The initial goal is to eliminate all acutehrombus followed by correction of underlying venous pathology andherapeutic anticoagulation to avoid rethrombosis.
reatment Options and Patient EvaluationAn important part of the initial evaluation of patients with iliofemoralVT is a CT scan of the head, chest, abdomen, and pelvis. Martinez andomerota159 reported their CT scan findings in patients presenting with
liofemoral DVT. In addition to finding asymptomatic pulmonary embolin 50% of patients and assessing the proximal extent of thrombus, theyound an undiagnosed malignancy in 79% of patients with idiopathicliofemoral DVT. Since iliofemoral DVT is generally the result of anggressive thrombotic stimulus, it is not surprising that a large proportionf idiopathic patients are found to have an underlying malignancy.lthough chest, abdomen, and pelvic CT scans have been a routine partf the evaluation of iliofemoral DVT patients at Jobst Vascular Center forhe past several years, a head CT is now added to rule out intracranialathology.Contemporary venous thrombectomy is generally available to allatients where vascular surgeons practice. There are few contraindica-ions to operative thrombectomy, especially when the thrombus is lesshan 10 days old. Treatment goals are straightforward: to removehrombus in the iliofemoral and infrainguinal venous segments and
estore unobstructed venous return into the vena cava. Knowing the full70 Curr Probl Surg, December 2008

et
mAta
Tniadt
smdrme
O
htflparcmPvlcFpoa
C
xtent of thrombus preoperatively and having good imaging intraopera-ively is imperative for a well-planned and successful procedure.Catheter-directed thrombolysis is the preferred treatment option forost patients who have no contraindications to thrombolytic therapy.djunctive mechanical techniques are becoming increasingly popular and
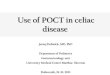
end to shorten treatment time and reduce the dose of plasminogenctivator.A frequent concern of physicians is the risk of procedure-related PE.he patients at highest risk of procedure-related PE are those withonocclusive thrombus in their vena cava. Therefore, it is important tomage the proximal and distal extent of thrombus and particularly themount and level of vena caval involvement. This will assist in theecision whether vena caval filtration or other forms of embolic protec-ion (eg, balloon occlusion) are used (Fig 4).The traditional contraindications to the use of thrombolytic agents are
oftened by direct intrathrombus infusion and the use of adjunctiveechanical techniques. If the dose of lytic agent can be reduced and the
uration of therapy shortened, the risk of a systemic lytic effect iseduced, since circulating plasminogen activator inhibitors and antiplas-ins neutralize the effect of plasminogen activators and plasmin that
scape into the systemic circulation.
perative Venous ThrombectomyContemporary venous thrombectomy for iliofemoral venous thrombosisas been shown to be effective in both the short and the longerm.154,155,160 The largest report of operative venous thrombectomyailed to show fatal PE and reported only 1 operative death.161 Theong-term benefits of venous thrombectomy relate to its ability to achieveroximal patency and maintain distal valve competence. Both outcomesre influenced by the initial technical success and the avoidance ofecurrent thrombosis. Therefore, attention to operative detail in terms ofomplete thrombus removal, correcting underlying venous stenoses, andaintaining therapeutic anticoagulation postoperatively are crucial.ooled data from a number of contemporary reports on iliofemoralenous thrombectomy (Table 5154,162-173) demonstrate that early andong-term patency of the iliofemoral venous segment is 70% to 80%ompared with 30% of patients treated with anticoagulation alone.139
emoropopliteal venous valve function is preserved in the majority ofatients. The Scandinavian investigators reported their randomized trialutcomes of operative venous thrombectomy versus anticoagulation
lone in patients with iliofemoral venous thrombosis.154-156 Patientsurr Probl Surg, December 2008 871

uyi0
Fsaintftv
8
nderwent complete follow-up evaluation at 6 months, 5 years, and 10ears. They showed that those randomized to venous thrombectomy hadmproved iliac vein patency (P � 0.05), lower venous pressures (P �
IG 4. A young man with an acute gastrointestinal bleed from Crohn’s colitis developed a painful,wollen left leg with bluish discoloration (phlegmasia cerulea dolens). Venous duplex documentedcute thrombus extending from the distal femoral vein into the external iliac vein. A contralateral
liocavagram was performed to evaluate the vena cava, which demonstrated a sizable amount ofonocclusive thrombus extending into the vena cava (A). In preparation for his operative venoushrombectomy, a caval occlusion balloon was positioned under fluoroscopy from the right commonemoral vein and was inflated during the iliocaval thrombectomy (B, C). The entire proximal and distalhrombus was removed intact (D, E). (Reprinted with permission from Comerota and Gale.174) (Colorersion of figure is available online.)
.05), less leg edema (P � 0.05), and fewer patients with post-thrombotic
72 Curr Probl Surg, December 2008

savC
C
ttdc
Tf
17
T
MR
C
yndrome (P � 0.05) compared with patients treated with anticoagulationlone. Table 6 briefly summarizes the general aspects of the contemporaryenous thrombectomy. Specific operative detail has been published byomerota and Gale.174,175
atheter-Directed ThrombolysisEarly attempts of pharmacologic clot dissolution of acute venous
hrombosis used systemic delivery of plasminogen activators. Althoughhe results demonstrated reduced post-thrombotic morbidity, the highoses of plasminogen activators resulted in higher rates of bleeding
ABLE 5. Long-term results of venous thrombectomy with arteriovenous fistula: iliac vein patency andemoral-popliteal valve competence
No. of reports PatientsFollow-up
(mos) (mean)Iliac veinpatency
Femoral-poplitealvalve competence
1154,162-171 702 41 78% —154,163,165,169,170,172,173 352 45 — 63%
ABLE 6. Technique of contemporary venous thrombectomy
1. Identify etiology of extensive venous thromboembolic processa. Complete thrombophilia evaluationb. Rapid CT scan of head, chest, abdomen, and pelvis
2. Define full extent of thrombusa. Venous duplex examinationb. Contralateral iliocavagram, MRV, or spiral CT
3. Prevent pulmonary embolism (numerous techniques)a. Anticoagulationb. Vena caval filter (if nonocclusive caval clot)c. Balloon occlusion of vena cava during thrombectomyd. Positive end-expiratory pressure during thrombectomy
4. Perform complete thrombectomya. Iliofemoral (vena cava) thrombectomyb. Infrainguinal venous thrombectomy (if required)
5. Ensure unobstructed venous inflow to and outflow from thrombectomized iliofemoralvenous systema. Infrainguinal venous thrombectomy (if required)b. Correct iliac vein stenosis (if present)
6. Prevent recurrent thrombosisa. Construct arteriovenous fistula (3.5- 4 mm)b. Continuous therapeutic anticoagulationc. Catheter-directed postoperative anticoagulation (if infrainguinal venous
thrombectomy is required)d. Extended oral anticoagulation
RV, magnetic resonance venography; CT, computerized tomography.eprinted with permission from Comerota and Gale.175
omplications.176 Many patients in these studies were treated for infrain-
urr Probl Surg, December 2008 873

T
S
S
VB
M
C
HKA
V
E
CG
L
SJO
K
L
P
G
CIptR
8
ABLE 7. Review of studies of catheter directed thrombolysis for acute DVT
Author, year
Total no.of patients
(limbs) Intervention
emba et al,180 1994 21 (27) CDT with UK, angioplasty/stenting forresidual stenosis
emba et al,181 1996 32 (41) CDT with UK, angioplasty/stenting forresidual stenosis
erhaeghe et al,182 1997 24 CDT with rt-PA, stenting for residual stenosisjarnason et al,151 1997 77 (87) CDT with UK, angioplasty, stenting,
thrombectomy, bypass for residualstenosis
ewissen et al,152 1999 287 (312) CDT with UK, stenting for residual stenosis;systemtic lysis (n � 6)
omerota et al,153 2000 54 CDT with UK or rt-PA, thrombectomy forresidual stenosis
orne et al,183 2000 10 CDT with rt-PAasirajan et al,184 2001 9 CDT with UK, rt-PA, or rPAbuRahma et al,185 2001 51 CDT w/UK or rt-PA, stents/18 Hep/33
edantham et al,186 2002 20 (28) CDT with UK, rt-PA, or rPA, thrombectomy,stenting
lsharawy et al,157 2002 35 CDT w/SK, angio, stent/18 Hep/17
astaneda et al,187 2002 15 CDT with rPArunwald et al,188 2004 74 (82) CDT with UK, tPA, or rPA, angioplasty,
stentingaiho et al,189 2004 32 CDT with rt-PA/16
Systemic lysis with rt-PA/16illesen et al,190 2005 45 CDT with rt-PA, angioplasty, stentingackson et al,191 2005 28 CDT with UK or rPA, stentinggawa et al,192 2005 24 CDT with UK/10
CDT with UK � IPC/14im et al,193 2006 37 (45) CDT with UK/23
CDT � PMT/14in et al,194 2006 93 (98) CDT with rPA, rt-PA, or UK, angioplasty,
stenting/46PMT with rPA, rt-PA, or UK, angioplasty,
stenting/52rotack et al,195 2007 69 CDT with UK, tPA, retavase, pulse-spray,
mechanical thrombectomy, stenting, IVCfilters
oldenberg et al,196 2007 22 CDT and/or systemic lysis with mechanicalthrombectomy/9
Anticoagulation alone/13
DT, catheter-directed thrombolysis; Hep, heparin; IPC, intermittent pneumatic compression;VC, inferior vena cava; NR, not reported; rPA, recombinant plasminogen activator; PMT,harmacomechanical thrombolysis; rt-PA, recombinant tissue plasminogen activator; tPA,issue plasminogen activator; UK, urokinase.
eprinted with permission from Comerota and Gravett.14074 Curr Probl Surg, December 2008

C
Results Complications
Significant/completeresolution
(%)
Partialresolution
(%)
Noresolution
(%)
Bleeding
Minor(%)
Major(%) PE
Death dueto Rx (%)
18 (72) 5 (25) 2 (8) 1 (4) 0 (0) None None
21 (32) 9 (28) 2 (6) 0 (0) 0 (0) None None
19 (79) 5 (21) 0 (0) 0 (0) 6 (25) None None69 (79) 0 (0) 18 (21) 11 (14) 5 (6) 1 None
96 (31) 162 (52) 54 (17) 15 (28) 54 (11) 6 2 (�1)
14 (26) 28 (52) 6 (11) 8 (15) 4 (7) 1 None
9 (90) 1 (10) 0 (0) 3 (30) None 2 (20) None7 (78) 1 (11) 1 (11) NA NA NA NA
15 (83)1 (3)
NRNR
NRNR
3 (17)3 (9)
2 (11)2 (6)
None2 (6)
NoneNone
23 (82) NR NR None 3 (14) None None
13 (72)2 (12)
5 (28)8 (47)
0 (0)7 (41)
NoneNone
NoneNone
NoneNone
NoneNone
15 (100) NR NR None None None None54 (73) 26 (32) NR 6 (8) 4 (5) None None
8 (50) 5 (31) NR 4 (25) 2 (13) 2 (13) None5 (31) 8 (50) NR 6 (38) 1 (6) 5 (31) None
42 (93) NR NR 4 (8) None 1 (2) None5 (18) 20 (72) NR 2 (7) None None None0 (0) 10 (100) None None None None None5 (36) 9 (64) None None None None None
21 (81) 3 (11) 2 (8) 1 (4) 2 (7) 1 (4) None16 (84) 3 (16) None None 1 (5) 1 (5) None32 (70) 14 (30) 5 (11) 2 (4) 1 (2) None None39 (75) 13 (25) 4 (8) 2 (4) None None None
40 (63) 19 (30) 4 (6) None None None None
8 (89) NR NR 1 1 None None5.5 (42) NR NR
urr Probl Surg, December 2008 875

gcv
Pse
opdTnscoam
tdHspcplwtp
cspfbPm
br
8
uinal DVT; therefore, even when lytic therapy was successful, thelinical benefits were not as apparent as with patients with iliofemoralenous thrombosis.However, important observations were made in randomized trials.atients successfully treated with intravenous thrombolytic therapy had aignificantly better chance of preserving normal vein valve function andnjoyed reduced post-thrombotic morbidity.177-179
Delivery of thrombolytic agents into the thrombus results in higher ratesf clot dissolution, shorter treatment times, and reduced bleeding com-lications. Many reports have documented good outcomes of catheter-irected thrombolysis for acute DVT. Most of these reports are listed inable 7,151-153,157,180-196 which also includes pharmacomechanical tech-iques used as adjuncts to catheter-directed thrombolysis. Generally,uccess rates in the 75% to 90% range can be anticipated. Bleedingomplications have been reported in up to 11%; however, in the majorityf the reports published within the past 6 years, bleeding complicationsre 5% or less. Symptomatic PE during thrombolytic infusion is uncom-on and fatal PE is a rarity.The National Venous Registry is the largest report to date of patients
reated with lytic therapy for acute DVT. It is hampered with theeficiencies of nonrandomization and the biases of patient selection.owever, the authors reported a significant correlation of thrombus-free
urvival with the results of initial therapy (P � 0.001). At 1 year, 78% ofatients who initially had complete clot resolution had patent veinsompared with only 37% of patients who had less than 50% lysis. Inatients with first-time iliofemoral DVT who had initially successful clotysis, 96% remained patent at 1 year. Initial lytic success also correlatedith valve function at 6 months. Sixty-two percent of patients with less
han 50% thrombolysis had venous valve incompetence, whereas 72% ofatients who had complete lysis had normal valve function (P � 0.02).A quality-of-life (QOL) study was published demonstrating that suc-
essful thrombolysis for patients with iliofemoral DVT resulted in aignificantly improved quality of life compared with a control cohort ofatients treated with anticoagulation alone.153 A randomized trial per-ormed by Elshawary and Elzayat157 compared catheter-directed throm-olysis with anticoagulation alone in patients with iliofemoral DVT.atients treated with thrombolysis had considerably better outcomes at 6onths, demonstrating improved patency and vein valve function.The above data are a compelling argument for catheter-directed throm-olysis. Larger randomized trials are required to establish definitive
ecommendations for care. Fortunately, 2 large trials are under way that76 Curr Probl Surg, December 2008

wvc
P
bahlwwydlap
Fvwptccv
C
ill randomize patients with acute DVT to catheter-directed thrombolysisersus anticoagulation alone,197,198 evaluating anatomic, physiologic, andlinical endpoints.
harmacomechanical ThrombolysisAlthough good results have been reported with catheter-directed throm-olysis, treatment times are often long and doses of plasminogenctivators often high to successfully complete a course of therapy. Thisas dampened the enthusiasm of many physicians. Sillesen and col-eagues190 reported that 93% of their patients were successfully treatedith catheter-directed thrombolysis and that 90% of their patients whoere discharged with patent veins had normal venous valve function at 1ear. However, they reported an average treatment time for catheter-irected thrombolysis of 71 hours. This duration of acute care isogistically difficult for many practitioners and medical centers. Thessociated cost of care is high, especially when considering that all
IG 5. A 32-week pregnant woman presented with left leg pain and swelling of 3 days’ duration. Aenous duplex examination suggested external iliac and common iliac vein thrombosis, confirmedith ascending phlebography (A). Isolated segmental pharmacomechanical thrombolysis waserformed with a Trellis catheter using 3 mg recombinant tissue plasminogen activator (rt-PA). The
hrombus was eliminated, demonstrating stenosis of the left common iliac vein (May-Thurner). The leftommon iliac vein was dilated and stented (B), resulting in unobstructed venous drainage into the venaava (C). The patient subsequently delivered a healthy infant boy and was asymptomatic with normalenous function 1 year later.
atients receiving lytic therapy are monitored in intensive care units.
urr Probl Surg, December 2008 877

Ffi
TD
I
F
I
P
FF
P
D
8
IG 6. Treatment algorithm for patients with iliofemoral deep venous thrombosis. (Color version of
gure is available online.)ABLE 8. Evidence-based recommendations for the aggressive treatment of patients with iliofemoralVT15,201
Recommendation Grade
n patients with extensive (iliofemoral) DVT, operative venous thrombectomy maybe used to reduce acute symptoms and post-thrombotic morbidity
2B
ollowing venous thrombectomy, the same duration and intensity ofanticoagulation should be used as in those who do not undergothrombectomy
1C
n patients with extensive proximal DVT and low risk for bleeding, CDT can beused to reduce acute symptoms and post-thrombotic morbidity
2B
harmacomechanical thrombolysis should be considered in preference to CDTalone
2C
ollowing CDT, underlying venous lesions should be corrected 2Collowing CDT, the same intensity and duration of anticoagulation should beused as those who are not treated with CDT
1C
atients with acute DVT should be treated with a 30-40 mm Hg compressionstocking to reduce post-thrombotic morbidity
1A
VT, deep venous thrombosis; CDT, catheter-directed thrombolysis.
78 Curr Probl Surg, December 2008

FaapoC
IG 7. Patient being treated for a gastrointestinal bleed with sudden shortness of breath, tachycardia,nd drop in blood pressure (A). Pulmonary arteriogram showed large PE of the left main pulmonaryrtery. Following treatment with pulse-spray infusion of thrombus with 6 mg of recombinant tissuelasminogen activator (rt-PA) and catheter-based fragmentation, patient’s clinical condition improved,
xygenation improved, and subsequent cardiac echo was normal (B).urr Probl Surg, December 2008 879
tsmtobifiwotsr
crwvct
tcht
T
G
RPAHALT
P
8
Percutaneous mechanical techniques alone or in combination withhrombolysis have been developed to more rapidly clear the venousystem. Vedantham and colleagues198 evaluated the effectiveness ofechanical thrombectomy alone or in combination with pharmacologic
hrombolysis in 28 limbs of patients with acute DVT. They used a varietyf mechanical devices and catheters. They found that mechanical throm-ectomy alone was successful for removing thrombus that developedntraprocedurally (which is generally gelatinous and not cross-linked withbrin). However, in the remaining patients, only 26% of the thrombusas removed by mechanical thrombectomy. The addition of a plasmin-gen activator solution to the mechanical technique removed 82% of thehrombus. This underestimates the benefit to patients with acute DVT,ince these authors included patients with chronic occlusions who did notespond to treatment.Several reports have recently surfaced documenting the benefits of
ombined pharmacomechanical thrombolysis. Martinez and colleagues199
eported the outcome of patients with iliofemoral DVT treated initiallyith isolated segmental pharmacomechanical thrombolysis (ISPMT)ersus catheter-directed thrombolysis. Isolated segmental pharmacome-hanical thrombolysis was associated with better success rates, shorterreatment times, and lower doses of plasminogen activators (Figs 4, 5).Lin and colleagues194 reported their 8-year experience with rheolytic
hrombectomy. Patients treated with the AngioJet catheter had signifi-antly fewer phlebograms, shorter intensive care unit (ICU) stays, shorterospital stays, and fewer blood transfusions. A smaller group of patients
ABLE 9. Review of studies of mechanical thrombectomy catheters for PE
Catheter typeTotal no.patients
ConcurrentCDT (%)
Results
Completeresolution
(%)
Partialresolution
(%)
Noresolution
(%)
reenfield219-227 108 19 (18) 82 (76) 8 (7) 9 (8)
heolytic (AngioJet)228-234 70 29 (41) 65 (93) 0 2 (3)igtail235-248 175 169 (97) 156 (89) 1 (0.6) 0mplatz249-251 15 7 (47) 14 (93) 0 0ydrolyser252-254 20 20 (100) 19 (95) 0 0rrow-Trerotola255 15 0 0 1 (7) 0ang256 3 0 0 3 (100) 0otals 406 244 (60) 336 (83) 13 (3) 11 (3)
E, pulmonary embolism; MI, myocardial infarction; CDT, catheter-directed thrombolysis.
reated by Kasirajan and colleagues184 reported that rheolytic thrombec-
80 Curr Probl Surg, December 2008

tt
uDiceapt
S
tiai
vtrs
A
p
C
omy alone was less effective than combined pharmacomechanicalhrombolysis.Parikh and colleagues200 reported their initial clinical experience withltrasound-accelerated thrombolysis in both upper and lower extremityVT. Complete lysis was observed in 70% of patients and overall lysis
n 91%. The median infusion time was 22 hours and 4% had majoromplications. These results, compared with historical controls of cath-ter-directed thrombolysis, suggest an advantage to ultrasound-acceler-ted thrombolysis. It is this author’s opinion that each device may have aarticular advantage in a given clinical situation and that a combination ofechniques may be required in a given patient’s scenario.
ummary: Iliofemoral DVTThe aggregate information on operative venous thrombectomy, cathe-
er-directed thrombolysis, and pharmacomechanical thrombolysis forliofemoral DVT demonstrate substantial benefits for patients treated withstrategy of thrombus removal. A treatment algorithm for patients with
liofemoral DVT is presented in Fig 6.The recent ACCP consensus conference on antithrombotic therapy forenous thromboembolic disease has reviewed the existing evidence forhe management of patients with iliofemoral DVT and incorporatedecommendations for care. These evidence-based recommendations areummarized in Table 8.201
ggressive Treatment for Pulmonary EmbolismAnticoagulation is the recommended management for the majority of
Complications
Bleeding
Other DescriptionDeath due to
Rx (%)Minor (%) Major (%)
0 1 (0.9) 16 (15) Renal failure, pulmonary infarct, MI,pleural effusion, thrombocytopenia
8 (7)
0 10 (14) 4 (6) Heart block, thrombocytopenia 8 (11)2 (1) 2 (1) 2 (1) Cardiac arrest, catheter problems 6 (3)0 0 0 00 0 0 2 (10)0 0 0 00 0 0 02 (0.5) 13 (3) 22 (5) 24 (6)
atients with acute PE. However, patients with large pulmonary emboli
urr Probl Surg, December 2008 881

cwownnc4spadd2ptftpa
pdrhfptwllwHsiam
owt
8
ausing hemodynamic instability or pulmonary hypertension associatedith right heart abnormalities benefit considerably by restoring normalutflow from the right ventricle.202 Ideally, the goal of therapy in patientsith large pulmonary emboli is to improve/restore normal cardiopulmo-ary hemodynamics, thereby avoiding chronic thromboembolic pulmo-ary hypertension with its associated morbidity and mortality. Pengo andolleagues77 reported that within 2 years of a first episode of PE, almost% of patients developed chronic thromboembolic pulmonary hyperten-ion. Unquestionably, this percentage will increase in patients with largeulmonary emboli. Chronic thromboembolic pulmonary hypertension isssociated with recurrent PE, younger age at onset, large perfusionefects, and idiopathic PE. Pulmonary emboli that cause right ventricularysfunction are associated with a 6-fold increase in hospital mortality and.4-fold increase in 1-year mortality following discharge.203 Surgicalulmonary embolectomy can reduce thromboembolic pulmonary hyper-ension. The operative mortality rate for pulmonary thromboembolectomyor massive PE has diminished, with contemporary reports indicating thathere remains a definitive role for operative pulmonary embolectomy inatients who do not have other options to open their occluded pulmonaryrteries.204,205
Intravenous infusion of thrombolytic agents decreases mortality, im-roves right ventricular function, improves pulmonary function, andecreases chronic thromboembolic pulmonary hypertension as well aseducing recurrent venous thromboembolic disease206-217 (Fig 7). Gold-aber and colleagues202 showed rapid improvement in right ventricularunction, reduction in end diastolic right ventricular area, improvedulmonary perfusion, and reduction in recurrent PE when patients werereated with recombinant tissue plasminogen activator (rt-PA) comparedith heparin. Konstantinides and colleagues218 reported the results of a
arge international PE registry and showed that 30-day mortality wasower in patients receiving lytic therapy and that primary thrombolysisas the only independent predictor of survival on multivariate analysis.owever, not all patients with major pulmonary emboli are candidates for
ystemic thrombolytic therapy. Several authors have recently reportedmproved outcomes in patients treated with catheter-based thrombusspiration, maceration, fragmentation, and power-pulse infusion of plas-inogen activators175,219-256 (Table 9).Improvements in catheter-based techniques, with power-pulse infusionf plasminogen activators into proximally occluding pulmonary emboliith mechanical fragmentation, rapidly reduce pulmonary hypertension,
hereby improving patient oxygenation and cardiopulmonary hemody-
82 Curr Probl Surg, December 2008

ntib
S
terwart
Fo
C
amics (Fig 8). Lower doses of plasminogen activators pulsed into thehrombus promote subsequent lysis of the fragmented thrombus trappedn the proximal pulmonary artery as a result of the plasminogen activatorinding to fibrin-bound plasminogen.
ummary: Pulmonary EmbolismPatients with pulmonary emboli that raise pulmonary artery pressures to
he point of affecting right ventricular function have a markedly increasedarly and long-term mortality, increased risk of recurrence, and increasedisk of chronic thromboembolic pulmonary hypertension. All patientsith PE should undergo cardiac echocardiography to assess pulmonary
rtery pressure and right heart function. Patients with abnormalities ofight heart function should be considered for systemic thrombolytic
IG 8. Treatment algorithm for patients with pulmonary embolism. (Color version of figure is availablenline.)
herapy or catheter-based fragmentation with thrombolysis or operative
urr Probl Surg, December 2008 883

p(
8
ulmonary embolectomy, as suggested by the PE management algorithmFig 8).201
REFERENCES1. Heit JA, Cohen AT, Anderson FJ. Estimated annual number of incident and
recurrent, non-fatal venous thromboembolism (VTE) events in the US. Blood2005;106.
2. Prandoni P, Lensing AW, Prins MR. Long-term outcomes after deep venousthrombosis of the lower extremities. Vasc Med 1998;3:57-60.
3. Bauer KA, Rosendaal FR, Heit JA. Hypercoagulability: too many tests, too muchconflicting data. Hematology Am Soc Hematol Educ Program 2002:353-68.
4. Henke P. Vascular thrombosis due to hypercoagulable states. Rutherford’s Text-book of Vascular Surgery. 6th ed. Philadelphia, PA: Elsevier Saunders, 2004:568-78.
5. Andreotti F, Becker RC. Atherothrombotic disorders: new insights from hematol-ogy. Circulation 2005;111:1855-63.
6. Stewart GJ. Neutrophils and deep venous thrombosis. Haemostasis 1993;23(suppl1):127-40.
7. Wakefield TW, Myers DD, Henke PK. Mechanisms of venous thrombosis andresolution. Arterioscler Thromb Vasc Biol 2008;28:387-91.
8. Myers DD Jr, Schaub R, Wrobleski SK, Londy FJ 3rd, Fex BA, Chapman AM,et al. P-selectin antagonism causes dose-dependent venous thrombosis inhibition.Thromb Haemost 2001;85:423-9.
9. Myers D, Wrobleski S, Londy F, Fex B, Hawley A, Schaub R, et al. New andeffective treatment of experimentally induced venous thrombosis with anti-inflammatory rPSGL-Ig. Thromb Haemost 2002;87:374-82.
10. Day SM, Reeve JL, Pedersen B, Farris DM, Myers DD, Im M, et al. Macrovascularthrombosis is driven by tissue factor derived primarily from the blood vessel wall.Blood 2005;105:192-8.
11. Wells PS, Anderson DR, Rodger M, Forgie M, Kearon C, Dreyer J, et al.Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N EnglJ Med 2003;349:1227-35.
12. Perkins JM, Magee TR, Galland RB. Phlegmasia caerulea dolens and venousgangrene. Br J Surg 1996;83:19-23.
13. Fowl RJ, Strothman GB, Blebea J, Rosenthal GJ, Kempczinski RF. Inappropriateuse of venous duplex scans: an analysis of indications and results. J Vasc Surg1996;23:881-5; discussion 885-6.
14. Douglas MG, Sumner DS. Duplex scanning for deep vein thrombosis: has itreplaced both phlebography and noninvasive testing? Semin Vasc Surg1996;9:3-12.
15. Guyatt GH, Cook DJ, Jaeschke R, Pauker SG, Schünemann HJ. Grades ofrecommendation for antithrombotic agents: American College of Chest PhysiciansEvidence-Based Clinical Practice Guidelines (8th ed). Chest 2008;133:123S-31S.
16. Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD, et al.Multidetector computed tomography for acute pulmonary embolism. N Engl J Med2006;354:2317-27.
17. Schellong SM, Schwarz T, Halbritter K, Beyer J, Siegert G, Oettler W, et al.
84 Curr Probl Surg, December 2008

C
Complete compression ultrasonography of the leg veins as a single test for thediagnosis of deep vein thrombosis. Thromb Haemost 2003;89:228-34.
18. Cornuz J, Ghali WA, Hayoz D, Stoianov R, Depairon M, Yersin B. Clinicalprediction of deep venous thrombosis using two risk assessment methods incombination with rapid quantitative D-dimer testing. Am J Med 2002;112:198-203.
19. Rectenwald JE, Myers DD Jr, Hawley AE, Longo C, Henke PK, Guire KE, et al.D-dimer, P-selectin, and microparticles: novel markers to predict deep venousthrombosis. A pilot study. Thromb Haemost 2005;94:1312-7.
20. The PIOPED Investigators. Value of the ventilation/perfusion scan in acutepulmonary embolism. Results of the prospective investigation of pulmonaryembolism diagnosis (PIOPED). JAMA 1990;263:2753-9.
21. Worsley DF, Alavi A. Comprehensive analysis of the results of the PIOPED Study.Prospective Investigation of Pulmonary Embolism Diagnosis Study. J Nucl Med1995;36:2380-7.
22. Remy-Jardin M, Remy J. Spiral CT angiography of the pulmonary circulation.Radiology 1999;212:615-36.
23. Prandoni P, Bernardi E. Upper extremity deep vein thrombosis. Curr Opin PulmMed 1999;5:222-6.
24. Hull RD, Raskob GE, Brant RF, Pineo GF, Valentine KA. Relation between thetime to achieve the lower limit of the APTT therapeutic range and recurrent venousthromboembolism during heparin treatment for deep vein thrombosis. Arch InternMed 1997;157:2562-8.
25. Douketis JD, Kearon C, Bates S, Duku EK, Ginsberg JS. Risk of fatal pulmonaryembolism in patients with treated venous thromboembolism. JAMA 1998;279:458-62.
26. Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. Thelong-term clinical course of acute deep venous thrombosis. Ann Intern Med1996;125:1-7.
27. Bates SM, Ginsberg JS. Clinical practice. Treatment of deep-vein thrombosis.N Engl J Med 2004;351:268-77.
28. van Den Belt AG, Prins MH, Lensing AW, Castro AA, Clark OA, Atallah AN,et al. Fixed dose subcutaneous low molecular weight heparins versus adjusted doseunfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev2008;3:CD001100.
29. Ageno W, Turpie AG. Low-molecular-weight heparin in the treatment of pulmo-nary embolism. Semin Vasc Surg 2000;13:189-93.
30. Hull RD, Pineo GF, Mah AF, Brant R. A randomized trial evaluating long-termlow-molecular-weight heparin therapy out-of-hospital versus warfarin sodiumcomparing the post-phlebotic outcomes at three months. Blood 2001;98:447A.
31. van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcuta-neous low molecular weight heparins versus adjusted dose unfractionated heparinfor venous thromboembolism. Cochrane Database Syst Rev 2004;4:CD001100.
32. Hyers TM, Agnelli G, Hull RD, Morris TA, Samama M, Tapson V, et al.Antithrombotic therapy for venous thromboembolic disease. Chest 2001;119(1suppl):176S-93S.
33. Prandoni P, Lensing AW, Prins MH, Bernardi E, Marchiori A, Bagatella P, et al.Residual venous thrombosis as a predictive factor of recurrent venous thromboem-
bolism. Ann Intern Med 2002;137:955-60.urr Probl Surg, December 2008 885

8
34. Hull RD, Marder VJ, Mah AF, Biel RK, Brant RF. Quantitative assessment ofthrombus burden predicts the outcome of treatment for venous thrombosis: asystematic review. Am J Med 2005;118:456-64.
35. Cosmi B, Legnani C, Cini M, Guazzaloca G, Palareti G. D-dimer levels incombination with residual venous obstruction and the risk of recurrence afteranticoagulation withdrawal for a first idiopathic deep vein thrombosis. ThrombHaemost 2005;94:969-74.
36. Palareti G, Cosmi B, Legnani C, Tosetto A, Brusi C, Iorio A, et al. D-dimer testingto determine the duration of anticoagulation therapy. N Engl J Med 2006;355:1780-9.
37. Ridker PM, Goldhaber SZ, Danielson E, Rosenberg Y, Eby CS, Deitcher SR, et al.Long-term, low-intensity warfarin therapy for the prevention of recurrent venousthromboembolism. N Engl J Med 2003;348:1425-34.
38. Kearon C, Ginsberg JS, Kovacs MJ, Anderson DR, Wells P, Julian JA, et al.Comparison of low-intensity warfarin therapy with conventional-intensity warfarintherapy for long-term prevention of recurrent venous thromboembolism. N EnglJ Med 2003;349:631-9.
39. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients takingoral anticoagulant therapy for venous thromboembolism: a meta-analysis. AnnIntern Med 2003;139:893-900.
40. Almeida JI, Coats R, Liem TK, Silver D. Reduced morbidity and mortality rates ofthe heparin-induced thrombocytopenia syndrome. J Vasc Surg 1998;27:309-14;discussion 315-16.
41. Greinacher A, Michels I, Mueller-Eckhardt C. Heparin-associated thrombocytopenia:the antibody is not heparin specific. Thromb Haemost 1992;67:545-9.
42. Alving BM. How I treat heparin-induced thrombocytopenia and thrombosis. Blood2003;101:31-7.
43. Baldwin ZK, Spitzer AL, Ng VL, Harken AH. Contemporary standards for thediagnosis and treatment of heparin-induced thrombocytopenia (HIT). Surgery2008;143:305-12.
44. Greinacher A, Volpel H, Janssens U, Hach-Wunderle V, Kemkes-Matthes B,Eichler P, et al. Recombinant hirudin (lepirudin) provides safe and effectiveanticoagulation in patients with heparin-induced thrombocytopenia: a prospectivestudy. Circulation 1999;99:73-80.
45. Kovacs MJ. Successful treatment of heparin induced thrombocytopenia (HIT) withfondaparinux. Thromb Haemost 2005;93:999-1000.
46. Lee AY, Levine MN, Baker RI, Bowden C, Kakkar AK, Prins M, et al.Low-molecular-weight heparin versus a coumarin for the prevention of recurrentvenous thromboembolism in patients with cancer. N Engl J Med 2003;349:146-53.
47. Bergqvist D, Agnelli G, Cohen AT, Eldor A, Nilsson PE, Le Moigne-Amrani A, etal. Duration of prophylaxis against venous thromboembolism with enoxaparin aftersurgery for cancer. N Engl J Med 2002;346:975-80.
48. van Dongen CJ. Once versus twice daily LMWH for the initial treatment of venousthromboembolism. Cochrane Database Syst Rev 2006;3:CD003074.
49. Merli G, Spiro TE, Olsson CG, Abildgaard U, Davidson BL, Eldor A, et al.Subcutaneous enoxaparin once or twice daily compared with intravenous unfrac-tionated heparin for treatment of venous thromboembolic disease. Ann Intern Med
2001;134:191-202.86 Curr Probl Surg, December 2008

C
50. Gross PL, Weitz JI. New anticoagulants for treatment of venous thromboembolism.Arterioscler Thromb Vasc Biol 2008;28:380-6.
51. Turpie AG, Bauer KA, Eriksson BI, Lassen MR. Fondaparinux vs enoxaparin forthe prevention of venous thromboembolism in major orthopedic surgery: ameta-analysis of 4 randomized double-blind studies. Arch Intern Med 2002;162:1833-40.
52. Wolozinsky M, Yavin YY, Cohen AT. Pharmacological prevention of venousthromboembolism in medical patients at risk. Am J Cardiovasc Drugs 2005;5:409-15.
53. Agnelli G, Bergqvist D, Cohen AT, Gallus AS, Gent M. Randomized clinical trialof postoperative fondaparinux versus perioperative dalteparin for prevention ofvenous thromboembolism in high-risk abdominal surgery. Br J Surg 2005;92:1212-20.
54. Eriksson BI, Lassen MR. Duration of prophylaxis against venous thromboembo-lism with fondaparinux after hip fracture surgery: a multicenter, randomized,placebo-controlled, double-blind study. Arch Intern Med 2003;163:1337-42.
55. Buller HR, Davidson BL, Decousus H, Gallus A, Gent M, Piovella F, et al.Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venousthrombosis: a randomized trial. Ann Intern Med 2004;140:867-73.
56. Buller HR, Davidson BL, Decousus H, Gallus A, Gent M, Piovella F, et al.Subcutaneous fondaparinux versus intravenous unfractionated heparin in the initialtreatment of pulmonary embolism. N Engl J Med 2003;349:1695-702.
57. Buller HR, Cohen AT, Davidson B, Decousus H, Gallus AS, Gent M, et al.Idraparinux versus standard therapy for venous thromboembolic disease. N EnglJ Med 2007;357:1094-104.
58. Spyropoulos AC. Investigational treatments of venous thromboembolism. ExpertOpin Investig Drugs 2007;16:431-40.
59. Agnelli G, Gallus A, Goldhaber SZ, Haas S, Huisman MV, Hull RD, et al.Treatment of proximal deep-vein thrombosis with the oral direct factor Xa inhibitorrivaroxaban (BAY 59-7939): the ODIXa-DVT (Oral Direct Factor Xa InhibitorBAY 59-7939 in Patients With Acute Symptomatic Deep-Vein Thrombosis) study.Circulation 2007;116:180-7.
60. Weitz JI, Hirsh J, Samama MM. New anticoagulant drugs: the Seventh ACCPConference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126(3suppl):265S-86S.
61. Saiah E, Soares C. Small molecule coagulation cascade inhibitors in the clinic. CurrTop Med Chem 2005;5:1677-95.
62. Greenfield LJ, Proctor MC. Twenty-year clinical experience with the Greenfieldfilter. Cardiovasc Surg 1995;3:199-205.
63. Berry RE, George JE, Shaver WA. Free-floating deep venous thrombosis. Aretrospective analysis. Ann Surg 1990;211:719-22; discussion 722-3.
64. Langan EM 3rd, Miller RS, Casey WJ 3rd, Carsten CG 3rd, Graham RM, TaylorSM. Prophylactic inferior vena cava filters in trauma patients at high risk: follow-upexamination and risk/benefit assessment. J Vasc Surg 1999;30:484-8.
65. Sugerman HJ, Sugerman EL, Wolfe L, Kellum JM Jr, Schweitzer MA, DeMaria EJ.Risks and benefits of gastric bypass in morbidly obese patients with severe venousstasis disease. Ann Surg 2001;234:41-6.
66. Chiou AC. Beside placement of IVC filters. Endovasc Today 2005;4:60-3.
urr Probl Surg, December 2008 887

8
67. Decousus H, Leizorovicz A, Parent F, Page Y, Tardy B, Girard P, et al. A clinicaltrial of vena caval filters in the prevention of pulmonary embolism in patients withproximal deep-vein thrombosis. Prevention du Risque d’Embolie Pulmonaire parInterruption Cave Study Group. N Engl J Med 1998;338:409-15.
68. Prandoni P, Lensing AW, Prins MH, Frulla M, Marchiori A, Bernardi E, et al.Below-knee elastic compression stockings to prevent the post-thromboticsyndrome: a randomized, controlled trial. Ann Intern Med 2004;141:249-56.
69. Aschwanden M, Labs KH, Engel H, Schwob A, Jeanneret C, Mueller-Brand J,et al. Acute deep vein thrombosis: early mobilization does not increase thefrequency of pulmonary embolism. Thromb Haemost 2001;85:42-6.
70. Partsch H. Ambulation and compression after deep vein thrombosis: dispellingmyths. Semin Vasc Surg 2005;18:148-52.
71. Henke P. Effect of venous thromboembolism on mortality costs, and length of stayin hospitalized medical patients. Circ 2005;111:e322.
72. Heit JA. Venous thromboembolism: disease burden, outcomes and risk factors. JThromb Haemost 2005;3:1611-7.
73. Anderson FA Jr, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA,Jovanovic B, et al. A population-based perspective of the hospital incidence andcase-fatality rates of deep vein thrombosis and pulmonary embolism. The Worces-ter DVT Study. Arch Intern Med 1991;151:933-8.
74. Anderson FA Jr, Zayaruzny M, Heit JA, Fidan D, Cohen AT, Anderson FA Jr,et al. Estimated annual numbers of US acute-care hospital patients at risk forvenous thromboembolism. [see comment]. Am J Hematol 2007;82:777-82.
75. Heit J, Cohen A, Anderson F. Estimated annual number of incident and recurrentnon-fatal and fatal venous thromboembolism (VTE) events in the US. Blood1995;106:Abstract 910.
76. Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR, Colwell CW, et al.Prevention of Venous Thromboembolism: the Seventh ACCP Conference onAntithrombotic and Thrombolytic Therapy. Chest 2004;126(3 suppl):338S-400S.
77. Pengo V, Lensing AWA, Prins MH, Marchiori A, Davidson BL, Tiozzo F, et al.Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronicthromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med2004;350:2257-64.
78. Prandoni P, Lensing AW, Prins MH, Frulla M, Marchiori A, Bernardi E, et al.Below-knee elastic compression stockings to prevent the post-thromboticsyndrome: a randomized, controlled trial. Ann Intern Med 2004;141:249-56.
79. Borow M, Goldson H. Postoperative venous thrombosis. Evaluation of fivemethods of treatment. Am J Surg 1981;141:245-51.
80. Borow M, Goldson HJ. Prevention of postoperative deep venous thrombosis andpulmonary emboli with combined modalities. Am Surg 1983;49:599-605.
81. Pesavento R, Bernardi E, Concolato A, Dalla Valle F, Pagnan A, Prandoni P.Postthrombotic syndrome. Semin Thromb Hemost 2006;32:744-51.
82. Heit JA. Venous stasis syndrome: the long-term burden of deep vein thrombosis.Hosp Med 2003;64:593-8.
83. Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. Thelong-term clinical course of acute deep venous thrombosis. Ann Intern Med
1996;125:1-7.88 Curr Probl Surg, December 2008

1
1
1
1
C
84. Puggioni A, Kalra M, Gloviczki P. Practical aspects of the postthromboticsyndrome. Dis Mon 2005;51:166-75.
85. Salinger MH, Feldman TE. Patent foramen ovale: the missing link between deepvenous thrombotic disease and embolic stroke. Dis Mon 2005;51:94-103.
86. Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ 3rd.Risk factors for deep vein thrombosis and pulmonary embolism: a population-basedcase-control study. Arch Intern Med 2000;160:809-15.
87. Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis Mon2005;51:70-8.
88. Heit JA, O’Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, et al.Relative impact of risk factors for deep vein thrombosis and pulmonary embolism:a population-based study. Arch Intern Med 2002;162:1245-8.
89. Sugerman HJ, Sugerman EL, Wolfe L, Kellum JM Jr, Schweitzer MA, DeMaria EJ.Risks and benefits of gastric bypass in morbidly obese patients with severe venousstasis disease. Ann Surg 2001;234:41-6.
90. Kroger K, Weiland D, Ose C, Neumann N, Weiss S, Hirsch C, et al. Risk factorsfor venous thromboembolic events in cancer patients. Ann Oncol 2006;17:297-303.
91. Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circula-tion 2003;107(23 suppl 1):I9-16.
92. Geerts WH, Heit JA, Clagett GP, Pineo GF, Colwell CW, Anderson FA Jr, et al.Prevention of venous thromboembolism. Chest 2001;119(1 suppl):132S-75S.
93. Kucher N, Koo S, Quiroz R, Cooper JM, Paterno MD, Soukonnikov B, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med 2005;352:969-77.
94. Zakai NA, Wright J, Cushman M. Risk factors for venous thrombosis in medicalinpatients: validation of a thrombosis risk score. J Thromb Haemost 2004;2:2156-61.
95. Kakkar VV. Prevention of fatal postoperative pulmonary embolism by low doses ofheparin. An international multicentre trial. Lancet 1975;2:45-51.
96. Collins R, Scrimgeour A, Yusuf S, Peto R. Reduction in fatal pulmonary embolismand venous thrombosis by perioperative administration of subcutaneous heparin.Overview of results of randomized trials in general, orthopedic, and urologicsurgery. N Engl J Med 1988;318:1162-73.
97. Geerts W. Antithrombotic and thrombolytic therapy. 8th Ed: ACCP Guidelines.Chest 2008;133:381S-451S.
98. Warkentin TE. Heparin-induced thrombocytopenia. Dis Mon 2005;51:141-9.99. Nurmohamed MT, Rosendaal FR, Buller HR, Dekker E, Hommes DW, Vanden-
broucke JP, et al. Low-molecular-weight heparin versus standard heparin in generaland orthopaedic surgery: a meta-analysis. Lancet 1992;340:152-6.
00. Leizorovicz A, Haugh MC, Chapuis FR, Samama MM, Boissel JP. Low molecularweight heparin in prevention of perioperative thrombosis. BMJ 1992;305:913-20.
01. Bergqvist D. Low molecular weight heparin for the prevention of venous throm-boembolism after abdominal surgery. Br J Surg 2004;91:965-74.
02. Haas S, Wolf H, Kakkar AK, Fareed J, Encke A. Prevention of fatal pulmonaryembolism and mortality in surgical patients: a randomized double-blind comparisonof LMWH with unfractionated heparin. Thromb Haemost 2005;94:814-19.
03. Rasmussen MS, Jorgensen LN, Wille-Jorgensen P, Nielsen JD, Horn A, Mohn AC,
et al. Prolonged prophylaxis with dalteparin to prevent late thromboembolicurr Probl Surg, December 2008 889

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
8
complications in patients undergoing major abdominal surgery: a multicenterrandomized open-label study. J Thromb Haemost 2006;4:2384-90.
04. Turpie AG, Eriksson BI, Bauer KA, Lassen MR. New pentasaccharides for theprophylaxis of venous thromboembolism: clinical studies. Chest 2003;124(6suppl):371S-8S.
05. Sigel B, Edelstein AL, Felix WR Jr, Memhardt CR. Compression of the deepvenous system of the lower leg during inactive recumbency. Arch Surg 1973;106:38-43.
06. Comerota AJ, Stewart GJ, Alburger PD, Smalley K, White JV. Operativevenodilation: a previously unsuspected factor in the cause of postoperative deepvein thrombosis. Surgery 1989;106:301-8; discussion 308-9.
07. Coleridge-Smith PD, Hasty JH, Scurr JH. Venous stasis and vein lumen changesduring surgery. Br J Surg 1990;77:1055-9.
08. Coleridge Smith PD, Hasty JH, Scurr JH. Deep vein thrombosis: effect of graduatedcompression stockings on distension of the deep veins of the calf. Br J Surg1991;78:724-6.
09. Wells PS, Lensing AW, Hirsh J. Graduated compression stockings in the preven-tion of postoperative venous thromboembolism. A meta-analysis. Arch Intern Med1994;154:67-72.
10. Amaragiri SV, Lees TA. Elastic compression stockings for the prevention of DVT.Cochrane Database Syst Rev 2008;3:CD001484.
11. Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al. Towardsevidence-based guidelines for the prevention of venous thromboembolism: systematicreviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesiaas thromboprophylaxis. Health Technol Assess 2005;9:iii-iv, ix-x, 1-78.
12. Benko T, Cooke EA, McNally MA, Mollan RA. Graduated compression stockings:knee length or thigh length. Clin Orthop Rel Res 2001;383:197-203.
13. Byrne B. Deep vein thrombosis prophylaxis: the effectiveness and implications ofusing below-knee or thigh-length graduated compression stockings. Heart Lung2001;30:277-84.
14. Kakkos SK, Griffin M, Geroulakos G, Nicolaides AN. The efficacy of a newportable sequential compression device (SCD Express) in preventing venous stasis.J Vasc Surg 2005;42:296-303.
15. Comerota AJ, Chouhan V, Harada RN, Sun L, Hosking J, Veermansunemi R, et al.The fibrinolytic effects of intermittent pneumatic compression: mechanism ofenhanced fibrinolysis. Ann Surg 1997;226:306-313; discussion 313-4.
16. Kessler CM, Hirsch DR, Jacobs H, MacDougall R, Goldhaber SZ. Intermittentpneumatic compression in chronic venous insufficiency favorably affects fibrino-lytic potential and platelet activation. Blood Coagul Fibrinolysis 1996;7:437-46.
17. Guyton DP, Khayat A, Husni EA, Schreiber H. Elevated levels of 6-keto-prostaglandin-F1a from a lower extremity during external pneumatic compression.Surg Gynecol Obstet 1988;166:338-42.
18. Summaria L, Caprini JA, McMillan R, Sandesara J, Axelrod CA, Mueller ME,et al. Relationship between postsurgical fibrinolytic parameters and deep veinthrombosis in surgical patients treated with compression devices. Am Surg1988;54:156-60.
19. Urbankova J, Quiroz R, Kucher N, Goldhaber SZ. Intermittent pneumatic com-
90 Curr Probl Surg, December 2008

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
C
pression and deep vein thrombosis prevention. A meta-analysis in postoperativepatients. Thromb Haemost 2005;94:1181-5.
20. Comerota AJ, Katz ML, White JV. Why does prophylaxis with external pneumaticcompression for deep vein thrombosis fail? Am J Surg 1992;164:265-8.
21. PEP. Prevention of pulmonary embolism and deep vein thrombosis with low doseaspirin: Pulmonary Embolism Prevention (PEP) Trial. Lancet 2000;355:1295-302.
22. Wille-Jorgensen P, Rasmussen MS, Andersen BR, Borly L. Heparins and mechan-ical methods for thromboprophylaxis in colorectal surgery. Cochrane Database SystRev 2003;4:CD001217.
23. Borow M, Goldson H. Postoperative venous thrombosis. Evaluation of fivemethods of treatment. Am J Surg 1981;141:245-51.
24. Woolson ST, Watt JM. Intermittent pneumatic compression to prevent proximaldeep venous thrombosis during and after total hip replacement. A prospective,randomized study of compression alone, compression and aspirin, and compressionand low-dose warfarin. J Bone Joint Surg Am 1991;73:507-12.
25. Bradley JG, Krugener GH, Jager HJ. The effectiveness of intermittent plantarvenous compression in prevention of deep venous thrombosis after total hiparthroplasty. J Arthroplasty 1993;8:57-61.
26. Ramos R, Salem BI, De Pawlikowski MP, Coordes C, Eisenberg S, Leidenfrost R.The efficacy of pneumatic compression stockings in the prevention of pulmonaryembolism after cardiac surgery. Chest 1996;109:82-5.
27. Silbersack Y, Taute BM, Hein W, Podhaisky H. Prevention of deep-vein thrombosisafter total hip and knee replacement. Low-molecular-weight heparin in combinationwith intermittent pneumatic compression. J Bone Joint Surg 2004;86:809-12.
28. Eisele R, Kinzl L, Koelsch T. Rapid-inflation intermittent pneumatic compressionfor prevention of deep venous thrombosis. J Bone Joint Surg Am 2007;89:1050-6.
29. Westrich GH, Bottner F, Windsor RE, Laskin RS, Haas SB, Sculco TP. VenaFlowplus Lovenox vs VenaFlow plus aspirin for thromboembolic disease prophylaxis intotal knee arthroplasty. J Arthroplasty 2006;21(6 suppl 2):139-43.
30. Turpie AG, Bauer KA, Caprini JA, Comp PC, Gent M, Muntz JE. Fondaparinuxcombined with intermittent pneumatic compression vs. intermittent pneumatic com-pression alone for prevention of venous thromboembolism after abdominal surgery: arandomized, double-blind comparison. J Thromb Haemost 2007;5:1854-61.
31. Amin A, Stemkowski S, Lin J, Yang G. Thromboprophylaxis rates in US medicalcenters: success or failure? J Thromb Haemost 2007;5:1610-16.
32. Caprini JA, Arcelus JI, Hoffman K, Mattern T, Laubach M, Size GP, et al.Prevention of venous thromboembolism in North America: results of a surveyamong general surgeons. J Vasc Surg 1994;20:751-8.
33. Cohen AT, Tapson VF, Bergmann JF, Goldhaber SZ, Kakkar AK, Deslandes B, etal. Venous thromboembolism risk and prophylaxis in the acute hospital care setting(ENDORSE study): a multinational cross-sectional study. Lancet 2008;371:387-94.
34. Warwick D, Friedman R, Agnelli G, et al. Global orthopedic registry (GLORY).J Bone Joint Surg Br 2007;89:1409.
35. Kahn SR, Hirsch A, Shrier I. Effect of postthrombotic syndrome on health-relatedquality of life after deep venous thrombosis. Arch Intern Med 2002;162:1144-8.
36. Kahn SR, Elman EA, Bornais C, Blostein M, Wells PS. Post-thrombotic syndrome,functional disability and quality of life after upper extremity deep venous
thrombosis in adults. Thromb Haemost 2005;93:499-502.urr Probl Surg, December 2008 891

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
8
37. Delis KT, Bountouroglou D, Mansfield AO. Venous claudication in iliofemoralthrombosis: long-term effects on venous hemodynamics, clinical status, and qualityof life. Ann Surg 2004;239:118-26.
38. O’Donnell TF Jr, Browse NL, Burnand KG, Thomas ML. The socioeconomiceffects of an iliofemoral venous thrombosis. J Surg Res 1977;22:483-8.
39. Akesson H, Brudin L, Dahlstrom JA, Eklof B, Ohlin P, Plate G. Venous functionassessed during a 5 year period after acute ilio-femoral venous thrombosis treatedwith anticoagulation. Eur J Vasc Surg 1990;4:43-8.
40. Comerota AJ, Gravett MH. Iliofemoral venous thrombosis. J Vasc Surg2007;46:1065-76.
41. Comerota AJ, Paolini D. Treatment of acute iliofemoral deep venous thrombosis:a strategy of thrombus removal. Eur J Vasc Endovasc Surg 2007;33:351-60;discussion 361-2.
42. Shull KC, Nicolaides AN, Fernandes E, Fernandes J, Miles C, Horner J, et al.Significance of popliteal reflux in relation to ambulatory venous pressure andulceration. Arch Surg 1979;114:1304-6.
43. Nicolaides A, Schull K, Fernandes E. Ambulatory venous pressure: new informa-tion. In: Nicolaides AN, Yao JS, eds. Investigation of Vascular Disorders. NewYork: Churchill Livingston; 1981:488-94.
44. Welkie JF, Comerota AJ, Katz ML, Aldridge SC, Kerr RP, White JV. Hemody-namic deterioration in chronic venous disease. J Vasc Surg 1992;16:733-40.
45. Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr. Relationship betweenchanges in the deep venous system and the development of the postthromboticsyndrome after an acute episode of lower limb deep vein thrombosis: a one- tosix-year follow-up. J Vasc Surg 1995;21:307-12; discussion 313.
46. Meissner MH, Manzo RA, Bergelin RO, Markel A, Strandness DE Jr. Deep venousinsufficiency: the relationship between lysis and subsequent reflux. J Vasc Surg1993;18:596-605; discussion 606-8.
47. Cho JS, Martelli E, Mozes G, Miller VM, Gloviczki P. Effects of thrombolysis andvenous thrombectomy on valvular competence, thrombogenicity, venous wallmorphology, and function. J Vasc Surg 1998;28:787-99.
48. Rhodes JM, Cho JS, Gloviczki P, Mozes G, Rolle R, Miller VM. Thrombolysis forexperimental deep venous thrombosis maintains valvular competence and vasore-activity. J Vasc Surg 2000;31:1193-205.
49. Johnson BF, Manzo RA, Bergelin RO, Strandness DEJ. Relationship betweenchanges in the deep venous system and the development of the postthromboticsyndrome after an acute episode of lower limb deep vein thrombosis: a one- tosix-year follow-up. J Vasc Surg 1995;21:307-13.
50. Markel A, Manzo RA, Bergelin RO, Strandness DE Jr. Valvular reflux after deepvein thrombosis: incidence and time of occurrence. J Vasc Surg 1992;15:377-82;discussion 383-4.
51. Bjarnason H, Kruse JR, Asinger DA, Nazarian GK, Dietz CA Jr, Caldwell MD,et al. Iliofemoral deep venous thrombosis: safety and efficacy outcome during 5 yearsof catheter-directed thrombolytic therapy. J Vasc Interv Radiol 1997;8:405-18.
52. Mewissen MW, Seabrook GR, Meissner MH, Cynamon J, Labropoulos N,Haughton SH. Catheter-directed thrombolysis for lower extremity deep venousthrombosis: report of a national multicenter registry. Radiology 1999;211:39-49.
53. Comerota AJ, Throm RC, Mathias SD, Haughton S, Mewissen M. Catheter-
92 Curr Probl Surg, December 2008

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
C
directed thrombolysis for iliofemoral deep venous thrombosis improveshealth-related quality of life. J Vasc Surg 2000;32:130-7.
54. Plate G, Einarsson E, Ohlin P, Jensen R, Qvarfordt P, Eklof B. Thrombectomy withtemporary arteriovenous fistula: the treatment of choice in acute iliofemoral venousthrombosis. J Vasc Surg 1984;1:867-76.
55. Plate G, Akesson H, Einarsson E, Ohlin P, Eklof B. Long-term results of venousthrombectomy combined with a temporary arterio-venous fistula. Eur J Vasc Surg1990;4:483-9.
56. Plate G, Eklof B, Norgren L, Ohlin P, Dahlstrom JA. Venous thrombectomy foriliofemoral vein thrombosis—10-year results of a prospective randomized study.Eur J Vasc Endovasc Surg 1997;14:367-374.
57. Elsharawy M, Elzayat E. Early results of thrombolysis vs anticoagulation iniliofemoral venous thrombosis. A randomised clinical trial. Eur J Vasc EndovascSurg 2002;24:209-14.
58. Buller HR, Agnelli G, Hull RD, Hyers TM, Prins MH, Raskob GE. AntithromboticTherapy for Venous Thromboembolic Disease: the Seventh ACCP Conference onAntithrombotic and Thrombolytic Therapy. Chest 2004;126(3 suppl):401S-28S.
59. Martinez J PD, Comerota AJ. Chest and abdominopelvic CT scans are importanttools for evaluating patients with iliofemoral venous thrombosis. J Vasc Surg 2008.In press.
60. Plate G, Eklof B, Norgren L, Ohlin P, Dahlstrom JA. Venous thrombectomy foriliofemoral vein thrombosis—10-year results of a prospective randomised study.Eur J Vasc Endovasc Surg 1997;14:367-74.
61. Eklof B, Juhan C. Revival of thromboectomy in the management of acuteiliofemoral venous thrombosis. Contemp Surg 1992;40:21.
62. Piquet P. Traitement chirurgical des thromboses iliocaves: exigences et resultats.In: Kieffer E, ed. Chirurgie de la Veine Cave Inferieure et de Ses Branches. Paris:Expansion Scientifique Francaise; 1985:210-6.
63. Einarsson E, Albrechtsson U, Eklof B. Thrombectomy and temporary AV-fistula iniliofemoral vein thrombosis. Technical considerations and early results. Int Angiol1986;5:65-72.
64. Vollmar JF. Robert May Memorial Lecture: Advances in reconstructive venoussurgery. Int Angiol 1986;5:117-29.
65. Juhan C, Alimi Y, Di Mauro P, Hartung O. Surgical venous thrombectomy.Cardiovasc Surg 1999;7:586-90.
66. Torngren S, Swedenborg J. Thrombectomy and temporary arterio-venous fistula forilio-femoral venous thrombosis. Int Angiol 1988;7:14-8.
67. Rasmussen A, Mogensen K, Nissen FH, Wadt J, Skibsted L. [Acute iliofemoralvenous thrombosis. 26 cases treated with thrombectomy, temporary arteriovenousfistula and anticoagulants]. Ugeskr Laeger 1990;152:2928-30.
68. Eklof B, Kistner RL. Is there a role for thrombectomy in iliofemoral venousthrombosis? Semin Vasc Surg 1996;9:34-45.
69. Neglen P, al-Hassan HK, Endrys J, Nazzal MM, Christenson JT, Eklof B.Iliofemoral venous thrombectomy followed by percutaneous closure of the tempo-rary arteriovenous fistula. Surgery 1991;110:493-9.
70. Meissner AJ, Huszcza S. Surgical strategy for management of deep venousthrombosis of the lower extremities. World J Surg 1996;20:1149-55.
71. Pillny M, Sandmann W, Luther B, Muller BT, Tutschek B, Gerhardt A, et al. Deep
urr Probl Surg, December 2008 893

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
8
venous thrombosis during pregnancy and after delivery: indications for and resultsof thrombectomy. J Vasc Surg 2003;37:528-32.
72. Ganger KH, Nachbur BH, Ris HB, Zurbrugg H. Surgical thrombectomy versusconservative treatment for deep venous thrombosis; functional comparison oflong-term results. Eur J Vasc Surg 1989;3:529-38.
73. Kniemeyer HW, Sandmann W, Schwindt C, Grabitz K, Torsello G, Stuhmeier K.Thrombectomy with arteriovenous fistula for embolizing deep venous thrombosis:an alternative therapy for prevention of recurrent pulmonary embolism. TheClinical Investigator 1993;72:40-5.
74. Comerota AJ, Gale SS. Technique of contemporary iliofemoral and infrainguinalvenous thrombectomy. J Vasc Surg 2006;43:185-91.
75. Comerota A, Gale SS. Operative venous thrombectomy. In: Bergan JJ, ed. TheVein Book. San Diego: Elsevier; 2006:405-16.
76. Goldhaber SZ, Buring JE, Lipnick RJ, Hennekens CH. Pooled analyses ofrandomized trials of streptokinase and heparin in phlebographically documentedacute deep venous thrombosis. Am J Med 1984;76:393-7.
77. Elliot MS, Immelman EJ, Jeffery P, Benatar SR, Funston MR, Smith JA, et al. Acomparative randomized trial of heparin versus streptokinase in the treatment ofacute proximal venous thrombosis: an interim report of a prospective trial. Br JSurg 1979;66:838-43.
78. Arnesen H, Hoiseth A, Ly B. Streptokinase or heparin in the treatment of deep veinthrombosis. Follow-up results of a prospective study. Acta Med Scand 1982;211:65-8.
79. Jeffery P, Immelman EJ, Moore J. Treatment of deep vein thrombosis with heparinor streptokinase: long-term venous function assessment. Proceedings of the SecondInternational Vascular Symposium. 1989; Abstract N. S20.3.
80. Semba CP, Dake MD. Iliofemoral deep venous thrombosis: aggressive therapy withcatheter-directed thrombolysis. Radiology 1994;191:487-94.
81. Semba CP, Dake MD. Catheter-directed thrombolysis for iliofemoral venousthrombosis. Semin Vasc Surg 1996;9:26-33.
82. Verhaeghe R, Stockx L, Lacroix H, Vermylen J, Baert AL. Catheter-directed lysisof iliofemoral vein thrombosis with use of rt-PA. Eur Radiol 1997;7:996-1001.
83. Horne MK 3rd, Mayo DJ, Cannon RO 3rd, Chen CC, Shawker TH, Chang R.Intraclot recombinant tissue plasminogen activator in the treatment of deep venousthrombosis of the lower and upper extremities. Am J Med 2000;108:251-5.
84. Kasirajan K, Gray B, Ouriel K. Percutaneous AngioJet thrombectomy in themanagement of extensive deep venous thrombosis. J Vasc Interv Radiol 2001;12:179-85.
85. AbuRahma AF, Perkins SE, Wulu JT, Ng HK. Iliofemoral deep vein thrombosis:conventional therapy versus lysis and percutaneous transluminal angioplasty andstenting. Ann Surg 2001;233:752-60.
86. Vedantham S, Vesely TM, Parti N, Darcy M, Hovsepian DM, Picus D. Lowerextremity venous thrombolysis with adjunctive mechanical thrombectomy. J VascInterv Radiol 2002;13:1001-8.
87. Castaneda F, Li R, Young K, Swischuk JL, Smouse B, Brady T. Catheter-directedthrombolysis in deep venous thrombosis with use of reteplase: immediate resultsand complications from a pilot study. J Vasc Interv Radiol 2002;13:577-80.
88. Grunwald MR, Hofmann LV. Comparison of urokinase, alteplase, and reteplase for
94 Curr Probl Surg, December 2008

1
1
1
1
1
1
1
1
1
1
1
2
2
2
C
catheter-directed thrombolysis of deep venous thrombosis. J Vasc Interv Radiol2004;15:347-52.
89. Laiho MK, Oinonen A, Sugano N, Harjola VP, Lehtola AL, Roth WD, et al.Preservation of venous valve function after catheter-directed and systemic throm-bolysis for deep venous thrombosis. Eur J Vasc Endovasc Surg 2004;28:391-6.
90. Sillesen H, Just S, Jorgensen M, Baekgaard N. Catheter directed thrombolysis fortreatment of ilio-femoral deep venous thrombosis is durable, preserves venousvalve function and may prevent chronic venous insufficiency. Eur J Vasc EndovascSurg 2005;30:556-62.
91. Jackson LS, Wang XJ, Dudrick SJ, Gersten GD. Catheter-directed thrombolysisand/or thrombectomy with selective endovascular stenting as alternatives tosystemic anticoagulation for treatment of acute deep vein thrombosis. Am J Surg2005;190:864-8.
92. Ogawa T, Hoshino S, Midorikawa H, Sato K. Intermittent pneumatic compressionof the foot and calf improves the outcome of catheter-directed thrombolysis usinglow-dose urokinase in patients with acute proximal venous thrombosis of the leg.J Vasc Surg 2005;42:940-4.
93. Kim HS, Patra A, Paxton BE, Khan J, Streiff MB. Adjunctive percutaneousmechanical thrombectomy for lower-extremity deep vein thrombosis: clinical andeconomic outcomes. J Vasc Interv Radiol 2006;17:1099-104.
94. Lin PH, Zhou W, Dardik A, Mussa F, Kougias P, Hedayati N, et al. Catheter-directthrombolysis versus pharmacomechanical thrombectomy for treatment of symp-tomatic lower extremity deep venous thrombosis. Am J Surg 2006;192:782-8.
95. Protack CD, Bakken AM, Patel N, Saad WE, Waldman DL, Davies MG.Long-term outcomes of catheter directed thrombolysis for lower extremity deepvenous thrombosis without prophylactic inferior vena cava filter placement. J VascSurg 2007;45:992-7; discussion 997.
96. Goldenberg NA, Durham JD, Knapp-Clevenger R, Manco-Johnson MJ. A throm-bolytic regimen for high-risk deep venous thrombosis may substantially reduce therisk of postthrombotic syndrome in children. Blood 2007;110:45-53.
97. Enden T, Sandvik L, Klow NE, Hafsahl G, Holme PA, Holmen LO, et al.Catheter-directed venous thrombolysis in acute iliofemoral vein thrombosis—theCaVenT study: rationale and design of a multicenter, randomized, controlled,clinical trial (NCT00251771). Am Heart J 2007;154:808-14.
98. Vedantham S, Vesely TM, Parti N, Darcy M, Hovsepian DM, Picus D. Lowerextremity venous thrombolysis with adjunctive mechanical thrombectomy. J VascInterv Radiol 2002;13:1001-8.
99. Martinez J CA, Kazanjian S, DiSalle RS, Sepanski DM, Assi A. The quantitativebenefit of isolated, segmental, pharmacomechanical thrombolysis for iliofemoralDVT. J Vasc Surg 2008. In press.
00. Parikh S, Motarjeme A, McNamara T, Raabe R, Hagspiel K, Benenati JF, et al.Ultrasound-accelerated thrombolysis for the treatment of deep vein thrombosis:initial clinical experience. J Vasc Interv Radiol 2008;19:521-8.
01. Kearon C, Kahn SR, Agnelli G, Goldhaber SZ, Raskob G, Comerota AJ.Antithrombotic Therapy for Venous Thromboembolic Disease: ACCP Evidence-Based Clinical Practice Guidelines (8th ed). Chest 2008;133(6 Suppl):454S-545S.
02. Goldhaber SZ, Haire WD, Feldstein ML, Miller M, Toltzis R, Smith JL, et al.
urr Probl Surg, December 2008 895

2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
8
Alteplase versus heparin in acute pulmonary embolism: randomised trial assessingright-ventricular function and pulmonary perfusion. Lancet 1993;341:507-11.
03. Ribeiro A, Lindmarker P, Juhlin-Dannfelt A, Johnsson H, Jorfeldt L. Echocardi-ography Doppler in pulmonary embolism: right ventricular dysfunction as apredictor of mortality rate. Am Heart J 1997;134:479-87.
04. Aklog L, Williams CS, Byrne JG, Goldhaber SZ. Acute pulmonary embolectomy:a contemporary approach. Circulation 2002;105:1416-9.
05. Yalamanchili K, Fleisher AG, Lehrman SG, Axelrod HI, Lafaro RJ, SarabuMR, et al. Open pulmonary embolectomy for treatment of major pulmonaryembolism. Ann Thorac Surg 2004;77:819-23; discussion 823.
06. Agnelli G, Becattini C, Kirschstein T. Thrombolysis vs heparin in the treatment ofpulmonary embolism: a clinical outcome-based meta-analysis. Arch Intern Med2002;162:2537-41.
07. Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Heparin plusalteplase compared with heparin alone in patients with submassive pulmonaryembolism. N Engl J Med 2002;347:1143-50.
08. The urokinase pulmonary embolism trial. A national cooperative study. Circulation1973;47(2 suppl):II1-108.
09. Dong B, Jirong Y, Liu G, Wang Q, Wu T. Thrombolytic therapy for pulmonaryembolism. Cochrane Database Syst Rev 2006;2:CD004437.
10. Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared withheparin for the initial treatment of pulmonary embolism: a meta-analysis of therandomized controlled trials. Circulation 2004;110:744-9.
11. Dalla-Volta S, Palla A, Santolicandro A, Giuntini C, Pengo V, Visioli O, et al.PAIMS 2: alteplase combined with heparin versus heparin in the treatment of acutepulmonary embolism. Plasminogen activator Italian multicenter study 2. J Am CollCardiol 1992;20:520-6.
12. Dotter C, Seaman AJ, Rosch J, Porter J. Streptokinase and heparin in the treatmentof pulmonary embolism: a randomized comparison. Vasc Endovascular Surg 1979;13:42-52.
13. Jerjes-Sanchez C, Ramirez-Rivera A, de Lourdes Garcia M, Arriaga-Nava R,Valencia S, Rosado-Buzzo A, et al. Streptokinase and heparin versus heparin alonein massive pulmonary embolism: A randomized controlled trial. J ThrombThrombolysis 1995;2:227-9.
14. Ly B, Arnesen H, Eie H, Hol R. A controlled clinical trial of streptokinase andheparin in the treatment of major pulmonary embolism. Acta Med Scand1978;203:465-70.
15. Tibbutt DA, Davies JA, Anderson JA, Fletcher EW, Hamill J, Holt JM, et al.Comparison by controlled clinical trial of streptokinase and heparin in treatment oflife-threatening pulmonary embolism. BMJ 1974;1:343-7.
16. Tissue plasminogen activator for the treatment of acute pulmonary embolism. Acollaborative study by the PIOPED Investigators. Chest 1990;97:528-33.
17. Urokinase Pulmonary Embolism Trial Study Group. Urokinase pulmonary embo-lism trial: phase I result. JAMA 1970;214:2163-72.
18. Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser K, Rauber K, et al.Association between thrombolytic treatment and the prognosis of hemodynamicallystable patients with major pulmonary embolism: results of a multicenter registry.
Circulation 1997;96:882-8.96 Curr Probl Surg, December 2008

2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
C
19. Greenfield LJ, Bruce TA, Nichols NB. Transvenous pulmonary embolectomy bycatheter device. Ann Surg 1971;174:881-6.
20. Scoggins WG, Greenfield LJ. Transvenous pulmonary embolectomy for acutemassive pulmonary embolism. Chest 1977;71:213-6.
21. Greenfield LJ, Zocco JJ. Intraluminal management of acute massive pulmonarythromboembolism. J Thorac Cardiovasc Surg 1979;77:402-10.
22. Moore JH Jr, Koolpe HA, Carabasi RA, Yang SL, Jarrell BE. Transvenous catheterpulmonary embolectomy. Arch Surg 1985;120:1372-5.
23. Nakasaki Y, Tsujiyama S, Higo M, Yamamoto M, Yamashina H, Fujii T, et al. [Acase of acute massive pulmonary embolism successfully treated with transvenouspulmonary embolectomy by catheter]. Kokyu to junkan 1989;37:1363-6.
24. Timsit JF, Reynaud P, Meyer G, Sors H. Pulmonary embolectomy by catheterdevice in massive pulmonary embolism. Chest 1991;100:655-8.
25. Greenfield LJ, Proctor MC, Williams DM, Wakefield TW. Long-term experiencewith transvenous catheter pulmonary embolectomy. J Vasc Surg 1993;18:450-7;discussion 457-8.
26. Hiramatsu S, Ogihara A, Kitano Y, Mashiko M, Iseki S, Muramatsu J, et al.[Clinical outcome of catheter fragmentation and aspiration therapy in patients withacute pulmonary embolism]. J Cardiol 1999;34:71-8.
27. Tajima H, Murata S, Kumazaki T, Nakazawa K, Kawamata H, Fukunaga T, et al.Manual aspiration thrombectomy with a standard PTCA guiding catheter for treatmentof acute massive pulmonary thromboembolism. Radiat Med 2004;22:168-72.
28. Koning R, Cribier A, Gerber L, Eltchaninoff H, Tron C, Gupta V, et al. A newtreatment for severe pulmonary embolism: percutaneous rheolytic thrombectomy.Circulation 1997;96:2498-500.
29. Voigtlander T, Rupprecht HJ, Nowak B, Post F, Mayer E, Stahr P, et al. Clinicalapplication of a new rheolytic thrombectomy catheter system for massive pulmo-nary embolism. Catheter Cardiovasc Interv 1999;47:91-6.
30. Zeni PT Jr, Blank BG, Peeler DW. Use of rheolytic thrombectomy in treatment ofacute massive pulmonary embolism. J Vasc Interv Radiol 2003;14:1511-5.
31. Chiam P, Kwok V, Johan BA, Chan C. Major pulmonary embolism treated with arheolytic thrombectomy catheter. Singapore Med J 2005;46:479-82.
32. Siablis D, Karnabatidis D, Katsanos K, Kagadis GC, Zabakis P, et al. AngioJetrheolytic thrombectomy versus local intrapulmonary thrombolysis in massive pulmo-nary embolism: a retrospective data analysis. J Endovasc Ther 2005;12:206-14.
33. Chauhan MS, Kawamura A. Percutaneous rheolytic thrombectomy for largepulmonary embolism: a promising treatment option. Catheter Cardiovasc Interv2007;70:121-8.
34. Margheri M, Vittori G, Vecchio S, Chechi T, Falchetti E, et al. Early and long-termclinical results of AngioJet rheolytic thrombectomy in patients with acute pulmo-nary embolism. Am J Cardiol 2008;101:252-8.
35. Brady AJ, Crake T, Oakley CM. Percutaneous catheter fragmentation and distaldispersion of proximal pulmonary embolus. Lancet 1991;338:1186-9.
36. Sigmund M, Rubart M, Vom Dahl J, Uebis R, Hanrath P. Successful treatment ofmassive pulmonary embolism by combined mechanical and thrombolytic therapy.J Interv Cardiol 1991;4:63-8.
37. Rafique M, Middlemost S, Skoularigis J, Sareli P. Simultaneous mechanical clot
urr Probl Surg, December 2008 897

2
2
2
2
2
2
2
2
2
2
2
2
2
2
8
fragmentation and pharmacologic thrombolysis in acute massive pulmonaryembolism. Am J Cardiol 1992;69:427-30.
38. Manthey J, Frohlich G, Mautner JP, Munderloh KH, Zimmermann R. [Mechanicalrecanalization and local thrombolysis in a patient with fulminant pulmonaryembolism and craniocerebral trauma]. Anasthesiol Intensivmed NotfallmedSchmerzther 1994;29:446-9.
39. Fava M, Loyola S, Flores P, Huete I. Mechanical fragmentation and pharmacologicthrombolysis in massive pulmonary embolism. J Vasc Interv Radiol 1997;8:261-6.
40. Stock KW, Jacob AL, Schnabel KJ, Bongartz G, Steinbrich W. Massive pulmonaryembolism: treatment with thrombus fragmentation and local fibrinolysis withrecombinant human-tissue plasminogen activator. Cardiovasc Intervent Radiol1997;20:364-8.
41. Schmitz-Rode T, Janssens U, Schild HH, Basche S, Hanrath P, Gunther RW.Fragmentation of massive pulmonary embolism using a pigtail rotation catheter.Chest 1998;114:1427-36.
42. Wong PS, Singh SP, Watson RD, Lip GY. Management of pulmonary thrombo-embolism using catheter manipulation: a report of four cases and review of theliterature. Postgrad Med J 1999;75:737-41.
43. Murphy JM, Mulvihill N, Mulcahy D, Foley B, Smiddy P, Molloy MP. Percuta-neous catheter and guidewire fragmentation with local administration of recombi-nant tissue plasminogen activator as a treatment for massive pulmonary embolism.Eur Radiol 1999;9:959-64.
44. Schmitz-Rode T, Janssens U, Duda SH, Erley CM, Gunther RW. Massivepulmonary embolism: percutaneous emergency treatment by pigtail rotation cath-eter. J Am Coll Cardiol 2000;36:375-80.
45. Schmitz-Rode T, Janssens U, Hanrath P, Gunther RW. Fragmentation of massivepulmonary embolism by pigtail rotation catheter: possible complication. Eur Radiol2001;11:2047-9.
46. Prokubovski VI, Kapranov SA, Bobrov B. Endovascular rotary fragmentation inthe treatment of massive pulmonary thromboembolism. Angiol Vasc Surg 2003;9:31-9.
47. Tajima H, Murata S, Kumazaki T, Nakazawa K, Abe Y, Komada Y, et al.Treatment of acute massive pulmonary thromboembolism: mechanical frag-mentation with a modified rotating pigtail catheter, local fibrinolytic therapy,and clot aspiration followed by systemic fibrinolytic therapy. AJR Am JRoentgenol 2004;183:589-95.
48. De Gregorio MA, Gimeno MJ, Mainar A, Herrera M, Tobio R, Alfonso R, et al.Mechanical and enzymatic thrombolysis for massive pulmonary embolism. J VascInterv Radiol 2002;13(2 pt 1):163-9.
49. Uflacker R, Strange C, Vujic I. Massive pulmonary embolism: preliminary resultsof treatment with the Amplatz thrombectomy device. J Vasc Interv Radiol1996;7:519-28.
50. Peuster M, Bertram H, Windhagen-Mahnert B, Paul T, Hausdorf G. [Mechan-ical recanalization of venous thrombosis and pulmonary embolism with theClotbuster thrombectomy system in a 12-year-old boy]. Z Kardiol 1998;87:283-7.
51. Muller-Hulsbeck S, Brossmann J, Jahnke T, Grimm J, Reuter M, Bewig B, et al.
98 Curr Probl Surg, December 2008

2
2
2
2
2
C
Mechanical thrombectomy of major and massive pulmonary embolism with use ofthe Amplatz thrombectomy device. Invest Radiol 2001;36:317-22.
52. Michalis LK, Tsetis DK, Rees MR. Case report: percutaneous removal ofpulmonary artery thrombus in a patient with massive pulmonary embolismusing the hydrolyser catheter: the first human experience. Clin Radiol 1997;52:158-61.
53. Fava M, Loyola S, Huete I. Massive pulmonary embolism: treatment with thehydrolyser thrombectomy catheter. J Vasc Interv Radiol 2000;11:1159-64.
54. Reekers JA, Baarslag HJ, Koolen MG, Van Delden O, van Beek EJ. Mechanicalthrombectomy for early treatment of massive pulmonary embolism. CardiovascIntervent Radiol 2003;26:246-50.
55. Rocek M, Peregrin J, Velimsky T. Mechanical thrombectomy of massive pulmo-nary embolism using an Arrow-Trerotola percutaneous thrombolytic device. EurRadiol 1998;8:1683-5.
56. Lang EV, Barnhart WH, Walton DL, Raab SS. Percutaneous pulmonary throm-bectomy. J Vasc Interv Radiol 1997;8:427-32.
urr Probl Surg, December 2008 899