Embed Size (px)
Citation preview

Pulmonary Embolism ALERT Think Fast, Act Together!™
Acute Pulmonary Embolism Therapies:Resource Guide

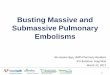
Example of a PE protocol roadmap - use of a roadmap such as this offers an effective and efficient care continuum for acute PE†
02
PE symptoms are recognized
Call the local emergency
service (EMS)
EMS assess
EMS identifies PE
EMS departs for the hospital
Primary PE center
Comprehensive PE center
Community Hospital
Go to ER
Pulmonary Embolism (PE) Protocol Roadmap

High risk
RV function (echo or CT) laboratory testing
Assess clinical risk (PESI or sPESI)
Shock / Hypotension?
Intermediate- high risk
Intermediate risk
Intermediate- low risk
Primary reperfusion
A/C; monitoring consider rescue
reperfusion
A/C; hospitalization
A/C; consider early discharge & home treatment,
if feasible
Low risk
Example of a PE protocol roadmap - use of a roadmap such as this offers an effective and efficient care continuum for acute PE†
Pulmonary Embolism (PE) Protocol Roadmap
† ESC Guidelines on the diagnosis and management of acute pulmonary embolism. European Heart Journal. doi:10.1093
Jaff M et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation 2011;123(16):1788-1830
Clinical suspicion of PE
Yes
PE Confirmed
PESI Class I-II or sPESI=0
PESI Class III-IV or sPESI≥1
Consider further risk stratification
Both positive
One positive or both negative
PE Confirmed
Diagnostic algorithm for suspected
high-risk PE
Diagnostic algorithm for
suspected not high-risk PE
No
03
Massive Sub-massive Sub-massive Minor

EKOS Corporation, a BTG International group company, is committed to advancing the treatment of acute pulmonary embolism (PE). Through technological innovation, such as Acoustic Pulse Thrombolysis™ treatment, and a comprehensive approach to clinical research, EKOS® is dedicated to improving patient outcomes. Our approach, however, extends beyond devices – our goal is to be your ally in improving the patient treatment pathway, from onset to recovery. The EKOS® team and our distribution partners are at your disposal to provide – and help implement – a series of programs to help your facility treat PE patients more safely and effectively.
EKOS CorporationA BTG International group company
04
Pulmonary Embolism ALERT Think Fast, Act Together!™

02 PE Protocol Roadmap 08 Pulmonology
06 What is Acute PE? 08 Internal/Vascular Medicine
06 Public Awareness 08 Other Specialties
07 Emergency Department 08 Administrators and Executives
07 PE Checklist 09 Circle Strategy
08 ICU/CCU 10 Product Description
08 Interventional Radiology 12 Clinical Studies
08 Interventional Cardiology 20 Professional Education Program
08 Vascular Surgery 22 References
05
Contents

What is Acute Pulmonary Embolism (PE)?
06
PE is a condition where one or more clots break off and travel from existing venous clots in the arms or legs in the circulatory system, getting trapped in the pulmonary arteries, where they can block blood flow and access to the lungs' vital oxygenation system. In intermediate-risk or high-risk cases, this may lead to a strain on the heart’s ability to pump blood through the lungs which can then lead to heart failure and/or cardiovascular collapse.
Common PE symptoms include:
• Shortness of breath
• Progressively worsening chest pain
• Cough
• Clammy or discoloured skin
• Excessive sweating
• Rapid or irregular heartbeat
• Lightheadedness or dizziness
Public Awareness
• Over 600,000 cases annually in the US2
• Responsible for more deaths in the EU each year than breast cancer and AIDS combined3,4
• PE causes or contributes to 15% of all hospital deaths5,6
• PE commonly originates from lower limb deep vein thrombosis (DVT)
• 79% of patients presenting with PE have evidence of DVT
• PE occurs in up to 50% of patients with proximal DVT
Annual incidence Venous thromboembolism1
15%
PEs can be immediately fatal. However, if PE can be diagnosed and appropriate therapy started, the mortality can be reduced from approximately 30 percent to less than 10 percent.1

07
Emergency Medical Services and Emergency Department
PE Alert Checklist Pre-hospital identification is a vital initial step in the emergency medical management of PE. A symptoms-based screening tool facilitates rapid, standardized, symptomatic clinical assessment. Based on the assessment, routing the acute PE patient to the most appropriate treatment facility which offers the latest therapies and interventional technologies, including the EKOS® system, will improve outcomes for patients.
Emergency Department When someone suffers an acute PE, recognizing symptoms, calling 911, response by EMS, and transportation to the Emergency Department with diagnostic and treatment capabilities can make a significant impact on a successful outcome.
Rapid assessment, knowing what level of PE care each hospital offers and whom to contact within the hospital are critical to optimizing an acute PE patient’s outcome. Developing an acute PE network, with incorporation of a PE Response Team (PERT) and implementation of a standardized critical care pathway is an innovative and effective treatment approach for acute PE.8
PE occurs in up to 50% of patients with proximal DVT
79% of patients presenting with PE have evidence of DVT

Specialties Involved in the PE Patient Pathway
08
ICU/CCU: Before and after placement of the EKOS® Device, a patient with PE (risk stratification: intermediate-high and high) is admitted to the Intensive Care Unit (ICU).
Interventional Radiologists, Interventional Cardiologists, and Vascular Surgeons: Placement of the EKOS® Device is usually done by an Interventional Radiologist, Interventional Cardiologist, or a Vascular Surgeon and their team. The procedure is carried out in the cath lab or angio lab under fluoroscopy. They use catheters and wires to navigate through the vasculature and usually place the EKOS® Device in the lower branch of the pulmonary artery.
Vascular Medicine: In some hospitals, Vascular Surgeons play a key role in the treatment of PE because of their diagnosis and treatment of DVT. A high number of PE patients have had a DVT. In many hospitals, Vascular Surgeons are part of the PERT program and place the EKOS® Device in PE patients.
Internal Medicine, Vascular Medicine, and Pulmonologists: Assessment of the status of a PE patient and decision on treatment is a multidisciplinary approach where other groups play a key role as well. Depending on the patient situation at onset, i.e. coming into the Emergency Department or already admitted to the hospital because of comorbidities, several doctors are included in the decision-making process.
To facilitate an easier decision-making process, a PERT approach has been shown to be beneficial to the patient. In this way, protocols have been prepared and discussed prior to the arrival of an acute PE patient.
Other Specialties: Orthopedists, Hematologists, and Oncologists can see patients who develop a PE due to the patient disease. They refer patients to the ICU or the PERT.
Administrators and Executives: Caring for patients suffering from PE takes a concerted effort of many medical specialties and technologies to optimize patient care. In order to have a successful PERT, the executive board must consider the following:
• Manpower
• Imaging and angiography equipment
• Intensive care unit
• Raising awareness for the new PERT program in the community
Building a comprehensive PE program center should be a collaborative effort involving the physicians, and should include measures of quality, resource utilization, efficiency, and market development. Benefits of committing to a PERT program include the ability to better serve the community and bring more patients into the institution.

PERT8
Emergency Department
Internal Medicine
Urgent CareUrgent Care
Vascular Medicine
ICU
Community Hospital
Primary Care
Community Hospital
Primary Care
Pulmonologists
EKOS® User*
Circle Strategy PE Referral Center and PE Response Team (PERT)
09* Interventional cardiologist, interventional radiologist or vascular surgeon.

The EKOS® system includes an Ultrasonic Core within an Infusion Catheter and the Control Unit.
Targeting the Thrombus, Safely With EKOS® Acoustic Pulse Thrombolysis™ treatment, most of the drug remains in the thrombus and typically, less lytic is used. It dissolves the thrombus, without damaging vessels, valves or walls.9,10 There is no mechanical disruption resulting in distal embolization.11
The EKOS® system’s safety and efficacy is supported by Level 1 and Level 2 data.12,13,14,15
Reduced Procedure Time16,17
EKOS® requires significantly shorter treatment times, typically only 33–50% of standard CDT. Unlike more complex surgical solutions,18,19 EKOS® is an efficient, three-step process:
1) Insert the EKOS® 5.4 F Infusion Catheter through the thrombus.
2) Insert the ultrasonic core and luer lock into place.
3) Activate the lytic infusion and begin Acoustic Pulse Thrombolysis™ treatment.
Ultrasonic CoreRadiopaque Marker
5.4 F Infusion Catheter
Therapy Optimization Sensor
Cross Section
Drug Delivery Lumen
Central Coolant LumenUltrasonic Core in
Central Lumen
At-a-glance user interface makes it easy to optimize
settings during lysis.
EKOS® System. Lower Patient Risk. Higher Procedure Predictability.
10
Therapy Optimization Sensor

Treatment zones range from 6cm to 50cm with radiopaque marker bands at each end of the treatment zone to enhance visualization. At-a-glance operating status, alarms and treatment times are easy to read from a distance.
EKOS® Acoustic Pulse Thrombolysis™ treatment is a minimally invasive system for dissolving thrombus. The Ultrasonic Core generates a localized acoustic field which greatly accelerates lytic dispersion by driving the drug deeper into the clot and unwinding the fibrin strands to expose plasminogen receptor sites.
Acoustic Pulse Thrombolysis™ Treatment: • Speeds time-to-dissolution
•Increases thrombus removal and clinical improvement compared to either standard Catheter Directed Therapy (CDT) or thrombectomy18,19
•Lowers the risk of bleeding and other complications17,18
More Effective Drug Delivery: • Reduces dosage requirements
by as much as 68% compared to standard CDT17
•Requires up to 4x less drug dosage than systemic delivery12,13
Superior Thrombus Clearance:16,17 • 48% greater drug absorption
within 1 hour20
•84% greater drug absorption within 2 hours20
The Acoustic Pulse Difference
The Thrombosis BarrierTightly wound fibrin strands prevent
lytic from reaching receptor sites
With Acoustic PulseUltrasonic energy thins fibrin strands
and exposes receptor sites
With Acoustic Pulse + LyticMore drug reaches entire thrombus,
accelerating absorption
11
Treatment Zone
Coolant

Randomized, Controlled Trial of Ultrasound-Assisted Catheter-Directed Thrombolysis for Acute Intermediate-Risk
Pulmonary Embolism Nils Kucher, MD et al. Circulation 2014; 129: 479-486
EKOS® PE Clinical Studies The ULTIMA TrialStudy Design
Patients Acute PE with RV/LV ratio ≥ 1.0
Methods
Infusion Protocol
• rtPA1mg/h;salinecoolant 35ml/h
• Patientsmonitoredinthe intermediate or ICU
• Afterfivehours,rtPAreduced to 0.5mg/h
• At15(+/-1)hours,rtPA infusion, saline coolant and ultrasound discontinued
• Removedintheintermediate or ICU
Randomization
29 patients
Unfractionated heparin
Unfractionated heparin*
•IVbolus:80IU/kg•Infusion:18IU/kg/hour
30 patients
Unfractionated heparin +
Ultrasound-assisted CDT using EKOS®
12
* Unfractionated heparin administered immediately after randomization

13
The ULTIMA Trial Key Results & Conclusion
1.5
1.0
0.5
1.28
0.99
1.20 1.17
RV/L
V Ra
tio
P<0.001P=0.31
24 hrs
EKOS® with tPA + Heparin Heparin
0.6
0.4
0.2
0.0
0.35
0.03
0.24
Redu
ctio
n in
RV/
LV R
atio
P=0.07
P<0.001
EKOS® with tPA + Heparin Heparin
0.30
EKOS® with tPA + HeparinN = 30
0 0%
0 0%
0 0%
3** 10%
HeparinN = 29
1* 0%
0 0%
0 0%
1 †3%
* Rehospitalization and death from advanced pancreatic cancer** Two patients with transient mild hemoptysis without medical intervention, one patient with groin hematoma requiring manual compression† One patient with transient anal bleeding following endoscopic removal of colon polyp
Conclusion: ULTIMA confirmed that a fixed-dose, ultrasound-assisted catheter-directed thrombolysis using EKOS® regimen was superior to anticoagulation alone in improving RV dysfunction at 24 hours without an increase in bleeding complications.
Baseline 24 hrs BaselineBaseline
to 90 daysBaseline to 24 hrs
Baselineto 90 days
Baseline to 24 hrs
100%
80%
60%
40%
20%
0%
Syst
olic
RV
Dys
func
tion
P=0.003*
P<0.001† P<0.001
Baseline 24hrs 90 days Baseline 24hrs 90 days
EKOS® with tPA + Heparin Heparin
SevereModerateMildNormal
* Two-sided exact Mantel-Haenzel test † Wilcoxon rank sum test
RV/LV ratio significantly improved at 24 hours
No deaths or significant bleeding complications
Reduction in RV/LV ratio significantly greater at 24 hours and improved at 90 days
Systolic RV dysfunction significantly improved
Clinical outcomes at 90 days
Death
Recurrent venous thromboembolism
Major bleeding
Minor bleeding
p-value
0.49
1.00
1.00
0.61

EKOS® PE Clinical Studies SEATTLE II trialStudy Design
Methods
Ultrasound-facilitated fibrinolysis using EKOS®
A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Low-Dose Fibrinolysis for
Acute Massive and Submassive Pulmonary Embolism G. Piazza MD, MS et al, JACC Cardiovasc Interv. 2015 Aug 24; 8(10): 1382-92
Patients Acute Massive and Submassive PE
with RV/LV ratio ≥ 0.9 (n = 150; 22 centers)
14
If unilateral PE:• tPA 1 mg/hr using one
EKOS® system for 24 hours
Follow up at 48 +/- 6 hours
• CT measurement of RV/LV ratio
• Echocardiogram to estimate PA systolic pressure
If bilateral PE:• tPA 1 mg/hr/per EKOS® system
(using two simultaneously) for 12 hours

15
SEATTLE II Trial Key Results & Conclusion
Conclusion: Ultrasound-facilitated, catheter-directed, low-dose fibrinolysis for acute PE improves RV function and decreases pulmonary hypertension and angiographic obstruction. By minimizing the risk of intracranial bleed, it represents a potential “game-changer” in the treatment of high-risk PE patients.
25% decrease in RV/LV ratio over 48 hours
Rapidly relieved pulmonary artery obstruction
Minimized risk of intracranial hemorrhage
Reduced pulmonary hypertension
2.0
1.5
1.0
0.5
0
RV/L
V Ra
tio
P<0.0001
Pre-Procedure 48 Hours
1.55
1.13
25
20
15
10
5
0
Mea
n M
odifi
ed M
iller
Sco
re
P<0.0001
Pre-Procedure 48 Hours
22.5
15.8
60
50
40
30
20
10
0Mea
n PA
Sys
tolic
Pre
ssur
e (m
mH
g)
P<0.0001
Pre-Procedure
Post-Procedure
51.4
37.5
48 Hours
36.9
P<0.0001
Intracranial Haemorrhage
(Fibrinolysis Group)
9/304 (3%)
10/506 (2%)
0/150 (0%)
Study
ICOPER(Goldhaber SZ, et al. 1999)
PEITHO(Meyer G, et al. 2014)
SEATTLE II(Piazza G, et al. 2014)

EKOS® PE Clinical Studies
16
Ultrasound-Accelerated Catheter-Directed Thrombolysis for Acute Submassive Pulmonary Embolism. J Vasc Interv Radiol 2015; 26(7): 1001-1006
A single-center, retrospective study (15 patients enrolled prospectively in SEATTLE II)
Authors/Investigators: Sandeep Bagla, MD, John B. Smirniotopoulos, MD, Arletta van Breda, MSN, Michael J. Sheridan, ScD, and Keith M. Sterling, MD from the Cardiovascular and Interventional Radiology department at Inova Alexandria Hospital in Alexandria, VA, USA
Objective: To evaluate the safety and efficacy of EKOS® treatment in patients with submassive PE.
Results: EKOS® treatment was technically successful in all 45 (100%) patients.
• A statistically significant decrease in PA pressure from an average of 49.8 mmHg to an average of 31.1 mmHg (p<.0001)
• There was complete concordance between PA pressures measured via the EKOS® catheter and the angiographic catheter in three patients who underwent measurements both ways
• A statistically significant decrease in RV:LV ratio from an average of 1.59 to 0.93 (p<.0001)
• No patient died through the 30-day follow up, and there were no 30-day readmissions for PE
• Four minor bleeding episodes at access sites
• Two major bleeding episodes – one patient had flank hematoma 3 days post-lysis possibly due to supratherapeutic anticoagulation, and one patient had major bleeding from a previous brachial artery blood-gas puncture site

A single-center retrospective review of 45 (26 men and 19 women) patients undergoing EKOS® treatment for acute massive or submassive PE between Jan 2011 – Dec 2013
Authors: Madeline Nykamp, Angela VandenHull, Tyler Remund PhD, Angelo Santos MD, Patrick Kelly MD, Greg Schultz MD, and Chad Laurich MD, of Sanford Vascular Associates in Sioux Falls, SD, USA
Objective: To evaluate the safety and effectiveness of ultrasound-accelerated thrombolysis in acute pulmonary embolism.
• Patients had either massive PE as evidenced by hemodynamic instability (defined as systolic bp <100 mm Hg; tachycardia >100 beats/min), or submassive PE defined as:
- right-heart strain evidenced by RV dilation, septal deviation, or hypokinesis
- right ventricle dilatation by CT scan or
- pulmonary hypertension by direct catheter measurement
• A separate “control group” of 45 intermediate to massive PE patients who were treated with systemic infusion of heparin or anticoagulation from 2011 to 2013 were randomly selected. Their charts were reviewed for similar demographic and baseline characteristics, periprocedural parameters, and follow-up information. This allowed for comparison of EKOS® treatment vs. heparin
Results: • The average length of hospital stay for the EKOS®-treated group was 3.2 days (± 2 SD), which was
significantly shorter when compared to 6.7 days (± 4.4 SD) for the anti-coagulation control group
• Survival in the EKOS® treated group when followed up to 2 years was significantly higher compared to the anti-coagulation control group
• No deaths through 90 days of follow-up and no major periprocedural bleeding events
• EKOS® treated patients received a total average rtPA dose of 30.5 mg (range 14-66 mg) over 14.2 hours (range, 8-21 hrs). However, over two-thirds (31) of patients did not receive a bolus of rtPA and received a total dose of 22.5 mg rtPA (range, 14-48 mg)
Safety and efficacy of ultrasound-accelerated catheter-directed lytic therapy in acute pulmonary embolism with and without hemodynamic instability. J Vasc Surg: Venous and Lymphatic Disorders 2015; 3(5): 251-7
17

Professional Education
18
Circle Strategy Programs
PE Center of Excellence Training
Annual Regional Network Meeting
Objective: Circle Strategy Programs are held to strengthen the relationship between the different teams in the Pulmonary Embolism care chain of your hospital. The development of regional networks that link primary care hospitals and physicians to comprehensive pulmonary embolism centers can help to improve patient outcomes.
Suggested topics to cover:• Patient flow and transfers from referring hospitals
• What is required from referring hospitals?
• Protocol discussion
• Endovascular treatment of pulmonary embolism
• Patient selection
• Intensive care
• Case discussions
• Management of complications
• Latest clinical data
Please contact your EKOS® Representative for more information.
Duration: 1 day
Sites: Coming Soon
Objective: • Educate interventionalists and other specialties on acute pulmonary embolism treatment and
considerations
• Develop/modify PE protocols – patient selection and diagnostics
• Workshop includes didactic presentations and review of clinical experience
This workshop is dedicated to teams of interventionalists and other specialties from the same hospital who want to initiate a PERT program in their center.
Please contact your EKOS® Representative for more information.

19
EKOS® User Meetings
EKOS® Scientific Exchange
Regional Pulmonary Embolism Updates
Objective: EKOS® Users Meetings are held regionally throughout the year to educate your team of interventionalists, ER staff, Cath Lab staff, ICU nurses and other specialties. The intent of the User Meetings is to learn from world renowned faculty who engage in a comprehensive approach to the treatment of Pulmonary Embolism – from symptom onset to recovery. Our esteemed faculty will identify rapid assessment, diagnosis, imaging, and treatment options from lytics and best-medical management, to best-practices around the use of the EKOS® system and Acoustic Pulse Thrombolysis™ therapy.
Suggested topics to cover:• Patient flow and transfers from referring hospitals
• Imaging in pulmonary embolism
• Patient selection (guidelines and risk stratification)
• Intensive care
• Latest clinical data
• Management of complications
• Case discussion
Please contact your EKOS ® Representative for more information.
Duration: 2 days
Sites: Bothell, WA
Objective:
• Production tour and discuss a PERT organization in a US hospital
• Gain more insight into the PE protocol, patient selection, patient workflow, imaging, and networking with specialties and surrounding hospitals, etc.
This workshop is dedicated to hospitals that want to improve their PE care care pathway.
Please contact your EKOS® Representative for more information.

EKOS, the EKOS logo and EkoSonic are registered trademarks and 'Think Fast, Act Together!' and Acoustic Pulse Thrombolysis are trademarks of EKOS Corporation, a BTG International group company. ’Imagine where we can go’, BTG and the BTG roundel logo are trademarks of BTG International Ltd. BTG and the BTG roundel logo are registered trademarks in the US, EU and certain other territories. All rights reserved. © 2016 EKOS Corporation. NA-EKO-2016-0546b.
1. Reporting standards for endovascular treatment of pulmonary embolism. Banovac, R et al. J Vasc Interv Radiol, 2010; 21: 44-53
2. Wood KE et al. Major pulmonary embolism: review of a pathphysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest 2002;121:877-905.
3. EuroStat 2010 – http://ec.europa.eu/eurostat/statistocs-explained/index.php/ Causes_of_death_statistics#Further_Eurostat_information
4. Venous thromboembolism (VTE) in Europe. The number of VTE events and associated morbidity and mortality. Cohen et al. Thromb Haemost, 2007; 98(4): 756-764
5. Goldhaber. Deep-vein thrombosis: Advancing awareness to protect patient lives. American Public Health Association White Paper. 2003
6. Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. Kasper et al. J Am Coll Cardiol, 1997; 30: 1165-1171
7. http://www.sirweb.org/patients/deep-vein-thrombosis (last verified February 2016)
8. Acute Pulmonary Embolism Network and Multidisciplinary Response Team Approach to Treatment. Bloomer, TL, Thomassee EJ, Fong PP; Critical Pathways in Cardiology, 2015; 14(3): 90-96
9. Ultrasound-Accelerated Thrombolysis for the Treatment of Deep Vein Thrombosis: Initial Clinical Experience. Parikh S et al. Journal of Vascular and Interventional Radiology, April 2008; 19(4): 521-528
10. Absence of Biological Damage from Prolonged Exposure to Intravascular Ultrasound: A Swine Model. Soltani A et al. Ultrasonics, 2007; (46): 60-67
11. Ultrasound Reversibly Disaggregates Fibrin Fibers. Braaten, JV et al. Journal of Thrombosis and Haemostasis, 1997; (78): 1063-8
12. The Ultima Trial, Randomized, Controlled Trial of Ultrasound-Assisted Catheter- Directed Thrombolysis for Acute Intermediate-Risk Pulmonary Embolism. Nils Kucher, MD et al., Circulation, 2014; 129: 479-486
13. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. Piazza G, Hohlfelder B, Jaff MR, Ouriel K, Engelhardt TC, Sterling KM, Jones NJ, Gurley JC, Bhatheja R, Kennedy RJ, Goswami N, Natarajan K, Rundback J, Sadiq IR, Liu SK, Bhalla N, Raja ML, Weinstock BS, Cynamon J, Elmasri FF, Garcia MJ, Kumar M, Ayerdi J, Soukas P, Kuo W, Liu PY, Goldhaber SZ; SEATTLE II Investigators.JACC Cardiovasc Interv, 2015; 8(10): 1382-92
14. Treatment of Critical Limb Ischemia Using Ultrasound-Enhanced Thrombolysis (PARES TRIAL):
Final Results. Wissgott C et al. Journal of Endovascular Therapy, 2007; 14(4): 438-443
15. Dutch Randomized Trial Comparing Standard Catheter-Directed Thrombolysis Versus Ultrasound-Accelerated Thrombolysis for Arterial Thromboembolic Infrainguinal Disease (DUET). Schrijver AM et al. Journal of Endovascular Therapy, 2015; 22(1): 87-95
16. Ultrasound-Accelerated Thrombolysis Is Superior to Catheter-Directed Thrombolysis for the Treatment of Acute Limb Ischemia. Litzendorf M et al. Journal of Vascular Surgery, 2011; 53(Suppl S): p106S-107S
17. RCT Comparing Standard Thrombolysis with US Accelerated Thrombolysis: The DUET Study and Beyond. De Vries J et al. Charing Cross International Symposium, London, UK, April 2014
18. Comparison of Percutaneous Ultrasound-Accelerated Thrombolysis versus Catheter- Directed Thrombolysis in Patients with Acute Massive Pulmonary Embolism. Lin P et al, Vascular, 2009; 17(3): S137-S147
19. Catheter-Directed Thrombectomy and Thrombolysis for Symptomatic Lower-Extremity Deep Vein Thrombosis: Review of Current Interventional Treatment Strategies. Lin P et al. Perspectives in Vascular Surgery and Endovascular Therapy, 2010; 22(3): 152-163
20. Ultrasound Accelerates Transport of Recombinant Tissue Plasminogen Activator into Clots. Francis CW et al. Ultrasound in Medicine and Biology, 1995; 21(3): 419-424
21. Ultrasound-Accelerated Catheter-Directed Thrombolysis for Acute Submassive Pulmonary Embolism. Bagla, MD, John B. Smirniotopoulos, MD, Arletta van Breda, MSN, Michael J. Sheridan, ScD, and Keith M. Sterling, MD. J Vasc Interv Radiol, 2015; 26(7): 1001-1006
22. Safety and efficacy of ultrasound-accelerated catheter-directed lytic therapy in acute pulmonary embolism with and without hemodynamic instability. Madeline Nykamp, Angela VandenHull, Tyler Remund PhD, Angelo Santos MD, Patrick Kelly MD, Greg Schultz MD, and Chad Laurich MD. Journal of Vascular Surgery: Venous and Lymphatic Disorders, 2015; 3(5): 251-257
About BTG
BTG is a growing international specialist healthcare company bringing to market innovative products in specialist areas of medicine to better serve doctors and their patients. We have a portfolio of Interventional Medicine products to advance the treatment of liver tumor, advanced emphysema, severe blood clots and varicose veins, and Specialty Pharmaceuticals that help patients overexposed to certain medications or toxins. Inspired by patient and physician needs, BTG is investing to expand its portfolio to address some of today’s most complex healthcare challenges.
To learn more about BTG, please visit: www.btgplc.com.
FDA CLEARED INDICATIONS: The EkoSonic® Endovascular System is intended for controlled and selective infusion of physician-specified fluids, including thrombolytics, into the peripheral vasculature. The EkoSonic® Endovascular System is intended for the infusion of solutions into the pulmonary arteries. The EkoSonic® Endovascular System is indicated for the ultrasound-facilitated, controlled and selective infusion of physician-specified fluids, including thrombolytics, into the vasculature for the treatment of pulmonary embolism.
CONTRAINDICATIONS: Not designed for peripheral vasculature dilatation purposes. The system is contraindicated when, in the medical judgement of the physician, such procedure may compromise the patient’s condition. See device instructions for use for complete prescribing information
References
Contact us:
Address: 11911 North Creek Parkway S Bothell, Washington 98011 USAEmail: [email protected]: www.ekoscorp.comOnline Learning Center: www.btg-im.com/EKOS/US/Learning-Center
About EKOS
EKOS Corporation, a BTG International group company, pioneered the development and clinical application of ultrasound infusion technologies in medicine, introducing its first system for the treatment of vascular thrombosis in 2005.
Today, interventional radiologists, cardiologists, and cardiothoracic and vascular surgeons at leading institutions around the world use the EKOS® system to provide faster, safer and more complete dissolution of thrombus. To find out more about the EKOS® system, visit www.ekoscorp.com.