-
7/26/2019 Thromboembolic and Hematologic
1/105
Hematological andThromboembolic
Disorders inPregnancy
TAGUD, LYZELCSU!ED"C"#E
-
7/26/2019 Thromboembolic and Hematologic
2/105
-
7/26/2019 Thromboembolic and Hematologic
3/105
#ormal PregnancyHypervolemic statePhysiologic/ Dilutional
Anemia
"ncrease $%C!ild thrombocyto&enia
Hypercoagulable state
Diminished 'brinolysis
-
7/26/2019 Thromboembolic and Hematologic
4/105
Blood volume
HYPERVOE!"#$%A%E
-
7/26/2019 Thromboembolic and Hematologic
5/105
Plasma Volume
-
7/26/2019 Thromboembolic and Hematologic
6/105
Red #ell Volume
D"&%"O'A
A'E!"A
-
7/26/2019 Thromboembolic and Hematologic
7/105
Dilutional/
Physiological AnemiaDe'ned by CDC as(
(( g/d in the 'rst and thirdtrimesters, and
()*+ g/d in the second trimester
lo) hgb le*el
lo) hct le*el
-
7/26/2019 Thromboembolic and Hematologic
8/105
eu,ocyte #ount
D+ring acti*e labor there may be anothernormal increase, e*en in
the absence oinection-.,///0+L
-
7/26/2019 Thromboembolic and Hematologic
9/105
Platelet #ount
GESTAT"1#AL TH21!%1CYT1PE#"A
Ty&ically de'ned as belo) the -3.th&ercentileor
445,///0+L
&artially d+e to the hemodil+tional e6ectalso d+e to
increased &latelet cons+m&tion
-
7/26/2019 Thromboembolic and Hematologic
10/105
Coag+lation and
7ibrinolysis
-
7/26/2019 Thromboembolic and Hematologic
11/105
Coag+lation and
7ibrinolysis7ibrinogen, 7actors "", 8"", 9, 9"", and 9"""
increase8on $illebrand actor increases
Antithrombin, Protein C, 7actor 8, and 7actor "9le*els remain
+nchanged or increased slightly
7ibrinolytic acti*ity is red+ced in normal
®nancyHYPER#OA-&ABE $%A%E
-
7/26/2019 Thromboembolic and Hematologic
12/105
-
7/26/2019 Thromboembolic and Hematologic
13/105
HematologicDisorders
-
7/26/2019 Thromboembolic and Hematologic
14/105
"3 2ED %L11D CELLA3 Anemia
a3 Ac:+ired
b3 Hereditary
%3 Polycythemia
""3 PLATELET D"S12DE2SC3 "nherited Thrombocyto&enia
D3 "TP
E3 Thrombocytosis
73 Thrombotic !icroangio&athies
"""3 "#HE2"TED C1AGULAT"1# DE7ECTSG3 Hemo&hilia
H3 7actor 8"" or "9 "nhibitor Deects
"3 8on $illebrand disease
;3 1ther Coag+lation 7actor Deects
-
7/26/2019 Thromboembolic and Hematologic
15/105
A'E!"A
-
7/26/2019 Thromboembolic and Hematologic
16/105
Clinical &ict+reor orms in*ol*es
Fim&aired &rod+ction or instability either o
M&e&tide chains @;
-
7/26/2019 Thromboembolic and Hematologic
40/105
Alpha6 %halassemias
Alpha6 %halassemias
-
7/26/2019 Thromboembolic and Hematologic
41/105
"n Pregnancy:*Hemoglobin H disease >= 8?
Fcompatible 1ith e4trauterine li0e
FThe neonate a&&ears )ell at birth b+t soonde*elo&s
hemolytic anemia3
FAnemia in these )omen +s+ally is )orsenedd+ring
®nancy
Alpha6 %halassemias
-
7/26/2019 Thromboembolic and Hematologic
42/105
Pregnancy
Hemoglobin Bart DiseaseFdeletion o all o+r Mglobin chain
genes@NN0NN
FhomozygousNthalassemia
FHemoglobin %art ( has an a&&reciablyincreased aOnity or
oygen
FCa+ses stillbirths
-
7/26/2019 Thromboembolic and Hematologic
43/105
@6%HAA$$E!"A !AOR OR#OOEY A'E!"A
F Homo=ygo+s
F the neonate is healthy at birth, b+t as thehemoglobin 7 le*el
alls, the inant becomes
se*erely anemic and ails to thri*e3F Prognosis is im&ro*ed
by iron chelation
thera&y )ith deeroamine
-
7/26/2019 Thromboembolic and Hematologic
44/105
PlateletDisorders
Platelet Disorders
-
7/26/2019 Thromboembolic and Hematologic
45/105
"nherited %hrombocytopenias Bernard-Soulier syndrome
characteri=ed by lac o &latelet membraneglyco&rotein
@GP"b0"9
May-Hegglin anomaly
a+tosomally dominant
characteri=ed by thrombocyto&enia, giant&latelets, and
le+ocyte incl+sions
Platelet Disorders
-
7/26/2019 Thromboembolic and Hematologic
46/105
"mmune %hrombocytopenicPurpura
Also called idiopathic thrombocytopenic purpura(IT!
+s+ally res+lts rom a cl+ster o "gG antibodiesdirected against
one or more &lateletglyco&roteins
Antibodycoated &latelets are destroyed&remat+rely in the
retic+loendothelial system,es&ecially the s&leen3
-
7/26/2019 Thromboembolic and Hematologic
47/105
Acute vs* #hronic
Acute "%P #hronic "%P
oten a childhood disease Ad+lts @yo+ng )omen
resol*e s&ontaneo+sly rarely resol*es s&ontaneo+sly
Secondary orms o chronic thrombocyto&eniaa&&ear in
association )ith(a3 systemic l+&+s erythematos+sb3
Lym&homasc3 Le+emiasd3 systemic diseases3
Platelet Disorders
-
7/26/2019 Thromboembolic and Hematologic
48/105
"mmune %hrombocytopenicPurpura
%reatment
Prednisone 4 mg0g0day P1 @or im&ro*ement
Corticosteroid thera&y +s+ally &rod+ces
amelioration3 highdose imm+noglob+lin ( "8
Platelet Disorders
-
7/26/2019 Thromboembolic and Hematologic
49/105
"mmune %hrombocytopenic
Purpura"n ®nant )omen )ith no res&onse tosteroid or
imm+noglob+lin thera&y( o&en or la&arosco&ic
s&lenectomy may be
e6ecti*e3 "n late ®nancy, cesarean deli*ery may
benecessary or e&os+re3
"ntra*eno+s antiD "gG
There +s+ally is im&ro*ement by 4 to ? days )itha &ea at
a&&roimately days3
-
7/26/2019 Thromboembolic and Hematologic
50/105
9etal and 'eonatal EectsPlateletassociated "gG antibodies cross
the&lacenta and may ca+se thrombocyto&enia inthe
et+sneonate3
!ay ca+se(7etal death rom hemorrhage
increased ris or intracranial hemorrhage )ithlabor and
deli*ery
-
7/26/2019 Thromboembolic and Hematologic
51/105
%hrombocytosis
>thromocythemia )de'ned as &ersistent &latelet co+nts
Q ./,///0L3
+s+ally is asym&tomatic, b+t arterial and *eno+sthromboses
may de*elo&
a! secondaryor reacti"e thromocytosis Common ca+ses(
iron de'ciency
inection inRammatory diseases
malignant t+mors
b3 essential thromocytosis
-
7/26/2019 Thromboembolic and Hematologic
52/105
%hrombocytosis in Pregnancy
#ormal ®nancies ha*e been described in)omen )hose mean
&latelet co+nts )ere Q43-. million0L
com&licated by s&ontaneo+s abortion, etaldemise, and
&reeclam&sia @#iitty*+o&io andcolleag+es, -//
Treatment d+ring ®nancy incl+des(
as&irin, di&yridamole,
he&arin,
&latelet &heresis, or combinations thereo
-
7/26/2019 Thromboembolic and Hematologic
53/105
%HRO!BO%"# !"#ROA'-"OPA%H"E$
(*%HRO!BO%"# %HRO!BO#Y%OPE'"#P&RP&RA Pentad o
thrombocyto&enia @!oschco)it=
7e*er
#e+rological abnormalities
2enal im&airment
Hemolytic anemia
De'ciency o a *on $illebrand actor clearing &rotease
ADA!TS4?
*HE!OY%"# &RE!"# $Y'DRO!E $ithmore &roo+nd renal
in*ol*ement and e)er ne+rological
aberrations
Us+ally d+e to endothelial damage incited by *iral or
bacterial
inections
%HRO!BO%"# !"#ROA'-"OPA%H"E$
-
7/26/2019 Thromboembolic and Hematologic
54/105
#"'"#A PRE$E'%A%"O'
Thrombocyto&enia, ragmentation hemolysis, and*ariable organ
dys+nction
Preceding *iral &rodrome @/ cases
#e+rological sym&toms de*elo& in +& to /
Headache
Altered conscio+sness
7e*er
Stroe
2enal ail+reSe*erity( HUS Q TTP
%HRO!BO%"# !"#ROA'-"OPA%H"E$
-
7/26/2019 Thromboembolic and Hematologic
55/105
%reatment
Plasma&heresis )ith reshro=en &lasmare&lacement not
indicated or &reeclam&siaeclam&sia com&licated
by hemolysis and thrombocyto&enia2ed cell trans+sions
Prednisone
7or those )ith mild ne+rological sym&toms
-// mg orally, daily
Plasma echange )ith 77P
%HRO!BO%"# !"#ROA'-"OPA%H"E$
-
7/26/2019 Thromboembolic and Hematologic
56/105
PRE-'A'#Y$evere preeclampsia andecclampsia complicated
bythrombocytopenia and overt
hemolysis have been con0used 1ith%%P and vice versaHemolytic
anemia is rarely seen in&reeclam&sia, e*en )ith HELLP
syndrome
He&atocell+lar necrosis is not described inTTP
Deli*ery does not im&ro*ed TTP
%HRO!BO%"# !"#ROA'-"OPA%H"E$
-
7/26/2019 Thromboembolic and Hematologic
57/105
O'- %ER! PRO-'O$"$
Pregnant 1omen 1ith thromboticmicroangiopathy have a number
o0long6term complications.
renal disease re:+iring dialysis ,trans&lantation, or
both
se*ere hy&ertension
trans+sionac:+ired inectio+s diseases
'on6pregnant 1omen 1ho haverecovered 0rom %%P.Persistent
cogniti*e deects
-
7/26/2019 Thromboembolic and Hematologic
58/105
"'HER"%ED #OA-&A%"O'DE9E#%$
-
7/26/2019 Thromboembolic and Hematologic
59/105
von Cillebrand Disease
Heterogeno+s gro+& o a&&roimately -/
+nctionaldisorders!ost commonly inherited bleeding disorders
&re*alence is as high as 4 to - &ercent
"n*ol*es aberrations o actor 8""" com&le and&latelet
dys+nction
!ost *ariants are inherited as a+tosomal dominanttraits
a* %ypes " and "" most common *ariants @Ty&e " acco+ntsor B.
o *$D
b* %ype """ most se*ere and is &henoty&ically
recessi*e
-
7/26/2019 Thromboembolic and Hematologic
60/105
Pathogenesis. von CillebrandDisease
Aberrations in vC9
"m&aired &lateletadhesion to
s+bendothelialcollagen
"m&aired ormation oa &rimary hemostatic&l+g at the
site oblood *essel in>+ry
"m&aired stabili=ationo the coag+lant&ro&erties o
actor 8"""
Bleedingproblems
-
7/26/2019 Thromboembolic and Hematologic
61/105
#"'"#A !A'"9E$%A%"O'
Characteri=ed clinicallyby (43Easy br+ising
-3E&istais
?3!+cosal hemorrhage
3Ecessi*e bleeding )ithtra+ma, incl+dings+rgery
ABORA%ORY 9EA%&RE$.
Prolonged bleedingtime
Prolonged PTT
Decreased *$7antigen le*els
Decreased actor 8"""imm+nological as )ellas
coag+lation&romoting acti*ity
"nability o &latelets in&lasma rom ana6ected &erson
toreact to a *ariety ostim+li
-
7/26/2019 Thromboembolic and Hematologic
62/105
Pregnancy and vCD
'ormal pregnancy!aternal le*els o both actor 8""" as )ell as *)
antigen increases
Pregnant 1omen 1ith vCDDe*elo& normal le*els o actor 8"""
coag+lant acti*ity as )ell as
*) antigen
"0 0actor V""" activity is very lo1 or i0 there is
bleeding.Treatment is recommended
Desmo&ressin by in+sion may transiently increase actor *iii
and*) actor le*els, es&ecially in &atients )ith ty&e "
disease
Cith signi2cant bleeding4. or -/ +nits or bags o
cryo&reci&itate are gi*en e*ery 4- ho+rs
Pregnancy outcomes are generally goodPost&art+m hemorrhage
is enco+ntered in +& to ./ &ercent o
cases
-
7/26/2019 Thromboembolic and Hematologic
63/105
%HRO!BOE!BO"#
D"$ORDER$
-
7/26/2019 Thromboembolic and Hematologic
64/105
"ntroduction
The ris o *eno+s thrombosis and&+lmonary embolism(
5 higher d+ring the 5rd trimester,
-- higher in the (st7 1,s postpartum @"ultan,
20##, $% "ncidence o thromboembolic e*ents
a*erages a&&roimately 40 4///®nancies3
DV%is more re:+ent antepartum, Pulmonary embolism is more common
in the
2rst 7 1,s postpartum @&acobsen et'al', 200,)or*ay
-
7/26/2019 Thromboembolic and Hematologic
65/105
Pathophysiology
Predisposing 0actors or thrombosisde*elo&ment that is +rther
increasedd+ring ®nancy @+' ircho*(
a*$tasis
!ost constant &redis&osing ris actor
b*ocal trauma
c*Hypercoagulability
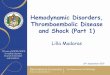
%able +6(* $ome Ris, 9actors Associated
-
7/26/2019 Thromboembolic and Hematologic
66/105
%able + (* $ome Ris, 9actors Associated1ith an "ncreased Ris,
0or%hromboembolism
%able +6(* $ome Ris, 9actors Associated
-
7/26/2019 Thromboembolic and Hematologic
67/105
%able + (* $ome Ris, 9actors Associated1ith an "ncreased Ris,
0or%hromboembolismObstetrical
CSD
Diabetes
Hemmorrhage K anemia
Hy&eremesis
"mmobility
!+ltietal gestation
!+lti&arity
Preeclam&sia
P+er&eral inection
-eneral
Prior history o0embolism
?. y0o and abo*e
Cancer
Connecti*e tiss+e dse
Dehydration
"mmobility
"nection and inRammatory dse
!yelo&rolierati*e dse
#e&hrotic syndrome
1besity
1ral contrace&ti*e +se
1rtho&edic s+rgery
Para&legia
Sicle cell dse
Smoing
Thrombo hilia
%he most important ris,0actor
(+ < + o all *eno+sthromboembolism casesd+ring ®nancy
arerecurrent events @AC1G,-/443
%able +6(* $ome Ris, 9actors Associated
-
7/26/2019 Thromboembolic and Hematologic
68/105
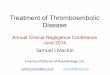
%able + (* $ome Ris, 9actors Associated1ith an "ncreased Ris,
0or%hromboembolismObstetrical
CSD
Diabetes
Hemmorrhage K anemia
Hy&eremesis
"mmobility
!+ltietal gestation
!+lti&arity
Preeclam&sia
P+er&eral inection
-eneral
Prior history o embolism
?. y0o and abo*e
Cancer
Connecti*e tiss+e dse
Dehydration
"mmobility
"nection and inRammatory dse
!yelo&rolierati*e dse
#e&hrotic syndrome
1besity
1ral contrace&ti*e +se 1rtho&edic s+rgery
Para&legia
Sicle cell dse
Smoing
%hrombophilia
%he ne4t most importantindividual ris, 0actor
)6 +) o )omen )ho
de*elo& a *eno+s thrombosisd+ring ®nancy
or&ost&art+m ha*e anidenti2able underlyinggenetic
disorder@ACOG,20##3
%hrombophilias
-
7/26/2019 Thromboembolic and Hematologic
69/105
%hrombophilias
"nherited or ac:+ired de'ciencies on&roteins that inhibit
coag+lationcascade )hich can lead tohy&ercoag+lability and
rec+rrent 8TE3
1bstetrical com&lications associated)ith
thrombo&hilias(
Pregnacy loss
Preeclam&sia Placental Abr+&tion
7G2
%hrombophilias
-
7/26/2019 Thromboembolic and Hematologic
70/105
%hrombophilias
"nherited %hrombophilias.
a3 Antithrombin De'ciency
b3 Protein C De'ciency
c3 Protein S De'ciency
d3 Acti*ated Protein C 2esistanceN 7actor 8Leiden !+tation
G-/-4/A
e3 Hy&erhomocystenemia
Ac3uired %hrombophilias(a3 Anti&hos&holi&id
antibody
b3 He&arin ind+ced thrombocyto&enia
c3 cancer
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
71/105
Antithrombin De2ciency
%he most thrombogenic o0 theheritable coagulopathies*
2areN 4 in -/// to ./// indi*id+al3
Thrombosis ris d+ring ®nancy )itho+t&ersonal or amily
history is ? B3
Thrombosis ris d+ring ®nancy )ith
&ersonal or amily history is 44 /3
Almost al)ays a+tosomal dominant andhomo=ygo+s and is
lethal3
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
72/105
Antithrombin De2ciency
Antithrombin Synthesi=ed in the li*er3
%inds and inacti*ate thrombin and the acti*atedcoag+lation
actors "9a, 9a, 9"a, and 9""a3
Accelerated by he&arin3 %YPE " Antithrombin De2ciency
res+lt o reduced synthesis o biologicallynormal antithrombin
%YPE "" Antithrombin De2ciency
Characteri=ed by normal le*els o antithrombin
)ith reduced 0unctional activity3
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
73/105
Antithrombin De2ciency
Untreated )omen had a ./ ris ostillbirth and 9-R3
!anagement(
a* Heparin or a6ected )omen d+ring ®nancy
)ith or )itho+t &rior thrombosis3
b* Recombinant human antithrombin "anticoag+lation m+st be
necessarily )ithheld@s+rgery, deli*ery3
c* Antithrombin concentrate in0usion therapeutic coagulation
®nant )oman)ith antithrombin de'ciency )ho
de*elo&edthrombosis d+ring ?rdtrimester3
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
74/105
Protein # De2ciency
Pre*alence( - to ? &er 4///
7 to ( 0old increased ris or8TE3
Protein # Acti*ated by binding o thrombin to
thrombomod+lin
inacti*ating actor 8a and 8"""a3
Also inhibits the synthesis o&lasminogen acti*ator inhibitor
43
Largely +nchanged in ®nancy3
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
75/105
Protein $ De2ciency
Pre*alence( - &er 4///
!eas+red antigenically determinedree, +nctional and total S
le*els3
All three decline d+ring normalgestation th+s diagnosis is
diOc+lt in®nant )omen
7or screening( meas+re ree S
Protein d+ring -ndor ?rdtrimester3
-
7/26/2019 Thromboembolic and Hematologic
76/105
Purpura 9ulminans
Associated )ith neonatalhomo=ygo+s &rotein C or
SDe'ciency3
Characteri=ed by etensi*e
thromboses in microcirc+lation soonater birth leading to sin
necrosis3
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
77/105
Activated Protein # De2ciency /9actor V eiden !utation
%he most prevalent o0 the ,no1nthrombophilia syndrome
HeteroFygous inheritance o0 0actor V
leiden is the most common heritablethrombophilia*
Acco+nts or / o 8TE cases in®nancy
characteri=ed by resistance o &lasma to theanticoag+lant
e6ects o acti*ated &rotein C3
Ca+ses(
a3 !issense m+tation in actor 8 gene
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
78/105
Activated Protein # De2ciency /9actor V eiden !utation
The abnormal actor 8 retains its&rocoag+lant acti*ity th+s
&redis&osed tothrombosis3
Diagnosis( D#A analysis
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
79/105
Prothrombin -)()A !utation
missense m+tation in &rothrombin gene
There is ecessi*e acc+m+lation o&rothrombin )hich can be
con*erted tothrombin3
7or hetero=ygo+s carrier )ith history, theris eceeds 4/ 3
"nherited thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
80/105
Hyperhomocysteinemia
There is ele*ated le*els o &lasmahomocysteine and is a 1ea,
ris, 0actor3
A+tosomal recessi*e
Ca+ses(
C55BT thermolabile mutation o0 +G()6methylene6tetrahydro0olate
reductase>!%H9R? the most common cause
De'ciency in the en=ymes in*ol*ed in
methionine metabolism3 #+tritional de'ciencies( olic acid,
8itamin
%5, or 8itamin %4-3
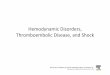
Overvie1 o0 inherited thrombophilias and their eect on
coagulation cascade*
-
7/26/2019 Thromboembolic and Hematologic
81/105
-)(Amutatio
n
c3 Prothrombin le*el
O%HRO!B"' %HRO!B"' #OA-&A%"O
Antithrombin De2ciency
Dec3
thrombinne+trali=ation
9actor Vleiden
!utation
7actor 8
resistant todegradationby &rotein C
"nacti*ates actor8a
"nacti*ates actor
8"""a
Protein
$
Acti*ated &rotein C
Hyperhomocysteinem
ia
Protein C
Protein#
de2ciency
Thrombin binds tothrombomod+linon endothelial
cells
Protein S Protein S
Ac3uired thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
82/105
Antiphospholipid Antibodies
A+toantibodies directed againstcardioli&in or against
&hos&holi&idbinding &roteins s+ch as
-glyco&rotein "3
CommonlyN b+t not al)aysN o+nd in&atients )ith SLE
.4- ris o thrombosis d+ring
®nancy and &+er&eri+m @ACOG,20#23
Ac3uired thrombophilias
-
7/26/2019 Thromboembolic and Hematologic
83/105
Antiphospholipid Antibodies
De'ned by the ollo)ing eat+res @ACOG,20#2(
43 At least 4 +ne&lained etal death at orbeyond 4/ )s3
-3 At least one &reterm birth beore ? )sbeca+se o &re
eclam&sia, se*ereeclam&sia, or &lacental
ins+Ociency3
?3 At least ? +ne&lained consec+ti*e
s&ontaneo+s abortion beore 4/ )s3 "n 1omen 1ith this
stateG
thromboembolism most commonlyinvolves the lo1er e4tremities*
Deep6 Vein %hrombosis
-
7/26/2019 Thromboembolic and Hematologic
84/105
Deep Vein %hrombosis
#linical Presentation(most venous thromboses are
con2ned to the deep veins o0lo1er e4tremities*
a3 "lioemoral B/
b3 "liac *ein 4B
c3 Cal *eins 5
!ost cases during pregnancyare le0t sided3
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
85/105
#linical Presentation
Abr+&t in onset, )ith &ain and edemao the leg and
thigh
2eRe arterial s&asm &ale, cooletremity )ith diminished
&+lsations
Homans sign6 cal &ain in res&onseto s:+ee=ing or to
Achilles tendonstretching3
?/ 5/ o )omen )ith D8T areasym&tomatic3
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
86/105
Diagnosis
A*#ompression <rasonography
2ecommended by AC1G as initialdiagnostic test
'on6invasive techni3ue that is
currently the most used 2rst line testto detect DV%*
normal 'ndings )ith *eno+s UTZ res+lt donot al1ays e4clude
pulmonary
embolism* Thrombosis assoc3 )ith PE d+ring ®nancy
re:+ently originates in the iliac *eins3
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
87/105
Diagnosis
A* #ompression <rasonography
B* !R"
"mmensely +se+l or diagnosis oilioemoral and &el*ic
thrombosis3
#* D6Dimer $creening %ests Their +se in ®nancy is
+ncertain b+t
negati*e res+lt is reass+ring3
D* Venography
-old standard to e4clude lo1ere4tremity DV%*
Com&lications( etal e&os+re, thrombosis,
time cons+ming3
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
88/105
!anagement
Anticoagulation and limited activity During pregnancy(
he&arin
@+nractionated0 L!$H is contin+ed
Post- partum ( beg+n sim+ltaneo+sly )ith
)ararin3
#fter symptoms ha"e aated( gradedamb+lation, elastic stocings
Kanticoag+lation contin+ed3
Com&ression stocings is contin+ed or -yrs to red+ce
incidence o Posthrombotic$yndrome @ chonic leg &aresthesial
&ain,intractable edema, sin change, leg +lcer
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
89/105
!anagement. Anticoagulation
ACCP s+ggest &reerential +se oL!$H d+ring ®nancy
beca+se o(
%etter bioa*ailability Longer &lasma hallie
!ore &redictable dose res&onse
2ed+ced riss o osteo&orosis andthrombocyto&enia
Less re:+ent dosing
i l i
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
90/105
!anagement. Anticoagulation
&n0actionated Heparin
Sho+ld be considered initial treatment othromboembolism and in
sit+ation in )hichdeli*ery, s+rgery, or thrombosis
maybenecessary3
Sae d+ring breasteeding3
!CH
Deri*ati*es o U7H
Cannot cross &lacenta
Acti*ates antithrombin, greater acti*ity againstactor 9a
Sho+ld be a*oided in )omen )ith renal ail+re
i l i
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
91/105
!anagement. Anticoagulation
Car0arin
Generally contraindicated d+ring ®nancy
Used d+ring postpartum together )ithhe&arin
Thera&e+tic doses o U7H0 L!$H aremaintained or . days K
+nitl "#2 is maintainedat -? or - consec+ti*e days @ACOG, 20#03
This is to &re*ent the anti &rotein C e6ect o
)ararin leading to &aradoical thrombosisand sin
necrosis3
Sae d+ring breasteeding
! A i l i
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
92/105
!anagement. Anticoagulation
During abor
Anticoag+lation sho+ld be con*erted romL!$H to shoter hal lie
U7H to a*oid e&id+ralor s&inal hematoma d+ring ne+raial
blocade3
ACCP or &lanned deli*ery discontin+e - dailySV U7H or L!H$ -
ho+rs beore laborind+ction or CSD3
AC1G ad>+sted dose SV L!$H o U7H can be
discontin+ed -?5h beore labor ind+ction orCSD3
! t A ti l ti
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
93/105
!anagement. Anticoagulation
During abor
AS2AP )ithholding ne+raial blocadeor 4/ 4-h ater last
&ro&hylactic dose oL!H$ or -h ater the last
thera&e+ticdose3
" labor begins )hile taing U7H,clearance can be *eri'ed by
aPTTProtamine s+late3
7or )omen in )hom anticoag+lationthera&y has tem&orarily
beendiscontin+ed, &ne+matic com&ressionde*ices are
recommended @ACOG, 20##
! t A ti l ti
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
94/105
!anagement. Anticoagulation
During Delivery
He&arin thera&y is generally sto&&edd+ring labor
and deli*ery
AC1G and AAP recommend restarting
U7H or L!H$ no sooner than 5h ater*aginal deli*ery, or 54-h ater
CSD3
Slo) "8 administration o &rotamines+late generally re*erses
the e6ect o
he&arin
! t A ti l ti
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
95/105
!anagement. Anticoagulation
#omplication
Hemorrhage6 most seriouscomplication
Thrombocyto&enia @H"T
1steo&orosisThe latter t)o can be red+ced )ith
L!H$
! t A ti l ti
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
96/105
!anagement. Anticoagulation
Heparin "nduced %hrombocytopenia
T)o ty&es
a3 !ost common nonimm+ne, benign, re*ersiblethat de*elo&s
)ithin 4ste) days o thera&y andresol*es W. days )0o thera&y
cessation3
b3 Se*ere orm res+lt rom an imm+ne reactionin*ol*ing "gG
antibodies direstec againstcom&lees o &latelet actor and
he&arin3
"ncidence( X /34
!anagement( sto& he&arin thera&y And
initiate alternati*e anticoag+lation3a3 L!H$
b3 Dana&aroid @AC
c3 7onda&arin+ and argatroban
! t A ti l ti
DEEP VE"' %HRO!BO$"$
-
7/26/2019 Thromboembolic and Hematologic
97/105
!anagement. Anticoagulation
Heparin "nduced Osteoporosis
%one loss may de*elo& )ithin 5 monthsor longer o he&arin
thera&y and more&re*alent )ith cigarette smoer3
$omen treated )ith any hae&arin sho+ldbe enco+raged to tae
4,.// mg calci+ms+&&lement3
$uper2cial Venous %hrombophlebitis
-
7/26/2019 Thromboembolic and Hematologic
98/105
Strictly limited to the s+&er'cial *eins o
sa&heno+s system ty&ically seen )ith*aricosities or
se:+ela to an ind)elling "8catheter3
He&arin is gi*en )hen D8T is in*ol*ed
Pulmonary Embolism
-
7/26/2019 Thromboembolic and Hematologic
99/105
y
ca+ses 4/ o maternal death b+t is+ncommon in ®nancy
"ncidence( 4 in B/// ®nancies
?/ 5/ o )omen )ith D8T )ill ha*e
coeisting silent P+lmonary embolism3
#li i l P t ti
P&!O'ARY E!BO"$!
-
7/26/2019 Thromboembolic and Hematologic
100/105
#linical Presentation
Dys&nea, chest &ain
Co+gh
Synco&e
Hemo&tysis
Tachy&nea, a&&rehension, tachycardia
P+lmonic clos+re so+nd, rales, rictionr+b
ECG( right ais de*iation, T )a*e
in*ersion in anterior chest leads
Al*eolararterial di6erence o Q-/ mmHg
!assive Pulmonary Embolism
P&!O'ARY E!BO"$!
-
7/26/2019 Thromboembolic and Hematologic
101/105
!assive Pulmonary Embolism
De'ned as embolism ca+singhemodynamic instability3
!ost liely ca+sed by a saddle embolism3
"t is im&ortant to in+se crystalloids
care+lly and to s+&&ort %P )ith*aso&ressor3
1- treatment, ET int+bation and!echanical *entilation are
com&leted
&re&aratory to thrombolysis, 'lter&lacement, or
embolectomy3
Diagnosis
P&!O'ARY E!BO"$!
-
7/26/2019 Thromboembolic and Hematologic
102/105
Diagnosis
CT P+lmonary Angiogra&hy
8entilation Per+sion Scintigra&hy L+ngscan
!agnetic 2esonance Angiogra&hy
"ntra*asc+lar P+lmonary Angiogra&hy
There is contro*ersy regarding the bestimaging method to be +sed
in ®nancy3
!anagement
P&!O'ARY E!BO"$!
-
7/26/2019 Thromboembolic and Hematologic
103/105
!anagement
"mmediate treatment is +llanticoag+lation3
Com&lementary &roced+res
a* Vena #aval 9ilters can be +sed in®nant )omen )ho
recently s+6ered PEand m+st +ndergo CSD3
b* %hrombolysis &ro*ide more ra&id lysisthan
he&arin3 @eg3 Tiss+e &lasminogenacti*ator
c* Embolectomy stillbirth rate is -//
%hromboprophyla4is
-
7/26/2019 Thromboembolic and Hematologic
104/105
%hromboprophyla4is
AC1G recommended &lacement o &ne+matic
com&ression de*ices beore CSD or all )omen notalready
recei*ing thrombo&ro&hylais3
ACCP recommends ris ad>+sted a&&roach
tothrombo&ro&hylais
See table .-
A##P Recommendation 0orthromboprophyla4is 0ollo1ing #$D
-
7/26/2019 Thromboembolic and Hematologic
105/105
thromboprophyla4is 0ollo1ing #$D
!a>or 2is
actors "mmobility
Post&art+m hemorrhage Q 4 L )ith s+rgery
Pre*io+s 8TE
Thrombo&hilia
Antithrombin De'ciency 7actor 8 leiden
Prothrombin G-/-4/A
!edical condition
SLE
Heart Disease
Sicle Cell Anemia
%lood trans+sion
!inor 2is
7actors %!" Q ?/ g0m-
!+ltietal ®nancy
Post&art+m
hemorrhage Q4L Smoing Q 4/
cigarettes0day
7G2
Thrombo&hilia
Protein C de'ciency
Protein S de'ciency