Embed Size (px)
Citation preview
Endorsed by the Association for HospitalMedical Education
The Association for Hospital Medical Educationendorses HOSPITAL PHYSICIAN for the pur-pose of presenting the latest developments inmedical education as they affect residency pro-grams and clinical hospital practice.
®
ORTHOPAEDIC SURGERY BOARD REVIEW MANUAL
Orthopaedic Surgery Volume 7, Part 3 1
PUBLISHING STAFF
PRESIDENT, GROUP PUBLISHERBruce M. White
EXECUTIVE EDITORDebra Dreger
SENIOR EDITORBecky Krumm, ELS
ASSISTANT EDITORJennifer M. Vander Bush
EDITORIAL ASSISTANTNora H. Landon
EXECUTIVE VICE PRESIDENTBarbara T. White, MBA
PRODUCTION DIRECTORSuzanne S. Banish
PRODUCTION ASSOCIATESTish Berchtold KlusMary Beth Cunney
PRODUCTION ASSISTANTStacey Caiazzo
ADVERTISING/PROJECT MANAGERPatricia Payne Castle
Copyright 2001, Turner White Communications, Inc., 125 Strafford Avenue, Suite 220, Wayne, PA 19087-3391, www.turner-white.com. Allrights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means,mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White Communications, Inc.The editors are solely responsible for selecting content. Although the editors take great care to ensure accuracy, Turner WhiteCommunications, Inc., will not be liable for any errors of omission or inaccuracies in this publication. Opinions expressed are those of theauthors and do not necessarily reflect those of Turner White Communications, Inc.
NOTE FROM THE PUBLISHER:This publication has been developed withoutinvolvement of or review by the AmericanBoard of Orthopaedic Surgery.
Fractures of the Olecranonand Coronoid ProcessSeries Editor: Robert T. Trousdale, MDAssociate Professor of Orthopaedic Surgery, Mayo Graduate School ofMedicine, Consultant, Department of Orthopaedic Surgery, MayoClinic, Rochester, MN
Contributing Authors: Scott P. Steinmann, MDAssistant Professor of Orthopaedic Surgery, Mayo Graduate School ofMedicine, Senior Associate Consultant, Department of OrthopaedicSurgery, Mayo Clinic, Rochester, MN
Patricia Lee McKay, MD LCDR, MC, USN, Attending Orthopaedic Hand Surgeon, NationalNaval Medical Center, Bethesda, MD
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Fractures of the Olecranon. . . . . . . . . . . . . . . . . . . . 2
Fractures of the Coronoid Process . . . . . . . . . . . . . . 8
Board Review Questions. . . . . . . . . . . . . . . . . . . . . 11
Answers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Table of Contents
Cover Illustration by Marc Galindo
2 Hospital Physician Board Review Manual
I. INTRODUCTION
Fractures of the proximal ulna present a challenge tothe orthopedic surgeon. Fractures of the olecranonprocess are common and many classification systemsand treatment options have been described. Conversely,fractures of the coronoid process are relatively rare,especially in isolation, and management is often depen-dent on the concomitant injury. In all fractures of theproximal ulna, the fracture pattern and concomitantinjuries play a major role in surgical decision makingand prognosis. The guiding principle in treating thesefractures is to restore articular congruity and stability inorder to begin a program of early active motion.
II. FRACTURES OF THE OLECRANON
A. History of treatment techniques1. Prior to the 19th century, olecranon fractures
were treated with immobilization in exten-sion, which resulted in considerable stiffnessand loss of function.1
2. To achieve a better functional result, early limit-ed motion was attempted, which required rigidinternal fixation of the fracture fragments. In1883, Joseph Lister pioneered internal fixationfor the olecranon using a wire loop.2
3. Since Lister’s work, a number of fixation meth-ods have been employed, all with some success. a. McAtee device—a longitudinal fixation
device3
b. Zuelzer hook plate4
c. Longitudinal intramedullary screws5–7
d. Tension band wiring6,8–12
e. Plate fixation1,6,8,13,14
f. Fragment excision with triceps reattach-ment for comminuted fractures and forfractures in elderly patients1,15–19
B. Mechanisms of injury1. Direct trauma to the olecranon 2. A fall on the outstretched hand with eccentric
contraction of the triceps during resistedelbow flexion20
3. High-energy traumaa. In these cases, additional injury to the
elbow joint is often present. Radial headfracture, coronoid fracture, distal hum-erus fracture, and ligamentous instabilityare most common.
b. High-energy olecranon fractures haveincreased surgical complexity and carry a higher complication rate and poorerprognosis.
C. Classification systems. Several systems to describeolecranon fractures exist. 1. Colton’s classification system is based on frac-
ture pattern, comminution, and ligamentinjury.21
2. The AO classification system is more cumber-some, but it does provide a detailed descrip-tion according to the rules applied to otherarticular fractures. It also accounts for con-comitant fractures of the proximal radius.22
3. The Mayo classification system (Table 1) pro-vides a concise and manageable system thatassists in surgical decision making as well aspredicting outcome.1,17,20
D. Treatment by Mayo fracture type1. Mayo type I olecranon fractures (stable, nondis-
placed) (Figure 1). These can be treated withcasting or splinting and early mobilization. a. A long arm cast or posterior splint may
be used for comfort and protection,preferably in a position of mid-flexionand neutral forearm rotation.
b. A dynamic extension splint can also beused for early motion with active flexionand passive extension.1
c. Motion can often begin by 7 days post-injury with weekly radiographs during thefirst few weeks to follow the fracture andconfirm that it remains nondisplaced.1,17,20
ORTHOPAEDIC SURGERY BOARD REVIEW MANUAL
Fractures of the Olecranon and Coronoid Process
The views expressed in this monograph are those of the authorsand do not reflect the official policy or position of the US Depart-ment of the Navy, US Department of Defense, or the United StatesGovernment.
d. Flexion greater than 90 degrees shouldbe delayed until 3 to 6 weeks to allow sta-ble union.1,20
e. Results are usually excellent with nearnormal range of motion achieved.1
2. Mayo type II olecranon fractures (stable, dis-placed) (Figure 1). This is the most commonpattern of olecranon fracture.a. Articular incongruity, exacerbated by the
deforming forces of the triceps, bicepsand brachialis muscles, makes surgerynecessary to restore the articular surface,prevent redisplacement and allow earlymotion.
b. Type IIA olecranon fractures (non-comminuted, stable, displaced)1) These are best treated with ten-
sion band wiring by one of several methods described later (see Sec-tion II.E.1).1,6,8,10–12,18,20,23,24 This allowsneutralization of the deformingforces and compression of the frac-ture site.
2) Longitudinal intramedullary fixationhas also been advocated for this frac-ture pattern;1,3,7,17,23 however, higherrates of displacement, poor rotationalcontrol, and problems with screw pur-chase in the medullary canal havebeen reported.1,25 The techniqueworks best with a single large fragmentand minimal or no comminution.
c. Type IIB olecranon fractures (comminut-ed, stable, displaced)1) The nature of these fractures creates
increased difficulty obtaining articu-lar congruity with tension band wiretechniques.
2) Additional interfragmentary screw fix-ation or plate fixation can improve theresults in these fractures.1,4,6,8,13,17,20
3) Fragment excision and triceps ad-vancement may be considered, par-ticularly for small fragments or inelderly patients.1,15–18
3. Mayo type III olecranon fractures (displaced,unstable) (Figure 1) a. These fractures present the greatest chal-
lenge and have the highest rate of com-plications.1,20
1) The elbow joint is unstable, usuallywith anterior subluxation of the radius
and ulna on the distal humerus as aresult of the deforming forces createdby the triceps, biceps, and brachialis.20
2) These fractures are usually commin-uted (type IIIB).
3) These fracture carry a high inci-dence of additional elbow trauma. a) Concomitant injuries include
radial head fractures, distalhumerus fractures, and ligamentrupture.1,26
b) Concomitant injuries should beassessed and treated at the sametime as the olecranon fracturebecause they have tremendousimpact on the results achieved.
b. Principles of treatment1) Rigid fixation is required.
a) Plate fixation is often best, espe-cially when comminution is pre-sent, in order to maintain ulnarlength and alignment. A num-ber of plate fixation techniqueshave been described, most in-volving a contoured posterior orlateral plate with, when possible,interfragmentary screws (see sec-tion II.E.2).1,4–6,8,13,14,17,20,23
b) In addition to internal fixation,use of an external fixationdevice or distraction device canbe helpful or necessary to main-tain joint congruity while allow-ing an early motion program. In rare instances, external fixa-tion alone may be used when
Orthopaedic Surgery Volume 7, Part 3 3
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
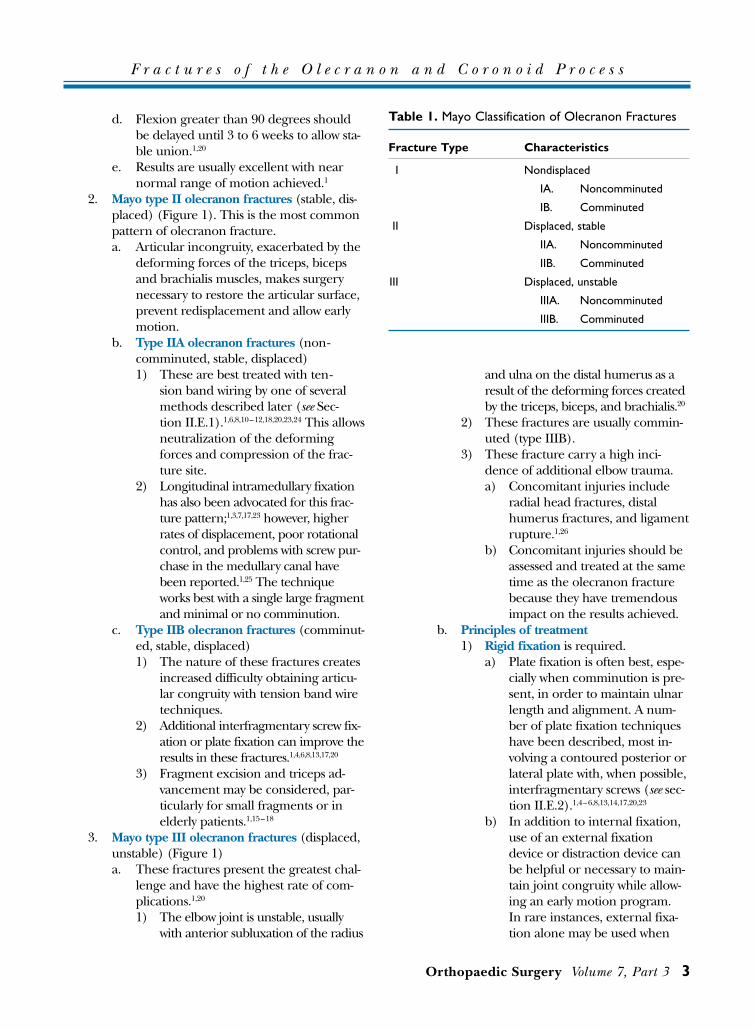
Table 1. Mayo Classification of Olecranon Fractures
Fracture Type Characteristics
I Nondisplaced
IA. Noncomminuted
IB. Comminuted
II Displaced, stable
IIA. Noncomminuted
IIB. Comminuted
III Displaced, unstable
IIIA. Noncomminuted
IIIB. Comminuted
internal fixation is prohibited(ie, soft tissue injury).1,17,27
2) Primary bone grafting should beconsidered to reduce the risk of non-union, especially in a type IIIB ole-cranon fracture.
3) Total elbow arthroplasty may beconsidered based on the fracturepattern, bone quality, and patientage. However, the results of elbowarthroplasty following trauma arenot as good as the results forpatients with inflammatoryarthritis.28
c. Restoration of articular congruity is a pri-mary goal of reduction and fixation ofolecranon fractures.1) Type IIIB olecranon fractures are not
well suited to tension band wiringbecause of the loss of bony stabilityunder compression.
2) Care must be taken to avoid narrow-ing of the olecranon to coronoid dis-tance.1
3) It is usually preferable to co-apt thecortical surfaces and leave a gap in thearticular surface in order to preserve amore normal articular contour.
4 Hospital Physician Board Review Manual
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
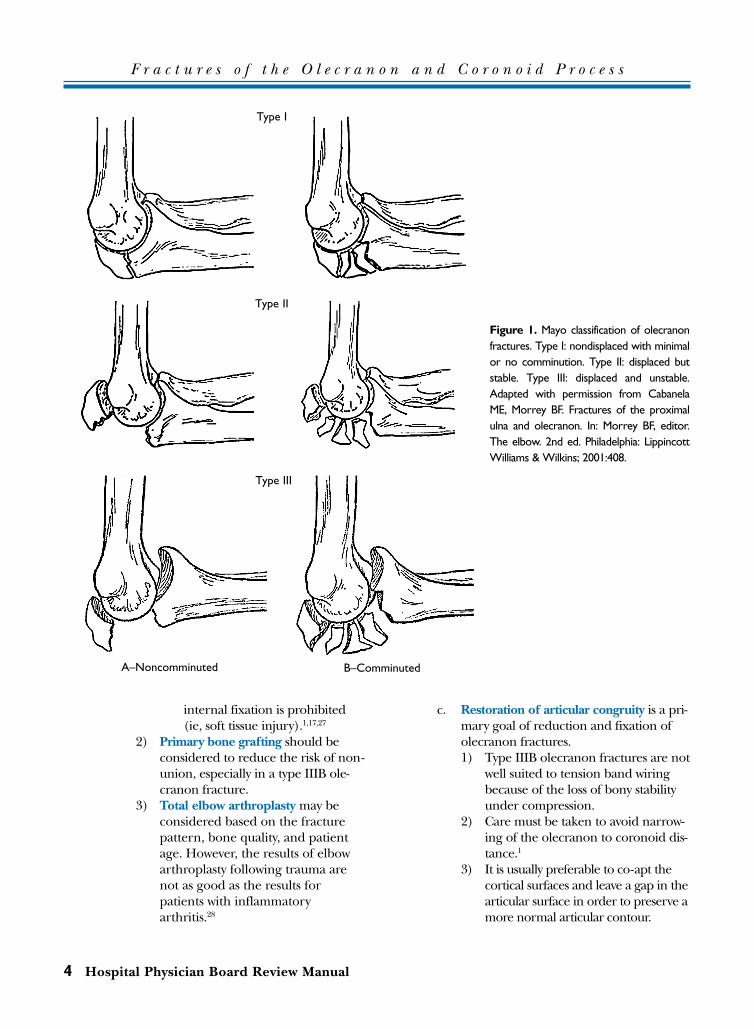
Figure 1. Mayo classification of olecranonfractures. Type I: nondisplaced with minimalor no comminution. Type II: displaced butstable. Type III: displaced and unstable.Adapted with permission from CabanelaME, Morrey BF. Fractures of the proximalulna and olecranon. In: Morrey BF, editor.The elbow. 2nd ed. Philadelphia: LippincottWilliams & Wilkins; 2001:408.
Type I
Type II
Type III
A–Noncomminuted B–Comminuted

E. Fixation techniques for olecranon fractures1. Tension band wiring. Various techniques have
been described. a. Standard AO technique. This technique,
which uses 2 intramedullary Kirschnerwires (K-wires) and a figure-of-eight wirewith a single knot, is acceptable in mosttype II olecranon fractures (Figure 2).1) Carefully bending the pins 180 de-
grees and impacting them into theproximal fragment, after placement ofthe wire loop, can minimize the prob-lem of prominent proximal pins orproximal pin migration.
2) It may be necessary to make smallslits in the triceps insertion to allowadequate impaction of the pins intobone followed by closure of the slitsover the pins.20
3) Placement of the K-wires and distaldrill hole dorsal to the mid-axis ofthe ulna helps produce compressionat the fracture site, particularly withelbow flexion.5
b. Intramedullary cancellous screw insteadof K-wires. Results have been variable. 1) Use of an intramedullary screw alone
or with a figure-of-eight wire gaveerratic results in biomechanical test-ing by Fyfe.6
2) In clinical evaluation by Murphy,these techniques yielded betterresults than standard tension bandwiring with K-wires.18
3) This variability may be related to theneed to obtain adequate distal pur-chase of the intramedullary screw. In addition, selecting noncomminut-ed fractures with some stability pro-duced through fracture compressionshould yield better results with intra-medullary screw fixation than ob-lique or comminuted fracture pat-terns.1,29
c. Distal fixation of the K-wires. K-wire posi-tion has been investigated in several bio-mechanical studies.1,24
1) Fixation to the anterior ulnar cortex.In an effort to avoid the commoncomplication of proximal migra-tion and hardware prominence, the K-wires can be directed anteriorly to
engage the ulnar cortex at the baseof the coronoid.1,30,31
a) In biomechanical testing, thistechnique has been shown toprovide stronger fixation thanthe usual intramedullary place-ment of the K-wires.30
b) Some concerns have been raisedover the potential for neurovas-cular injury with this technique,although no reports of suchinjuries could be found.24
2) Fixation to the ulnar styloid process.Wu described placement of 2 K-wiresthrough the medullary canal to theulnar styloid process and comparedthis to the anteriorly placed K-wires.24
a) In biomechanical testing, therewas no significant difference instability and no proximal migra-tion with either technique whenthe construct was tested to failure.
b) Wu proposes their technique issafer when impacting the K-wiresas there is diminished risk to neu-rovascular structures.
d. Use of 2 twist knots and anterior place-ment of the distal limb of the wireloop1,5,6,11,24,32
1) Use of 2 tightening knots in the wireloop provided increased rigidity overa single knot, when tested in a cadav-eric model.6
2) Kozin tested placement of the distallimb of the wire loop anterior to the K-wires, as described by Rowland,32
and demonstrated no biomechanicaladvantage over the standard tech-nique.9
2. Plate fixation. Several types of plates have beenadvocated for use in olecranon fractures, par-ticularly type IIB and type III fractures.a. General considerations
1) Plate fixation allows neutralization offorces across the fracture site andshould provide adequate rigid inter-nal fixation to begin early motion.
2) Interfragmentary compression screwsshould be utilized when possible.
3) Augmentation with an external fixa-tion or distraction device may bebeneficial when elbow stability is
Orthopaedic Surgery Volume 7, Part 3 5
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
lacking despite fracture fixa-tion.1,17,27
4) Small gaps in the articular surfaceare well tolerated as pointed out byWolfgang and others.1,12
5) Articular step-off of greater than2 mm has been associated with poor-er results.18
b. Results compared with tension bandwiring
1) Biomechanical and clinical studiesdemonstrate plate fixation to be supe-rior to tension band wiring when sig-nificant comminution is present.6,8,13
2) Hume compared plating with a pos-terior 1/3 semi-tubular plate to ten-sion band wiring in a prospectiverandomized clinical trial.8
a) The results suggested that platefixation allowed more anatomic
6 Hospital Physician Board Review Manual
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
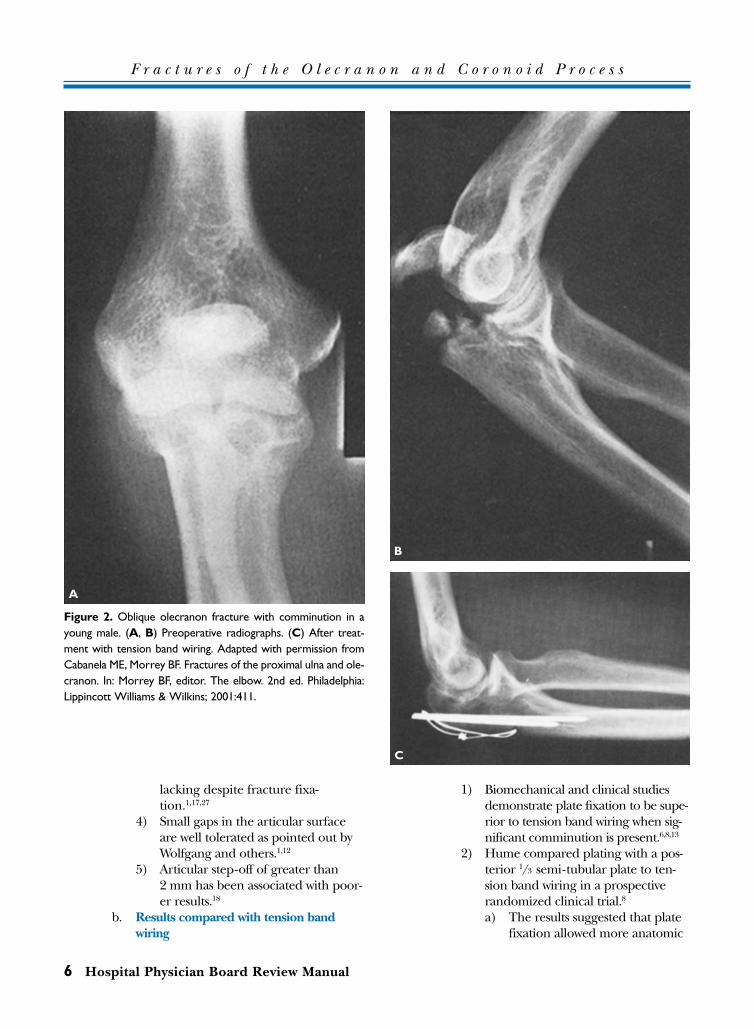
Figure 2. Oblique olecranon fracture with comminution in ayoung male. (A, B) Preoperative radiographs. (C) After treat-ment with tension band wiring. Adapted with permission fromCabanela ME, Morrey BF. Fractures of the proximal ulna and ole-cranon. In: Morrey BF, editor. The elbow. 2nd ed. Philadelphia:Lippincott Williams & Wilkins; 2001:411.
A
B
C
reductions and better mainte-nance of reductions than ten-sion band wiring.
b) They reported no significant dif-ference in range of motion,although plate fixation had a sig-nificantly better clinical resultbased on a scale evaluating painand motion.8
c. Plate position1) Most authors prefer posterior place-
ment of the plate; however, Kingreported a biomechanical investiga-tion showing no significant differ-ence in strength of fixation betweenposterior or lateral placement.13
2) Posterior plating allows a more directapproach to the proximal ulna andrequires less soft tissue stripping andless effort to contour the plate.
3) A laterally placed plate may be lessprominent and less likely to requirehardware removal.
d. Plate type1) A contoured, posterior 3.5 dynamic
compression plate or limited-contactdynamic compression plate providesexcellent rigidity and, when properlyapplied, will usually allow placementof 3 screws in the proximalfragment.33
2) A pelvic reconstruction plate can beused when a longer plate is needed.13
3) Nowinski described using the AOwrist fusion plate with the followingbenefits14:a) The lower-profile 2.7-mm seg-
ment is positioned over the sub-cutaneous border of the proxi-mal olecranon, therebyminimizing plate prominence.
b) There is added strength fromthe 3.5-mm segment distally
c) Ease of contouringd) Variable screw-hole sizing
4) A precontoured titanium plate is nowavailable from Acumed (Beaverton,OR) for posterior olecranon plating(Shawn O’Driscoll, MD, Rochester,MN, personal communication,May 2001). This plate minimizes theneed for plate manipulation and
allows for placement of 3 screws inthe proximal fragment.
3. Fragment excision with triceps advancement.Because of the potential for subsequent insta-bility, this technique should be reserved forcases involving small or comminuted frag-ments or low-demand patients.1,5,15,18
a. Biomechanical testing by An demonstrat-ed that the constraint of the ulnohumer-al joint is linearly proportional to thearea of articulation remaining.16 This sup-ports the clinical observation by Murphyand Horne that excision in patients withmore than 60% articular involvementyields poorer results.18,34
b. When reattaching the triceps, careshould be taken to bring the tendonclose to the articular surface, thus im-proving stability by acting as a sling forthe trochlea.35
4. Total elbow arthroplasty may be considered inelderly patients with significant comminutionand greater than 60% articular involvement.5
F. Postoperative care1. To minimize stiffness and reduce edema, the
limb should initially be elevated with theelbow in extension, followed by active motionbeginning within 7 days of surgery.
2. A dynamic extension splint allows protectedrange of motion (ROM) through the stable arc.
3. In cases involving severe soft tissue injury,early motion may need to be delayed untilthe soft tissue healing is adequate to toleratemotion.
G. Results. The rate of complications is directly relat-ed to the severity of the initial injury.1,20
1. Mayo type I olecranon fractures usually healwith excellent results, with near-normal rangeof motion.1
2. Outcomes of Mayo type III olecranon frac-tures are not as favorable as those for type I ortype II fractures. Type III fractures carry ahigh rate of complications, particularly stiff-ness.1,5,17,20,36
H. Complications1. Hardware prominence requiring removal
a. This is the most common complication,with some series reporting an incidenceas high as 80%.18
b. This complication is more common withtension band wiring than with plate fixa-tion.1,5,8,12,17,18,20
Orthopaedic Surgery Volume 7, Part 3 7
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
2. Stiffness occurs in up to 50% of cases. Loss ofextension is most common, but is not usuallyfunctionally significant.1,3,8,12,18
3. Nonunion occurs in 1% to 5% of olecranonfractures.5,35–37
a. The most common treatment describedis hardware revision with autogenousbone grafting.
b. Other treatments include bone plates,bone stimulators, and local muscleflaps.5,35–40
4. Other complications include:a. Ulnar neuropathyb. Post-traumatic arthritisc. Infectiond. Heterotopic ossification
III. FRACTURES OF THE CORONOID PROCESS
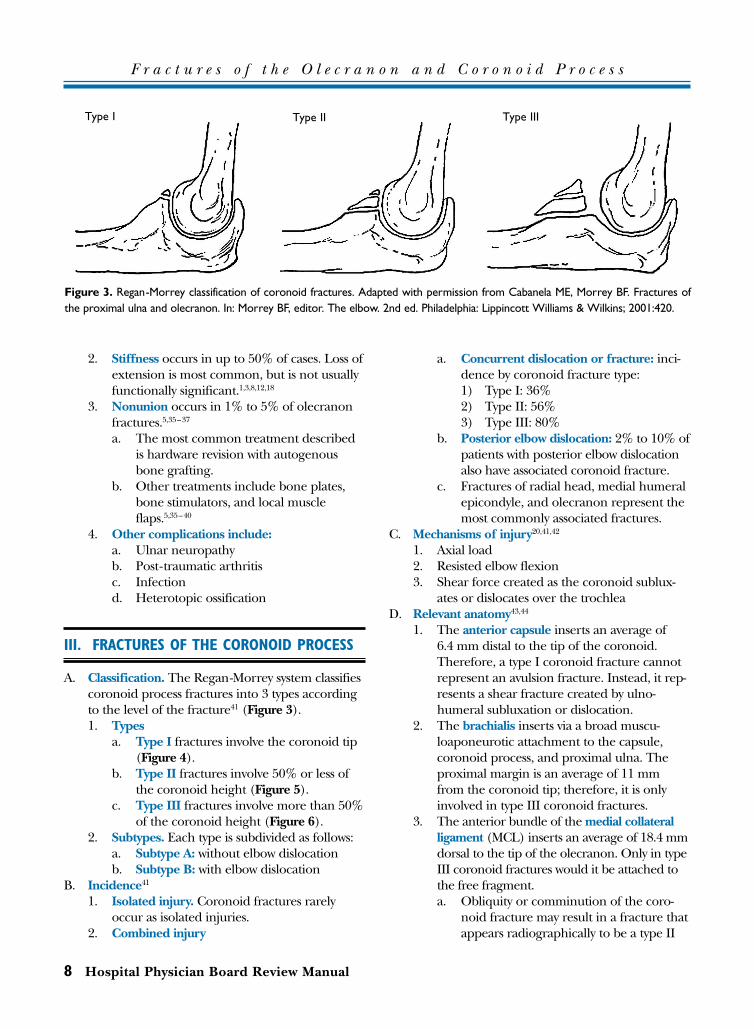
A. Classification. The Regan-Morrey system classifiescoronoid process fractures into 3 types accordingto the level of the fracture41 (Figure 3).1. Types
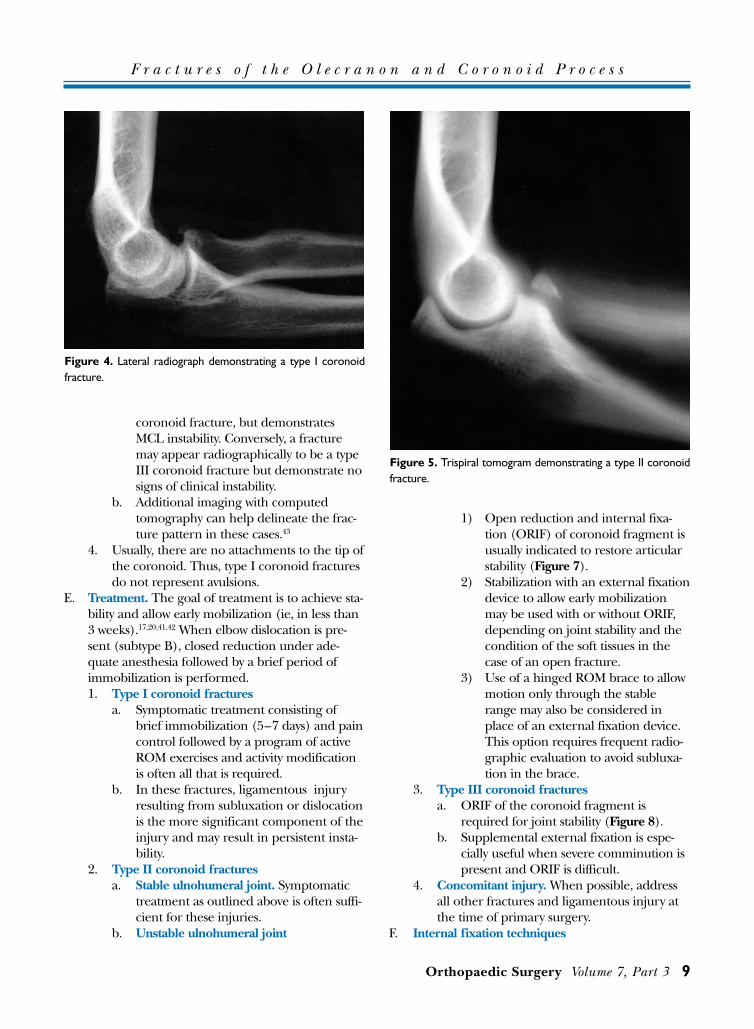
a. Type I fractures involve the coronoid tip(Figure 4).
b. Type II fractures involve 50% or less ofthe coronoid height (Figure 5).
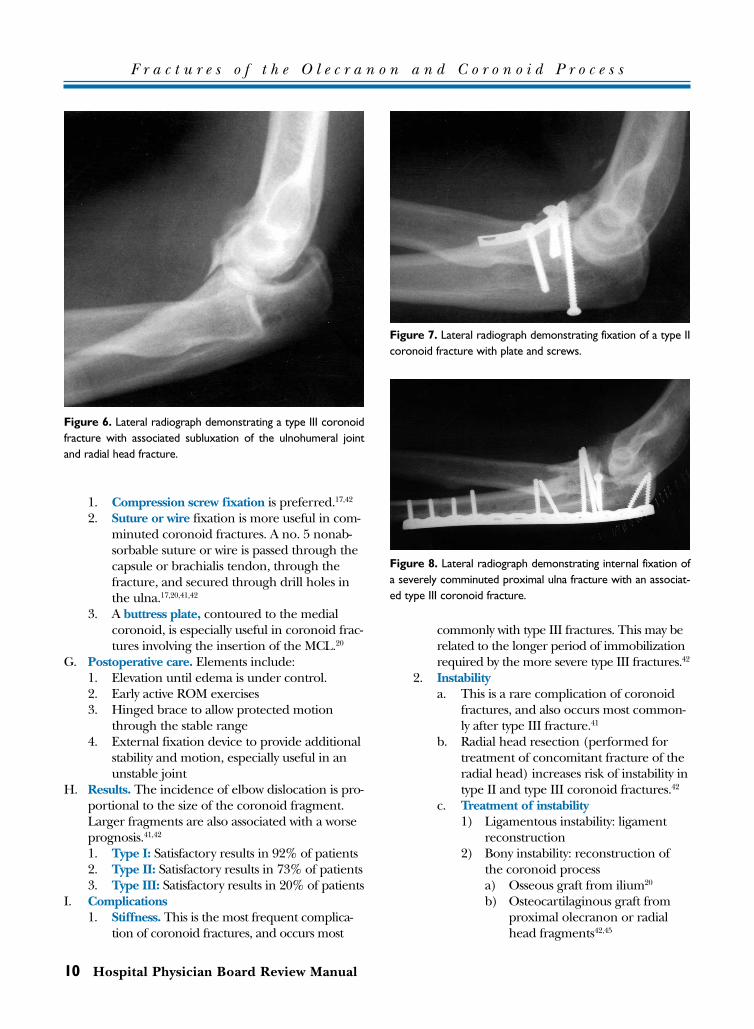
c. Type III fractures involve more than 50%of the coronoid height (Figure 6).
2. Subtypes. Each type is subdivided as follows:a. Subtype A: without elbow dislocationb. Subtype B: with elbow dislocation
B. Incidence41
1. Isolated injury. Coronoid fractures rarelyoccur as isolated injuries.
2. Combined injury
a. Concurrent dislocation or fracture: inci-dence by coronoid fracture type:1) Type I: 36%2) Type II: 56%3) Type III: 80%
b. Posterior elbow dislocation: 2% to 10% ofpatients with posterior elbow dislocationalso have associated coronoid fracture.
c. Fractures of radial head, medial humeralepicondyle, and olecranon represent themost commonly associated fractures.
C. Mechanisms of injury20,41,42
1. Axial load2. Resisted elbow flexion 3. Shear force created as the coronoid sublux-
ates or dislocates over the trochleaD. Relevant anatomy43,44
1. The anterior capsule inserts an average of6.4 mm distal to the tip of the coronoid.Therefore, a type I coronoid fracture cannotrepresent an avulsion fracture. Instead, it rep-resents a shear fracture created by ulno-humeral subluxation or dislocation.
2. The brachialis inserts via a broad muscu-loaponeurotic attachment to the capsule,coronoid process, and proximal ulna. Theproximal margin is an average of 11 mmfrom the coronoid tip; therefore, it is onlyinvolved in type III coronoid fractures.
3. The anterior bundle of the medial collateralligament (MCL) inserts an average of 18.4 mmdorsal to the tip of the olecranon. Only in typeIII coronoid fractures would it be attached tothe free fragment. a. Obliquity or comminution of the coro-
noid fracture may result in a fracture thatappears radiographically to be a type II
8 Hospital Physician Board Review Manual
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
Figure 3. Regan-Morrey classification of coronoid fractures. Adapted with permission from Cabanela ME, Morrey BF. Fractures ofthe proximal ulna and olecranon. In: Morrey BF, editor. The elbow. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2001:420.
Type I Type II Type III
coronoid fracture, but demonstratesMCL instability. Conversely, a fracturemay appear radiographically to be a typeIII coronoid fracture but demonstrate nosigns of clinical instability.
b. Additional imaging with computedtomography can help delineate the frac-ture pattern in these cases.43
4. Usually, there are no attachments to the tip ofthe coronoid. Thus, type I coronoid fracturesdo not represent avulsions.
E. Treatment. The goal of treatment is to achieve sta-bility and allow early mobilization (ie, in less than3 weeks).17,20,41,42 When elbow dislocation is pre-sent (subtype B), closed reduction under ade-quate anesthesia followed by a brief period ofimmobilization is performed.1. Type I coronoid fractures
a. Symptomatic treatment consisting ofbrief immobilization (5–7 days) and paincontrol followed by a program of activeROM exercises and activity modificationis often all that is required.
b. In these fractures, ligamentous injury resulting from subluxation or dislocationis the more significant component of theinjury and may result in persistent insta-bility.
2. Type II coronoid fracturesa. Stable ulnohumeral joint. Symptomatic
treatment as outlined above is often suffi-cient for these injuries.
b. Unstable ulnohumeral joint
1) Open reduction and internal fixa-tion (ORIF) of coronoid fragment isusually indicated to restore articularstability (Figure 7).
2) Stabilization with an external fixationdevice to allow early mobilizationmay be used with or without ORIF,depending on joint stability and thecondition of the soft tissues in thecase of an open fracture.
3) Use of a hinged ROM brace to allowmotion only through the stablerange may also be considered inplace of an external fixation device.This option requires frequent radio-graphic evaluation to avoid subluxa-tion in the brace.
3. Type III coronoid fracturesa. ORIF of the coronoid fragment is
required for joint stability (Figure 8).b. Supplemental external fixation is espe-
cially useful when severe comminution ispresent and ORIF is difficult.
4. Concomitant injury. When possible, addressall other fractures and ligamentous injury atthe time of primary surgery.
F. Internal fixation techniques
Orthopaedic Surgery Volume 7, Part 3 9
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
Figure 4. Lateral radiograph demonstrating a type I coronoidfracture.
Figure 5. Trispiral tomogram demonstrating a type II coronoidfracture.
1. Compression screw fixation is preferred.17,42
2. Suture or wire fixation is more useful in com-minuted coronoid fractures. A no. 5 nonab-sorbable suture or wire is passed through thecapsule or brachialis tendon, through thefracture, and secured through drill holes inthe ulna.17,20,41,42
3. A buttress plate, contoured to the medialcoronoid, is especially useful in coronoid frac-tures involving the insertion of the MCL.20
G. Postoperative care. Elements include: 1. Elevation until edema is under control. 2. Early active ROM exercises 3. Hinged brace to allow protected motion
through the stable range4. External fixation device to provide additional
stability and motion, especially useful in anunstable joint
H. Results. The incidence of elbow dislocation is pro-portional to the size of the coronoid fragment.Larger fragments are also associated with a worseprognosis.41,42
1. Type I: Satisfactory results in 92% of patients2. Type II: Satisfactory results in 73% of patients3. Type III: Satisfactory results in 20% of patients
I. Complications1. Stiffness. This is the most frequent complica-
tion of coronoid fractures, and occurs most
commonly with type III fractures. This may berelated to the longer period of immobilizationrequired by the more severe type III fractures.42
2. Instabilitya. This is a rare complication of coronoid
fractures, and also occurs most common-ly after type III fracture.41
b. Radial head resection (performed fortreatment of concomitant fracture of theradial head) increases risk of instability intype II and type III coronoid fractures.42
c. Treatment of instability1) Ligamentous instability: ligament
reconstruction2) Bony instability: reconstruction of
the coronoid processa) Osseous graft from ilium20
b) Osteocartilaginous graft fromproximal olecranon or radialhead fragments42,45
10 Hospital Physician Board Review Manual
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
Figure 7. Lateral radiograph demonstrating fixation of a type IIcoronoid fracture with plate and screws.
Figure 8. Lateral radiograph demonstrating internal fixation ofa severely comminuted proximal ulna fracture with an associat-ed type III coronoid fracture.
Figure 6. Lateral radiograph demonstrating a type III coronoidfracture with associated subluxation of the ulnohumeral jointand radial head fracture.
3. Nonuniona. Type I fractures have been reported to
form loose bodies or symptomatic fibrousunion with hypertrophy of the fragment.These nonunions are amenable to arth-roscopic débridement and fragment exci-sion.46
b. Type II and type III fractures may requirerevision ORIF with bone grafting or coronoid reconstruction.
4. Posttraumatic arthrosis. The incidence of thiscomplication correlates with the age of thepatient at the time of the injury more thanwith injury severity.41 Joint congruity is also animportant factor.20
5. Heterotopic ossification. Heterotopic ossifica-tion that limits ROM is most common aftertype III fractures, and rare after type I frac-tures.41
BOARD REVIEW QUESTIONS
1. What percentage of posterior elbow dislocations areaccompanied by an associated coronoid fracture?A) 10%B) 40%C) 65%D) 80%
2. A displaced olecranon fracture with anterior sublux-ation of the radius and ulna is best treated by whichone of the following options?A) K-wire and tension band fixationB) Intramedullary screw fixationC) Plate fixationD) Fragment excision
3. In which one of the following clinical settings is exci-sion of an olecranon fragment most appropriate? A) The patient is skeletally immatureB) The patient is elderly and the fracture is com-
minuted C) The fracture involves 25% of the olecranonD) The fracture involves 80% of the olecranon
4. Which one of the following describes a type III ole-cranon fracture?A) Displaced and unstableB) StableC) NondisplacedD) Nondisplaced and stable
ANSWERS
REFERENCES
1. Cabanela ME, Morrey BF. Fractures of the olecranon. In:Morrey BF, editor. The elbow and its disorders. 3rd ed.Philadelphia: WB Saunders; 2000:365–79.
2. Howard JL, Urist MR. Fracture dislocation of radius andulna at the elbow joint. Clin Orthop 1958;12:276.
3. Coughlin MJ, Slabaugh PB, Smith TK. Experience withthe McAtee olecranon device in olecranon fractures.J Bone Joint Surg 1979;61A:385–8.
4. Weseley MS, Barenfeld PA, Eisenstein AL. The use of theZuelzer hook plate in fixation of olecranon fractures.J Bone Joint Surg 1976;58A:859–63.
5. Coonrad RW. Management of olecranon fractures andnonunion. In: Morrey BF, editor. The elbow. New York:Raven Press; 1994:1–95. Thompson RC, editor. Mastertechniques in orthopaedic surgery; Vol 1.
6. Fyfe IS, Mossad MM, Holdsworth BJ. Methods of fixationof olecranon fractures. An experimental mechanicalstudy. J Bone Joint Surg Br 1985;67B:367–72.
7. MacAusland WR. The treatment of fractures of the ole-cranon by longitudinal screw or nail fixation. Ann Surg1942;116:293.
8. Hume MC, Wiss DA. Olecranon fractures. A clinical andradiographic comparison of tension band wiring andplate fixation. Clin Orthop 1992;285:229–35.
9. Kozin SH, Berglund LJ, Cooney WP, et al. Biomechanicalanalysis of tension band fixation for olecranon fracturetreatment. J Shoulder Elbow Surg 1996;5:442–8.
10. Matthewson MH, McCreath SW. Tension band wiring inthe treatment of olecranon fractures. J Bone Joint Surg1975;57B:399.
11. Paremain GP, Novak VP, Jinnah RH, Belkoff SM. Bio-mechanical evaluation of tension band placement forthe repair of olecranon fractures. Clin Orthop 1997;335:325–30.
12. Wolfgang, G, Burke F, Bush D, et al. Surgical treatmentof displaced olecranon fractures by tension band wiringtechnique. Clin Orthop 1987;224:192–204.
13. King GJ, Lammens PN, Milne AD, et al. Plate fixation ofcomminuted olecranon fractures: an in vitro biome-chanical study. J Shoulder Elbow Surg 1996;5:437–41.
14. Nowinski RJ, Nork SE, Segina DN, Benirschke SK. Com-minuted fracture-dislocations of the elbow treated withan AO wrist fusion plate. Clin Orthop 2000;378:238–44.
1.A2.C3.B4.A
Orthopaedic Surgery Volume 7, Part 3 11
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
15. Aldredge GH, Gregory CF. Triceps advancement in ole-cranon fractures. J Bone Joint Surg 1969;51A:816.
16. An KN, Morrey BF, Chao EY. The effect of partial removalof proximal ulna on elbow constraint. Clin Orthop 1986;209:270–9.
17. Morrey BF. Current concepts in the treatment of frac-tures of the radial head, the olecranon, and the coro-noid. J Bone Joint Surg 1995;77A:316–27.
18. Murphy DF, Greene WB, Dameron TB Jr. Displaced ole-cranon fractures in adults: clinical evaluation. Clin Orthop1987;224:215–23.
19. Wainwright D. Fractures of the olecranon process. Br JSurg 1942;29:403.
20. O’Driscoll SW. Olecranon and coronoid fractures. In:Norris TR, editor. Orthopedic knowledge update.Shoulder and elbow. Rosemont (IL): American Academyof Orthopaedic Surgery; 1997:409–13.
21. Colton CL. Fractures of the olecranon in adults: classifi-cation and management. Injury 1973;5:121–9.
22. Müller ME. The comprehensive classification of fracturesof long bones. Berlin: Springer-Verlag; 1990.
23. Givon U, Pritsch M, Levy O, et al. Monteggia and equiv-alent lesions. A study of 41 cases. Clin Orthop 1997;337:208–15.
24. Wu C, Tai C, Shih C. Biomechanical comparison for dif-ferent configurations of tension band wiring techniquesin treating an olecranon fracture. J Trauma 2000;48:1063–7.
25. Walker LG. Painful olecranon physeal nonunion in anadult weight lifter. A case report. Clin Orthop 1995;311:125–8.
26. Scharplatz D, Allgower M. Fracture-dislocation of theelbow. Injury 1975;7:143–59.
27. Cobb TK, Morrey BF. Use of distraction arthroplasty inunstable fracture dislocations of the elbow. Clin Orthop1995;312:201–10.
28. Hildebrand KA, Patterson SD, Regan WD, et al. Func-tional outcome of semiconstrained total elbow arthro-plasty. J Bone Joint Surg Am 2000;82-A:1379–86.
29. Helm RH, Hornby R, Miller SW. The complications ofsurgical treatment of displaced fractures of the olecra-non. Injury 1987;18:48–50.
30. Prayson MJ, Williams JL, Marshall MP, et al. Bio-mechanical comparison of fixation methods in trans-verse olecranon fractures: a cadaveric study. J OrthopTrauma 1997;11:565–72.
31. Schatzker J. Olecranon fractures. In: Schatzker J, Tile M,editors. The rationale of operative fracture care. NewYork: Springer-Verlag; 1987:89–95.
32. Rowland SA, Burkhart SS. Tension band wiring of ole-cranon fractures. A modification of the AO technique.Clin Orthop 1992;277:238–42.
33. O’Driscoll SW. Technique for unstable olecranon frac-ture-subluxations. Op Tech Orthop 1994;4:49–53.
34. Horne JG, Tanzer TL. Olecranon fractures: a review of100 cases. J Trauma 1981;21:469–72.
35. Papagelopoulos PJ, Coonrad RW, Morrey BF. Nonunionof the olecranon and proximal ulna. In: Morrey BF, edi-tor. The elbow and its disorders. 3rd ed. Philadelphia:WB Saunders; 2000:380–95.
36. Papagelopoulos PJ, Morrey BF. Treatment of nonunion ofolecranon fractures. J Bone Joint Surg 1994;76B:627–35.
37. Gallay H, McKee MD. Operative treatment of nonunionsabout the elbow. Clin Orthop 2000;370:87–101.
38. Brighton CT, Black J, Friedenberg ZB, et al. A multicenterstudy of the treatment of non-union with constant directcurrent. J Bone Joint Surg 1981;63A:2–13.
39. Meals RA. The use of a flexor carpi ulnaris muscle flap inthe treatment of an infected nonunion of the proximalulna. A case report. Clin Orthop 1989;240:168–72.
40. Sharrard WJ, Sutcliffe ML, Robson MJ, Maceacern AG.The treatment of fibrous non-union of fractures by pulsingelectromagnetic stimulation. J Bone Joint Surg Br 1982;64:189–93.
41. Regan W, Morrey B. Fractures of the coronoid process ofthe ulna. J Bone Joint Surg 1989;71A:1348–54.
42. Regan WD, Morrey BF. Coronoid process and monteg-gia fractures. In: Morrey BF, editor. The elbow and its disorders. 3rd ed. Philadelphia: WB Saunders; 2000:396–408.
43. Cage DJ, Abrams RA, Callahan JJ, Botte MJ. Soft tissueattachments of the ulnar coronoid process. Clin Orthop1995;320:154–8.
44. Morrey BF, An KN. Functional anatomy of the ligamentsof the elbow. Clin Orthop 1985;201:84–90.
45. Moritomo H, Tada K, Yoshida T, Kwatsu N. Reconstruc-tion of the coronoid for chronic dislocation of the elbow.J Bone Joint Surg Br 1998;80B:490–2.
46. Liu SH, Henry M, Bowen R. Complications of type Icoronoid fractures in competitive athletes: report of twocases and review of the literature. J Shoulder Elbow Surg1996;5:223–7.
12 Hospital Physician Board Review Manual
F r a c t u r e s o f t h e O l e c r a n o n a n d C o r o n o i d P r o c e s s
Copyright 2001 by Turner White Communications Inc., Wayne, PA. All rights reserved.