Embed Size (px)
Citation preview

PPPs in Healthcare (SDG-3) and Education(SDG-4) sectors
Regional Event on Financing Sustainable InfrastructureDevelopment in Asia and the Pacific
Organized by the United Nations ESCAP
6-7 December, 2017

Page 2
PPPs in Healthcare sector (Contributing to SDG-3)
Page 3
Agenda
Goal and objectives1
Key challenges in the sector
Prevalent PPP models3
Examples and learnings4
2
Key recommendations5
Page 4
SDG-3 goal is to ensure healthy lives and promotewell-being for all at all
Goal: To ensure healthy lives and promote well-being for all at all ages
Achieve universal health coverage, including financial risk protection
Goa
ltar
gets
rela
ted
toP
PP
proj
ects
Access to quality essential health-care services
Access to safe, effective, quality and affordable essential medicines and vaccines
Substantially increase health financing in developing countries
Increase the recruitment, development, training and retention of the health workforce
Page 5
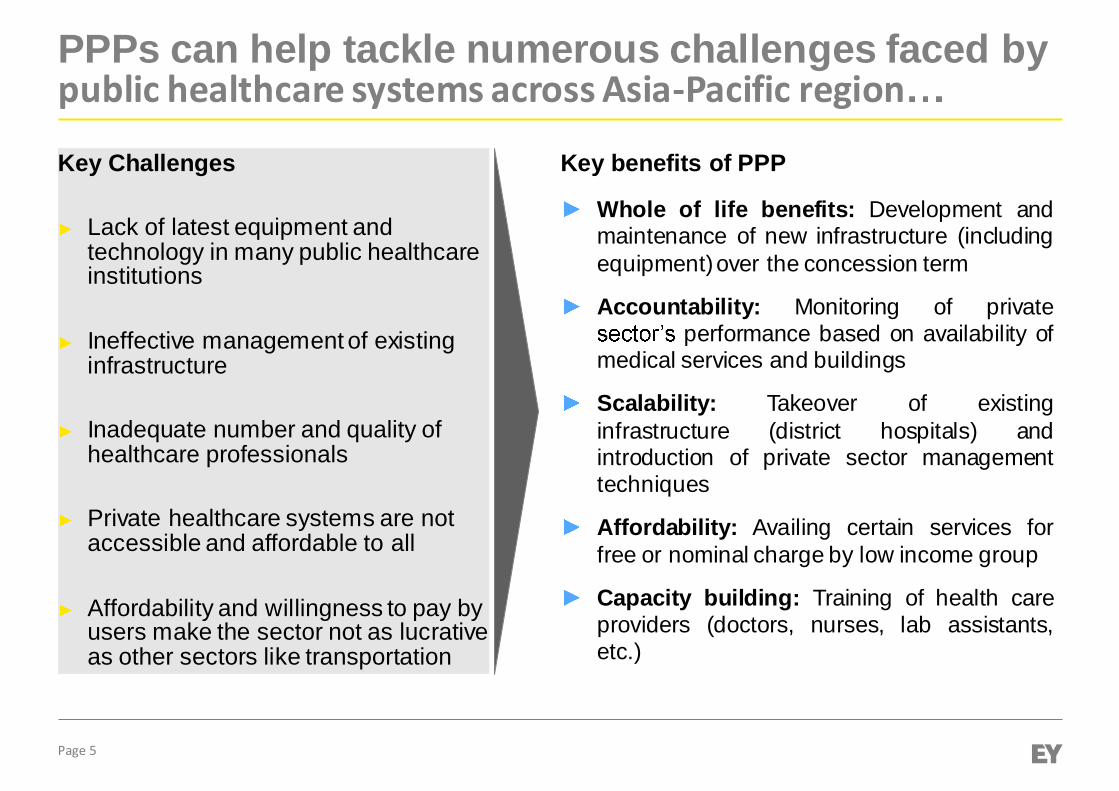
PPPs can help tackle numerous challenges faced bypublic healthcare systems across Asia-Pacific region
Key benefits of PPP
Whole of life benefits: Development andmaintenance of new infrastructure (includingequipment)over the concession term
Accountability: Monitoring of privateperformance based on availability of
medical services and buildings
Scalability: Takeover of existinginfrastructure (district hospitals) andintroduction of private sector managementtechniques
Affordability: Availing certain services forfree or nominal charge by low income group
Capacity building: Training of health careproviders (doctors, nurses, lab assistants,etc.)
Key Challenges
Lack of latest equipment andtechnology in many public healthcareinstitutions
Ineffective management of existinginfrastructure
Inadequate number and quality ofhealthcare professionals
Private healthcare systems are notaccessible and affordable to all
Affordability and willingness to pay byusers make the sector not as lucrativeas other sectors like transportation
Page 6
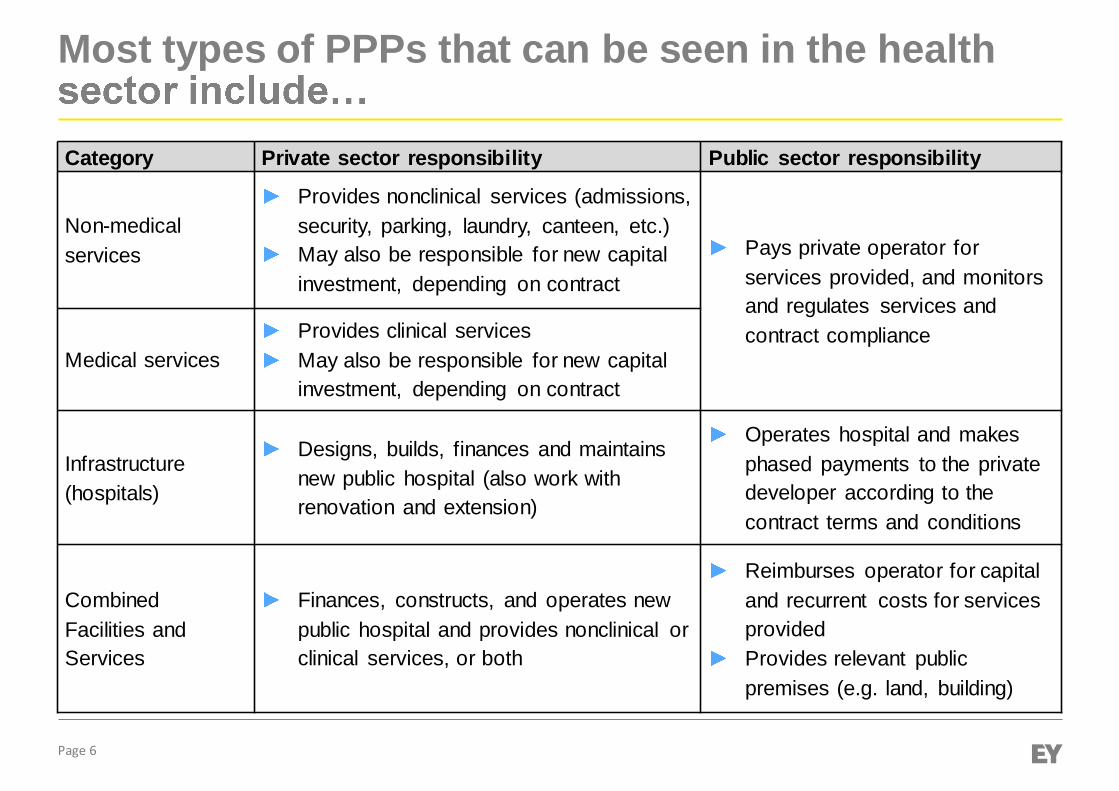
Most types of PPPs that can be seen in the health
Category Private sector responsibility Public sector responsibility
Non-medicalservices
Provides nonclinical services (admissions,security, parking, laundry, canteen, etc.)May also be responsible for new capitalinvestment, depending on contract
Pays private operator forservices provided, and monitorsand regulates services andcontract compliance
Medical servicesProvides clinical servicesMay also be responsible for new capitalinvestment, depending on contract
Infrastructure(hospitals)
Designs, builds, finances and maintainsnew public hospital (also work withrenovation and extension)
Operates hospital and makesphased payments to the privatedeveloper according to thecontract terms and conditions
CombinedFacilities andServices
Finances, constructs, and operates newpublic hospital and provides nonclinical orclinical services, or both
Reimburses operator for capitaland recurrent costs for servicesprovidedProvides relevant publicpremises (e.g. land, building)
Page 7
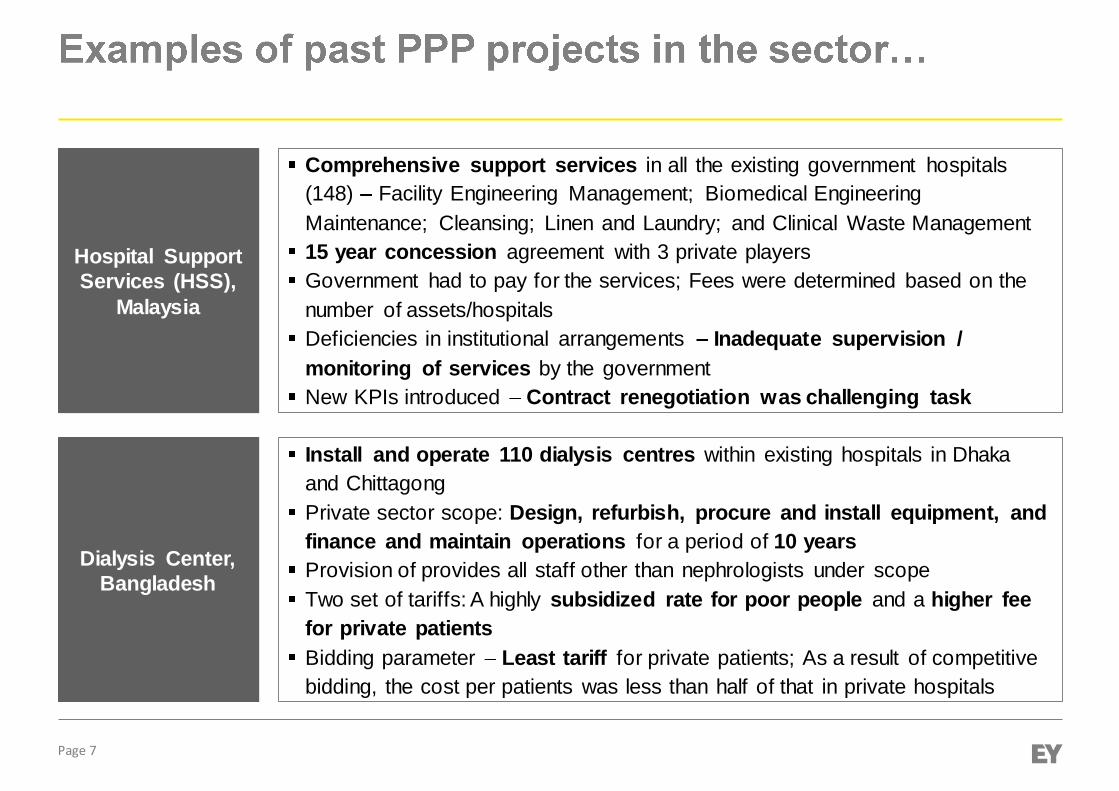
Dialysis Center,Bangladesh
Hospital SupportServices (HSS),
Malaysia
Comprehensive support services in all the existing government hospitals(148) Facility Engineering Management; Biomedical EngineeringMaintenance; Cleansing; Linen and Laundry; and Clinical Waste Management15 year concession agreement with 3 private playersGovernment had to pay for the services; Fees were determined based on thenumber of assets/hospitalsDeficiencies in institutional arrangements Inadequate supervision /monitoring of services by the governmentNew KPIs introduced Contract renegotiation was challenging task
Install and operate 110 dialysis centres within existing hospitals in Dhakaand ChittagongPrivate sector scope: Design, refurbish, procure and install equipment, andfinance and maintain operations for a period of 10 yearsProvision of provides all staff other than nephrologists under scopeTwo set of tariffs: A highly subsidized rate for poor people and a higher feefor private patientsBidding parameter Least tariff for private patients; As a result of competitivebidding, the cost per patients was less than half of that in private hospitals
Page 8
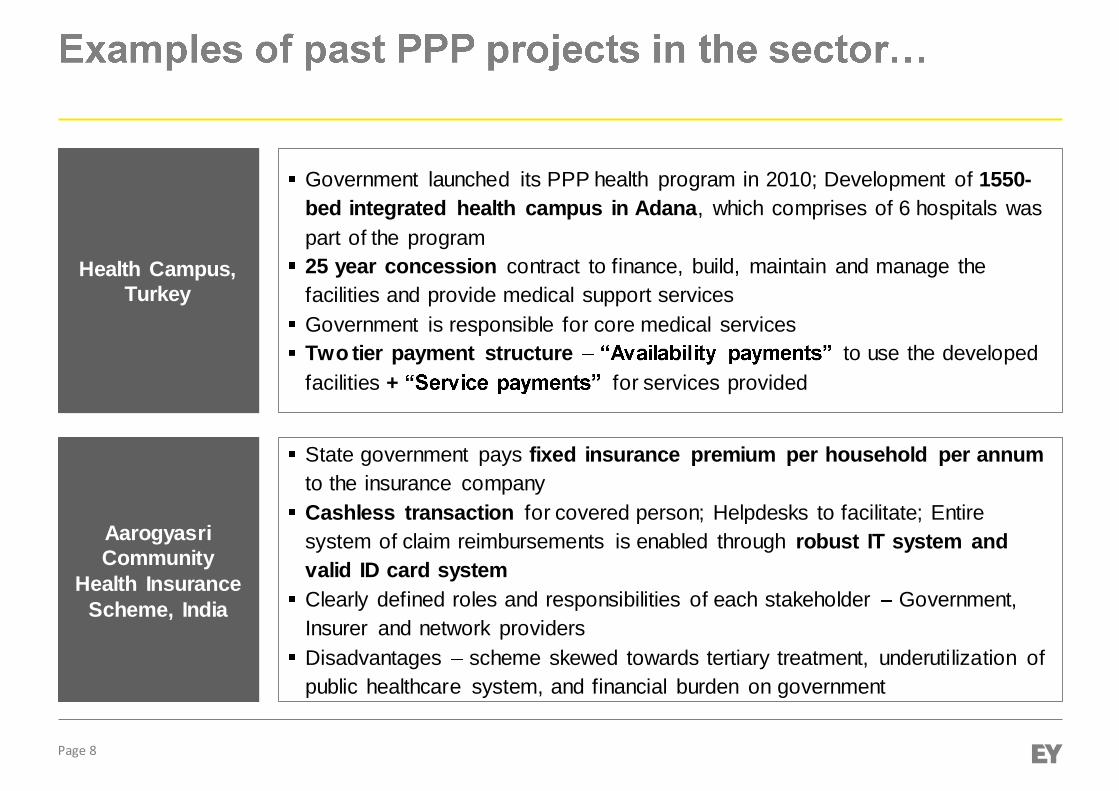
AarogyasriCommunity
Health InsuranceScheme, India
Health Campus,Turkey
Government launched its PPP health program in 2010; Development of 1550-bed integrated health campus in Adana, which comprises of 6 hospitals waspart of the program25 year concession contract to finance, build, maintain and manage thefacilities and provide medical support servicesGovernment is responsible for core medical servicesTwo tier payment structure to use the developedfacilities + for services provided
State government pays fixed insurance premium per household per annumto the insurance companyCashless transaction for covered person; Helpdesks to facilitate; Entiresystem of claim reimbursements is enabled through robust IT system andvalid ID card systemClearly defined roles and responsibilities of each stakeholder Government,Insurer and network providersDisadvantages scheme skewed towards tertiary treatment, underutilization ofpublic healthcare system, and financial burden on government
Page 9
EmergencyAmbulance
Services in TamilNadu, India
Telemedicineinitiative in
Karnataka, India
-medicine and Tele- -line health-care initiative in Karnataka, India.The project connects through telecommunication systems Coronary CareUnits Hrudayalayahospital in BangaloreThis provides access to specialists in underserved or unserved areas
To reduce the MMR in rural areas of Tamil Nadu, the government selectedSeva Nilayam (NGO partner) for implementation of the Emergency AmbulanceServices scheme in Theni district of Tamil NaduThe Government supports the scheme by supplying the vehicles while theNGO recruits the staff, operates the programme and maintains the vehiclesThis scheme was envisaged to be self-supporting through the collection ofuser charges, however revenues have been lower than anticipated
Page 10
Key recommendations
Better integration ofhealth sector into mainPPP framework
To establish andstrengthen regulatoryregime governinghealth infrastructure
To create enablingenvironment for universalhealth coverage
To distinguish betweensocial and economicsectorsTo strengthen the existingPPP framework or bring inhealth sector specific PPPpolicy or legislationTo detail out the deliverymodels that can be adoptedTo create awarenessamong government officialsToconfidence in undertakingthese projects
To create a robust systemthat would governdevelopment and operationof healthcare infrastructureTo ensure minimumstandards technical andoperations are maintainedthroughout the contractTo ensure accreditationsystem / mechanism forservices
To create enablingenvironment for maturity ofinsurance marketTo bring clarity on servicesrates and charges fordefined servicesPolicy on universal healthcoverage should becarefully drafted

Page 11
PPPs in Education sector (Contributing to SDG-4)
Page 12
Agenda
Goal and objectives1
Key challenges in the sector
Prevalent PPP models3
Examples and learnings4
2
Key recommendations5
Page 13
SDG-4 goal is to ensure inclusive and qualityeducation for all and promote lifelong
Goal: To ensure inclusive and quality education for all and promotelifelong learning
Provide free, equitable and quality primary and secondary education to all children
Goa
ltar
gets
rela
ted
toP
PP
proj
ects
Ensure inclusive and quality education for all and promote lifelong learning
Substantially increase the supply of qualified teachers, including through internationalcooperation for teacher training in developing countries
Substantially increase education sector in developing countries
Page 14
Key challenges faced by public education systems acrossAsia-Pacific region
Inadequate infrastructure facilities (huge demand supply gap in schools, colleges,vocational institutions)
Poor quality of infrastructure Lack of facilities such as toilets, playgrounds, labsetc.
Poor quality of staff, and outdated curriculum
Low enrolment rates, and high dropout rates (particularly among girl child)
Private schooling is costly and unaffordable to many
PPP projects in education include a focus on providing quality educational facilitiesand services without relying on user fees as the main source of revenue
Page 15
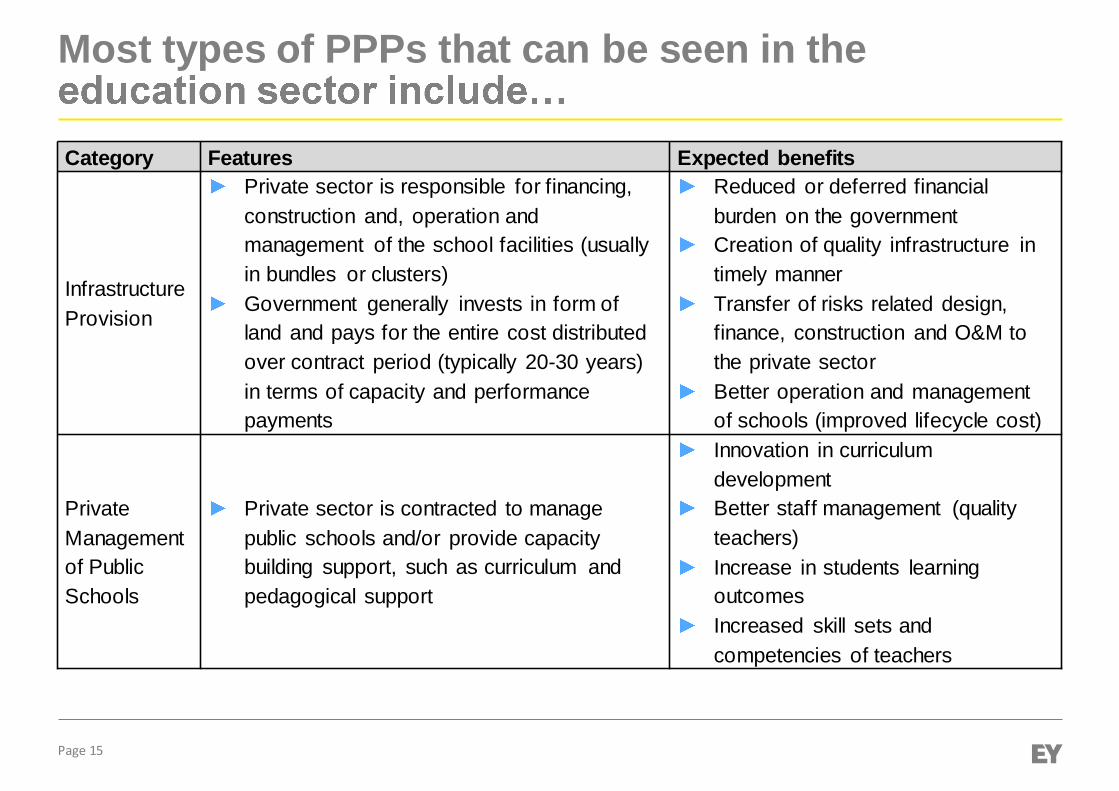
Most types of PPPs that can be seen in the
Category Features Expected benefits
InfrastructureProvision
Private sector is responsible for financing,construction and, operation andmanagement of the school facilities (usuallyin bundles or clusters)Government generally invests in form ofland and pays for the entire cost distributedover contract period (typically 20-30 years)in terms of capacity and performancepayments
Reduced or deferred financialburden on the governmentCreation of quality infrastructure intimely mannerTransfer of risks related design,finance, construction and O&M tothe private sectorBetter operation and managementof schools (improved lifecycle cost)
PrivateManagementof PublicSchools
Private sector is contracted to managepublic schools and/or provide capacitybuilding support, such as curriculum andpedagogical support
Innovation in curriculumdevelopmentBetter staff management (qualityteachers)Increase in students learningoutcomesIncreased skill sets andcompetencies of teachers
Page 16
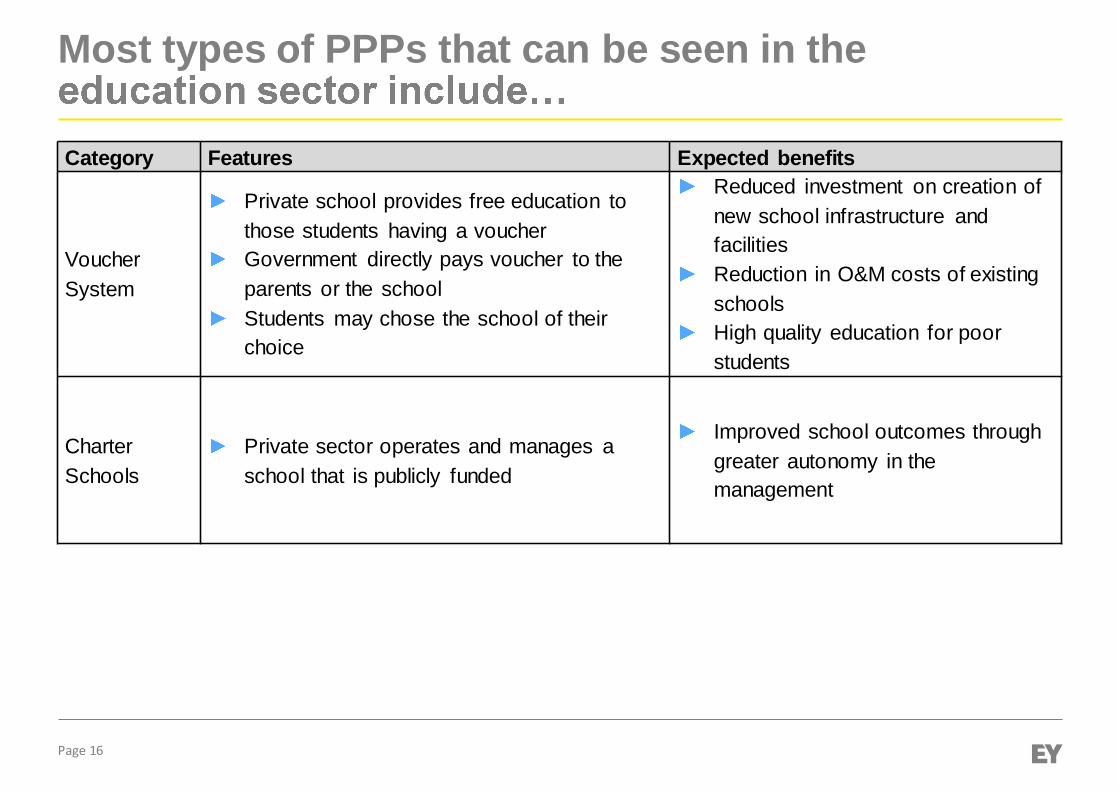
Most types of PPPs that can be seen in the
Category Features Expected benefits
VoucherSystem
Private school provides free education tothose students having a voucherGovernment directly pays voucher to theparents or the schoolStudents may chose the school of theirchoice
Reduced investment on creation ofnew school infrastructure andfacilitiesReduction in O&M costs of existingschoolsHigh quality education for poorstudents
CharterSchools
Private sector operates and manages aschool that is publicly funded
Improved school outcomes throughgreater autonomy in themanagement
Page 17
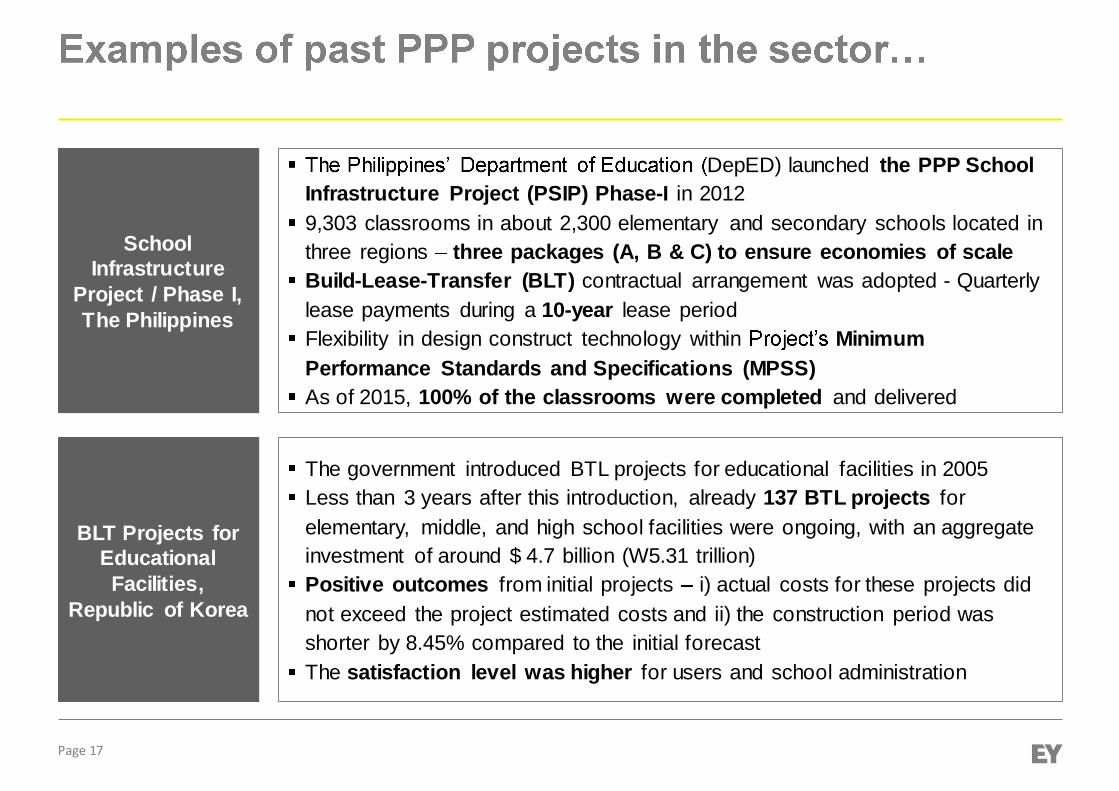
BLT Projects forEducationalFacilities,
Republic of Korea
SchoolInfrastructure
Project / Phase I,The Philippines
DepED) launched the PPP SchoolInfrastructure Project (PSIP) Phase-I in 20129,303 classrooms in about 2,300 elementary and secondary schools located inthree regions three packages (A, B & C) to ensure economies of scaleBuild-Lease-Transfer (BLT) contractual arrangement was adopted - Quarterlylease payments during a 10-year lease periodFlexibility in design construct technology within MinimumPerformance Standards and Specifications (MPSS)As of 2015, 100% of the classrooms were completed and delivered
The government introduced BTL projects for educational facilities in 2005Less than 3 years after this introduction, already 137 BTL projects forelementary, middle, and high school facilities were ongoing, with an aggregateinvestment of around $ 4.7 billion (W5.31 trillion)Positive outcomes from initial projects i) actual costs for these projects didnot exceed the project estimated costs and ii) the construction period wasshorter by 8.45% compared to the initial forecastThe satisfaction level was higher for users and school administration
Page 18
Quality SupportModel with
Government ofHaryana andPunjab, India
Trust SchoolModel, Malaysia
In 2010, the Ministry of Education launched the Trust School Programmetogether with Yayasan AMIR, which is a not-for-profit organization establishedto improve accessibility of quality education in Malaysian Government schoolsBy providing technical and financial assistance over a 5-year programme,Yayasan AMIR aims to improve the curriculum and delivery of education aswell as the management of schoolsThe programme started with 10 pilot schools but there were already 62 trustschools in nine states as of 2016. The objective is to raise this number to 700by 2025.
The Quality Support Model is an initiative by the Bharti Foundation in Indiathat intends to strengthen and improve quality of education in GovernmentSchools.Government continues to own the school with its existing teachers, fundsand resourcesBharti Foundation offers technical expertise and guidance - Improvement inacademic and non-academic processes, Infrastructure development /enhanced utilization of existing infrastructure / resources, Capacitydevelopment of school leadership and teachers
Page 19
Voucher System
Voucher like system In India, the Right to Education Act, 2009, mandates thereservation of 25% of the seats in the private school from economicallyweaker section (EWS) of the society for whom the government wouldreimburse the private schools on per student basis.The was enacted and launched in 1990and is considered first modern private school choice programValue of voucher is critical Voucher value in Milwaukee,USA was approximately USD 7,384 which was just more than half thegovernment spending on per student in public schools.Increasing voucher value can result in more participation from the privateschools.Another important aspect is to evaluate the performance of a student preand post admission in a private school.
Page 20
Key recommendations
Robust selection process andobjective selection Criteria
(To clarify the requirements, expectedservices and outcomes in the biddingdocuments; Selection criteria should beobjective)
Well-defined contract terms andprovisions
(PPP contract should clearly spell out thelevel of autonomy for the private partner interms of pedagogy, staffing and budgeting;financial terms in a transparent manner)
Strong monitoring and evaluationframework
(PPP contract should outline clear,measurable and attainable performancestandards with associated penalties)
Remuneration linked toperformance
(Fixed and variable payments - Thefixed component ensures thatunderperforming schools are notimmediately cut off and have sufficienttime to turnaround performance)
Fiscal sustainability
(The financial viability of PPP projects in education depends mainly on well-defined regularpayments capacity and service payments - from public authorities)

Page 21
Thank YouAbhaya AgarwalPartner - Infrastructure and PPP
Ernst & Young LLP3rd & 6th Floor, Worldmark-1;IGI AirportHospitality District; Aerocity, New Delhi,110037, India
Phone: +91 11 66233060Email: [email protected]