Embed Size (px)
Citation preview
Poster Design & Printing by Genigraphics® - 800.790.4001
INTRODUCTION
METHODS AND MATERIALSCONCLUSIONS
DISCUSSION
RESULTS REFERENCES
Table 2. Duration of hospitalisation and cost
Figure 1. Patient randomisation
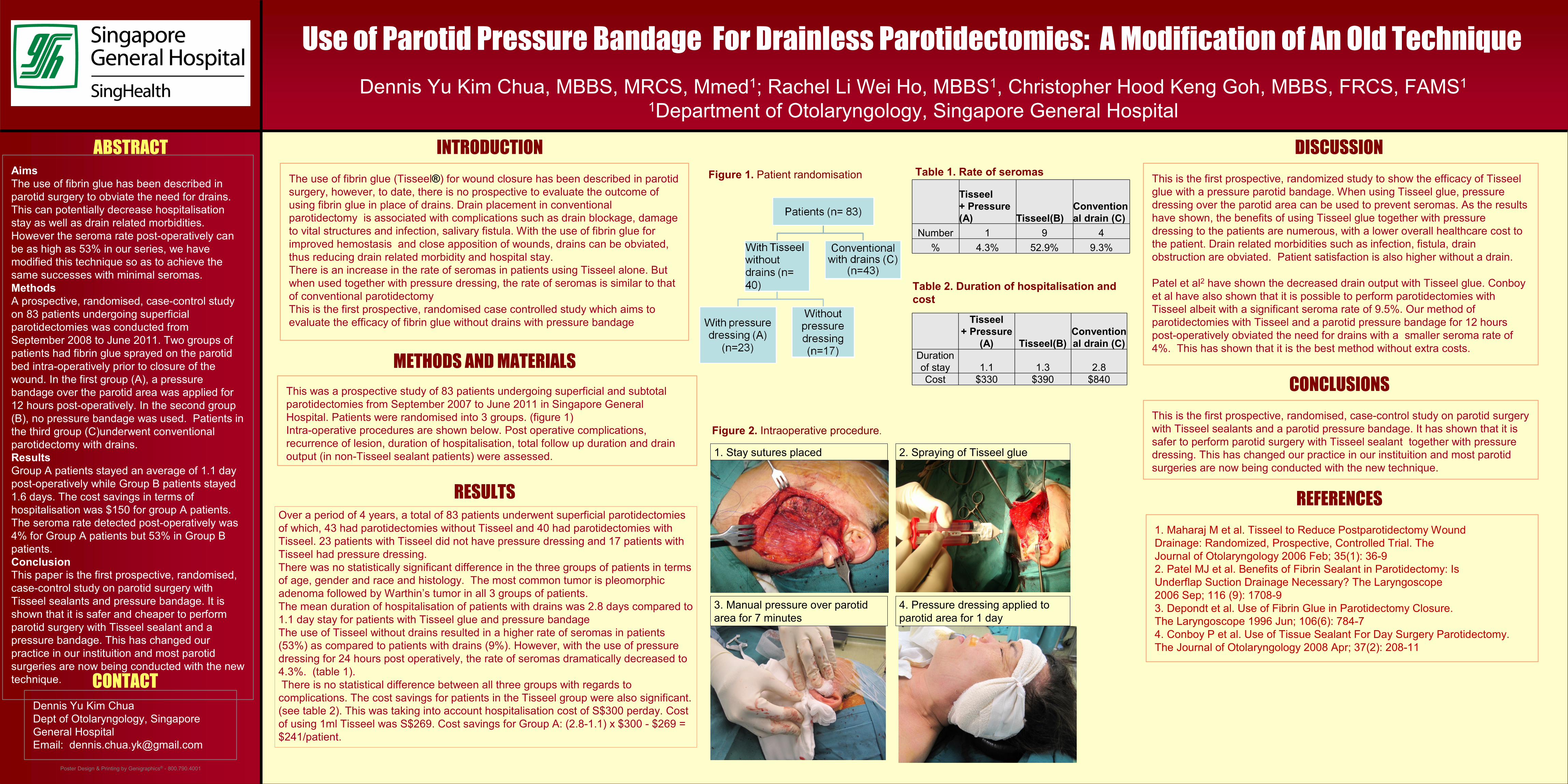
Figure 2. Intraoperative procedure.
ABSTRACT
CONTACTDennis Yu Kim ChuaDept of Otolaryngology, Singapore General HospitalEmail: [email protected]
Aims The use of fibrin glue has been described in parotid surgery to obviate the need for drains. This can potentially decrease hospitalisation stay as well as drain related morbidities. However the seroma rate post-operatively can be as high as 53% in our series, we have modified this technique so as to achieve the same successes with minimal seromas. MethodsA prospective, randomised, case-control study on 83 patients undergoing superficial parotidectomies was conducted from September 2008 to June 2011. Two groups of patients had fibrin glue sprayed on the parotid bed intra-operatively prior to closure of the wound. In the first group (A), a pressure bandage over the parotid area was applied for 12 hours post-operatively. In the second group (B), no pressure bandage was used. Patients in the third group (C)underwent conventional parotidectomy with drains.ResultsGroup A patients stayed an average of 1.1 day post-operatively while Group B patients stayed 1.6 days. The cost savings in terms of hospitalisation was $150 for group A patients. The seroma rate detected post-operatively was 4% for Group A patients but 53% in Group B patients. ConclusionThis paper is the first prospective, randomised, case-control study on parotid surgery with Tisseel sealants and pressure bandage. It is shown that it is safer and cheaper to perform parotid surgery with Tisseel sealant and a pressure bandage. This has changed our practice in our instituition and most parotid surgeries are now being conducted with the new technique.
This is the first prospective, randomized study to show the efficacy of Tisseel glue with a pressure parotid bandage. When using Tisseel glue, pressure dressing over the parotid area can be used to prevent seromas. As the results have shown, the benefits of using Tisseel glue together with pressure dressing to the patients are numerous, with a lower overall healthcare cost to the patient. Drain related morbidities such as infection, fistula, drain obstruction are obviated. Patient satisfaction is also higher without a drain.
Patel et al2 have shown the decreased drain output with Tisseel glue. Conboyet al have also shown that it is possible to perform parotidectomies with Tisseel albeit with a significant seroma rate of 9.5%. Our method of parotidectomies with Tisseel and a parotid pressure bandage for 12 hours post-operatively obviated the need for drains with a smaller seroma rate of 4%. This has shown that it is the best method without extra costs.
This was a prospective study of 83 patients undergoing superficial and subtotal parotidectomies from September 2007 to June 2011 in Singapore General Hospital. Patients were randomised into 3 groups. (figure 1)Intra-operative procedures are shown below. Post operative complications, recurrence of lesion, duration of hospitalisation, total follow up duration and drain output (in non-Tisseel sealant patients) were assessed.
This is the first prospective, randomised, case-control study on parotid surgery with Tisseel sealants and a parotid pressure bandage. It has shown that it is safer to perform parotid surgery with Tisseel sealant together with pressure dressing. This has changed our practice in our instituition and most parotid surgeries are now being conducted with the new technique.
The use of fibrin glue (Tisseel®) for wound closure has been described in parotid surgery, however, to date, there is no prospective to evaluate the outcome of using fibrin glue in place of drains. Drain placement in conventional parotidectomy is associated with complications such as drain blockage, damage to vital structures and infection, salivary fistula. With the use of fibrin glue for improved hemostasis and close apposition of wounds, drains can be obviated, thus reducing drain related morbidity and hospital stay. There is an increase in the rate of seromas in patients using Tisseel alone. But when used together with pressure dressing, the rate of seromas is similar to that of conventional parotidectomyThis is the first prospective, randomised case controlled study which aims to evaluate the efficacy of fibrin glue without drains with pressure bandage
1. Maharaj M et al. Tisseel to Reduce Postparotidectomy WoundDrainage: Randomized, Prospective, Controlled Trial. TheJournal of Otolaryngology 2006 Feb; 35(1): 36-92. Patel MJ et al. Benefits of Fibrin Sealant in Parotidectomy: IsUnderflap Suction Drainage Necessary? The Laryngoscope2006 Sep; 116 (9): 1708-93. Depondt et al. Use of Fibrin Glue in Parotidectomy Closure.The Laryngoscope 1996 Jun; 106(6): 784-74. Conboy P et al. Use of Tissue Sealant For Day Surgery Parotidectomy. The Journal of Otolaryngology 2008 Apr; 37(2): 208-11
Use of Parotid Pressure Bandage For Drainless Parotidectomies: A Modification of An Old Technique
Dennis Yu Kim Chua, MBBS, MRCS, Mmed1; Rachel Li Wei Ho, MBBS1, Christopher Hood Keng Goh, MBBS, FRCS, FAMS1
1Department of Otolaryngology, Singapore General Hospital
Over a period of 4 years, a total of 83 patients underwent superficial parotidectomies of which, 43 had parotidectomies without Tisseel and 40 had parotidectomies with Tisseel. 23 patients with Tisseel did not have pressure dressing and 17 patients with Tisseel had pressure dressing.There was no statistically significant difference in the three groups of patients in terms of age, gender and race and histology. The most common tumor is pleomorphic adenoma followed by Warthin’s tumor in all 3 groups of patients.The mean duration of hospitalisation of patients with drains was 2.8 days compared to 1.1 day stay for patients with Tisseel glue and pressure bandageThe use of Tisseel without drains resulted in a higher rate of seromas in patients (53%) as compared to patients with drains (9%). However, with the use of pressure dressing for 24 hours post operatively, the rate of seromas dramatically decreased to 4.3%. (table 1). There is no statistical difference between all three groups with regards to
complications. The cost savings for patients in the Tisseel group were also significant. (see table 2). This was taking into account hospitalisation cost of S$300 perday. Cost of using 1ml Tisseel was S$269. Cost savings for Group A: (2.8-1.1) x $300 - $269 = $241/patient.
1. Stay sutures placed 2. Spraying of Tisseel glue
3. Manual pressure over parotid area for 7 minutes
4. Pressure dressing applied to parotid area for 1 day
Table 1. Rate of seromas
Tisseel+ Pressure (A) Tisseel(B)
Conventional drain (C)
Number 1 9 4% 4.3% 52.9% 9.3%
Tisseel+ Pressure
(A) Tisseel(B)Conventional drain (C)
Duration of stay 1.1 1.3 2.8Cost $330 $390 $840




























