Embed Size (px)
Citation preview
Poster Design & Printing by Genigraphics® - 800.790.4001
Effect of the 532nm Pulsed KTP Laser in the Treatment of Reinke’s Edema
Pitman, MJ1, Lebowitz A1, Iacob C1, Tan M2
New York Eye and Ear Infirmary, Department of Otolaryngology 1Montefiore Medical Center, Department of Otorhinolaryngology2
INTRODUCTION
RESULTS
ABSTRACT
Objective: To evaluate the effect and safety of the 532nm Pulsed Potassium-Titanyl-Phosphate (KTP) laser in the office-based treatment of patients with Reinke's edema using objective and subjective scaled outcome measures.
Study Design: Case Series
Setting: Tertiary hospital center
Subjects: Seven adult females undergoing in-office KTP laser treatment for Reinke's Edema
Methods: Participants were studied pre and post treatment. Vocal function was evaluated by objective aerodynamic and acoustic analysis. Subjective changes were evaluated using the GRBAS scale, Voice Handicap Index and videostroboscopy.Histologic effects of the laser were investigated by comparing one patient treated with laser one year prior to excision, one treated with laser just prior to excision, and one control patient who underwent excision without prior laser treatment.
Results: At an average post-operative follow up of 17.8 weeks (range 5-78), maximumphonation time trended toward improvement. The median VHI score decreased from 37 to 26 (p=0.150). There was a reduction in each component of the GRBAS scoring and the median fundamental frequency increased from 162 to 186 (p=0.625). Stroboscopic findings demonstrated an intact post-treatment mucosal wave. Histologic comparison of the tissue effects of laser in three patients demonstrated changes in vocal fold vascularity but no acute or long-term damage to the overlying epithelium.
Conclusion: Objective and subjective scaled measures suggest that treatment of Reinke's edema in the office with a 532nm KTP laser results in improved voice. It appears safe with histologic preservation of the vocal fold vibratory epithelium and persistence of mucosal wave.
DISCUSSION
• VHI and GRBAS scoring demonstrated subjective improvement at an average of 17.8 weeks (range 5-78) after a single KTP laser treatment to each vocal fold.
• Decrease in the median VHI score is promising and includes one patient (patient #6) who was evaluated at 18 months post-treatment with KTP laser which suggests potential long-term benefit.
• Trend toward improvement in maximum phonation time may reflect a decrease in the edema of Reinke’s space, allowing for improved glottic efficiency.
• Median fundamental frequency increased from 162 to 186 which would change a voice perceived as masculine to a one perceived as desirably feminine.
• Histologic analysis of 3 RE patients managed differently allowed an assessment of the tissue effect of the KTP laser on the human vocal fold.
• Findings support the use of the KTP laser as a photoangiolytic laser targeting the vasculature without collateral damage to the surrounding tissue.
• Evaluation one year post laser treatment shows persistent vessel wall injury and a decrease in the myxoid and edematous stromal changes seen in RE.
Patients. In the study period between 2008 and 2009, 7 patients identified with RE (Grade II or III) were included. Inclusion criteria: diagnosis of bilateral RE by primary investigator (MP), men and women ages 18-70, who refused or failed a trial of conservative medical therapy and voice therapy.
Evaluation.• Patients underwent videostroboscopy and
laryngeal function testing. • The voice quality was subjectively evaluated
using the Voice Handicap Index - 10 (VHI) and the GRBAS scales (blindly rated by 2 trained laryngologists and a speech-language pathologist).
• Laryngeal function was assessed by several acoustic and physiologic measures, at the same time points as the subjective evaluations.
Treatment.• In the office endoscopy suite, the vocal fold was
treated with the KTP laser set at 35 watts with a pulsed width of 15 milliseconds.
• The end point was visualized blanching of the vocal fold at the time of laser treatment (Figure 1).
• An average of 93.1 joules (range 44-141) was delivered at a given session.
• Five patients were staged, receiving an average of 91 joules delivered per side,
• Two patients received an average of 103 joules to bilateral vocal folds in one setting.
• Staged patients underwent a total of 2 treatments while those who were not staged underwent a single treatment.
Although Reinke’s Edema (RE) is a benign disease, intervention is often indicated to improve voice quality and laryngeal function. Treatment begins with elimination of smoking, as well as addressing factors such as laryngopharyngeal reflux which may exacerbate the dysphonia. Short-term voice therapy is appropriate to introduce optimal vocal behavior and reduce vocal abuse. There is no universally accepted single surgical approach to the treatment of RE. Recently, studies have reported safe in-office treatment of RE with both the 585nm Pulse Dye (PDL) and the 532nm KTP in-office photoangiolytic lasers, however, to date, a quantitative evaluation of the benefits has yet to be reported.
We present a case series of 7 patients with clinically diagnosed RE who were treated with a 532nm KTP laser. Their voice improvement was subjectively and objectively evaluated before and after treatment. Additionally, we compared the pathologic effect of laser treatment in two cases to the histologic findings in a patient who had not been treated with laser.
METHODS AND MATERIALS
1. Koufman J WS. Unsedated, Office Based Treatment of Reinke’s Edema (Polypoid Degeneration) with the Pulsed Dye Laser: A Preliminary Report. Unpublished Presented at the Triological Society Southern Section Meeting January 2006 2006.
2. Lumpkin SM, Bennett S, Bishop SG. Postsurgical follow-up study of patients with severe polypoid degeneration. Laryngoscope 1990;100:399-402.
3. Lumpkin SM, Bishop SG, Bennett S. Comparison of surgical techniques in the treatment of laryngeal polypoid degeneration. Ann Otol Rhinol Laryngol 1987;96:254-7.
4. Mouadeb DA, Belafsky PC. In-office laryngeal surgery with the 585nm pulsed dye laser (PDL). Otolaryngol Head Neck Surg 2007;137:477-81.
5. Murry T, Abitbol J, Hersan R. Quantitative assessment of voice quality following laser surgery for Reinke's edema. J Voice 1999;13:257-64.
6. Yonekawa H. A clinical study of Reinke's edema. Auris Nasus Larynx 1988;15:57-78.
7. Zeitels SM, Akst LM, Burns JA, Hillman RE, Broadhurst MS, Anderson RR. Office-based 532-nm pulsed KTP laser treatment of glottal papillomatosis and dysplasia. Ann Otol Rhinol Laryngol 2006;115:679-85.
8. Zeitels SM, Hillman RE, Bunting GW, Vaughn T. Reinke's edema: phonatorymechanisms and management strategies. Ann Otol Rhinol Laryngol 1997;106:533-43.
CONCLUSIONS
SELECTED REFERENCES
Michael J Pitman, MDVoice and Swallowing InstituteDepartment of OtolaryngologyNew York Eye & Ear Infirmary
New York, NY [email protected]
CONTACTTable 1 GRBAS scores Pre-treatment Post-Treatment
G R B A S G R B A SPatient #1 2 2.1 1 0.7 1.8 1.4 1.4 0.2 0.2 1.2Patient #2 2.3 2.3 1.1 0.8 2 1.7 1.8 0.4 0.3 1.3Patient #3 1.9 1.9 0.9 0.6 1.3 1 1 0.1 0 0.7Patient #4 2.3 2.3 1.7 1.2 2 1 1.1 0.3 0 0.8Patient #5 2.8 3 2 0 3 3 3 2 0 2.9Patient #6 1.8 2 1.9 0.4 1.4 0.9 1 0.2 0.1 0.4Patient #7 1.7 1.8 1 0.4 1.6 1.7 2 1.7 0.7 1.8Averages 2.1 2.2 1.4 0.6 1.9 1.5 1.6 0.7 0.2 1.3
Figure 1. Vocal folds pre-treatment (1A). Demonstrating the ischemic end point immediately post-treatment (1B). Six weeks post-treatment the vocal folds are completely healed with mild residual RE.(1C) This result is representative of the general reduction achieved in Reinke’s edema after a single KTP laser treatment.
Table 1. There was a reduction in all components of the GRBAS scoring in the post-treatment evaluation when compared to the pre-treatment evaluation.
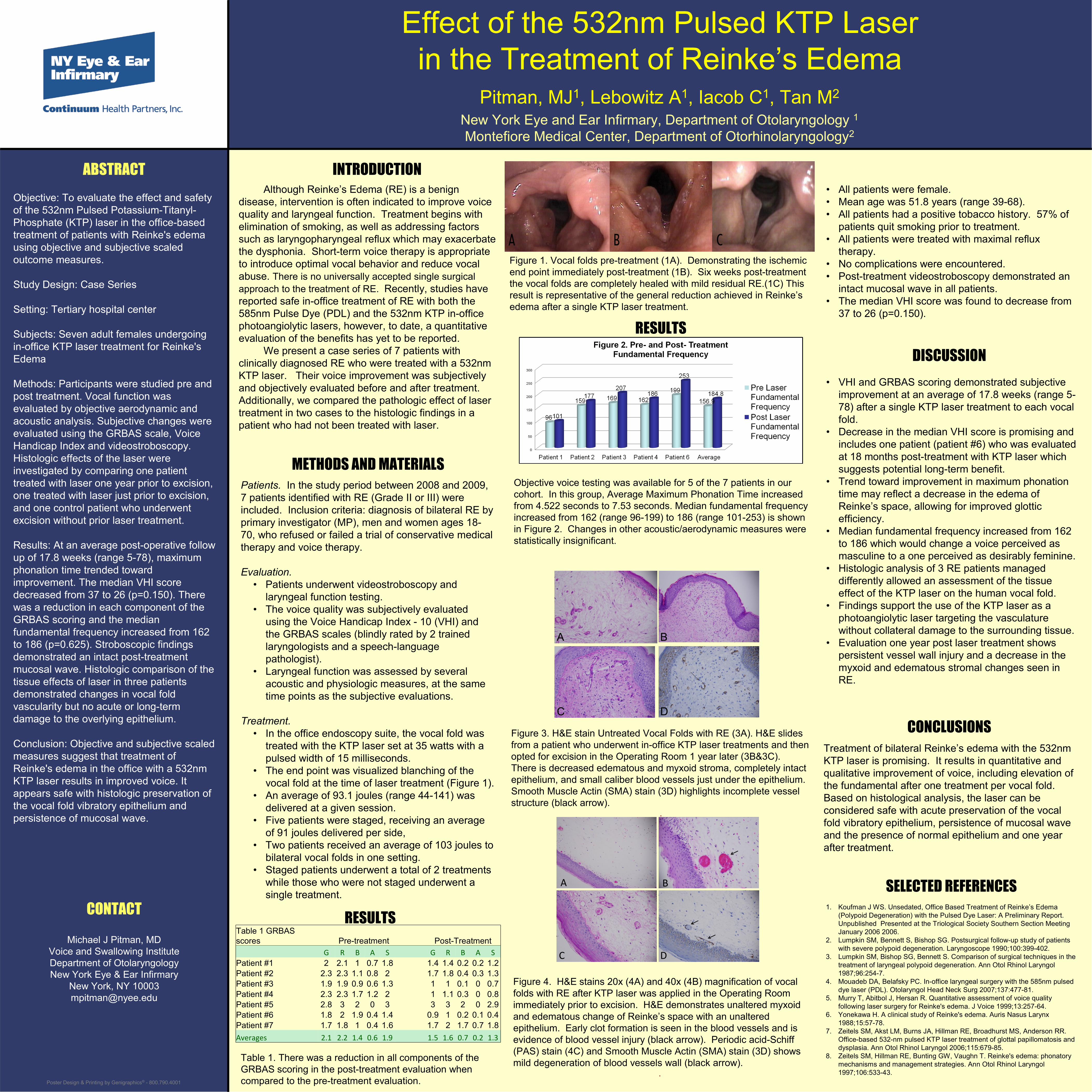
Objective voice testing was available for 5 of the 7 patients in our cohort. In this group, Average Maximum Phonation Time increasedfrom 4.522 seconds to 7.53 seconds. Median fundamental frequencyincreased from 162 (range 96-199) to 186 (range 101-253) is shown in Figure 2. Changes in other acoustic/aerodynamic measures were statistically insignificant.
Figure 3. H&E stain Untreated Vocal Folds with RE (3A). H&E slides from a patient who underwent in-office KTP laser treatments and then opted for excision in the Operating Room 1 year later (3B&3C). There is decreased edematous and myxoid stroma, completely intact epithelium, and small caliber blood vessels just under the epithelium. Smooth Muscle Actin (SMA) stain (3D) highlights incomplete vessel structure (black arrow).
.
Treatment of bilateral Reinke’s edema with the 532nm KTP laser is promising. It results in quantitative and qualitative improvement of voice, including elevation of the fundamental after one treatment per vocal fold. Based on histological analysis, the laser can be considered safe with acute preservation of the vocal fold vibratory epithelium, persistence of mucosal wave and the presence of normal epithelium and one year after treatment.
RESULTS
• All patients were female. • Mean age was 51.8 years (range 39-68). • All patients had a positive tobacco history. 57% of
patients quit smoking prior to treatment. • All patients were treated with maximal reflux
therapy. • No complications were encountered.• Post-treatment videostroboscopy demonstrated an
intact mucosal wave in all patients. • The median VHI score was found to decrease from
37 to 26 (p=0.150).
Figure 4. H&E stains 20x (4A) and 40x (4B) magnification of vocal folds with RE after KTP laser was applied in the Operating Room immediately prior to excision. H&E demonstrates unaltered myxoid and edematous change of Reinke’s space with an unaltered epithelium. Early clot formation is seen in the blood vessels and is evidence of blood vessel injury (black arrow). Periodic acid-Schiff (PAS) stain (4C) and Smooth Muscle Actin (SMA) stain (3D) shows mild degeneration of blood vessels wall (black arrow).
.
A B
C D
A B
C D





























