Embed Size (px)
DESCRIPTION
GI and Endocrine Case Study
Citation preview
NR 340 Module 8+9 Case Studies

J.R.
• J.R. is a 35-year-old female with a history of hypothyroidism and alcohol abuse. She presents to the emergency department with complaints of vomiting bright red blood. Her vital signs are as follows:
Temperature 36.6 ˚C
Heart Rate- HIGH 110 bpm
Respiratory Rate 22 breaths/min
Blood pressure- LOW 96/60 mmHg
Oxygen Saturation 100% on 2L nasal cannula
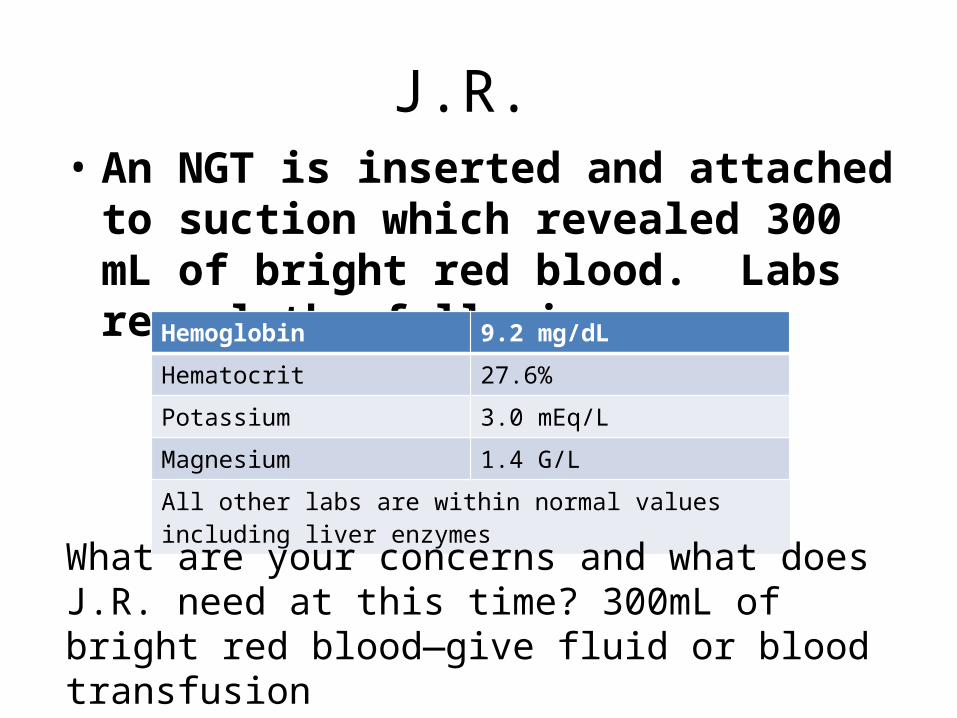
J.R. • An NGT is inserted and attached to suction
which revealed 300 mL of bright red blood. Labs reveal the following:
Hemoglobin 9.2 mg/dL
Hematocrit 27.6%
Potassium 3.0 mEq/L
Magnesium 1.4 G/L
All other labs are within normal values including liver enzymes
What are your concerns and what does J.R. need at this time? 300mL of bright red blood—give fluid or blood transfusion

J.R.
• Two 18 gauge IV’s are inserted one in the left antecubital space and the other in the right forearm. The patient is given a one liter bolus of IV 0.9 normal saline. J.R. is taken to the endoscopy suite and undergoes an EGD to determine the cause of bleeding.
J.R.
• J.R. undergoes the endoscopy and a Mallory-Weiss tear Longitudinal tear is discovered in her esophagus. The site is injected with epinephrine to stop the bleeding and she is transferred to the ICU for airway management and hemodynamic monitoring.
J.R.
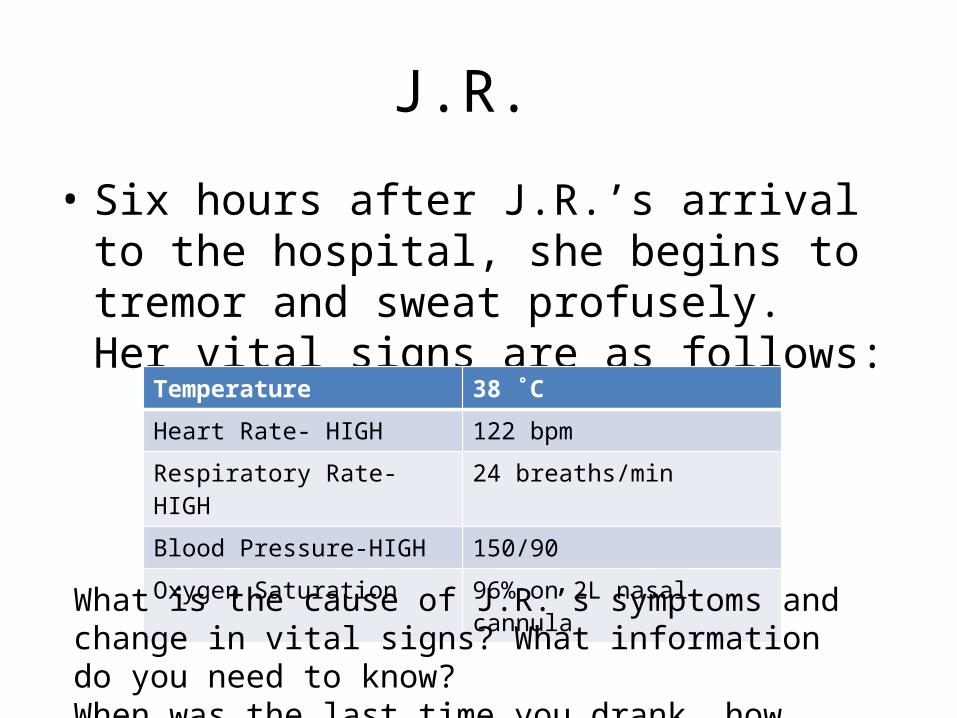
• Six hours after J.R.’s arrival to the hospital, she begins to tremor and sweat profusely. Her vital signs are as follows:
Temperature 38 ˚C
Heart Rate- HIGH 122 bpm
Respiratory Rate- HIGH 24 breaths/min
Blood Pressure-HIGH 150/90
Oxygen Saturation 96% on 2L nasal cannula
What is the cause of J.R.’s symptoms and change in vital signs? What information do you need to know?When was the last time you drank, how much
J.R.
• J.R. informs the nurse that her last alcoholic beverage was 2 hours before she went to the hospital. She is diagnosed with delerium tremens and is started on Ativan and a banana bag.
What is the purpose of these interventions?Ativan- to calm her downBanana bag- has vitamins, minerals, folic acid to replenish electrolytes
J.R.
• J.R. eventually recovers from her DT’s and discharged to an outpatient alcohol rehabilitation program. She does well for a few months but presents to the ED again with complaints of abdominal pain.
J.R.
• J.R. arrives to the ED with complaints of 10/10 knife-like epigastric pain which is relieved when she puts her knees to her chest. She also reports nausea and vomiting. Her assessment is positive for Chvostek sign.
What are you thinking of now? What labs or tests might be ordered? Pancreatitis pain- puts knees to her chestHypocalcemia- Chovstek sign
J.R.
• J.R.’s vital signs are as followed:
Temperature 38.5˚ C
Heart Rate HIGH 116 bpm
Respiratory Rate 24 breaths/minute
Blood Pressure LOW 92/60 mmHg
Oxygen Saturation 92% on RA
J.R.
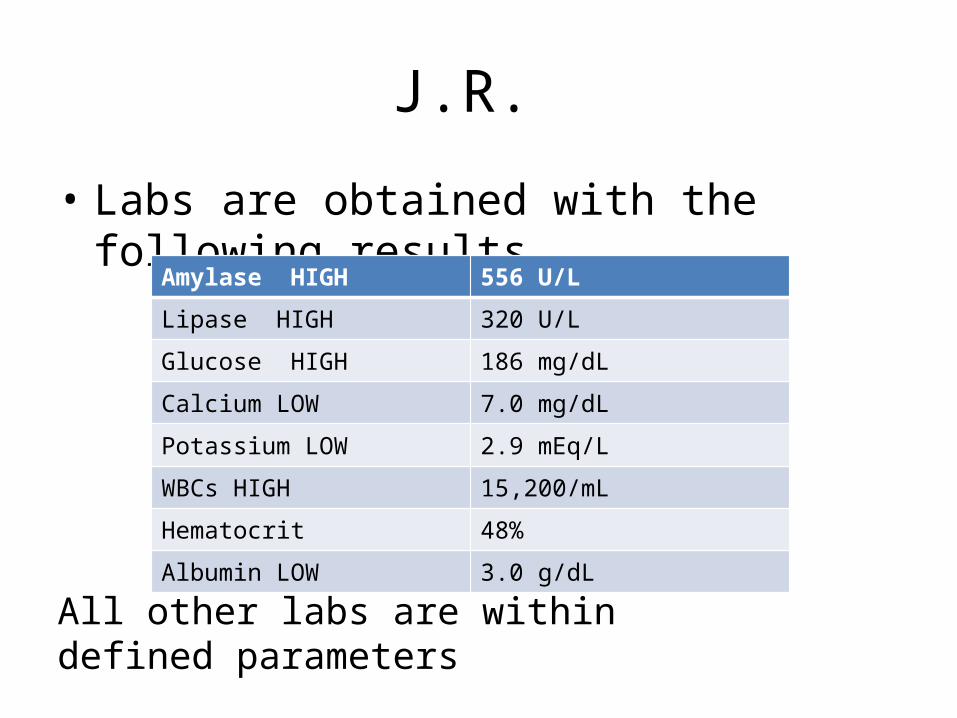
• Labs are obtained with the following resultsAmylase HIGH 556 U/L
Lipase HIGH 320 U/L
Glucose HIGH 186 mg/dL
Calcium LOW 7.0 mg/dL
Potassium LOW 2.9 mEq/L
WBCs HIGH 15,200/mL
Hematocrit 48%
Albumin LOW 3.0 g/dL
All other labs are within defined parameters

J.R.
• J.R. is diagnosed with acute pancreatitis. What interventions are required at this time?
J.R.
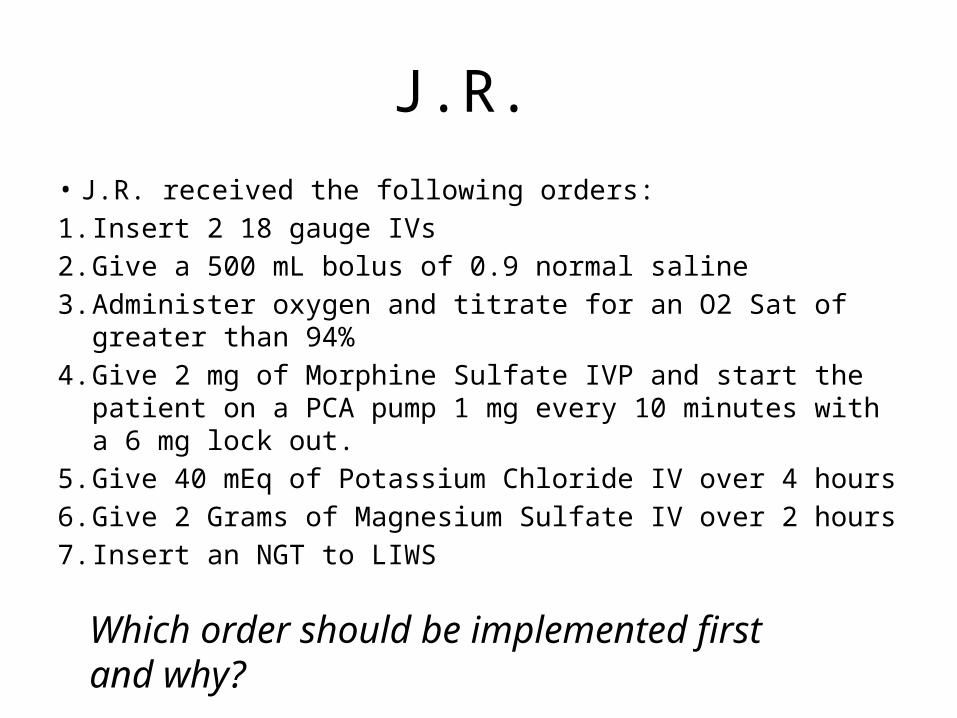
• J.R. received the following orders:1. Insert 2 18 gauge IVs2. Give a 500 mL bolus of 0.9 normal saline3. Administer oxygen and titrate for an O2 Sat of greater than
94%4. Give 2 mg of Morphine Sulfate IVP and start the patient on
a PCA pump 1 mg every 10 minutes with a 6 mg lock out.5. Give 40 mEq of Potassium Chloride IV over 4 hours6. Give 2 Grams of Magnesium Sulfate IV over 2 hours7. Insert an NGT to LIWS
Which order should be implemented first and why?
J.R.
• J.R.’s oxygen saturation increases to 96% with 2L nasal cannula, her blood pressure increases to 110/70 mmHg and her heart rate decreases to 100 bpm after the fluid bolus. Her morning accucheck reveals a blood glucose of 205 mg/dL. Why is this occurring? What needs to be done?
• b/c she’s not producing insulin—you need to give her insulin
J.R.
• J.R. is given 2 Units of Regular insulin and her blood sugar decreases to 170 mg/dL.

J.R.
• J.R. ultimately recovers from her pancreatitis and is discharged home.
• Because of the pancreatic damage related to her episode of pancreatitis, J.R. now requires insulin therapy
J.R.
• J.R returns to the emergency department 3 weeks later with complaints of dizziness, increased thirst and increased urination. She has a fruity acetone odor noted on her breath.
• She also mentions that she has lost 5 pounds in the past few days.
• What do you think is happening to J.R.?• Has DKA b/c not taking her insulin

J.R.
• J.R.’s vital signs are as follows
Temperature 36.5˚ C
Heart Rate 120 bpm
Respiratory Rate 26 breaths/minute
Blood Pressure 88/62 mmHg
Oxygen Saturation 97% on RA
J.R.’s weight is 125 lbs.

J.R.
• J.R.’s labs reveal the following:Glucose 402 mg/dL
Sodium 148 mEq/L
Potassium 4.6 mEq/L
pH 7.26
PaCO2 28 mmHg
PaO2 95 mmHg
HCO3 16 mEq/L
Urine Ketones Positive
What is the significance of these labs?Pt is partially compensated metabolic acidosis d/t DKAGlucose High
J.R.
• J.R. is admitted to the ICU with the following orders: – 0.9 Normal Saline 500 mL bolus over 30 minutes
followed by an infusion of 125 mL/hr– Regular insulin IV bolus of 0.1 Units/kg x1 followed by
an IV infusion of 0.1 Units/kg/hr• Give IV insulin b/c faster and have better control
– Accuchecks every hour– Electrolyte panel every 2 hours– 2,000 calorie ADA diet
Which order would you implement first?
J.R.
• Two 18 gauge IV’s are inserted and the 0.9 NS saline bolus is administered followed by the maintenance IV fluids
• Calculate the dose for the insulin bolus and the IV infusion rate
J.R.
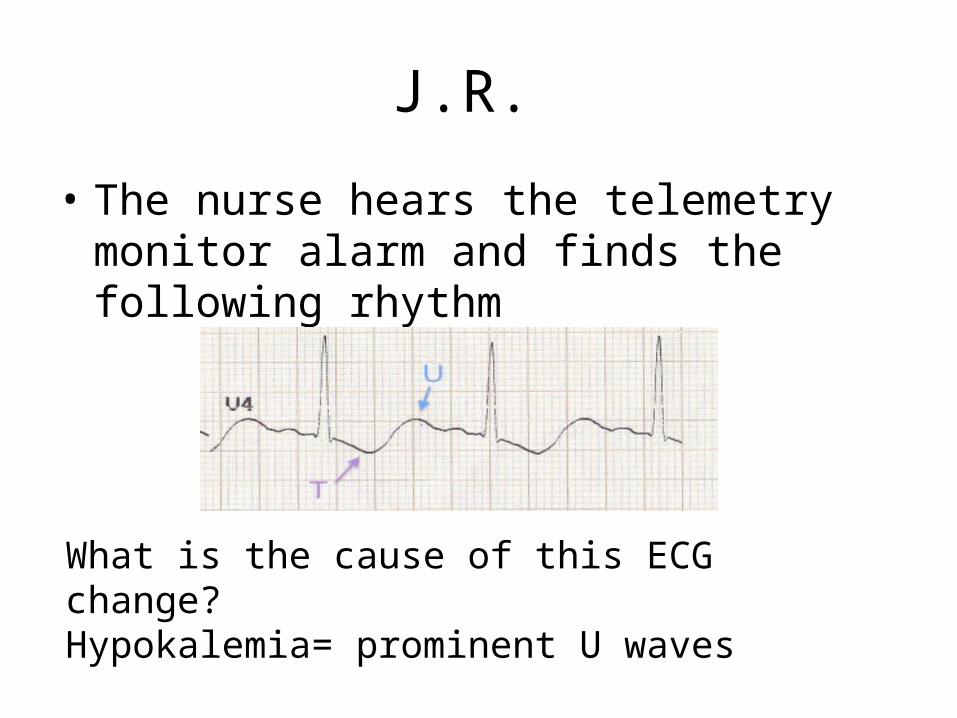
• The nurse hears the telemetry monitor alarm and finds the following rhythm
What is the cause of this ECG change?Hypokalemia= prominent U waves

J.R.
• J.R.’s blood glucose levels are trending downwards. Electrolyte panel demonstrates the following results:
Glucose 199 mg/dL
Potassium 2.9 mEq/L
What orders do you anticipate? Why is the potassium low? Low b/c K is being pushed back into cells. Need K-rider.
J.R.
• The nurse notifies the physician and receives the following orders:– Administer 40 mEq/L of Potassium Chloride IV
over 4 hours• K burns, give slowly• Piggyback to other fluid bag or have lidocaine in fluids
– Change IV fluid to D5.45 NS at 125 mL/hr• Why change to D5.45? b/c getting IV insulin- need
glucose. Don’t want to let blood sugar fall too fast.
J.R.
• J.R. puts on the call light stating that she feels “light-headed and sweaty.”
What should you do now?Check glucose
J.R.
• Accucheck reveals a glucose of 55 mg/dL• What should you do now?– Stop insulin and give juice, carbs
J.R.
• J.R. eventually recovers and is started on maintenance insulin therapy with the long acting insulin glargine and the rapid acting insulin aspart for bolus.
What is the purpose of this insulin combination?Long acting throughout the day, rapid acting before meals
J.R.
• J.R. continues to drink and has not taken steps to control her diabetes.
• J.R. arrives to the hospital two years later with nausea, vomiting, fatigue and jaundice.
• She is diagnosed with alcoholic hepatitis and is advised to stop drinking
J.R.
• J.R. returns again a year after her hepatitis episode with difficulty breathing, a distended abdomen, jaundice, petechiae, and she is vomiting bright red blood.
What is happening to J.R.? Has cirrhosis
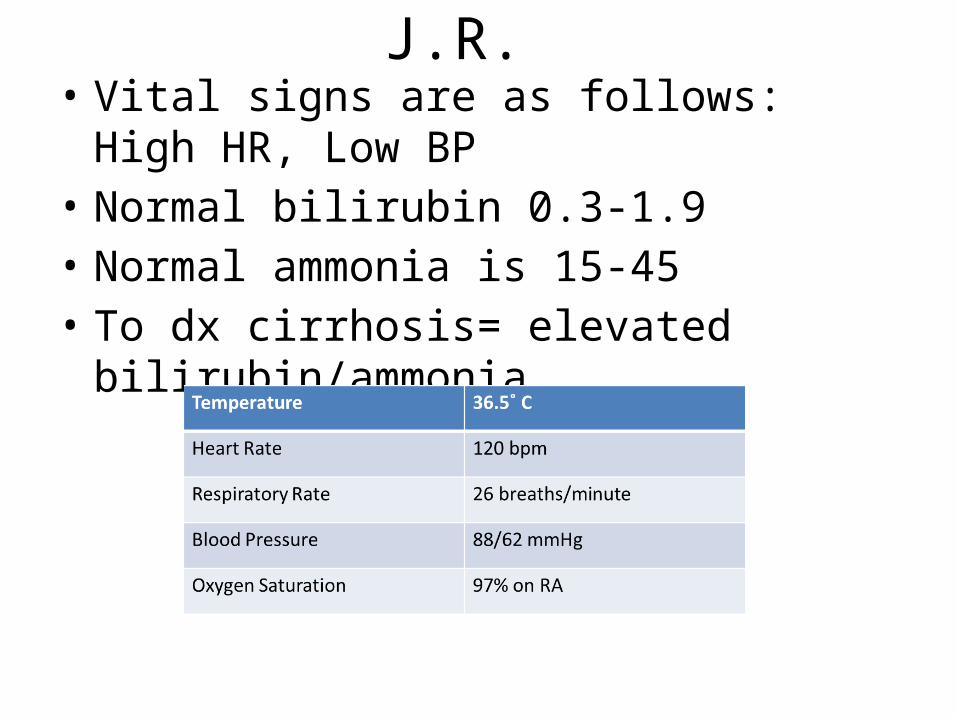
J.R. • Vital signs are as follows: High HR, Low BP• Normal bilirubin 0.3-1.9• Normal ammonia is 15-45• To dx cirrhosis= elevated bilirubin/ammonia
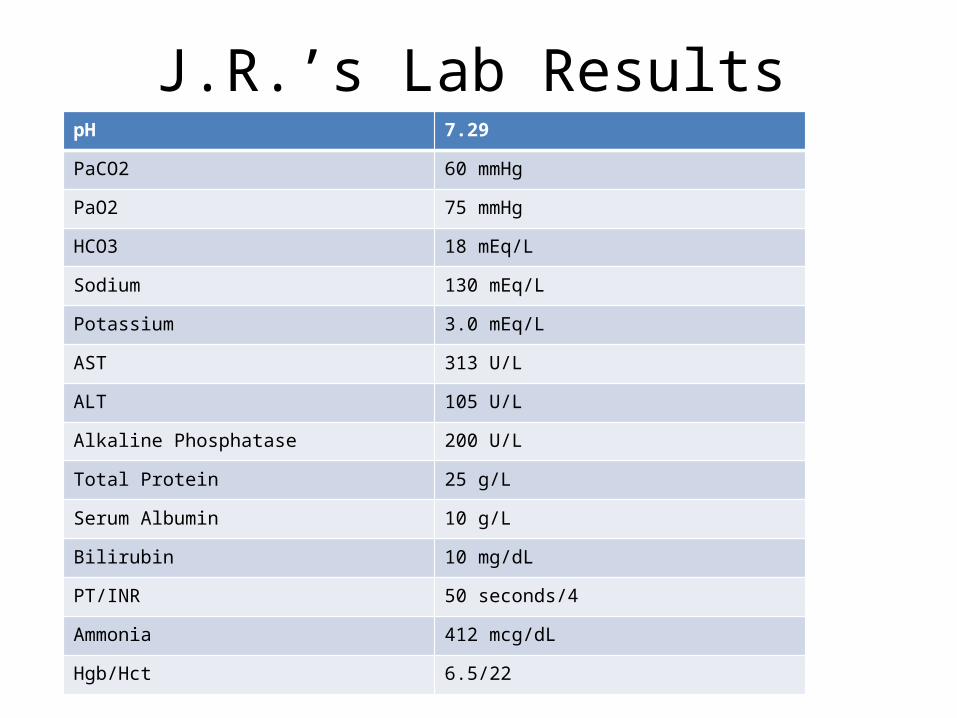
J.R.’s Lab ResultspH 7.29
PaCO2 60 mmHg
PaO2 75 mmHg
HCO3 18 mEq/L
Sodium 130 mEq/L
Potassium 3.0 mEq/L
AST 313 U/L
ALT 105 U/L
Alkaline Phosphatase 200 U/L
Total Protein 25 g/L
Serum Albumin 10 g/L
Bilirubin 10 mg/dL
PT/INR 50 seconds/4
Ammonia 412 mcg/dL
Hgb/Hct 6.5/22
J.R.
• Physical assessment reveals a grossly distended abdomen protubent umbilicus, dull percussion sounds throughout, jaundice, asterixis, clotted blood around the lips. Her respirations are shallow, she has thin arms and her legs have +2 pitting edema. Her weight is 160 lbs and her previous weight one year ago was 125 lbs.
J.R.
• She is intubated and placed on a mechanical ventilator
• Why was this intervention performed?– To help breathing w/ ascites
J.R.
• In addition she is typed and cross-matched and started on 2 units of FFP (Fresh frozen plasma) and given one unit of PRBC’s and 10mg of Vitamin K
• Why are these interventions performed? – FFP= b/c Hgb is low 6.5– PRBCS= given to thicken blood b/c INR is 4 (the higher
the #, the thinner the blood)– Vitamin K= for clotting factors

J.R.
• The GI lab arrives at the bedside to perform an endoscopy which reveals bleeding esophageal varices
• They are banded in hopes to stop the bleeding• Afterward the GI doctor places a nasogastric
tube to decompress the abdomen • A Foley was inserted as well
J.R.
• A paracentesis is performed on J.R. and 4L of fluid is removed. She is given 50g of albumin.
• She is also started on lactulose
J.R.
• Despite all of these interventions, J.R.’s condition becomes worse
• She is not a candidate for a liver transplant due to her recent ingestion of alcohol and unstable condition
• The family is contacted and they decide to withdraw support.





























