Embed Size (px)
DESCRIPTION
overview (N)OAC and comparison
Citation preview

Orale antistollingVergelijking oud versus nieuw

Geschiedenis AF en OAC
• 1978 Framingham relatie AF en stroke• 1980 Beschermend effect VKA op emboli bij
valvulair AF (mitraalstenose)• 1991 Beschermend effect VKA bij Non
Valvulair AF• 1999 VKA significant beter dan
Acetylsalicylzuur

CHADS2 is the most recognized risk stratification scheme
• 1 or 2 points are assigned as shown for each of the risk factors below• Stroke risk is determined by the cumulative score
Gage et al, JAMA 2001*Per 100 patient-years without antithrombotic therapy*Per 100 patient-years without antithrombotic therapy
Item Points
Congestive heart failure 1
Hypertension 1
Age ≥75 years 1
Diabetes mellitus 1
Stroke/TIA 2
CHADS2
6
5
4
3
2
1
0
Add points together
Stroke rate (95% CI)*
18.2 (10.5–27.4)
12.5 (8.2–17.5)
8.5 (6.3–11.1)
5.9 (4.6–7.3)
4.0 (3.1–5.1)
2.8 (2.0–3.8)
1.9 (1.2–3.0)

ESC 2010 guidelines: based on CHADS2 and CHA2DS2-VASc
• CHF/LV dysfunction +1• Hypertension +1• Age ≥75 years +2• Diabetes mellitus +1• Prior Stroke/TIA/TE +2• Vascular disease +1• Age 65–74 years +1• Sex category (female) +1
• Initial evaluation: CHADS2
• If CHADS2 ≥2 oral anticoagulation
• If CHADS2 <2 CHA2DS2-VASc
• Sex only in conjunction with other risk factor
Camm et al, Eur Heart J 2010
Risk category CHA2DS2-VASc score Antithrombotic therapy
No risk factors 0ASA 75–325 mg/day or nothing
(preferably nothing)
One ‘clinically relevantnon-major’ risk factor
1Oral anticoagulation (INR 2–3)
or ASA 75–325 mg/day(preferably oral anticoagulant)
One ‘major’ risk factor or ≥2 ‘clinically relevant non-major’risk factors
≥2 Oral anticoagulation (INR 2–3)

ESC richtlijn 2012 AF

Wat is op de markt
• Acetylsalicylzuur– Thrombocyten aggregatie remmer
• Vitamine K antagonist– Acenocoumarol– Warfarine (niet in Nederland)– Fenprocoumaron
• NOAC’s (Nieuwe Orale Anti-Coagulantia)

Acetylsalicylzuur
• Geen echte “bloedverdunner”• Volstaat niet als alternatief op het
indicatiegebied van VKA• “Bijwerking” als therapeutisch doel

Vitamine K antagonisten
• Acenocoumarol= Sintrom(Mitis) T1/2: ±11 uur• Warfarine = Coumadin T1/2: ±40 uur (niet
verkrijgbaar in NL wel alle trials )• Fenprocoumaron = Marcoumar T1/2 : ±140
uur

VKA geschiedenis
• 1948 geintroduceerd als gif tegen ratten en muizen, en wordt als zodanig nog steeds gebruikt
• In het begin van de 50-er jaren bleek warfarine effectief in het voorkomen van thrombose en embolieen
• 1954 geregistreerd als medicatie

VKA

VKA antagonisten
• Zeer hoge variabiliteit in effect zowel Inter-als Intra humaan
• Hierdoor regelmatig controle noodzakelijk• Variabele dosering per dag• Interactie niet alleen met medicatie maar ook
met voedingsmiddelen• Effect onvoldoende bescherming of verhoogd
bloedingsrisico• TTR Thrombosedienst NL ca 65.5%

Fuster V et al. Circulation 2006;114:e257–e354Connolly SJ, et al. N Engl J Med 2009;361:1139-1151Baker WL, Cios DA, Sander SD, Coleman CI. J Manag Care Pharm 2009;15:244–252.
1International Normalized Ratio (INR)
Odd
s ra
tio
2
15
8
10
5
01
3 4 5 6 7
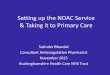
CVA
Intracraniële bloedingen
20
Smalle Therapeutische bandbreedte VKA’s
Tijd binnen Therapeutische Range: Thrombosedienst ca 64% (jrvsl Thdienst 2009)
19
TTR:

Ned thrombosedienst Jaarverslag 2011
• Intra craniele bloedingen – 2011: 757 (334†: 44%)
• Ernstige bloedingen :– 2011: 4101 (561 †: 14%) Totaal aantal mensen enigerlei tijd op VKA 2011: 404186
(± 322200 PY) (overleden mede als gevolg bloeding 0.22 % =1 : 454) CVA’s onder VKA gebruik 714 (88 †:12%) Waarschijnlijk onderschatting door gebrekkige registratie

HAS-BLEDH = Hypertensie (systolische bloeddruk > 160 mmHg) 1 punt*, **A = Abnormale nierfunctie 1 punt
Abnormale leverfunctie 1 puntS = Stroke, CVA in voorgeschiedenis 1 punt*,***B = Bloeding in de voorgeschiedenis 1 puntL = Labiele INR 1 punt****E = leeftijd > 65 jaar 1 punt*,*****D = Drugs, medicatie die het bloedingsrisico verhoogt (o.a.NSAID) 1 punt
Alcoholmisbruik 1 punt
A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010 Nov;138(5):1093-100
Verhoogde valneiging is geen risicofactor (Man-Son-Hing M, et al. Choosing antitrombotic therapy for elderly patients with atrial fibrillation who are at risk for falls. ArchIntern Med 1999;159:677-685.)
Inschatting bloedingsrisico
•*Komt inCHADS score voor•** Andere definitie CHADS•*** Telt dubbel in CHADS•**** Weet je pas na start•***** >75 in CHADS dubbel

HASBLED vs CHADS2
24

Er is dus behoefte aan orale anticoagulantia die even effectief zijn, maar veiliger en gemakkelijker in het
gebruik
bescherming
schade

NOAC’s
• Competitieve IIa remmer– Dabigratan = Pradaxa (Boehringer Ingelheim)
75,110,150 mg
• Direkte Xa remmer– Rivaroxaban = Xarelto (Bayer) 2.5,5,10,15,20 mg– Apixaban = Eliquis (Pfizer/BMS) 2.5,5,10 mg

Dabigratan
RivaroxabanApixaban

1DD
2DD
2DD

Eliq
uis®
-con
cent
ratie
(n
g/m
l)
Eliquis® 2,5 mg 2dd
150
100
50
0
Eliquis® 5 mg 1dd
168 180 192
Tijd na eerste dosis (u)
2dd 1dd
0
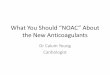
2DD lage dosering
1DD hoge dosering
Conc
entr
atie
in µ
g/m
l
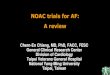
Verschil in 1 dd hoge dosering vs 2dd lage dosering bij zelfde ½ waarde tijd
Hoger bloedingsrisico
Lagere bescherming

Vergelijking NOAC studies Prim uitkomst.(non inferiority)
Middel doses Studie N Man%
CHADS2 FU-Y TTR %
Apixaban 2dd 5 Aristotle 9120/9081 65 2.1±1.1 (1->3) 1.8 62
Dabigratan 2dd110 Rely 6015/6022 64.3 2.1 ±1.1 (0-6) 2.0 64
Dabigratan 2dd 150 Rely 6076/6022 63.2 2.2±1.2 (0-6) 2.0 64
Rivaroxaban 1dd 20 Rocket AF 7081/7090 60 3.48±0.9 4(1-6) 1.94 55
Middel Stroke/embolie
%/y
Stroke %/y Embolie%/Y
MI%/y All cause%/y
Apixaban 1.27vs1.60 1.19vs1.51 0.09vs0.10 0.53vs0.61 4.85vs5.49
Dabigratan110 1.53vs1.69 1.44vs1.57 0.12vs0.09 0.72vs0.53 3.75vs4.13
Dabigratan150 1.11vs1.69 1.01vs1.57 0.15vs0.09 0.74vs0.53 3.64vs4.13
Rivaroxaban 1.7 vs 2.2 1.34vs1.42 0.04vs0.19 0.91vs1.12 1.9vs2.2

Vergelijking NOAC’s studies negatieve aspecten
Middel Major bleeding %/y
Intra cranial bleeding
%/y
GI bleeding%/y
Discontinuance rate %
Apixaban 2.13 vs 3.09 0.33 vs 0.8 0.76vs0.86 25.3vs27.5
Dabigratan 110 2.71 vs 3.36 0.23 vs 0.74 1.12vs1.02 20.7vs16.6
Dabigratan 150 3.11 vs 3.36 0.30 vs 0.74 1.51vs1.02 23.9vs16.6
Rivaroxaban 3.6vs3.4 0.5 vs 0.7 1.6vs1.1 23.9vs22.4
Middel Netto clinical outcome benefit
Apixaban 0.85(0.78-0.92)
Dabigratan 110 0.92(0.84-1.02)
Dabigratan 150 0.91(0.82-1.00)
Rivaroxaban 0.88(0.75-1.03)

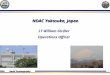
Stroke or systemic embolism (A) and ischemic stroke (B) during oral anticoagulant treatment.
Dentali F et al. Circulation 2012;126:2381-2391
Copyright © American Heart Association

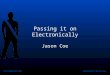
Major (A) and intracranial (B) bleeding during oral anticoagulant treatment.
Dentali F et al. Circulation 2012;126:2381-2391
Copyright © American Heart Association

Hartinfarcten tijdens gebruik NOAC’s.
Dentali F et al. Circulation 2012;126:2381-2391
Copyright © American Heart Association

Total (A) and cardiovascular (B) mortality during oral anticoagulant treatment.
Dentali F et al. Circulation 2012;126:2381-2391
Copyright © American Heart Association

Efficacy and Safety of the Novel Oral Anticoagulants in Atrial Fibrillation: A Systematic Review and Meta-Analysis of the Literature.
Circulation :published ahead of print online Okt 15 2012 DOI 10.1161
• total of 54875 patients. • NOACs significantly reduced in comparison with warfarin:
-total mortality (5.61% vs 6.02%; RR 0.89; 95%CI, 0.83-0.96), -cardiovascular mortality (3.45% vs 3.65%; RR 0.89; 95%CI, 0.82-0.98)-stroke/SE (2.40% vs 3.13%; RR 0.77; 95%CI, 0.70-0.86).
• There was a trend towards:- reduced major bleeding (RR 0.86; 95%CI, 0.72-1.02), - with a significant reduction of intracranial hemorrhage (RR 0.46; 95%CI, 0.39-0.56).
• No difference in myocardial infarction was observed.– FDA revised data RELY :not a higher risk (with and without previous
MI)

Real world
• Post marketing surveillance EMEA/FDA > 100.000 gebruikers even effectief, veiliger– Presentatie AHA nov 2012
• Post marketing surveillance verzekerings database V.S. > 12.000 gebruikers.– NEJM 2013 mar 13DOI: 10.1056/NEJMp1302834
• Post marketing surveillance Denemarken Nationaal patienten register >5000 gebruikers
– Efficacy and safety of dabigatran etexilate and warfarin in ‘real world’ patients with atrial fibrillation: A prospective nationwide cohort study.Larsen TB, Rasmussen LH, Skjoth F et al.,J Am Coll Cardiol. 2013

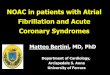
Post Marketing surveillance verzekerings database VS
NEJM 2013 mar 13DOI: 10.1056/NEJMp1302834

Efficacy and safety of dabigatran etexilate and warfarin in ‘real world’ patients with atrial fibrillation: A prospective nationwide cohort study.Larsen TB, Rasmussen LH, Skjoth F et al.,J Am Coll Cardiol. 2013

Conclusies(gelden alleen voor geregistreerde indicaties)
• NOAC’s zijn minstens even effectief als VKA • NOAC’s zijn veiliger dan VKA• NOAC’s bieden meer gebruikersgemak• NOAC’s zijn niet duurder dan VKA • NOAC’s volledig vergoed via basisverzekering

Indicaties

Vergelijking dosering NOAC’s indicatie AF
Middel Interval dosering GFR 50-30 GFR 29-15 GFR<15
Apixaban 2 dd 5 mg 5mg 2.5mg 0
Dabigratan 2 dd 150 mg 110mg 0 0
Rivaroxaban 1 dd 20 mg 15 mg 15 mg 0
Middel <60 kg >80 jaar Kreat > 133 µmol/l *
Vergoeding
Apixaban 2.5 mg** 2.5 mg** 2.5 mg** Ja
Dabigratan 150 mg 110 mg GFR Ja
Rivaroxaban 20 mg 20 mg GFR Ja
** indien 2 van de 3 , dus de enkele factor niet voldoende voor aanpassing


Cardioversie
• Hoe sneller een cardioversie wordt ondernomen hoe groter de kans op succes
• Bij boezemfibrilleren langer dan 48 uur bestaand, dient de patient minimaal 3 weken adequaat te zijn ontstold.– VKA 3 weken achtereen INR > 2.0
• In praktijk ECV pas na 4-6 weken.
– NOAC na 3weken: ECV

Geen antidotum
• VKA heeft:– Vit K: werkzaam pas na 5-10 uur : niet effectief bij
acute bloeding– Vier factoren concentraat (II, VII, IX, X)– Rebound effect
• Handelingen bij bloeding onder VKA of NOAC gebruik vrijwel exact hetzelfde
• NOAC veiliger dus minder vaak nodig

Wat doe je ? VKA
• Lokale haemostase maatregelen
• Mechanische compressie• Stop VKA TNO• Heroverweeg co
medicatie (aggregratieremmers)
NOAC
• Lokale haemostase maatregelen
• Mechanische compressie• Stop NOAC TNO• Heroverweeg co
medicatie (aggregratieremmers)

bloeding bij NOAC gebruikBepaal LAB:
APTT en/of dTT bij dabigratanpT en/of directe Xa test bij rivaroxaban/apixaban
HB, Thr, Nierfu (kruisbloed)
Milde bloeding
Matig ernstige bloeding
Levensbedreigende bloeding
•Lokale haemostase maatregelen
•Mechanische compressie•Stop NOAC TNO•Heroverweeg co
medicatie (aggregratieremmers)
•Chirurgische haemostase•Haemodynamische
ondersteuning•Adequate diurese
•Erythrocyten transfusie•Thrombocyten transfusie
(thrombopenie of aggregratieremmers)
•4 factoren concentraat 25-50 IE/kg
•Actieve kool <3 uur na inname
•4 F concentraat 50 IE/Kg•rFVII a 90µg/kg
•FEIBA 50-100 IE/kg•Hemodialyse bij
nierfalen en dabigratan+ +





Vraag?
• Zouden Vit K antagonisten , indien nu op de markt gebracht tegen de NOAC’s , wel geregistreerd worden?


ZGT- beleid
• Nieuwe patienten: Keuze OAC met patient bespreken(90% kiest NOAC)
• Geen actief omzettingsbeleid• Bij aanbieden zelfcontrole of controle aan huis
door thrombose dienst: Keuze• Op verzoek patient• Bij bijwerkingen of moeilijk instelbaar VKA

Literatuur
• Leidraad begeleide introductie NOACS• Alle 1B teksten• Originele Publicaties: Rely, Rely-able, Rocket-AF, Aristotle, Averroes (Incl
supplementen en vele sub analyses)• Farmacotherapeutisch kompas• ESC richtlijnen AF 2010 en update 2012 (onderschreven door NVVC)• Jaarverslag Thrombosedienst Nederland 2011• Diverse andere publicaties (op verzoek verkrijgbaar)
Europace 2013;15:625-651
http://www.escardio.org/communities/EHRA/publications/novel-oral-anticoagulants-for-atrial-fibrillation/Pages/welcome.aspx

Hoe voor te schrijven
• Alleen door specialisten (vooralsnog)• FAX: met verwijzing indicatie AF: hierin
nierfunctie (<2 maanden), en apotheek : wij faxen machtiging en recept naar apotheek
• Echter HA kan voorlopige machtiging afgeven– Indicatie AF– GFR bekend, niet ouder dan 2 maanden– Verwijzing naar specialist– Patient heeft het middel eerder gebruikt?


Omzetten VKA naar NOAC
• Acenocoumarol Stop; 3 dagen daarna start NOAC
• Fenprocoumaron Stop; 7 dagen daarna start NOAC
• Gebruik plaatjes aggregratie remmers, indien na PCI < 1 jaar geleden: niet doen
• Anders stop plaatjes aggregratie remmers en start direkt NOAC (cave NSAID gebruik)

controles
• Eigen verantwoordelijkheid patient– Gesprek en uitleg patient risico’s– Controle apotheek?
• Ideaal middel voor baxter (vaste dosering)• Jaarlijks nierfunctie• Aanpassing op basis leeftijd• Thrombosedienst poogt zichzelf hierin een
plaats te geven???? (thuismeetweken)

Disclosure
• Sub investigator RElY• Adviesraad Boehringer-Ingelheim 2012