Embed Size (px)
Citation preview

NOAC trials for AF:
A review
Chern-En Chiang, MD, PhD, FACC, FESCGeneral Clinical Research Center
Division of CardiologyTaipei Veterans General Hospital
National Yang-Ming UniversityTaipei, Taiwan

Presenter Disclosures
• Research Grant: nothing to disclose
• Honorarium: has spoken at symposia
sponsored by and served on scientific advisory
boards for Astrazeneca, Bayer, Boehringer
Ingelheim, Chugai, Daiichi-Sankyo, GSK, MSD,
Novartis, Pfizer, Roche, Sanofi-aventis, Servier,
Tanabe, Takeda, TTY
• Stockholding: None

• Role of aspirin in Asians
• Role of warfarin in Asians
• Role of NOACs in Asians
• Reversal agents
• Asian algorithm
Outlines

1. ASA is not effective in cohort
studies in Asia

Aspirin and warfarin in Chinese
Siu et al. Heart Rhythm. 2014 Aug;11(8):1401.
• 9,727 AF patients in HK, mean age 77 y, FU 3.2 years
CHADS2
CHA2DS2-VASc
Aspirin
-18.7%
-18.7%
Warfarin
-52.7%
--52.7%

2. ASA is not effective in RCT in Asia

Stroke 2006;37;447-451
JAST

Stroke 2006;37;447-451

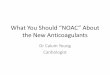
3. ASA is worse than NOACs

AVERROES Trial
ASA(81-324 mg daily; up to 36 mo/end of study)
Apixaban(5 mg twice daily; 2.5 mg in selected patientsa; up to 36 mo/end of study)
E
Unsuitable for warfarin therapy
N= 5600Double-blindR
Connolly S, N Engl J Med 2011;364:806

Cu
mu
lative
Ris
k
0.0
0.0
10.0
30.0
5
0 3 6 9 12 18 21
ASA
Apixaban*
No. at RiskASA
Apix
2791 2720 2541 2124 1541 626 329
2809 2761 2567 2127 1523 617 353
Months
RR=0.4595% CI, 0.32-0.62
P<.001
AVERROES: Stroke or Systemic Embolic Event
Connolly S, N Engl J Med 2011;364:806
*Apixaban is not FDA approved.
-55%

Fewer hemorrhagic stroke and ICH in Apixaban group
0.670.851 1
0
1
2
Hemorrhagic stroke ICH
Apixaban
HR
Connolly S, N Engl J Med 2011;364:806

Chi-Wai HO, …Chung-Wah Siu, Stroke, 2015 Jan;46(1):23-30
Annual incidence of ICH
Real Life data from Hong Kong
110 mg

• Role of aspirin in Asians
• Role of warfarin in Asians
• Role of NOACs in Asians
• Reversal agents
• Asian algorithm
Outlines

1. It is very difficult for Asians to
maintain optimal INR (2.0-3.0)

RE-LY AF registry

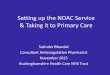
2. A lower INR, which is common in
Asia, could not protect your patients
from Stroke!

17.6
11.9
8.36
4.4 3.3 2.5 2 1.5 1.2 10
10
20
1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9
INRHylek EM, et al. N Engl J Med 1996;335:540
2.0
Low INR is not protective from strokeA
dju
ste
d O
dd
s r
ati
o
********
*
** P<0.05

3. In Asians, even a lower INR could
not protect you from bleeding!

35.419.8
37.1 29.1 28.6 18 28.4 22.2
54.566.2
50.3 55.2 6067
63.6 65
10.1 14 12.6 15.7 11.4 15 8 12.8
0%
50%
100%
INR>3.0
RE-LY ROCKET ARISTOTLE ENGAGE
Lip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

3.53 3.43
3.3
3.82
5.14
3.84
4.8
0
3
6
RE-LY ROCKET ARISTOTLE ENGAGE
Non-…Asians
%
Major bleeding (Warfarin)More bleeding occurs even at lower INR range
Lip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

0.71 0.63 0.67 0.74
1.1
2.46
1.88 1.92
0
1.5
3
RE-LY ROCKET ARISTOTLE ENGAGE
Non-…Asians
%
Intra-cranial hemorrhage (Warfarin)More bleeding occurs even at lower INR range
Lip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

4. In Asians, even a high TTR could
not protect you from hemorrhagic
stroke!

Time in Therapeutic Range for
Warfarin-treated Patients
INR 1.6─2.6 ≥70 years
% T
ime in t
hera
peutic r
ange (
media
n)
Yukihiro Koretsune, JCS2014

Hemorrhagic stroke
2.61
0.840.70.42
0.72
0.21
0
1
2
3
China Japan
Warfarin
Edoxaban 60
Edoxaban 30
%/y

5. Intra-cranial hemorrhage (ICH) is
more catastrophic in Asians!

Warfarin associated intracerebral
hemorrhage in Hong Kong Chinese
• The mean INR on presentation was 2.9 ± 1.0
• The mortality rate at 3-6 months for WICH
was 62.0%
Neurol Res. 2014 Feb;36(2):143

• Role of aspirin in Asians
• Role of warfarin in Asians
• Role of NOACs in Asians
• Reversal agents
• Asian algorithm
Outlines

(NOACs)Non-vitamin K antagonist Oral Anti-Coagulants
(NOACs)

Lancet. 2014;383:955
• 4 trials
• N= 71,683 patientsGlobal

Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61
• 5 trials– Asians = 8,928 patients
– Non-Asians = 64,033 patients
Asians vsNon-Asians

Standard doses
• Dabigatran 150 mg
• Rivaroxaban 20 mg
• Apixaban 5 mg
• Edoxaban 60 mg
Lancet. 2014;383:955 Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Lancet. 2014;383:955
Stroke and systemic embolism
Global
-19%
P<0.0001

Stroke and systemic embolism
-35%
-15%
Interaction P=0.045
Asian
Non-Asian
Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Lancet. 2014;383:955
All-cause-mortality
Global
-10%
P=0.0003

All-cause mortality
-20%
-9%
Interaction P=0.219
Asian
Non-Asian
Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Lancet. 2014;383:955
Major bleeding
Global
-14%
P=0.06

Major bleeding
-43%
-11%
Interaction P=0.004
Asian
Non-Asian
Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Lancet. 2014;383:955
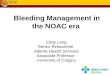
Hemorrhagic stroke
Global
-51%
P<0.0001

Hemorrhagic stroke
-68%
-44%
Interaction P=0.046
Asian
Non-Asian
Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Lancet. 2014;383:955
Gastrointestinal bleeding
Global
+25%
P=0.043

Gastrointestinal bleeding
-21%
+44%
Interaction P=0.041
Asian
Non-Asian
Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Low doses
• Dabigatran 110 mg
• Rivaroxaban 15 mg (J-ROCKET)
• Edoxaban 30 mg
Lancet. 2014;383:955 Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Global
Ruff, Lancet. 2014;383:955
-67%V
-69%V

Ischemic stroke
Global+28%P=0.046
Ruff, Lancet. 2014;383:955

Ischemic stroke
+6%
+29%
Interaction P=0.504
Asian
Non-Asian
Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

Lancet. 2014;383:955
Myocardial infarction
Global
+25%
P=0.019

Myocardial infarction
-8%
+28%
Interaction P=0.352
Asian
Non-Asian
Wang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

NOACs in Asia
• Standard dose
Efficacy:
NOACsWarfarin
Safety:
NOACswarfarin
• Low dose
Efficacy:
NOACsWarfarin
Safety:
NOACswarfarinWang, Lip, Lin, and Chiang, Stroke. 2015 Sep;46(9):2555-61

0.0 0.5 1.0 1.5 2.0
1.14 (0.97-1.61)1.08 (0.73-1.61)
0.88 (0.75-1.05)0.71 (0.46-1.10)
0.81 (0.66-0.99)0.74 (0.50-1.10)
0.89 (0.75-1.05)0.78 (0.44-1.39)
0.93 (0.74-1.17)0.81 (0.54-1.21)
0.72 (0.56-0.92)0.45 (0.28-0.72)
Non-AsianAsian
Edoxaban 30mg o.d.Non-AsianAsian
Edoxaban 60mg o.d.Non-AsianAsian
Apixaban 5mg b.d.Non-AsianAsian
Rivaroxaban 20mg o.d.Non-AsianAsian
Dabigatran 110mg b.d.Non-AsianAsian
Dabigatran 150mg b.d.
Stroke and SEEin Asian vs non-Asian in 4 RCTs
V
Warfarin betterNOACs better
Lip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

0.0 0.5 1.0 1.5 2.0
1.38 (1.15-1.64)1.77 (0.93-3.36)
1.01 (0.83-1.22)0.64 (0.28-1.46)
0.86 (0.68-1.10)1.17 (0.74-1.85)
0.94 (0.75-1.17)0.94
1.17 (0.89-1.53)1.01 (0.63-1.61)
0.82 (0.61-1.10)0.55 (0.32-0.95)
Non-AsianAsian
Edoxaban 30mg o.d.Non-AsianAsian
Edoxaban 60mg o.d.Non-AsianAsian
Apixaban 5mg b.d.Non-AsianAsian
Rivaroxaban 20mg o.d.Non-AsianAsian
Dabigatran 110mg b.d.Non-AsianAsian
Dabigatran 150mg b.d.
Ischemic strokein Asian vs non-Asian in 4 RCTs
V
Warfarin betterNOACs better
Lip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

0.0 0.5 1.0 1.5 2.0
0.32 (0.20-0.51)0.36 (0.15-0.86)
0.57 (0.39-0.84)0.40 (0.18-0.92)
0.62 (0.41-0.96)0.25 (0.10-0.62)
0.59 (0.37-0.93)0.40 (0.13-1.27)
0.37 (0.19-0.72)0.15 (0.03-0.66)
0.28 (0.13-0.58)0.22 (0.06-0.77)
Non-AsianAsian
Edoxaban 30mg o.d.Non-AsianAsian
Edoxaban 60mg o.d.Non-AsianAsian
Apixaban 5mg b.d.Non-AsianAsian
Rivaroxaban 20mg o.d.Non-AsianAsian
Dabigatran 110mg b.d.Non-AsianAsian
Dabigatran 150mg b.d.
Hemorrhagic strokein Asian vs non-Asian in 4 RCTs
V
V
V
V
V
Warfarin betterNOACs better
Lip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

Efficacy and safety endpoints of different NOACs in Asians
Stroke/SSE Ischemic stroke
Hemorrhagic stroke
Myocardial infarction
All-cause death
Major bleeding Intra-cranial hemorrhage
GI bleeding Bleeding of any cause
Dabigatran 150 mg V V V V V V
Dabigatran 110 mg V V V V
RivaroxabanV NR
ApixabanV V V NR V
Edoxaban60 mg V V V V V
Edoxaban 30 mg V V V V
Lip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

Efficacy and safety endpoints of different NOACs in non-Asians
Stroke/SSE Ischemic stroke
Hemorrhagic stroke
Myocardial infarction
All-cause death
Major bleeding Intra-cranial hemorrhage
GI bleeding Bleeding of any cause
Dabigatran 150 mg V V V X
Dabigatran 110 mg V V V V
RivaroxabanV V X
ApixabanV V V V V V
Edoxaban60 mg V V V X V
Edoxaban 30 mg X V V V V V
Chiang, Wang, Lin, Europace. 2015 Oct;17 Suppl 2:ii31-ii39

Real-life data of dabigatran in Asia:
Taiwan experience
• Dabigatran (n=9940) and warfarin (n=9913)
non-valvular atrial fibrillation patients
• 88% taking dabigatran 110 mg
Stroke 2016 Feb;47(2):441

Stroke 2016 Feb;47(2):441
-38%

Stroke 2016 Feb;47(2):441
-56%

Stroke 2016 Feb;47(2):441
-42%
-55%

Low dose dabigatran (110 mg)Major
bleeding ICH
69%
Ischemic
strokeAll-cause
mortality
GlobalRE-LY
9% 20%
Asian meta-analysis
Wang
Hong Kong
Chan
79% 43% 43%
32% 71%
11%
3%
Taiwan NHIRD
Chan56% 38% 55% 42%
NS
NS
NS

• Role of aspirin in Asians
• Role of warfarin in Asians
• Role of NOACs in Asians
• Reversal agents
• Asian algorithm
Outlines

Non-valvular AF
CHA2DS2-VASc score
1 (male)0 (male) or 1 (female)Ie. ‘low risk’
2
No antithrombotic
therapy
NOACsDabigatranApixaban
NOACsDabigatranEdoxabanApixaban
RivaroxabanLip GYH, Wang KL, Chiang CE. Int J Cardiol 2015 Feb 1;180C:246

Summary (I)
• Aspirin has no role in stroke prevention in AF in Asians
• Warfarin should only be spared for those in whom NOAC is contraindicated
• In our meta-analysis, standard-dose NOACs were more effective and safer in Asians than in non-Asians. The increased risk of GI bleeding was not found in Asians.
• Low-dose NOACs performed similarly in efficacy in both populations, but the safety was much better than warfarin in both populations. Increased risk of myocardial infarction was not found in Asians.
• All NOACs are preferable over warfarin
• NOACs is now revolutionizing SPAF in Asians