Embed Size (px)
Citation preview

NOAC in patients with Atrial
Fibrillation and Acute
Coronary Syndromes
Department of Cardiology,
Arcispedale S. Anna
University of Ferrara
Matteo Bertini, MD, PhD

Among ACS patients undergoing PCI, approximately 5% to 21% of patients have concomitant AF.
Despite overlap in the occurence of these syndromes, the pharmacotherapies used to manage AF and ACS differ
Atrial fibrillation and PCI
Rubboli et al., J Interv Cardiol 2009


The management of AF patients who
undergo stent placement for an ACS is
challenging
VKA + antiplatelets
Thrombotic riskHaemorragic risk
-AF-related ischaemic stroke-Bleeding associated with
antithrombotic therapy-Stent thrombosis

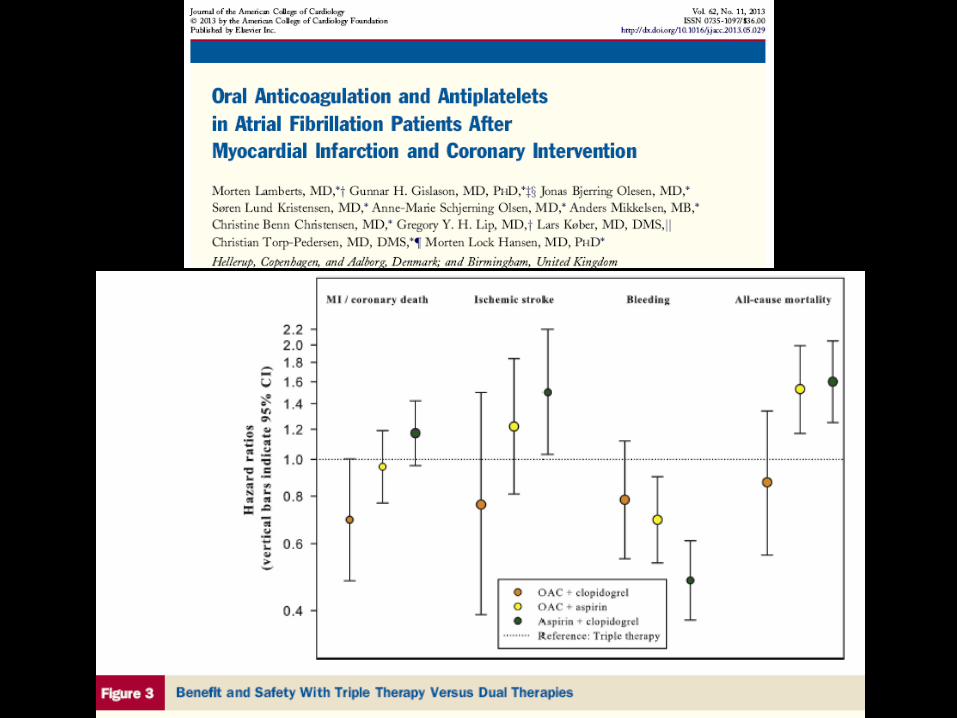
Ischaemic stroke associated with warfarin, aspirin and clopidogrel in patients with AF
Hansen et al. Arch Int Med 2010; 170: 1433-1441
n = 82854
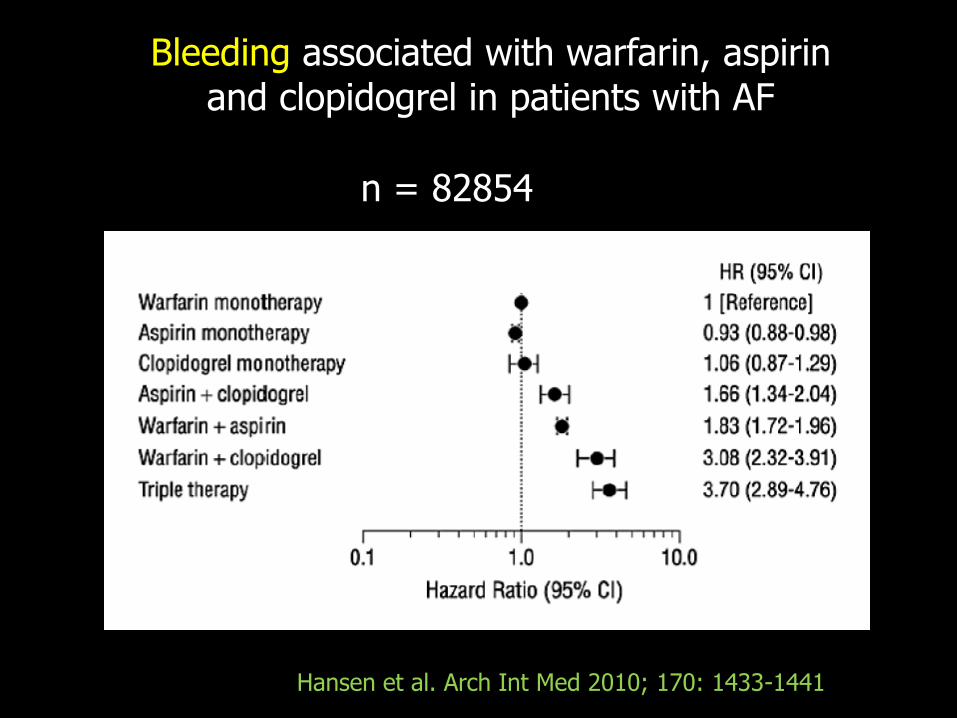
Bleeding associated with warfarin, aspirin and clopidogrel in patients with AF
n = 82854
Hansen et al. Arch Int Med 2010; 170: 1433-1441

TRIPLE THERAPY: clinical evidences
WOEST Trial

Primary outcome: any bleeding episode within 1 year of PCI

ISAR-TRIPLE
• 600 pts
• Indication to VKA+DES (ACS or elective)
• 9-month follow-up
• Composite endpoint : death, MI, stroke, ST, TIMI-bleeding


NOACS in association with DAPT (aspirin+clopidogrel) ?
In all NOACS trials ( RELY, ROCKET-AF, ARISTOTLE, ENGAGE-AF) patients wereexcluded from enrollment if receiving newP2Y12
And conversely, AF patients requiring OAC were systematically excluded from recent ACS trials.
Some data are available in non AF patients

97% patients were taking aspirin81% patients were taking aspirin plus a P2Y12-receptor inhibitor (predominantly clopidogrel)

Primary OutcomeCV Death, MI, Ischemic Stroke
Apixaban 279 (7.5%)
Placebo 293 (7.9%)
HR 0.95; 95% CI 0.80-1.11; p=0.509
APPRAISE-2

TIMI Major BleedingApixaban 48 (1.3%)
Placebo 18 (0.5%)
HR 2.59; 95% CI 1.50–4.46; p=0.001
APPRAISE-2

ATLAS ACS 2 TIMI 51
Rivaroxaban
2.5 mg bid
n=4825
Placebo
n=4821
Rivaroxaban
5 mg bid
n=4827
Event-driven study – 1002 events
Stratum 2: ASA +
thienopyridine (93%)
Rivaroxaban
2.5 mg bid
n=349
Placebo
n=355
Rivaroxaban
5 mg bid
n=349
Physician's decision to add thienopyridine or not
N=15,526*
ASA dose =
75–100 mg/day
Stratum 1: ASA
alone (7%)
Mega et al, 2011

Primary efficacy endpoint (CV death/MI/stroke)Both rivaroxaban doses, both strata
Number at risk
Placebo 5113 4307 3470 2664 1831 1079 421
Rivaroxaban 10,229 8502 6753 5137 3554 2084 831
Months after randomization
HR=0.84
(0.74–0.96)
ARR=1.7%
mITT p=0.008ITT p=0.002
NNT=56
10.7%
8.9%
2-year Kaplan–Meier estimate
Estim
ate
d c
um
ula
tive r
ate
(%
)
Rivaroxaban
Placebo
12
00 16
10
8
6
4
2
201284 24
Mega et al, 2011 ATLAS ACS 2 TIMI 51

Rivaroxaban
2.5 mg bid
(n=5115)
Rivaroxaban
5 mg bid
(n=5110)
Placebo
(n=5125)
Non-CABG TIMI major bleed
K–M estimate at 2 years 1.8% 2.4% 0.6%
p value versus placebo <0.001 <0.001
ICH
K–M estimate at 2 years 0.4% 0.7% 0.2%
p value versus placebo 0.04 0.005
Fatal bleeding
K–M estimate at 2 years 0.1% 0.4% 0.2%
p value versus placebo 0.45 0.20
Fatal ICH
K–M estimate at 2 years 0.1% 0.2% 0.1%
p value versus placebo – –
Mega et al, 2011ATLAS ACS 2 TIMI 51
Safety endpoint


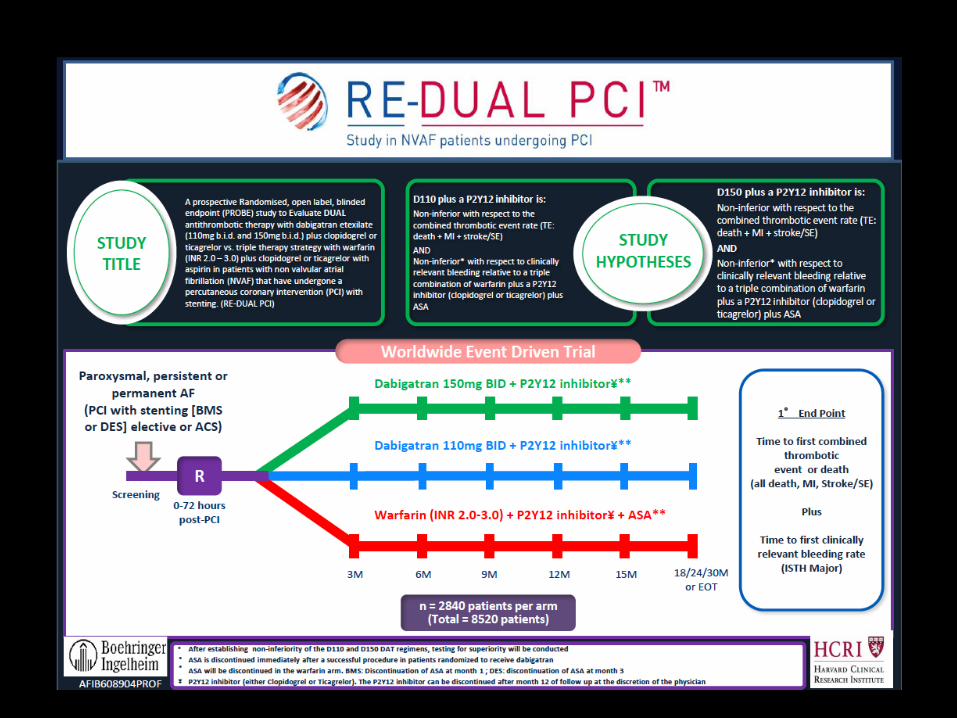
AF + NOAC + DAPT
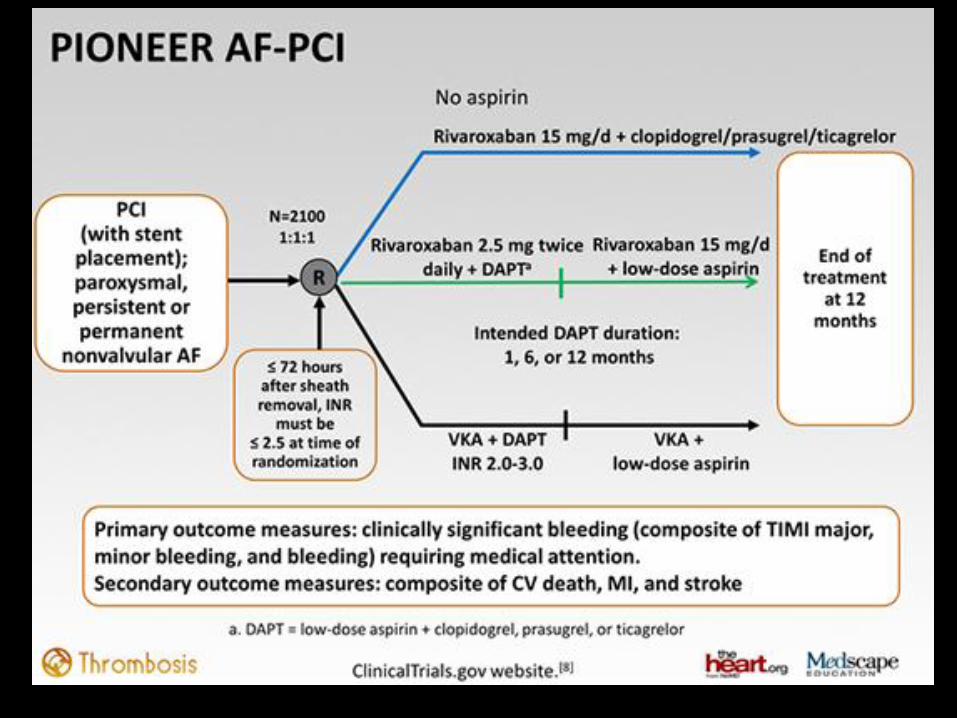

1. PIONEER–AF-PCI is not powered to detect differences in stroke rates…
2. it will still remain uncertain if rivaroxaban 2.5 mg b.i.d. would adequately reduce strokes in AF, even when combined with antiplatelet agents…
However….


1. Personalize antithrombotic therapy according to:
- Stroke risk (CHA2DS2 VASC)- Bleeding risk (HAS BLED)- Clinical setting (ACS vs elective)- Stent type (DES vs BMS)- Time from PCI/ACS
In practice… what to do?

2. Prefer:
- The lower tested dose for stroke prevention in
AF (that is, dabigatran 110 mg b.i.d., rivaroxaban
15 mg o.d. or apixaban 2.5 mg b.i.d.) to minimize
the risks of bleeding
- Clopidogrel instead of the more potent ticagrelor and prasugrel- New generation DES (or BMS) over first
generation DES
- Use of the radial approach, thus minimizing the
risk of access site bleeding
In practice… what to do?

Thanks!


Thanks!

Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: a joint consensus document of the European Society of Cardiology Working Group on
Thrombosis, European Heart Rhythm Association (EHRA), uropean Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS)




WOEST Trial limitations
- Only 69% of patients received OAC due to AF
- Most of the patients underwent elective PCI (70–75%)
-The femoral approach was used in 74%, increasing access site bleeding
- The differences between dual and triple therapy for theprimary end-point of ‘all bleeding’ were driven by minor bleeding events
- Proton pump inhibitors (PPIs) were not used routinely
- Triple therapy was continued for 12 months (and thus, the increased risk of bleeding is unsurprising)
- The trial population size was too small to meaningfullyassess major efficacy outcomes such as stent thrombosis or death