Embed Size (px)
Citation preview

Novel Oral Anticoagulant (OAC) Reversal Agents
Alexander Mok
EPE-2 Pharmacy Student
June 2, 2016

Today’s Learning Objectives
• Briefly review the coagulation pathway and NOAC pharmacology
• Describe the current limitations of NOAC uses • Describe the pharmacology behind the NOAC reversal
agents (praxabind, andexanet alfa) • Evaluating the literature on NOAC reversal agents by
using PICO to analyze the study objectives, population, interventions, comparator, outcomes, and limitations – RE-VERSE AD Trial (Praxabind) – ANNEXA-A and ANNEXA-R trials (Andexanet)
• Discuss future directions for the reversal agents

Coagulation Pathway

NOACs vs Warfarin
Study Drug vs Warfarin
Dabigatran (RE-LY)
150mg BID 110mg BID*
Rivaroxban (ROCKET-AF)
20mg QD 15mg QD*
Apixaban (ARISTOTLE)
5mg BID 2.5mg BID*
Edoxaban (ENGAGE-TIMI-AF 48)
60mg QD 30mg QD*
Stroke or Systemic Embolism
150mg: ↓
Non-inferior ↓
60mg: ↓
110mg: Non-inferior 30mg: Non-inferior
Major Bleeding
150mg: No difference
No difference, but demonstrated
superiority over warfarin for fatal
and critical bleeds
↓
60mg: ↓
110mg: ↓ 30mg: ↓
GI Bleeding 150mg: ↑ ↑ No difference 60mg: ↑
30mg: ↓
ICH ↓
Mortality NS NS ↓ ↓

Limitations of NOACs
• Less clinical experience with NOACs1,2
– vs. 60 years of warfarin experience
• Measurement issues1,3
– Not widely available in clinical settings
• ECT, DTT Dabigatran
• Anti-Factor Xa Rivaroxaban or Apixaban
• No established reversal agents4,11
– Lack of guidance in emergency surgery or major bleeding due to NOAC use

Andexanet Alfa
Idarucizumab (Praxabind)
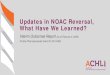
Reversal Agents on Coagulation Pathway

Idarucizumab (Praxabind)1,5,9,10
• Monoclonal, humanized antibody fragment
• Mimics thrombin (Factor II) • Binds exclusively to
dabigatran (both free dabigatran and thrombin/Factor II-bound dabigatran) – Binding affinity for dabigatran
is 350X higher than dabigatran’s affinity for thrombin
• Complex is then eliminated by kidneys

Andexanet Alfa1,6
• Recombinant modified human Factor Xa decoy protein
• Catalytically inactive
• Binds to Factor Xa inhibitors in their active site
• Enhances the activity of endogenous factor Xa and attenuates levels of anticoagulant activity
• Half-life: ~1 hour

Current Status of Reversal Agents7
Praxabind

RE-VERSE AD1,5: Reversal Effects of Idarucizumab on Active Dabigatran
• Study Objective:
– To determine the safety of idarucizumab (praxabind) in those who have serious bleeding or required an urgent procedure for those on dabigatran

RE-VERSE AD
• Population:
90 patients (18 y.o. or older on dabigatran) across 184 sites in 35
countries
Group A (n = 51): Those with overt,
uncontrollable, or life-threatening bleeding
(judged by the clinician)
Group B (n = 39): Those who required surgery or
other invasive procedures that could not be delayed for at least 8 hours and for
which normal hemostasis was required

RE-VERSE AD
• Intervention:
– Total dose of praxabind 5g administered IV as two bolus infusions (no more than 15 mins apart), each bolus containing 2.5g praxabind
• Comparison:
– No control group as it was deemed unethical by the authors to randomly assign patients to receive placebo or no active treatment

RE-VERSE AD • Outcomes:
– Efficacy Endpoints:
1° Outcomes (% Reversal of anticoagulant effect)
• Maximum reversal of anticoagulant effect of dabigatran based on central laboratory determination of dTT (dilute thrombin time) or ECT (ecarin clotting time), at any time between the end of the first infusion to 4 hours after the last infusion
2° Outcomes (Clinical resolution of bleeding)
• Group A: Extent of bleeding and hemodynamic stability at 10 and 30 mins, 1, 2, 4, 12, and 24 hrs after 2nd infusion or when deemed appropriate
• Group B: Hemostasis during the intervention was classified by the physician as normal or abnormal (on a scale of mild, moderate or severe) intra-operatively and 24 hrs post-surgery

RE-VERSE AD
• Outcomes:
– Safety Endpoints:
Adverse Events (Thrombotic Events or Death)
• Thrombotic events or deaths occurring from the time of idarucizumab infusion to 90 days after, with deaths classified as vascular (including bleeding) or nonvascular in origin

RE-VERSE AD Baseline Characteristics
Parameter Group A (n = 51) Group B (n = 39)
Median Age 77.0 76.0
Sex 63% male 46% male
Median Weight (kg) 70.5 73.0
Mean CrCl (ml/min) 59 65
Dose of Dabigatran • 150mg BID • 110mg BID • 75mg BID • Other
• 27% • 67% • 2% • 4%
• 38% • 62% • 0% • 0%
Indication of Dabigatran (AFIB) 92% 100%
Median Time since last dabigatran dose (hrs)
15.2 16.6
Elevated DTT at baseline (%) 78% 72%
Elevated ECT at baseline (%) 92% 87%
Type of Bleeding (%) • ICH • Trauma-related • GI • Other
• 35% • 18% • 39% • 22%
N/A

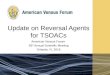
RE-VERSE AD: 1° Outcome (% Reversal of anticoagulant effect) in Group A
DTT in Group A ECT in Group A
2nd infusion 2nd infusion

RE-VERSE AD: 1° Outcome (% Reversal of anticoagulant effect) in Group B
DTT in Group B ECT in Group B
2nd infusion 2nd infusion

• Data was normalized using this equation:
% Reversal =
– Median Maximum percentage reversal in patients in group A and in those in group B was 100% for both DTT and ECT, as seen after the first infusion
RE-VERSE AD: 1° Outcome (% Reversal of anticoagulant effect)

• Out of the 90 patients analyzed:
– 31 patients (34%) had DTT or ECT values WNL at baseline
– These patients were enrolled and given praxabind because they fit the inclusion criteria, but were excluded from efficacy analysis because baseline clotting tests were within WNL
RE-VERSE AD: 1° Outcome (% Reversal of anticoagulant effect)

RE-VERSE AD: 2° Outcome (Clinical Resolution of Bleeding)
Patients that continued to Bleed
Type of Bleeding # of Patients (n = 13)
ICH 5
GI 4
Intramuscular 2
Pericardial 1
Retroperitoneal 1
Group A: Time to Cessation of Bleeding within 24 hours (n=51)
Remainder of Patients that Stopped Bleeding (n = 38)
Median Time to Cessation for Bleeding
11.4 hours

RE-VERSE AD: 2° Outcome (Clinical Resolution of Bleeding)
Category of Hemostasis # of Patients (n = 39)
Normal 33 (92%)
Mildly Abnormal 2
Moderately Abnormal 1
Other 3 - 1 patient idarucizumab obviated
need for emergency dialysis who had ingested too much dabigatran
- 2 patients despite full reversal, patients were too unstable for surgery
Group B: Occurrence of Major Bleeding intraoperatively and up to 24hrs post-surgery

RE-VERSE AD: Adverse Events (Deaths or Thrombotic Events)
Deaths Thrombotic Events
Total Number 18 in total 5 in total
Sub-categorized into:
9 in Group A 9 in Group B
1 DVT + PE two days after Tx 1 DVT + PE + Left Atrial Thrombus nine days after Tx 1 DVT seven days after Tx 1 NSTEMI thirteen days after Tx 1 ischemic stroke twenty-six days after Tx
10 deaths were due to vascular causes, including 5 fatal bleeding events
9/18 deaths within 96 hrs after treatment appear to be related to the index event (2 septic shock, 3 ICH, 1 multiorgan failure, 1 hemodynamic collapse, 1 respiratory failure, 1 cardiac arrest)

RE-VERSE AD
• Consider that:
– REVERSE-AD is still an ongoing trial
– Calculations are not all published
– Difficult study design

Limitations of RE-VERSE AD • Lack of a control
• Inclusion criteria and bleeding outcomes are subjective, due to judgements made by clinician
• Statistical analyses are descriptive
• Small sample size (n = 90, planned for 200-300; 34% were removed from efficacy analysis)
• Mortality rate is 20% (n = 18/90) and 5.6% for thrombotic events (n = 5/90)
• Correlation between prompt reversal and bleeding cessation after 11.4 hours in Group A
• 56% of patients used blood products, which is only reported in the supplemental appendix

Limitations of RE-VERSE AD
• Indications for patients in Group B undergoing surgery are in the supplemental appendix
– Uncertain the type of surgeries were carried out, how long they lasted
• 18% of the data on baseline renal function is missing
• Many hospitals lack these tests for rapid assessment of dabigatran levels

Summary of RE-VERSE AD • 1st trial that looked at the reversal of dabigatran by
praxabind in those who were bleeding or undergoing surgery
• Praxabind demonstrates immediate reversal of dabigatran’s effects by time reductions of DTT and ECT
• However, reductions of DTT and ECT do not translate to predictable times for clinical resolution of bleeding
• Remains to be seen if both the mortality and thrombotic rates are attributable to praxabind or the patient’s index event

ANNEXA-A and ANNEXA-R1,6
• Andexanet Alfa, a Novel Antidote to the Anticoagulation Effects of FXa Inhibitors Apixaban (ANNEXA-A) and Rivaroxaban (ANNEXA-R)
– 2 parallel trials
• Study Objective:
– To determine the efficacy and safety of andexanet alfa for the reversal of anticoagulation with apixaban or rivaroxaban in older healthy volunteers

ANNEXA-A and ANNEXA-R • Population:
145 healthy volunteers years of age 50-75
ANNEXA-A (n = 65): given apixaban
ANNEXA-R (n = 80): given rivaroxaban

ANNEXA-A and ANNEXA-R • Intervention and Comparison:
Step ANNEXA-A ANNEXA-R
Randomization to andexanet or placebo allocation
3:1
2:1
Anticoagulant Apixaban 5mg BID for 3.5 days Rivaroxaban 20mg QD for 4 days
Intervention Patients receive either: • Part 1 OR • Both Parts 1
and 2
Part 1: On day 4, 3 hours after last dose of apixaban andexanet 400mg IV bolus (30mg/min) Part 2: Followed by continuous infusion of 4mg/min for 2 hours (480mg in total)
Part 1: On day 4, 4 hours after last dose of rivaroxaban andexanet 800mg IV bolus (30mg/min) Part 2: Followed by continuous infusion of 8mg/min for 2 hours (960mg in total)
The dose for andenaxat is higher that in ANNEXA-A because of the higher initial maximum plasma concentration and larger volume of distribution of rivaroxaban

ANNEXA-A and ANNEXA-R • Outcomes:
– Efficacy Endpoints:
1° Outcome (% Reversal of anticoagulant effect)
• Percent change in anti-factor Xa activity from baseline (before andexanet or placebo administration) to nadir (after administration)

ANNEXA-A and ANNEXA-R
• Outcomes:
– Safety Endpoints:
Adverse Events
• Symptomatic thrombosis and bleeding
• Drug-related adverse events
• Safety outcomes were assessed on days 15, 36, and 43 after administration of the study drug

ANNEXA-A and ANNEXA-R Baseline Characteristics
• Age, BMI, CrCl generally similar
• Sex (39% were women from both trials)
• Race (varies; white is more predominant in all arms of the trials)

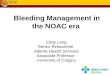
ANNEXA-A: 1° Outcome (% Reversal of anticoagulant effect)
Apixaban, Andexanet Bolus Apixaban, Andexanet Bolus + Infusion

ANNEXA-R: 1° Outcome (% Reversal of anticoagulant effect)
Rivaroxaban, Andexanet Bolus Rivaroxaban, Andexanet Bolus + Infusion

ANNEXA-A & ANNEXA-R: 1° Outcome (% Reversal of anticoagulant effect)

ANNEXA-A and ANNEXA-R Adverse Events
• No serious or severe adverse events or thrombotic events reported

ANNEXA-A and ANNEXA-R
• Limitations:
– Different doses of andexanet are required depending on the FXa inhibitor used
– Patients who require urgent reversal of factor Xa inhibition activity due to bleeding or for emergency surgery were excluded (ANNEXA-4 will address this)
– Unsure on the extent of duration of infusion to achieve hemostasis
– Limited baseline demographics (doesn’t mimic real-life situations)

Summary of ANNEXA-A and ANNEXA-R
• Trial looked at the efficacy and safety in reversal of apixaban or rivaroxaban by andexanet alfa in healthy volunteers
• Andexanet demonstrates immediate reversal of apixaban’s or rivaroxaban’s effects by time reductions of anti-factor Xa activity over placebo – Andexanet bolus + infusion allows for greater time reductions compared
to bolus alone
• However, this effect has not yet assessed if it can translate to predictable times for clinical resolution of bleeding (will be addressed by ANNEXA-4)
• Safety-wise there were no serious or severe adverse events or thrombotic events reported

Future Directions for Reversal Agents1
• As indicated by RE-VERSE AD study, it is challenging to design studies for these agents in patients with critical bleeds
• Cost/Convenience of agents
• Mortality and morbidity have still yet to be assessed in trials as primary outcomes
• Exact timing of usage for these drugs is not yet established
• Rebound anticoagulation

References
1. Tummala, R., Kavtaradze, A., Gupta, A. and Ghosh, R.K., 2016. Specific antidotes against direct oral anticoagulants: A comprehensive review of clinical trials data. International journal of cardiology, 214, pp.292-298.
2. Weitz, J.I., Semchuk, W., Turpie, A.G., Fisher, W.D., Kong, C., Ciaccia, A. and Cairns, J.A., 2015. Trends in Prescribing Oral Anticoagulants in Canada, 2008–2014. Clinical therapeutics, 37(11), pp.2506-2514.
3. Siegal, D.M. and Crowther, M.A., 2013. Acute management of bleeding in patients on novel oral anticoagulants. European heart journal, 34(7), pp.489-498.
4. Tran, H.A., Chunilal, S.D., Harper, P.L., Tran, H., Wood, E.M. and Gallus, A.S., 2013. An update of consensus guidelines for warfarin reversal. Med J Aust, 198(4), pp.198-199.
5. Pollack Jr, C.V., Reilly, P.A., Eikelboom, J., Glund, S., Verhamme, P., Bernstein, R.A., Dubiel, R., Huisman, M.V., Hylek, E.M., Kamphuisen, P.W. and Kreuzer, J., 2015. Idarucizumab for dabigatran reversal. New England Journal of Medicine, 373(6), pp.511-520.
6. Siegal, D.M., Curnutte, J.T., Connolly, S.J., Lu, G., Conley, P.B., Wiens, B.L., Mathur, V.S., Castillo, J., Bronson, M.D., Leeds, J.M. and Mar, F.A., 2015. Andexanet alfa for the reversal of factor Xa inhibitor activity. New England Journal of Medicine, 373(25), pp.2413-2424.
7. Leblanc, K. Stroke Prevention in Atrial Fibrillation: Adverse Bleeding. Presented on March 31 2016. University of Toronto: PHM204 Cardiology Lecture.
8. Stöllberger, C., Pommer, P., Schneider, B. and Finsterer, J., 2016. Concerns about idarucizumab for dabigatran reversal. Blood Coagulation & Fibrinolysis, 27(4), pp.473-474.
9. Dubé, P.A., Pharm, B. and Tox, C.C., 2014. Idarucizumab: a specific antidote for dabigatran. mars, 2015(6), p.1.
10. Glund, S., Stangier, J., Schmohl, M., Gansser, D., Norris, S., van Ryn, J., Lang, B., Ramael, S., Moschetti, V., Gruenenfelder, F. and Reilly, P., 2015. Safety, tolerability, and efficacy of idarucizumab for the reversal of the anticoagulant effect of dabigatran in healthy male volunteers: a randomised, placebo-controlled, double-blind phase 1 trial. The Lancet, 386(9994), pp.680-690.
11. 2015. Antidote Treatments for the Reversal of Direct Oral Anticoagulants. Canadian Agency for Drugs and Technologies in Health, 138, Report.